
Use of Venetoclax in Patients with Relapsed or Refractory Acute Myeloid Leukemia: The PETHEMA Registry Experience

 , , , , , , , , ,
, , , , , , , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Eligibility
2.3. Treatment Schedules
2.4. Study Definitions and Variables
2.5. Statistical Analysis
3. Results
3.1. Patient’s and Disease Characteristics
Venetoclax Treatment
3.2. Response Rates
3.3. Subsequent Salvage Therapy
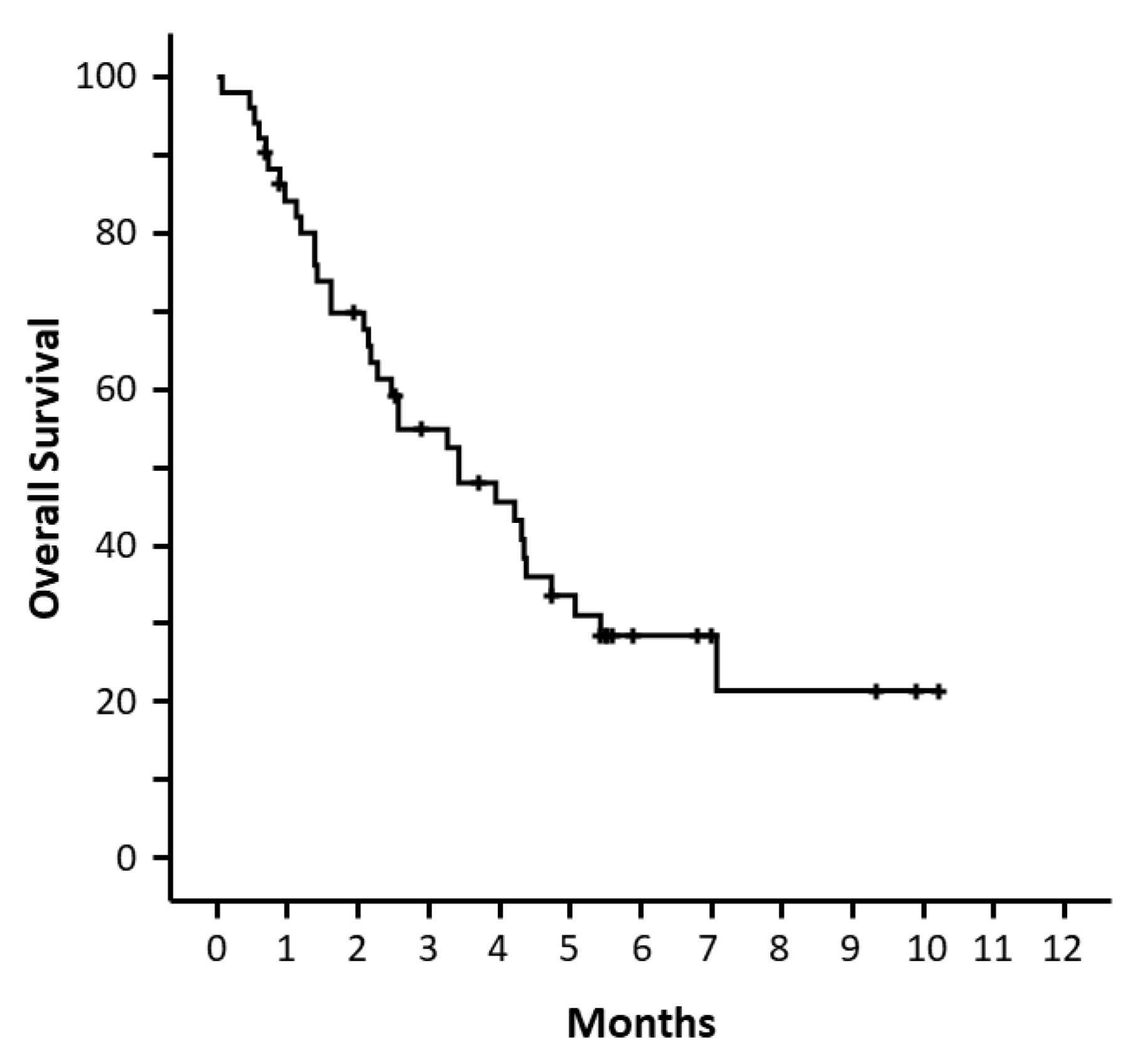
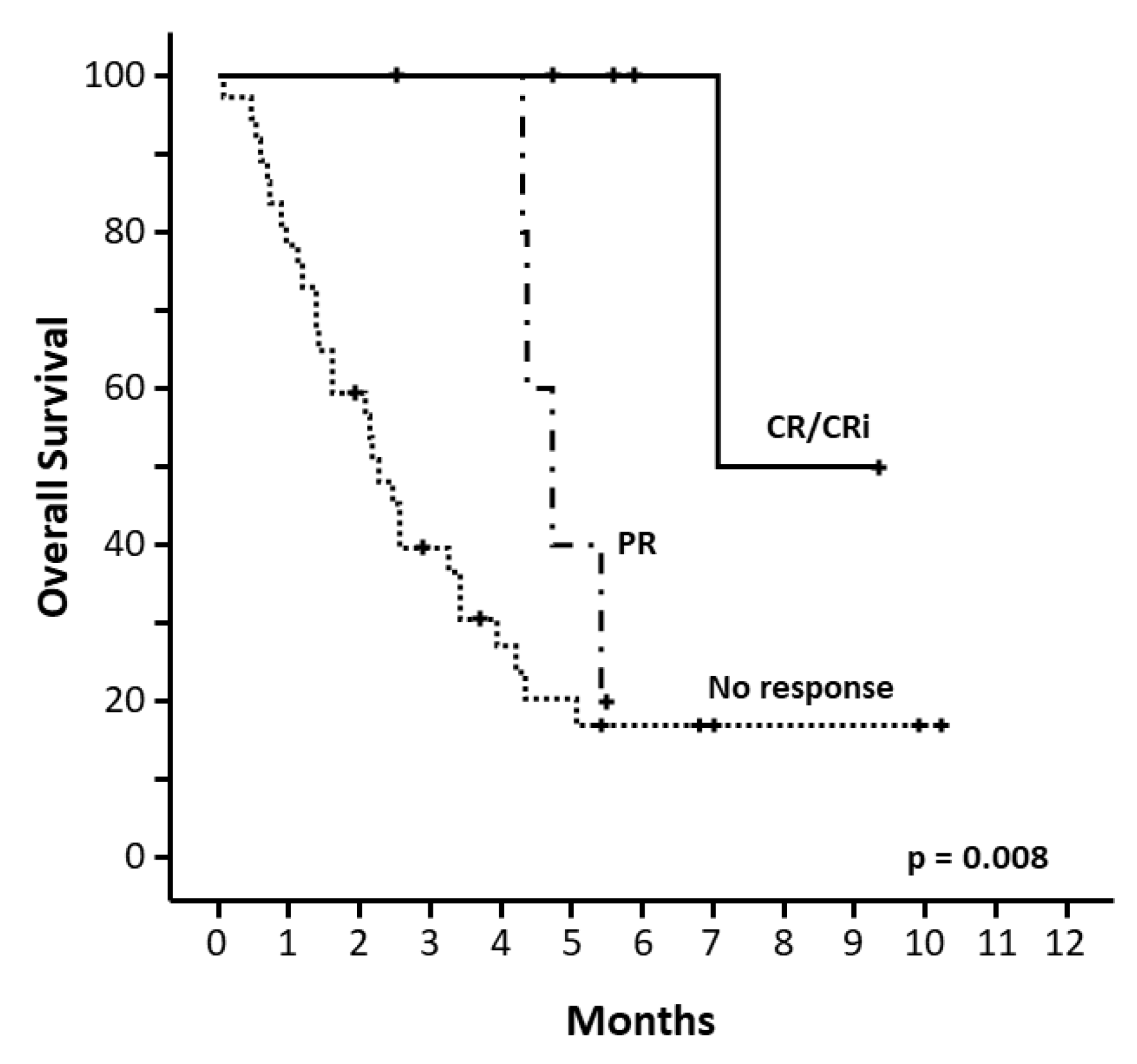
3.4. Overall Survival
3.5. Toxicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Appelbaum, F.R.; Gundacker, H.; Head, D.R.; Slovak, M.L.; Willman, C.L.; Godwin, J.E.; Anderson, J.E.; Petersdorf, S.H. Age and Acute Myeloid Leukemia. Blood 2006, 107, 3481–3485. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Andersson, T.M.-L.; Rachet, B.; Björkholm, M.; Lambert, P.C. Survival and Cure of Acute Myeloid Leukaemia in England, 1971-2006: A Population-Based Study. Br. J. Haematol. 2013, 162, 509–516. [Google Scholar] [CrossRef] [PubMed]
- DiNardo, C.D.; Pratz, K.; Pullarkat, V.; Jonas, B.A.; Arellano, M.; Becker, P.S.; Frankfurt, O.; Konopleva, M.; Wei, A.H.; Kantarjian, H.M.; et al. Venetoclax Combined with Decitabine or Azacitidine in Treatment-Naive, Elderly Patients with Acute Myeloid Leukemia. Blood 2019, 133, 7–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, A.H.; Strickland, S.A.; Hou, J.-Z.; Fiedler, W.; Lin, T.L.; Walter, R.B.; Enjeti, A.; Tiong, I.S.; Savona, M.; Lee, S.; et al. Venetoclax Combined With Low-Dose Cytarabine for Previously Untreated Patients With Acute Myeloid Leukemia: Results From a Phase Ib/II Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 1277–1284. [Google Scholar] [CrossRef]
- Kantarjian, H.M.; Thomas, X.G.; Dmoszynska, A.; Wierzbowska, A.; Mazur, G.; Mayer, J.; Gau, J.-P.; Chou, W.-C.; Buckstein, R.; Cermak, J.; et al. Multicenter, Randomized, Open-Label, Phase III Trial of Decitabine versus Patient Choice, with Physician Advice, of Either Supportive Care or Low-Dose Cytarabine for the Treatment of Older Patients with Newly Diagnosed Acute Myeloid Leukemia. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 2670–2677. [Google Scholar] [CrossRef] [Green Version]
- Dombret, H.; Seymour, J.F.; Butrym, A.; Wierzbowska, A.; Selleslag, D.; Jang, J.H.; Kumar, R.; Cavenagh, J.; Schuh, A.C.; Candoni, A.; et al. International Phase 3 Study of Azacitidine vs Conventional Care Regimens in Older Patients with Newly Diagnosed AML with >30% Blasts. Blood 2015, 126, 291–299. [Google Scholar] [CrossRef] [Green Version]
- Burnett, A.K.; Milligan, D.; Prentice, A.G.; Goldstone, A.H.; McMullin, M.F.; Hills, R.K.; Wheatley, K. A Comparison of Low-Dose Cytarabine and Hydroxyurea with or without All-Trans Retinoic Acid for Acute Myeloid Leukemia and High-Risk Myelodysplastic Syndrome in Patients Not Considered Fit for Intensive Treatment. Cancer 2007, 109, 1114–1124. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Jonas, B.A.; Pullarkat, V.; Thirman, M.J.; Garcia, J.S.; Wei, A.H.; Konopleva, M.; Döhner, H.; Letai, A.; Fenaux, P.; et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N. Engl. J. Med. 2020, 383, 617–629. [Google Scholar] [CrossRef]
- Wei, A.H.; Montesinos, P.; Ivanov, V.; DiNardo, C.D.; Novak, J.; Laribi, K.; Kim, I.; Stevens, D.A.; Fiedler, W.; Pagoni, M.; et al. Venetoclax plus LDAC for Newly Diagnosed AML Ineligible for Intensive Chemotherapy: A Phase 3 Randomized Placebo-Controlled Trial. Blood 2020, 135, 2137–2145. [Google Scholar] [CrossRef]
- Goldberg, A.D.; Horvat, T.Z.; Hsu, M.; Devlin, S.M.; Cuello, B.M.; Daley, R.J.; King, A.C.; Buie, L.W.; Glass, J.L.; Mauro, M.J.; et al. Venetoclax Combined with Either a Hypomethylating Agent or Low-Dose Cytarabine Shows Activity in Relapsed and Refractory Myeloid Malignancies. Blood 2017, 130, 1353. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Rausch, C.R.; Benton, C.; Kadia, T.; Jain, N.; Pemmaraju, N.; Daver, N.; Covert, W.; Marx, K.R.; Mace, M.; et al. Clinical Experience with the BCL2-Inhibitor Venetoclax in Combination Therapy for Relapsed and Refractory Acute Myeloid Leukemia and Related Myeloid Malignancies. Am. J. Hematol. 2018, 93, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Ganzel, C.; Ram, R.; Gural, A.; Wolach, O.; Gino-Moor, S.; Vainstein, V.; Nachmias, B.; Apel, A.; Koren-Michowitz, M.; Pasvolsky, O.; et al. Venetoclax Is Safe and Efficacious in Relapsed/Refractory AML. Leuk. Lymphoma 2020, 61, 2221–2225. [Google Scholar] [CrossRef]
- Gaut, D.; Burkenroad, A.; Duong, T.; Feammelli, J.; Sasine, J.; Schiller, G. Venetoclax Combination Therapy in Relapsed/Refractory Acute Myeloid Leukemia: A Single Institution Experience. Leuk. Res. 2020, 90, 106314. [Google Scholar] [CrossRef]
- Guerra, V.A.; DiNardo, C.; Konopleva, M. Venetoclax-Based Therapies for Acute Myeloid Leukemia. Best Pract. Res. Clin. Haematol. 2019, 32, 145–153. [Google Scholar] [CrossRef]
- Grimwade, D.; Hills, R.K.; Moorman, A.V.; Walker, H.; Chatters, S.; Goldstone, A.H.; Wheatley, K.; Harrison, C.J.; Burnett, A.K.; National Cancer Research Institute Adult Leukaemia Working Group. Refinement of Cytogenetic Classification in Acute Myeloid Leukemia: Determination of Prognostic Significance of Rare Recurring Chromosomal Abnormalities among 5876 Younger Adult Patients Treated in the United Kingdom Medical Research Council Trials. Blood 2010, 116, 354–365. [Google Scholar] [CrossRef] [Green Version]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and Management of AML in Adults: 2017 ELN Recommendations from an International Expert Panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [Green Version]
- Cheson, B.D.; Bennett, J.M.; Kopecky, K.J.; Büchner, T.; Willman, C.L.; Estey, E.H.; Schiffer, C.A.; Doehner, H.; Tallman, M.S.; Lister, T.A.; et al. Revised Recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J. Clin. Oncol. 2003, 21, 4642–4649. [Google Scholar] [CrossRef]
- Vives, S.; Martínez-Cuadrón, D.; Bergua Burgues, J.; Algarra, L.; Tormo, M.; Martínez-Sánchez, M.P.; Serrano, J.; Herrera, P.; Ramos, F.; Salamero, O.; et al. A Phase 3 Trial of Azacitidine versus a Semi-Intensive Fludarabine and Cytarabine Schedule in Older Patients with Untreated Acute Myeloid Leukemia. Cancer 2021, 127, 2003–2014. [Google Scholar] [CrossRef]
- Tenold, M.; Moskoff, B.; Benjamin, D.; Jonas, B.A. Retrospective Analysis of Adults with Acute Myeloid Leukemia Treated with Venetoclax Plus Hypomethylating Agents at a Comprehensive Cancer Center. Blood 2018, 132, 1424. [Google Scholar] [CrossRef]
- Aldoss, I.; Yang, D.; Pillai, R.; Sanchez, J.F.; Mei, M.; Aribi, A.; Ali, H.; Sandhu, K.; Al Malki, M.M.; Salhotra, A.; et al. Association of Leukemia Genetics with Response to Venetoclax and Hypomethylating Agents in Relapsed/Refractory Acute Myeloid Leukemia. Am. J. Hematol. 2019, 94, E253–E255. [Google Scholar] [CrossRef] [Green Version]
- Stahl, M.; Menghrajani, K.; Derkach, A.; Chan, A.; Xiao, W.; Glass, J.; King, A.C.; Daniyan, A.F.; Famulare, C.; Cuello, B.M.; et al. Clinical and Molecular Predictors of Response and Survival Following Venetoclax Therapy in Relapsed/Refractory AML. Blood Adv. 2021, 5, 1552–1564. [Google Scholar] [CrossRef]
- Konopleva, M.; Pollyea, D.A.; Potluri, J.; Chyla, B.; Hogdal, L.; Busman, T.; McKeegan, E.; Salem, A.H.; Zhu, M.; Ricker, J.L.; et al. Efficacy and Biological Correlates of Response in a Phase II Study of Venetoclax Monotherapy in Patients with Acute Myelogenous Leukemia. Cancer Discov. 2016, 6, 1106–1117. [Google Scholar] [CrossRef] [Green Version]
- Ram, R.; Amit, O.; Zuckerman, T.; Gurion, R.; Raanani, P.; Bar-On, Y.; Avivi, I.; Wolach, O. Venetoclax in Patients with Acute Myeloid Leukemia Refractory to Hypomethylating Agents-a Multicenter Historical Prospective Study. Ann. Hematol. 2019, 98, 1927–1932. [Google Scholar] [CrossRef]
- Aldoss, I.; Yang, D.; Aribi, A.; Ali, H.; Sandhu, K.; Al Malki, M.M.; Mei, M.; Salhotra, A.; Khaled, S.; Nakamura, R.; et al. Efficacy of the Combination of Venetoclax and Hypomethylating Agents in Relapsed/Refractory Acute Myeloid Leukemia. Haematologica 2018, 103, e404–e407. [Google Scholar] [CrossRef]
- Ramos, F.; Martinez-Cuadron, D.; Serrano, J.; Lopez-Pavia, M.; Fuertes-Nuñez, M.; Bernal, T.; Rodriguez-Gutierrez, J.I.; Recio, I.; Garrido, A.; Garcia, D.; et al. A Predictive Model for Early Death after Frontline Hypomethylating Agents in Elderly Unfit Acute Myeloid Leukemia Patients: Results from the Pethema Group. Blood 2019, 134, 648. [Google Scholar] [CrossRef]
- Acharya, U.H.; Halpern, A.B.; Wu, Q.V.; Voutsinas, J.M.; Walter, R.B.; Yun, S.; Kanaan, M.; Estey, E.H. Impact of Region of Diagnosis, Ethnicity, Age, and Gender on Survival in Acute Myeloid Leukemia (AML). J. Drug Assess. 2018, 7, 51–53. [Google Scholar] [CrossRef]
- Hossain, M.J.; Xie, L. Sex Disparity in Childhood and Young Adult Acute Myeloid Leukemia (AML) Survival: Evidence from US Population Data. Cancer Epidemiol. 2015, 39, 892–900. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | All Patients | Azacitidine + Venetoclax | Decitabine + Venetoclax | Low-Dose Cytarabine + Venetoclax | ||||
|---|---|---|---|---|---|---|---|---|
| n (%) | Median (Range) | n (%) | Median (Range) | n (%) | Median (Range) | n (%) | Median (Range) | |
| Total | 51 (100) | 30 (58.8) | 15 (29.4) | 6 (11.8) | ||||
| Sex (male), n (%) | 33 (64.7) | 19 (63.3) | 10 (66.7) | 4 (66.7) | ||||
| Age, median (range) | 51 | 68 (25–82) | 30 | 67 (41–76) | 15 | 64 (25–82) | 6 | 74 (71–77) |
| ≥65 y, n (%) | 34 (66.6) | 21 (70) | 7 (46.7) | 6 (100) | ||||
| Secondary AML | 20/50 (40) | 11/30 (36.7) | 7/15 (46.7) | 2/5 (40) | ||||
| MDS | 13/20 (65) | 6/ | 5 | 2 | ||||
| MPNs | 2/20 (10) | 1 | 1 | 0 | ||||
| t-AML | 6/20 (30) | 5 | 1 | 0 | ||||
| ECOG performance status | 50 | 30 | 9 | 5 | ||||
| 0 | 10 (20) | 7 (23.3) | 5 (55.6) | 3 (60) | ||||
| 1 | 14 (28) | 18 (60) | 3 (33.3) | 2 (40) | ||||
| ≥2 | 26 (52) | 5 (16.7) | 1 (11.1) | 0 | ||||
| WBC count (×109/L) | 48 | 2 (0–640) | 29 | 3.0 (0–110) | 13 | 1.0 (0–640) | 6 | 3.5 (1.0–20) |
| Hemoglobin (g/dL) | 48 | 8.0 (6–13) | 29 | 9.0 (7.0–13) | 13 | 8.0 (6.0–10.0) | 6 | 8.5 (7.0–10.0) |
| Bone marrow blast count, % | 44 | 36.5 (0–95) | 28 | 29 (2–92) | 10 | 45 (0–95) | 6 | 39 (24–86) |
| ≥50% | 16 (36.4) | 8 (28.6) | 5 (50) | 3 (50) | ||||
| FAB subtype | 43 | 30 | 15 | 6 | ||||
| M0/M6/M7 | 9 (21) | 5 (16.7) | 4 (26.7) | 0 | ||||
| M1/M2 | 10 (23) | 5 (16.7) | 3 (20) | 2 (33.3) | ||||
| M4/M5 | 11 (25.5) | 6 (20) | 3 (20) | 2 (33.3) | ||||
| Other | 13 (30) | 14 (19.8) | 5 (33.3) | 2 (33.3) | ||||
| Myelodysplasia-related changes AML | 34 (66.7) | 19 (63.3) | 12 (80) | 3 (50) | ||||
| Cytogenetics | 44 | 26 | 13 | 5 | ||||
| Favorable/Intermediate | 24 (54.5) | 14 (53.8) | 6 (46.2) | 4 (80) | ||||
| Adverse | 20 (45.5) | 12 (36.2) | 7 (53.8) | 1 (20) | ||||
| MRC risk stratification | 42 | 26 | 12 | 4 | ||||
| Favorable/intermediate | 20(47.6) | 12 (46.2) | 5 (41.7) | 3 (75) | ||||
| Adverse | 22 (52.4) | 14 (53.8) | 7 (58.3) | 1 (25) | ||||
| ELN 2017 risk stratification | 36 | 23 | 10 | 3 | ||||
| Favorable/intermediate | 5 (14) | 3 (139) | 1 (10) | 1 (33.3) | ||||
| Adverse | 31 (86) | 20 (87) | 9 (90) | 2 (66.7) | ||||
| Somatic mutations | ||||||||
| NPM1 | 6/41 (15) | 3/27 (11.1) | 2/11 (18.2) | 1/3 (33.3) | ||||
| FLT3-ITD | 5/41 (12) | 4/27 (14.8) | 1/11 (9.1) | 0/3 (0) | ||||
| P53 | 8/29 (27) | 6/20 (30) | 2/7 (28.6) | 0/2 (0) | ||||
| IDH1/2 | 9/27 (29) | 6/18 (33.3) | 1/7 (14.3) | 1/2 (50) | ||||
| First-line treatment | ||||||||
| Intensive chemotherapy, n = 35 | 35 (69) | 22 (73.3) | 11 (73.3) | 2 (33.3) | ||||
| LDAC-based regimen, n = 4 | 4 (8) | 2 (6.7) | 1 (6.7) | 1 (7.8) | ||||
| HMAs, n = 12 | 12 (23) | 6 (20.0) | 3 (20) | 12 (23.5) | ||||
| HMAs at any line prior to venetoclax, n = 26 | 26 (51) | 10 (33.3) | 10 (66.7) | 6 (100) | ||||
| Previous stem cell transplant, n = 12 | 12 (23) | 8 (26.7) | 4 (28.6) | 0 (0) | ||||
| Median number of previous lines (range) | 1 (1–4) | 2 (1–4) | 2 (1–3) | |||||
| AML status | ||||||||
| Refractory | 22 (43.1) | 16 (53.3) | 5 (33.3) | 1 (16.7) | ||||
| Relapse 1 | 23 (45.1) | 12 (40.0) | 8 (53.3) | 3 (50.0) | ||||
| Relapse ≥ 2 | 6 (11.8) | 2 (6.7) | 2 (13.3) | 2 (33.3) | ||||
| Refractory to any line prior VEN | 30 (58.8) | 18 (60.0) | 10 (66.7) | 2 (33.3) | ||||
| Refractory to prior HMAs | 17 (33.3) | 7 (23.3) | 8 (53.3) | 2 (33.3) | ||||
| Variable | Median (Days) | P-Univariate | P-Multivariate | HR (95% CI) |
|---|---|---|---|---|
| Total, n = 47 | 78 | |||
| Age | ||||
| <65 y, n = 17 | 34 | 0.919 | 0.326 | 1.48 (0.68–3.22) |
| ≥65 y, n = 34 | 34 | |||
| Sex | ||||
| Female, n = 18 | 131 | 0.217 | 0.010 | 3.37 (1.45–7.82) |
| Male, n = 33 | 78 | |||
| ECOG performance status | ||||
| 0, n = 10 | NR | 0.001 | 0.005 | 14.96 (1.91–117.21) |
| ≥1, n = 40 | 75 | |||
| ORR (CR + CRi + PR) | ||||
| Yes,11 | 215 | 0.004 | 0.002 | 6.13 (0.68–3.22) |
| No, 37 | 69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labrador, J.; Saiz-Rodríguez, M.; de Miguel, D.; de Laiglesia, A.; Rodríguez-Medina, C.; Vidriales, M.B.; Pérez-Encinas, M.; Sánchez-Sánchez, M.J.; Cuello, R.; Roldán-Pérez, A.; et al. Use of Venetoclax in Patients with Relapsed or Refractory Acute Myeloid Leukemia: The PETHEMA Registry Experience. Cancers 2022, 14, 1734. https://doi.org/10.3390/cancers14071734
Labrador J, Saiz-Rodríguez M, de Miguel D, de Laiglesia A, Rodríguez-Medina C, Vidriales MB, Pérez-Encinas M, Sánchez-Sánchez MJ, Cuello R, Roldán-Pérez A, et al. Use of Venetoclax in Patients with Relapsed or Refractory Acute Myeloid Leukemia: The PETHEMA Registry Experience. Cancers. 2022; 14(7):1734. https://doi.org/10.3390/cancers14071734
Chicago/Turabian StyleLabrador, Jorge, Miriam Saiz-Rodríguez, Dunia de Miguel, Almudena de Laiglesia, Carlos Rodríguez-Medina, María Belén Vidriales, Manuel Pérez-Encinas, María José Sánchez-Sánchez, Rebeca Cuello, Alicia Roldán-Pérez, and et al. 2022. "Use of Venetoclax in Patients with Relapsed or Refractory Acute Myeloid Leukemia: The PETHEMA Registry Experience" Cancers 14, no. 7: 1734. https://doi.org/10.3390/cancers14071734