
Blood Count Recovery Following Induction Therapy for Acute Myeloid Leukemia in Children Does Not Predict Survival

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analysis
3. Results
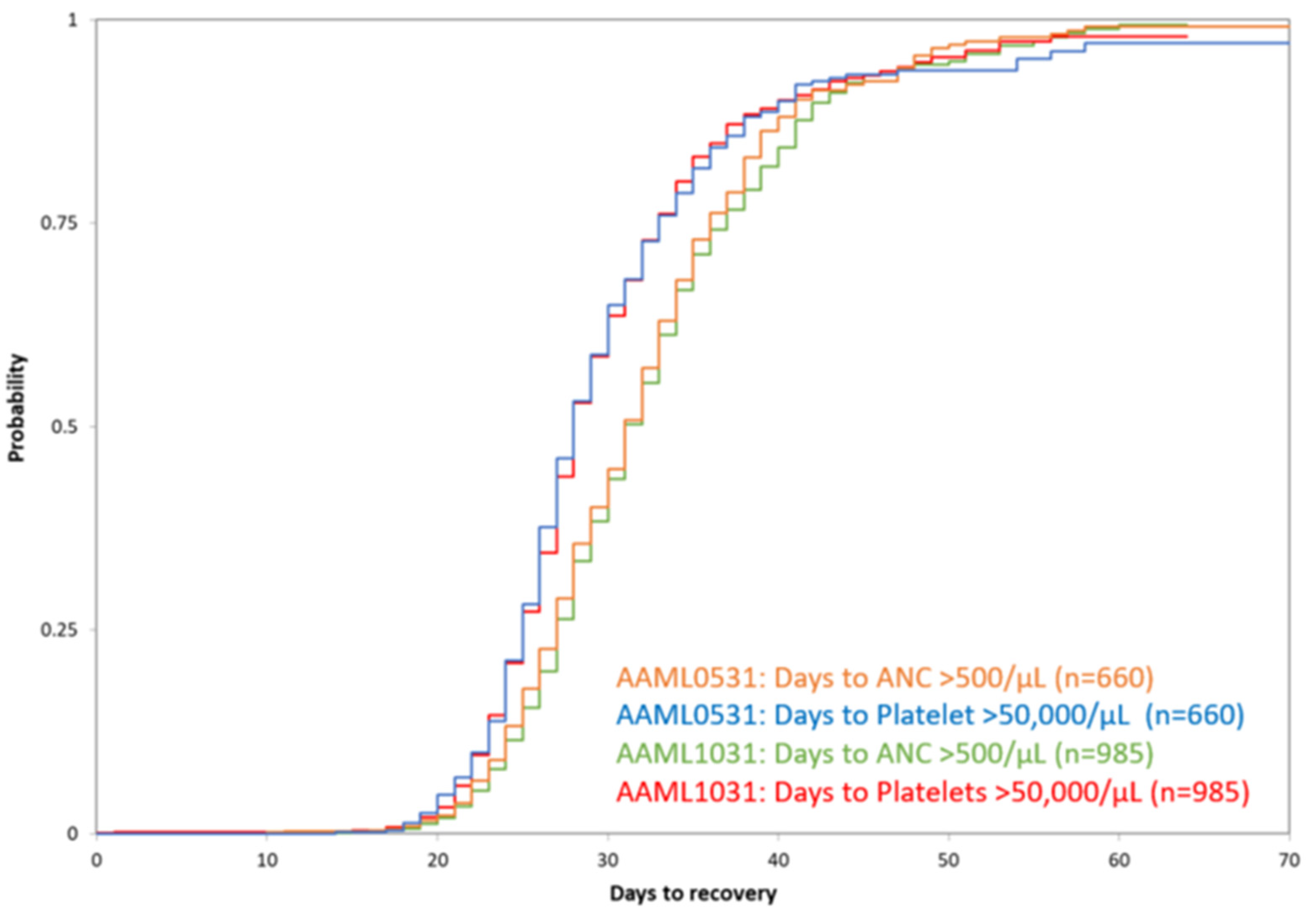
3.1. Proportion of Patients with Count Recovery
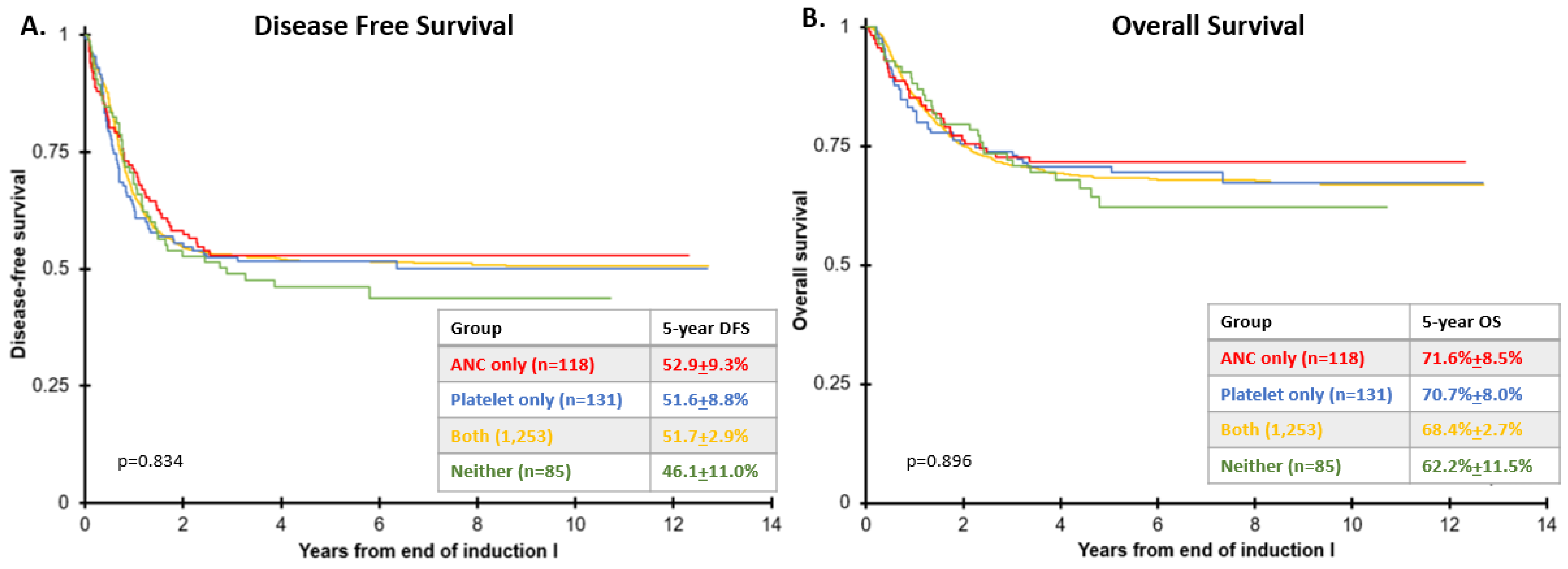
3.2. Survival According to Count Recovery
4. Discussion
4.1. Waiting for Count Recovery per IWG/ELN Criteria for CR Does Not Reflect Standard Practice in Pediatric AML
4.2. Count Recovery Does Not Significantly Impact Survival in These Large Pediatric Datasets
4.3. Cheson Criteria Should Be Reconsidered as the Standard Response Evaluation in Children with AML, and Perhaps Also in Adults
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Puumala, S.E.; Ross, J.A.; Aplenc, R.; Spector, L. Epidemiology of childhood acute myeloid leukemia. Pediatr. Blood Cancer 2013, 60, 728–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfied, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Bolouri, H.; Farrar, J.E.; Triche, T., Jr.; Ries, R.E.; Lim, E.L.; Alonzo, T.A.; Ma, Y.; Moore, R.; Mungal, A.J.; Marra, M.A.; et al. The molecular landscape of pediatric acute myeloid leukemia reveals recurrent structural alterations and age-specific mutational interactions. Nat. Med. 2018, 24, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarlock, K.; Zhong, S.; He, Y.; Ries, R.; Severson, E.; Bailey, M.; Morley, S.; Balasubramanian, S.; Erlich, R.; Lipson, D.; et al. Distinct age-associated molecular profiles in acute myeloid leukemia defined by comprehensive clinical genomic profiling. Oncotarget 2018, 9, 26417–26430. [Google Scholar] [CrossRef] [Green Version]
- Cheson, B.D.; Cassileth, P.A.; Head, D.R.; Schiffer, C.A.; Bennett, J.M.; Bloomfield, C.D.; Brunning, R.; Gale, R.P.; Grever, M.R.; Keating, M.J. Report of the National Cancer Institute-sponsored workshop on definitions of diagnosis and response in acute myeloid leukemia. J. Clin. Oncol. 1990, 8, 813–819. [Google Scholar] [CrossRef]
- Cheson, B.D.; Bennett, J.M.; Kopecky, K.J.; Büchner, T.; Willman, C.L.; Estey, E.H.; Schiffer, C.A.; Doehner, H.; Tallman, M.S.; Lister, T.A.; et al. Revised Recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J. Clin. Oncol. 2003, 21, 4642–4649. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.H.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Burnett, A.K.; Dombret, H.; Fenaux, P.; Grimwade, D.; Larson, R.A.; et al. Diagnosis and management of acute myeloid leukemia in adults: Recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood 2010, 115, 453–474. [Google Scholar] [CrossRef]
- Walter, R.B.; Kantarjian, H.M.; Huang, X.; Pierce, S.A.; Sun, Z.; Gundacker, H.M.; Ravandi, F.; Faderl, S.H.; Tallman, M.S.; Appelbaum, F.R.; et al. Effect of Complete Remission and Responses Less Than Complete Remission on Survival in Acute Myeloid Leukemia: A Combined Eastern Cooperative Oncology Group, Southwest Oncology Group, and M. D. Anderson Cancer Center Study. J. Clin. Oncol. 2010, 28, 1766–1771. [Google Scholar] [CrossRef]
- Gamis, A.S.; Alonzo, T.A.; Meshinchi, S.; Sung, L.; Gerbing, R.B.; Raimondi, S.C.; Hirsch, B.A.; Kahwash, S.B.; Winter, L.; Glick, K. Gemtuzumab ozogamicin in children and adolescents with de novo acute myeloid leukemia improves event-free survival by reducing relapse risk: Results from the randomized phase III Children’s Oncology Group trial AAML. J. Clin. Oncol. 2014, 32, 3021–3032. [Google Scholar] [CrossRef] [Green Version]
- Aplenc, R.; Meshinchi, S.; Sung, L.; Alonzo, T.; Choi, J.; Fisher, B.; Gerbing, R.; Hirsch, B.; Horton, T.; Kahwash, S.; et al. Bortezomib with standard chemotherapy for children with acute myeloid leukemia does not improve treatment outcomes: A report from the Children’s Oncology Group. Haematologica 2020, 105, 1879–1886. [Google Scholar] [CrossRef]
- Brodersen, L.E.; Gerbing, R.B.; Pardo, M.L.; Alonzo, T.A.; Paine, D.; Fritschle, W.; Hsu, F.-C.; Pollard, J.A.; Aplenc, R.; Kahwash, S.B.; et al. Morphologic remission status is limited compared to DeltaN flow cytometry: A Children’s Oncology Group AAML0531 report. Blood Adv. 2020, 4, 5050–5061. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457. [Google Scholar] [CrossRef]
- Kalbfleisch, J.; Prentice, R. The Statistical Analysis of Failure Time Data; John Wiley: New York, NY, USA, 1980. [Google Scholar]
- Cox, D.R. Regression Models and Life-Tables. Breakthr. Stat. 1992, 527–541. [Google Scholar] [CrossRef]
- Cooper, T.M.; Ries, R.E.; Alonzo, T.A.; Gerbing, R.B.; Loken, M.R.; Brodersen, L.E.; Raimondi, S.C.; Hirsch, B.A.; Aplenc, R.; Gamis, A.S.; et al. Revised Risk Stratification Criteria for Children with Newly Diagnosed Acute Myeloid Leukemia: A Report from the Children’s Oncology Group. Blood 2017, 130, 407. [Google Scholar]
- Lange, B.J.; Smith, F.O.; Feusner, J.; Barnard, D.R.; Dinndorf, P.; Feig, S.; Heerema, N.A.; Arndt, C.; Arceci, R.J.; Seibel, N.; et al. Outcomes in CCG-2961, a children’s oncology group phase 3 trial for untreated pediatric acute myeloid leukemia: A report from the children’s oncology group. Blood 2008, 111, 1044–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahamsson, J.; Forestier, E.; Heldrup, J.; Jahnukainen, K.; Jónsson, G.; Lausen, B.; Palle, J.; Zeller, B.; Hasle, H. Response-Guided Induction Therapy in Pediatric Acute Myeloid Leukemia with Excellent Remission Rate. J. Clin. Oncol. 2011, 29, 310–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Xie, H.; Wood, B.L.; Walter, R.; Pagel, J.M.; Becker, P.S.; Sandhu, V.K.; Abkowitz, J.L.; Appelbaum, F.R.; Estey, E.H. Relation of Clinical Response and Minimal Residual Disease and Their Prognostic Impact on Outcome in Acute Myeloid Leukemia. J. Clin. Oncol. 2015, 33, 1258–1264. [Google Scholar] [CrossRef]
- Kaspers, G.J.L.; Zimmermann, M.; Reinhardt, D.; Gibson, B.E.S.; Tamminga, R.Y.J.; Aleinikova, O.; Armendariz, H.; Dworzak, M.; Ha, S.-Y.; Hasle, H.; et al. Improved Outcome in Pediatric Relapsed Acute Myeloid Leukemia: Results of a Randomized Trial on Liposomal Daunorubicin by the International BFM Study Group. J. Clin. Oncol. 2013, 31, 599–607. [Google Scholar] [CrossRef]
- Rasche, M.; Zimmermann, M.; Steidel, E.; Alonzo, T.; Aplenc, R.; Bourquin, J.-P.; Boztug, H.; Cooper, T.; Gamis, A.; Gerbing, R.; et al. Survival Following Relapse in Children with Acute Myeloid Leukemia: A Report from AML-BFM and COG. Cancers 2021, 13, 2336. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services Food and Drug Administrations. Acute Myeloid Leukemia: Developing Drugs and Biological Products for Treatment; Guidance for Industry. August 2020. Available online: https://www.fda.gov/media/140821/download (accessed on 22 September 2021).
- Bloomfield, C.D.; Estey, E.; Pleyer, L.; Schuh, A.C.; Stein, E.M.; Tallman, M.S.; Wei, A. Time to repeal and replace response criteria for acute myeloid leukemia? Blood Rev. 2018, 32, 416–425. [Google Scholar] [CrossRef]
- Burnett, A.K.; Hills, R.K.; Hunter, A.E.; Milligan, D.; Kell, W.J.; Wheatley, K.; Yin, J.; McMullin, M.F.; Dignum, H.; Bowen, D.; et al. The addition of gemtuzumab ozogamicin to low-dose Ara-C improves remission rate but does not significantly prolong survival in older patients with acute myeloid leukaemia: Results from the LRF AML14 and NCRI AML16 pick-a-winner comparison. Leukemia 2013, 27, 75–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett, A.K.; Russell, N.H.; Hunter, A.E.; Milligan, D.; Knapper, S.; Wheatley, K.; Yin, J.; McMullin, M.F.; Ali, S.; Bowen, D.; et al. Clofarabine doubles the response rate in older patients with acute myeloid leukemia but does not improve survival. Blood 2013, 122, 1384–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Helm, L.H.; Scheepers, E.R.; Veeger, N.J.; Daenen, S.M.; Mulder, A.B.; van den Berg, E.; Vellenga, E.; Huls, G. Azacitidine might be beneficial in a subgroup of older AML patients compared to intensive chemotherapy: A single centre retrospective study of 227 consecutive patients. J. Hematol. Oncol. 2013, 6, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, N.; Miller, A.; Gandhi, S.; Ford, L.A.; Vigil, C.E.; Griffiths, E.A.; Thompson, J.E.; Wetzler, M.; Wang, E.S. Comparison of epigenetic versus standard induction chemotherapy for newly diagnosed acute myeloid leukemia patients >/=60 years old. Am. J. Hematol. 2015, 90, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Stein, E.M.; Dinardo, C.D.; Pollyea, D.A.; Fathi, A.T.; Roboz, G.J.; Altman, J.K.; Stone, R.M.; DeAngelo, D.J.; Levine, R.L.; Flinn, I.W.; et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood 2017, 130, 722–731. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| COG De Novo Cohort (AAML0531 and AAML1031 *) | Current COG AML Study (AAML1831 *) | IWG/ELN | |
|---|---|---|---|
| ANC | >1000 cells/μL | >500 cells/μL | >1000 cells/μL |
| Platelets | >75,000 cells/μL | >50,000 cells/μL | >100,000 cells/μL |
| Patients with <5% Marrow Disease by ΔN Flow Cytometry | ANC Threshold Only (>500/μL) | Platelet Threshold Only (>50,000/μL) | Met Both (ANC > 500/μL and Plt > 50,000/μL) | Met Neither (ANC ≤ 500/μL and Plt ≤ 50,000/μL) | ANC and/or Platelets Not Evaluated during Reporting Period | |
|---|---|---|---|---|---|---|
| AAML0531 | 660 | 57 (8.6%) | 55 (8.3%) | 507 (76.8%) | 41 (6.2%) | 4 (0.6%) |
| AAML1031 | 985 | 65 (6.6%) | 81 (8.2%) | 785 (79.7%) | 54 (5.5%) | 1 (0.1%) |
| Combined | 1645 | 122 (7.4%) | 136 (8.3%) | 1292 (78.5%) | 95 (5.8%) | 5 (0.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pommert, L.; Cooper, T.M.; Gerbing, R.B.; Brodersen, L.; Loken, M.; Gamis, A.; Aplenc, R.; Alonzo, T.A.; Kolb, E.A. Blood Count Recovery Following Induction Therapy for Acute Myeloid Leukemia in Children Does Not Predict Survival. Cancers 2022, 14, 616. https://doi.org/10.3390/cancers14030616
Pommert L, Cooper TM, Gerbing RB, Brodersen L, Loken M, Gamis A, Aplenc R, Alonzo TA, Kolb EA. Blood Count Recovery Following Induction Therapy for Acute Myeloid Leukemia in Children Does Not Predict Survival. Cancers. 2022; 14(3):616. https://doi.org/10.3390/cancers14030616
Chicago/Turabian StylePommert, Lauren, Todd M. Cooper, Robert B. Gerbing, Lisa Brodersen, Michael Loken, Alan Gamis, Richard Aplenc, Todd A. Alonzo, and Edward Anders Kolb. 2022. "Blood Count Recovery Following Induction Therapy for Acute Myeloid Leukemia in Children Does Not Predict Survival" Cancers 14, no. 3: 616. https://doi.org/10.3390/cancers14030616