
Demographic and Disease-Related Predictors of Socioemotional Development in Children with Neurofibromatosis Type 1 and Plexiform Neurofibromas: An Exploratory Study

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Socioemotional Development in the General Population
1.2. Socioemotional Development in Children with NF1
1.3. Demographic and Disease-Related Predictors of Socioemotional Development in Children with NF1
1.4. The Current Study
2. Materials and Methods
2.1. Participants and Inclusion Criteria
2.2. Measures
2.2.1. Socioemotional Functioning
2.2.2. Demographic Predictors
2.2.3. Disease-Related Predictors
2.3. Analysis Plan
3. Results
3.1. Characteristics of Participants
3.2. Descriptive Statistics and T-Test Results of Socioemotional Outcomes
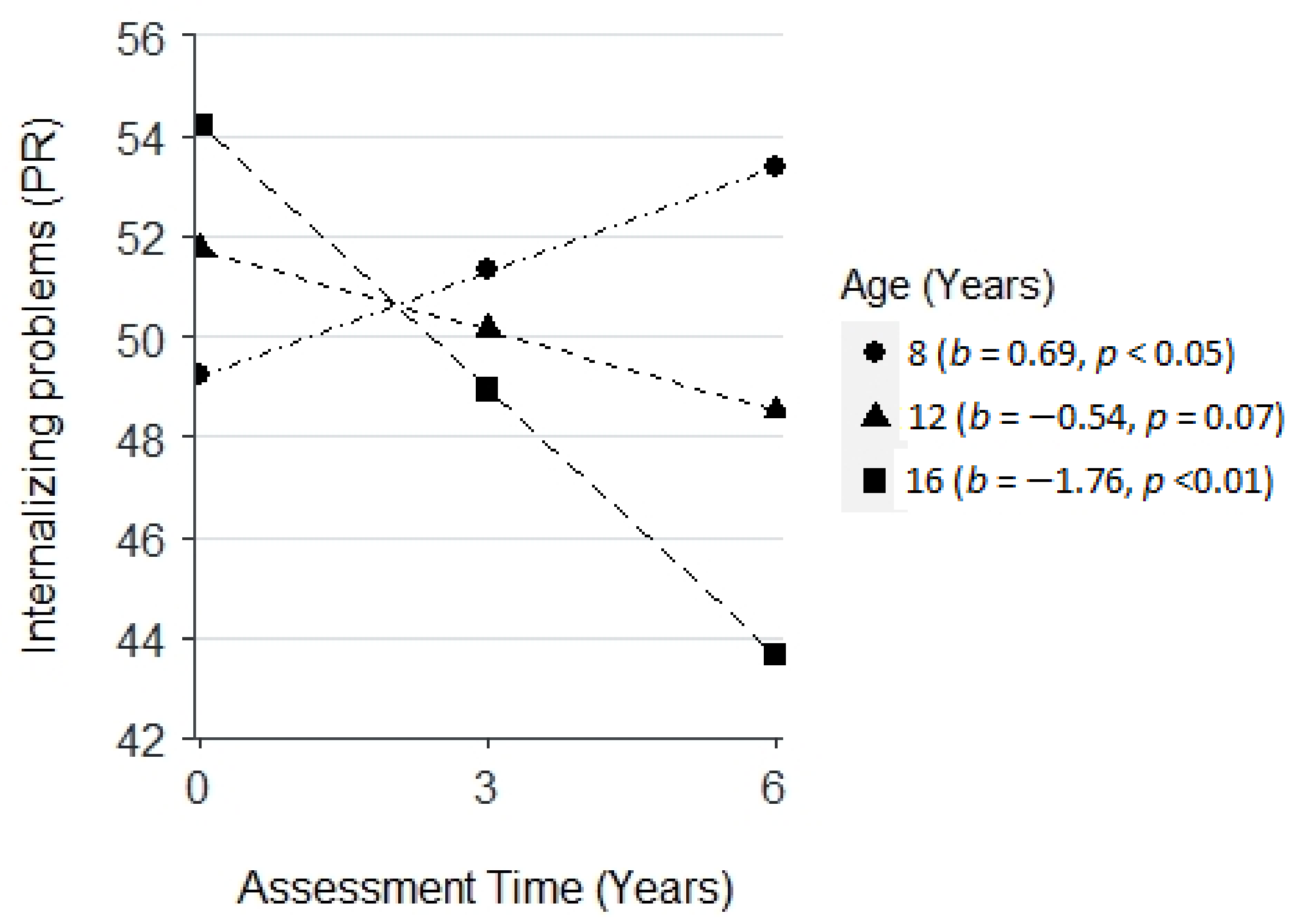
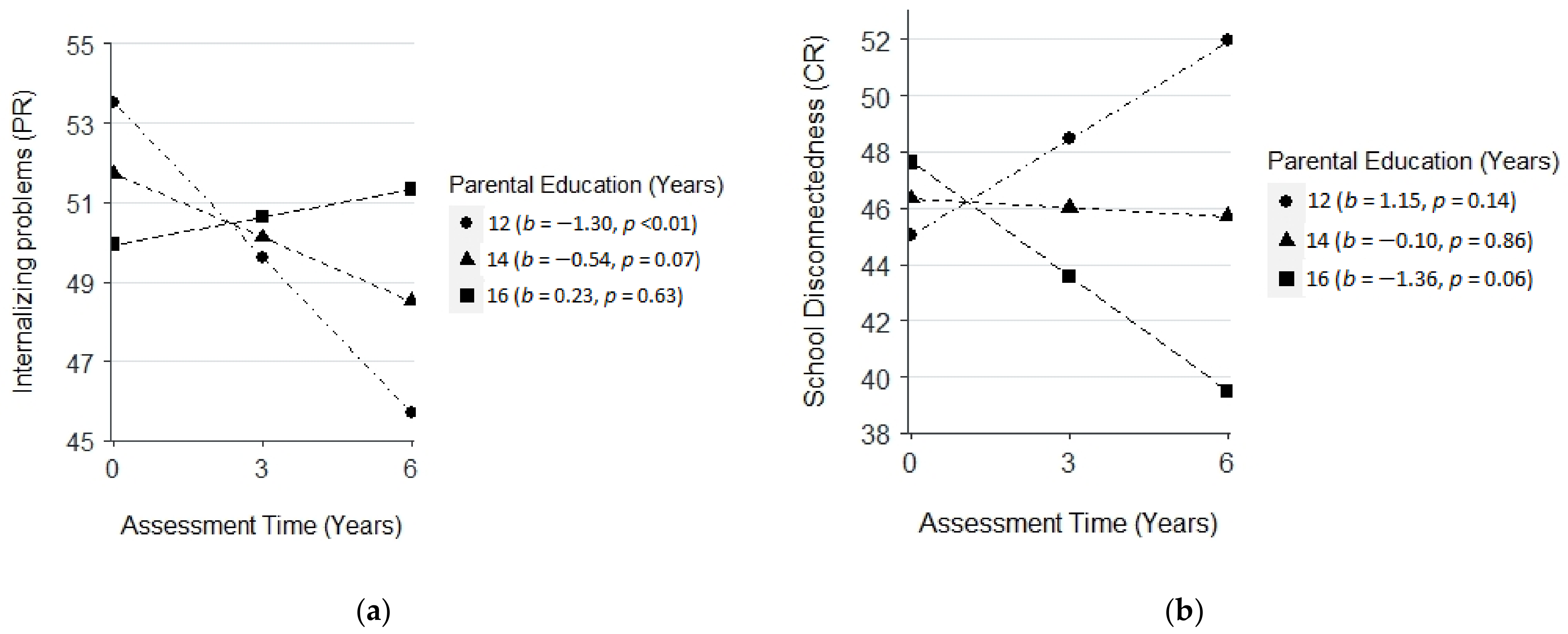
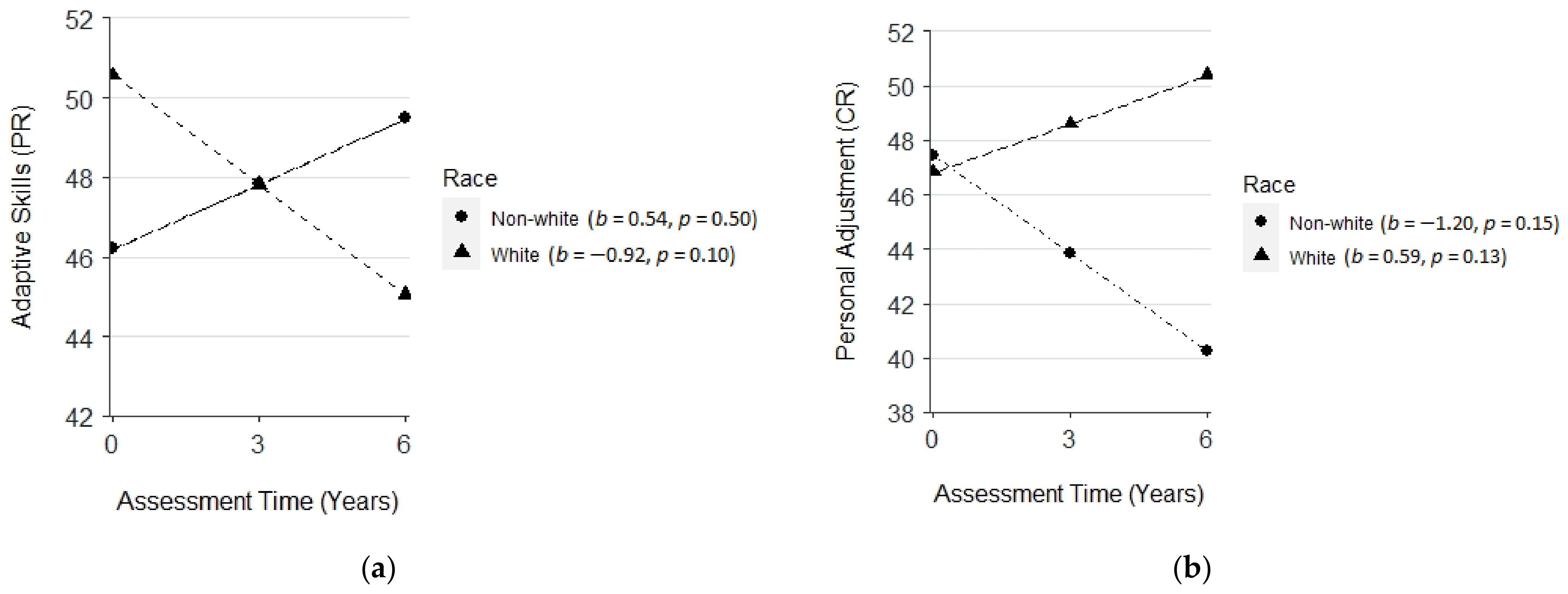
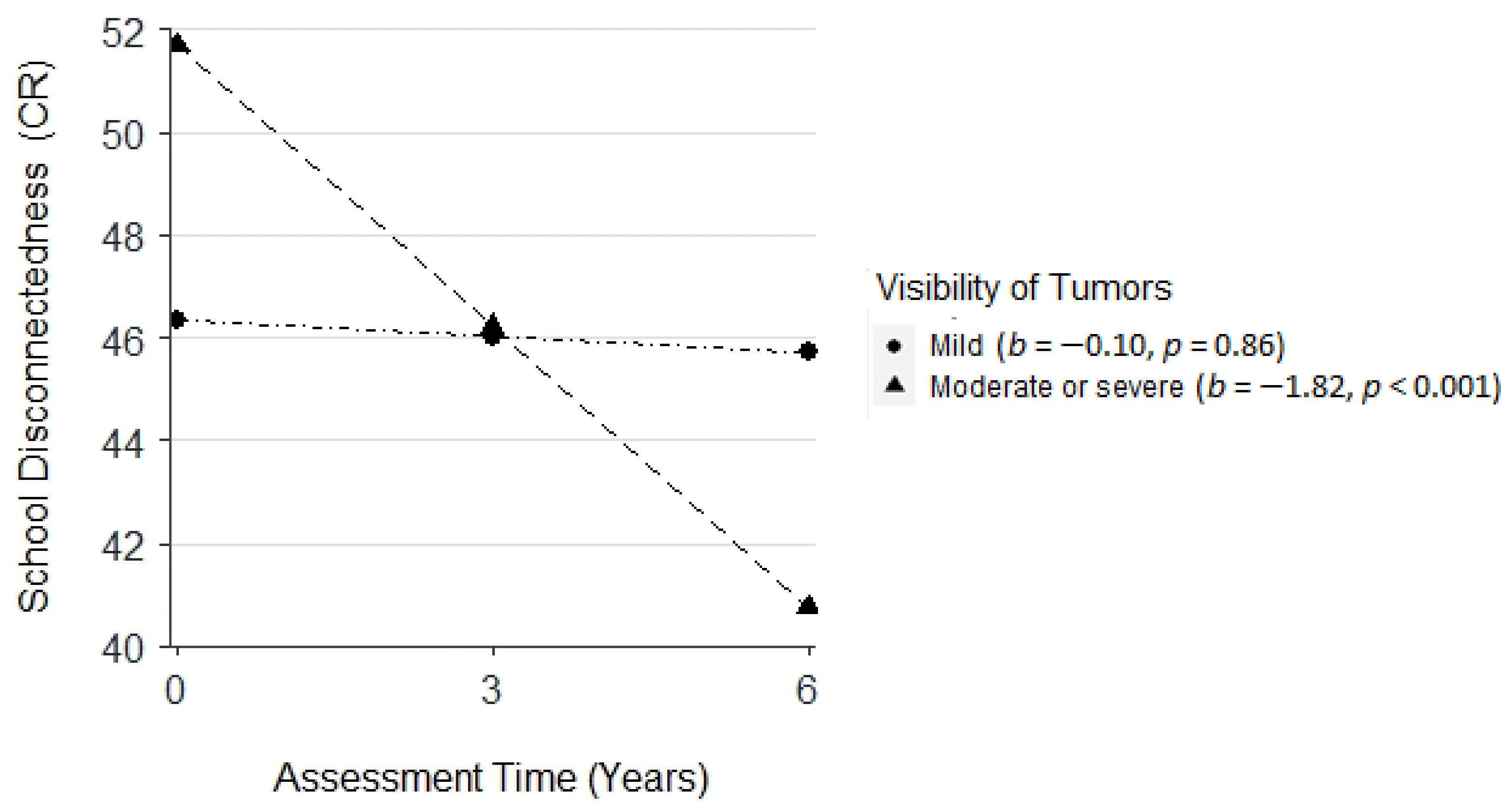
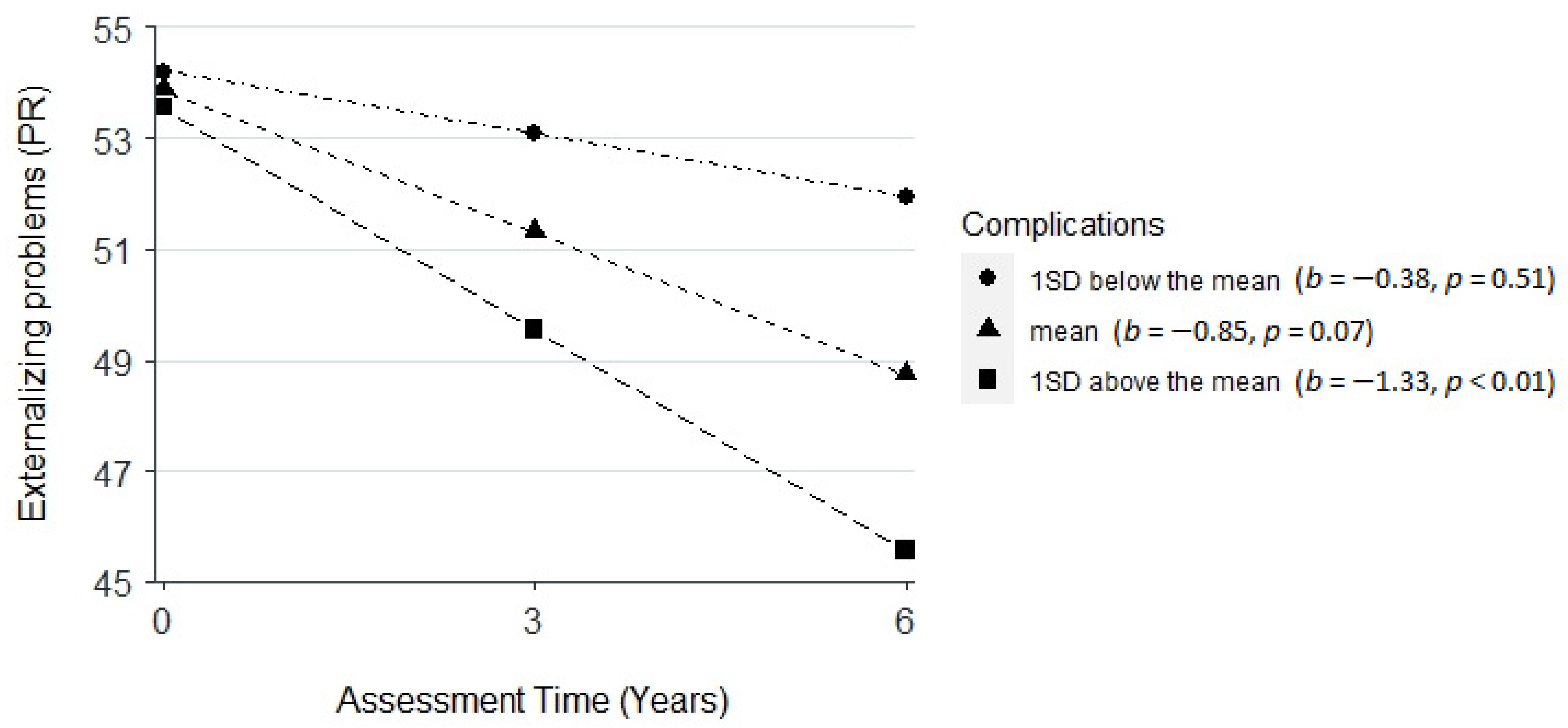
3.3. Change in Socioemotional Outcomes and Predictors
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McClatchey, A.I. Neurofibromatosis. Annu. Rev. Pathol. Mech. Dis. 2007, 2, 191–216. [Google Scholar] [CrossRef]
- Lehtonen, A.; Garg, S.; Roberts, S.A.; Trump, D.; Evans, D.G.; Green, J.; Huson, S.M. Cognition in children with neurofibromatosis type 1: Data from a population-based study. Dev. Med. Child Neurol 2015, 57, 645–651. [Google Scholar] [CrossRef]
- Vogel, A.C.; Gutmann, D.H.; Morris, S.M. Neurodevelopmental disorders in children with neurofibromatosis type 1. Dev. Med. Child Neurol. 2017, 59, 1112–1116. [Google Scholar] [CrossRef] [Green Version]
- Chisholm, A.K.; Haebich, K.M.; Pride, N.A.; Walsh, K.S.; Lami, F.; Ure, A.; Maloof, T.; Brignell, A.; Rouel, M.; Granader, Y.; et al. Delineating the autistic phenotype in children with neurofibromatosis type 1. Mol. Autism 2022, 13, 3. [Google Scholar] [CrossRef]
- Johnson, N.S.; Saal, H.M.; Lovell, A.M.; Schorry, E.K. Social and emotional problems in children with neurofibromatosis type 1: Evidence and proposed interventions. J. Pediatr. 1999, 134, 767–772. [Google Scholar] [CrossRef]
- Klein-Tasman, B.P.; Janke, K.M.; Luo, W.; Casnar, C.L.; Hunter, S.J.; Tonsgard, J.; Trapane, P.; van der Fluit, F.; Kais, L.A. Cognitive and Psychosocial Phenotype of Young Children with Neurofibromatosis-1. J. Int. Neuropsychol. Soc. 2014, 20, 88–98. [Google Scholar] [CrossRef] [Green Version]
- Martin, S.; Wolters, P.; Baldwin, A.; Gillespie, A.; Dombi, E.; Walker, K.; Widemann, B. Social-emotional functioning of children and adolescents with neurofibromatosis type 1 and plexiform neurofibromas: Relationships with cognitive, disease, and environmental variables. J. Pediatr. Psychol. 2012, 37, 713–724. [Google Scholar] [CrossRef]
- Morotti, H.; Mastel, S.; Keller, K.; Barnard, R.A.; Hall, T.; O’Roak, B.J.; Fombonne, E. Autism and attention-deficit/hyperactivity disorders and symptoms in children with neurofibromatosis type 1. Dev. Med. Child Neurol. 2021, 63, 226–232. [Google Scholar] [CrossRef]
- Keiley, M.K.; Bates, J.E.; Dodge, K.A.; Pettit, G.S. A cross-domain growth analysis: Externalizing and internalizing behaviors during 8 years of childhood. J. Abnorm. Child Psychol. 2000, 28, 161–179. [Google Scholar] [CrossRef]
- Marçal, K.E. Demographic and Socioeconomic Predictors of Behavioral Trajectories from Age 3 to 15: A Longitudinal Mixed Effects Approach. J. Child Fam. Stud. 2020, 29, 1818–1832. [Google Scholar] [CrossRef]
- Dopfner, M.; Hautmann, C.; Gortz-Dorten, A.; Klasen, F.; Ravens-Sieberer, U.; The BELLA Study Group. Long-term course of ADHD symptoms from childhood to early adulthood in a community sample. Eur. Child Adolesc. Psychiatry 2015, 24, 665–673. [Google Scholar] [CrossRef]
- Murray, A.L.; Booth, T.; Eisner, M.; Auyeung, B.; Murray, G.; Ribeaud, D. Sex differences in ADHD trajectories across childhood and adolescence. Dev. Sci 2019, 22, e12721. [Google Scholar] [CrossRef] [Green Version]
- Wustner, A.; Otto, C.; Schlack, R.; Holling, H.; Klasen, F.; Ravens-Sieberer, U. Risk and protective factors for the development of ADHD symptoms in children and adolescents: Results of the longitudinal BELLA study. PLoS ONE 2019, 14, e0214412. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Lerner, R.M. Trajectories of school engagement during adolescence: Implications for grades, depression, delinquency, and substance use. Dev. Psychol. 2011, 47, 233–247. [Google Scholar] [CrossRef]
- Flannery, K.M.; Vannucci, A.; Ohannessian, C.M. Using Time-Varying Effect Modeling to Examine Age-Varying Gender Differences in Coping Throughout Adolescence and Emerging Adulthood. J. Adolesc. Health 2018, 62, S27–S34. [Google Scholar] [CrossRef] [Green Version]
- Warren, M.T.; Wray-Lake, L.; Rote, W.M.; Shubert, J. Thriving while engaging in risk? Examining trajectories of adaptive functioning, delinquency, and substance use in a nationally representative sample of U.S. adolescents. Dev. Psychol. 2016, 52, 296–310. [Google Scholar] [CrossRef]
- Miner, J.L.; Clarke-Stewart, K.A. Trajectories of externalizing behavior from age 2 to age 9: Relations with gender, temperament, ethnicity, parenting, and rater. Dev. Psychol. 2008, 44, 771–786. [Google Scholar] [CrossRef]
- Petersen, I.T.; Bates, J.E.; Dodge, K.A.; Lansford, J.E.; Pettit, G.S. Describing and predicting developmental profiles of externalizing problems from childhood to adulthood. Dev. Psychopathol. 2015, 27, 791–818. [Google Scholar] [CrossRef] [Green Version]
- Gutman, L.M.; Codiroli McMaster, N. Gendered Pathways of Internalizing Problems from Early Childhood to Adolescence and Associated Adolescent Outcomes. J. Abnorm. Child Psychol. 2020, 48, 703–718. [Google Scholar] [CrossRef] [Green Version]
- Meyrose, A.K.; Klasen, F.; Otto, C.; Gniewosz, G.; Lampert, T.; Ravens-Sieberer, U. Benefits of maternal education for mental health trajectories across childhood and adolescence. Soc. Sci. Med. 2018, 202, 170–178. [Google Scholar] [CrossRef]
- Kuruczova, D.; Klanova, J.; Jarkovsky, J.; Pikhart, H.; Bienertova-Vasku, J. Socioeconomic characteristics, family structure and trajectories of children’s psychosocial problems in a period of social transition. PLoS ONE 2020, 15, e0234074. [Google Scholar] [CrossRef]
- Lansford, J.E.; Malone, P.S.; Castellino, D.R.; Dodge, K.A.; Pettit, G.S.; Bates, J.E. Trajectories of internalizing, externalizing, and grades for children who have and have not experienced their parents’ divorce or separation. J. Fam. Psychol. 2006, 20, 292–301. [Google Scholar] [CrossRef] [Green Version]
- Simons, R.L.; Lin, K.H.; Gordon, L.C.; Conger, R.D.; Lorenz, F.O. Explaining the Higher Incidence of Adjustment Problems among Children of Divorce Compared with Those in Two-Parent Families. J. Marriage Fam. 1999, 61, 1020–1033. [Google Scholar] [CrossRef]
- VanderValk, I.; Spruijt, E.; de Goede, M.; Maas, C.; Meeus, W. Family Structure and Problem Behavior of Adolescents and Young Adults: A Growth-Curve Study. J. Youth Adolesc. 2005, 34, 533–546. [Google Scholar] [CrossRef]
- Koth, C.W.; Cutting, L.E.; Denckla, M.B. The Association of Neurofibromatosis Type 1 and Attention Deficit Hyperactivity Disorder. Child Neuropsychol. 2000, 6, 185–194. [Google Scholar] [CrossRef]
- Dilts, C.V.; Carey, J.C.; Kircher, J.C.; Hoffman, R.O.; Creel, D.; Ward, K.; Clark, E.; Leonard, C.O. Children and adolescents with neurofibromatosis 1: A behavioral phenotype. J. Dev. Behav. Pediatr. 1996, 17, 229–239. [Google Scholar] [CrossRef]
- Van der Vaart, T.; Rietman, A.B.; Plasschaert, E.; Legius, E.; Elgersma, Y.; Moll, H.A.; Group, N.-S.S. Behavioral and cognitive outcomes for clinical trials in children with neurofibromatosis type 1. Neurology 2016, 86, 154–160. [Google Scholar] [CrossRef] [Green Version]
- Payne, J.M.; Haebich, K.M.; MacKenzie, R.; Walsh, K.S.; Hearps, S.J.C.; Coghill, D.; Barton, B.; Pride, N.A.; Ullrich, N.J.; Tonsgard, J.H.; et al. Cognition, ADHD Symptoms, and Functional Impairment in Children and Adolescents With Neurofibromatosis Type 1. J. Atten. Disord. 2021, 25, 1177–1186. [Google Scholar] [CrossRef]
- Wessel, L.E.; Gao, F.; Gutmann, D.H.; Dunn, C.M. Longitudinal Analysis of Developmental Delays in Children With Neurofibromatosis Type 1. J. Child Neurol. 2013, 28, 1689–1693. [Google Scholar] [CrossRef]
- Lorenzo, J.M.; Barton, B.P.; Arnold, S.S.B.A.; North, K.N.M.D. Developmental Trajectories of Young Children with Neurofibromatosis Type 1: A Longitudinal Study from 21 to 40 Months of Age. J. Pediatr. 2015, 166, 1006–1012.e1. [Google Scholar] [CrossRef]
- Glad, D.M.; Casnar, C.L.; Yund, B.D.; Enderle, M.J.; Siegel, D.H.; Basel, D.G.; Klein-Tasman, B.P. Adaptive Behavior and Executive Functioning in Children with Neurofibromatosis Type 1 Using a Mixed Design. J. Dev. Behav. Pediatr. 2020, 41, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Rietman, A.; Oostenbrink, R.; van Noort, K.; Franken, M.-C.; Catsman-Berrevoets, C.; Aarsen, F.; Heniksen, J.G.; de Nijs, P. Development of emotional and behavioral problems in neurofibromatosis type 1 during young childhood. Am. J. Med. Genet. Part A 2017, 173, 2373–2380. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, V.; Kemlin, I.; Dorison, N.; Billette de Villemeur, T.; Rodriguez, D.; Dellatolas, G. Neuropsychological evaluation and parental assessment of behavioral and motor difficulties in children with neurofibromatosis type 1. Res. Dev. Disabil. 2016, 48, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Rietman, A.; Vaart, T.; Plasschaert, E.; Nicholson, B.A.; Oostenbrink, R.; Krab, L.C.; Descheemaeker, M.J.; de Wit, M.C.; Moll, H.; Legius, E.; et al. Emotional and behavioral problems in children and adolescents with neurofibromatosis type 1. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2018, 177, 319–328. [Google Scholar] [CrossRef]
- Graf, A.; Landolt, M.A.; Mori, A.C.; Boltshauser, E. Quality of life and psychological adjustment in children and adolescents with neurofibromatosis type 1. J. Pediatr. 2006, 149, 348–353. [Google Scholar] [CrossRef]
- Granström, S.; Langenbruch, A.; Augustin, M.; Mautner, V.-F. Psychological Burden in Adult Neurofibromatosis Type 1 Patients: Impact of Disease Visibility on Body Image. Dermatology 2012, 224, 160–167. [Google Scholar] [CrossRef]
- Biotteau, M.; Déjean, S.; Lelong, S.; Iannuzzi, S.; Faure-Marie, N.; Castelnau, P.; Rivier, F.; Lauwers-Cancès, V.; Baudou, E.; Chaix, Y. Sporadic and Familial Variants in NF1: An Explanation of the Wide Variability in Neurocognitive Phenotype? Front. Neurol. 2020, 11, 368. [Google Scholar] [CrossRef]
- Leppich, K.; Schneider, J.; Eismann, C.; Ryczek, M.; Potratz, C.; Kaindl, A.M. Psychosocial and Socioeconomic Factors in Children with Neurofibromatosis Type 1. J. Pediatr. Neurol. 2021, 20, 188–193. [Google Scholar] [CrossRef]
- Hou, Y.; Allen, T.; Wolters, P.L.; Toledo-Tamula, M.A.; Martin, S.; Baldwin, A.; Reda, S.; Gillespie, A.; Goodwin, A.; Widemann, B.C. Predictors of cognitive development in children with neurofibromatosis type 1 and plexiform neurofibromas. Dev. Med. Child Neurol. 2020, 62, 977–984. [Google Scholar] [CrossRef]
- Jett, K.; Friedman, J.M. Clinical and genetic aspects of neurofibromatosis 1. Genet. Med. 2010, 12, 1–11. [Google Scholar] [CrossRef]
- Taddei, M.; Erbetta, A.; Esposito, S.; Saletti, V.; Bulgheroni, S.; Riva, D. Brain Tumors in NF1 Children: Influence on Neurocognitive and Behavioral Outcome. Cancers 2019, 11, 1772. [Google Scholar] [CrossRef] [Green Version]
- McNeill, A.M.; Hudock, R.L.; Foy, A.M.H.; Shanley, R.; Semrud-Clikeman, M.; Pierpont, M.E.; Berry, S.A.; Sommer, K.; Moertel, C.L.; Pierpont, E.I. Emotional functioning among children with neurofibromatosis type 1 or Noonan syndrome. Am. J. Med. Genet. Part A 2019, 179, 2433–2446. [Google Scholar] [CrossRef]
- Noll, R.B.; Reiter-Purtill, J.; Moore, B.D.; Schorry, E.K.; Lovell, A.M.; Vannatta, K.; Gerhardt, C.A. Social, emotional, and behavioral functioning of children with NF1. Am. J. Med. Genet. Part A 2007, 143A, 2261–2273. [Google Scholar] [CrossRef]
- Stumpf, D.A.; Alksne, J.F.; Annegers, J.F.; Brown, S.S.; Conneally, M.; Housman, D.; Leppert, M.F.; Miller, J.P.; Moss, M.L.; Pileggi, A.J.; et al. Neurofibromatosis. Conference statement. National Institutes of Health Consensus Development Conference. Arch. Neurol. 1988, 45, 575–578. [Google Scholar]
- Reynolds, C.R.; Kamphaus, R.W. The Clinician’s Guide to the Behavior Assessment System for Children (BASC); Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Reynolds, C.; Kamphaus, R. Behavior Assessment System for Children; Pearson Assessments: Bloomington, MN, USA, 2004. [Google Scholar]
- Pinheiro, J.; Bates, D.; DebRoy, S.; Sarkar, D.; Team, R.C. nlme: Linear and Nonlinear Mixed Effects Models; R Package Version 3.1-137; R Foundation: Vienna, Austria, 2018. [Google Scholar]
- Raudenbush, S.W.; Bryk, A.S. Hierarchical Linear Models: Applications and Data Analysis Methods; Sage: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Publications: New York, NY, USA, 2016. [Google Scholar]
- Huijbregts, S.C.; de Sonneville, L.M. Does cognitive impairment explain behavioral and social problems of children with neurofibromatosis type 1? Behav. Genet. 2011, 41, 430–436. [Google Scholar] [CrossRef] [Green Version]
- Bongers, I.L.; Koot, H.M.; van der Ende, J.; Verhulst, F.C. The Normative Development of Child and Adolescent Problem Behavior. J. Abnorm. Psychol. 2003, 112, 179–192. [Google Scholar] [CrossRef]
- Bolland, K.A.; Bolland, A.C.; Bolland, J.M.; Church, W.T.; Hooper, L.M.; Jaggers, J.W.; Tomek, S. Trajectories of School and Community Connectedness in Adolescence by Gender and Delinquent Behavior. J. Community Psychol. 2016, 44, 602–619. [Google Scholar] [CrossRef]
- Wallander, J.L.; Fradkin, C.; Chien, A.T.; Mrug, S.; Banspach, S.W.; Davies, S.; Elliott, M.N.; Franzini, L.; Schuster, M.A. Racial/ethnic disparities in health-related quality of life and health in children are largely mediated by family contextual differences. Acad. Pediatr. 2012, 12, 532–538. [Google Scholar] [CrossRef]
- Zilanawala, A.; Sacker, A.; Nazroo, J.; Kelly, Y. Ethnic differences in children’s socioemotional difficulties: Findings from the Millennium Cohort Study. Soc. Sci. Med. 2015, 134, 95–106. [Google Scholar] [CrossRef]
- Taylor, Z.E.; Conger, R.D. Promoting Strengths and Resilience in Single-Mother Families. Child Dev. 2017, 88, 350–358. [Google Scholar] [CrossRef]
- Martin, S.; Allen, T.; Toledo-Tamula, M.A.; Struemph, K.; Reda, S.; Wolters, P.L.; Baldwin, A.; Quinn, M.; Widemann, B.C. Acceptance and commitment therapy for adolescents and adults with neurofibromatosis type 1, plexiform neurofibromas, and chronic pain: Results of a randomized controlled trial. J. Context. Behav. Sci. 2021, 22, 93–101. [Google Scholar] [CrossRef]
- Martin, S.; Wolters, P.L.; Toledo-Tamula, M.A.; Schmitt, S.N.; Baldwin, A.; Starosta, A.; Gillespie, A.; Widemann, B. Acceptance and commitment therapy in youth with neurofibromatosis type 1 (NF1) and chronic pain and their parents: A pilot study of feasibility and preliminary efficacy. Am. J. Med. Genet. A 2016, 170, 1462–1470. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | 3 Years after Baseline | 6 Years after Baseline | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | t a | % AR/CS | n | Mean | SD | t a | % AR/CS | n | Mean | SD | t a | % AR/CS | |
| Externalizing Problems (PR) | 86 | 51.57 | 9.85 | 1.48 | 17 | 56 | 50.79 | 8.80 | 0.67 | 16 | 25 | 49.64 | 10.60 | −0.17 | 16 |
| Internalizing Problems (PR) | 86 | 56.85 | 12.24 | 5.19 *** | 37 | 56 | 56.45 | 11.67 | 4.13 *** | 36 | 25 | 55.16 | 11.13 | 2.32 * | 32 |
| Adaptive Skills (PR) | 86 | 45.59 | 9.66 | −4.23 *** | 34 | 56 | 46.41 | 10.33 | −2.60 *** | 34 | 25 | 45.24 | 11.23 | −2.12 * | 52 |
| School Disconnectedness (CR) | 67 | 48.87 | 11.43 | −0.81 | 18 | 52 | 46.83 | 10.84 | −2.11 | 19 | 23 | 46.61 | 11.73 | −1.39 | 13 |
| Internalizing Problems (CR) | 66 | 49.89 | 9.22 | −0.09 | 25 | 55 | 49.51 | 11.08 | −0.33 | 18 | 25 | 47.12 | 7.68 | −1.88 | 20 |
| Inattention/Hyperactivity (CR) | 67 | 51.51 | 11.95 | 1.03 | 25 | 55 | 51.44 | 9.99 | 1.07 | 18 | 25 | 51.64 | 10.59 | 0.77 | 20 |
| Personal Adjustment (CR) | 67 | 48.96 | 9.47 | −0.90 | 16 | 54 | 47.15 | 10.85 | −1.93 * | 30 | 25 | 51.00 | 9.66 | 0.52 | 8 |
| Age | 88 | 12.05 | 3.62 | 65 | 15.08 | 3.63 | 34 | 16.86 | 2.71 | ||||||
| Externalizing Problems (PR) | Internalizing Problems (PR) | Adaptive Skills (PR) | School Disconnectedness (CR) | Personal Adjustment (CR) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Parameters | β | SE | β | SE | β | SE | β | SE | β | SE |
| Intercept | 53.88 *** | 2.25 | 51.73 *** | 2.10 | 46.21 *** | 2.52 | 46.34 *** | 1.95 | 47.43 *** | 2.53 |
| Time | −0.85 | 0.46 | −0.54 | 0.29 | 0.54 | 0.80 | −0.10 | 0.57 | −1.20 | 0.82 |
| Age | −0.50 | 0.29 | 0.69 * | 0.33 | 0.37 | 0.28 | −0.97 ** | 0.35 | −0.04 | 0.31 |
| Male | −2.14 | 2.13 | ||||||||
| Pedu | −0.20 | 0.43 | −0.74 | 0.49 | 0.72 | 0.41 | 0.53 | 0.54 | ||
| White | −1.74 | 2.41 | 4.34 | 2.3 | −0.61 | 2.71 | ||||
| SINGLP | 4.32 * | 2.09 | ||||||||
| PNF1 | ||||||||||
| Visi | −2.64 | 2.38 | 5.35 * | 2.55 | ||||||
| Seve | 7.64 ** | 2.58 | −3.36 | 2.53 | ||||||
| Comp | −0.19 | 0.61 | 0.48 | 0.70 | ||||||
| Time × Age | −0.34 ** | 0.10 | ||||||||
| Time × Male | 0.35 | 0.41 | ||||||||
| Time × Pedu | 0.19 | 0.10 | 0.32 * | 0.14 | −0.22 | 0.16 | −0.52 * | 0.20 | ||
| Time × White | 0.58 | 0.50 | −1.46 * | 0.71 | 1.79 * | 0.89 | ||||
| Time × SINGLP | ||||||||||
| Time × PNF1 | ||||||||||
| Time × Visi | 1.25 | 0.72 | −1.72 * | 0.75 | ||||||
| Time × Seve | 0.22 | 0.78 | ||||||||
| Time × Comp | −0.28 * | 0.13 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, Y.; Wu, X.; Liu, D.; Martin, S.; Toledo-Tamula, M.A.; Allen, T.; Baldwin, A.; Gillespie, A.; Goodwin, A.; Widemann, B.C.; et al. Demographic and Disease-Related Predictors of Socioemotional Development in Children with Neurofibromatosis Type 1 and Plexiform Neurofibromas: An Exploratory Study. Cancers 2022, 14, 5956. https://doi.org/10.3390/cancers14235956
Hou Y, Wu X, Liu D, Martin S, Toledo-Tamula MA, Allen T, Baldwin A, Gillespie A, Goodwin A, Widemann BC, et al. Demographic and Disease-Related Predictors of Socioemotional Development in Children with Neurofibromatosis Type 1 and Plexiform Neurofibromas: An Exploratory Study. Cancers. 2022; 14(23):5956. https://doi.org/10.3390/cancers14235956
Chicago/Turabian StyleHou, Yang, Xian Wu, Dan Liu, Staci Martin, Mary Anne Toledo-Tamula, Taryn Allen, Andrea Baldwin, Andy Gillespie, Anne Goodwin, Brigitte C. Widemann, and et al. 2022. "Demographic and Disease-Related Predictors of Socioemotional Development in Children with Neurofibromatosis Type 1 and Plexiform Neurofibromas: An Exploratory Study" Cancers 14, no. 23: 5956. https://doi.org/10.3390/cancers14235956