
Impact of Systemic Autoimmune Diseases on Treatment Outcomes and Radiation Toxicities in Patients with Stage I Non-Small Cell Lung Cancer Receiving Stereotactic Body Radiation Therapy: A Matched Case-Control Analysis
 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Patients
2.2. RT Treatments
2.3. Follow-Up
2.4. Toxicities
2.5. Evaluation and Statistics
3. Results
3.1. Patients
3.2. Clinical Outcomes
3.3. Toxicities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boloker, G.; Wang, C.; Zhang, J. Updated Statistics of Lung and Bronchus Cancer in United States (2018). J. Thorac. Dis. 2018, 10, 1158–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer Incidence and Mortality Worldwide: Sources, Methods and Major Patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Matsumura, A.; Fukai, S.; Tamura, A.; Saito, R.; Zell, J.A.; Maruyama, Y.; Ziogas, A.; Kawahara, M.; Ignatius Ou, S.-H. Japanese Ethnicity Compared with Caucasian Ethnicity and Never-Smoking Status Are Independent Favorable Prognostic Factors for Overall Survival in Non-Small Cell Lung Cancer: A Collaborative Epidemiologic Study of the National Hospital Organization Study Group for Lung Cancer (NHSGLC) in Japan and a Southern California Regional Cancer Registry Databases. J. Thorac. Oncol. 2010, 5, 1001–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boily, G.; Filion, É.; Rakovich, G.; Kopek, N.; Tremblay, L.; Samson, B.; Goulet, S.; Roy, I.; Comité de L’évolution des Pratiques en Oncologie. Stereotactic Ablative Radiation Therapy for the Treatment of Early-Stage Non-Small-Cell Lung Cancer: CEPO Review and Recommendations. J. Thorac. Oncol. 2015, 10, 872–882. [Google Scholar] [CrossRef] [Green Version]
- Cooper, G.S.; Stroehla, B.C. The Epidemiology of Autoimmune Diseases. Autoimmun. Rev. 2003, 2, 119–125. [Google Scholar] [CrossRef]
- Wahren-Herlenius, M.; Dörner, T. Immunopathogenic Mechanisms of Systemic Autoimmune Disease. Lancet 2013, 382, 819–831. [Google Scholar] [CrossRef]
- Hayter, S.M.; Cook, M.C. Updated Assessment of the Prevalence, Spectrum and Case Definition of Autoimmune Disease. Autoimmun. Rev. 2012, 11, 754–765. [Google Scholar] [CrossRef]
- Khan, S.A.; Pruitt, S.L.; Xuan, L.; Gerber, D.E. Prevalence of Autoimmune Disease Among Patients With Lung Cancer: Implications for Immunotherapy Treatment Options. JAMA Oncol. 2016, 2, 1507–1508. [Google Scholar] [CrossRef] [Green Version]
- Benk, V.; Al-Herz, A.; Gladman, D.; Urowitz, M.; Fortin, P.R. Role of Radiation Therapy in Patients with a Diagnosis of Both Systemic Lupus Erythematosus and Cancer. Arthritis Care Res. 2005, 53, 67–72. [Google Scholar] [CrossRef]
- Giaj-Levra, N.; Sciascia, S.; Fiorentino, A.; Fersino, S.; Mazzola, R.; Ricchetti, F.; Roccatello, D.; Alongi, F. Radiotherapy in Patients with Connective Tissue Diseases. Lancet Oncol. 2016, 17, e109–e117. [Google Scholar] [CrossRef]
- Nilsen, L.B.; Missal, M.E.; Condemi, J.J. Appearance of Hodgkin’s Disease in a Patient with Systemic Lupus Erythematosus. Cancer 1967, 20, 1930–1933. [Google Scholar] [CrossRef] [PubMed]
- Diao, K.; Chen, Y.-H.; Catalano, P.J.; Lee, S.; Milani, N.; Killoran, J.H.; Baldini, E.H.; Chen, A.B.; Kozono, D.E.; Mak, R.H. Radiation Toxicity in Patients with Collagen Vascular Disease and Intrathoracic Malignancy Treated with Modern Radiation Techniques. Radiother. Oncol. 2017, 125, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Koukourakis, M.I.; Maltezos, E. Amifostine Administration during Radiotherapy for Cancer Patients with Genetic, Autoimmune, Metabolic and Other Diseases. AntiCancer Drugs 2006, 17, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Adzić, T.N.; Pesut, D.P.; Nagorni-Obradović, L.M.; Stojsić, J.M.; Vasiljević, M.D.; Bouros, D. Clinical Features of Lung Cancer in Patients with Connective Tissue Diseases: A 10-Year Hospital Based Study. Respir. Med. 2008, 102, 620–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirsadraee, S.; Oswal, D.; Alizadeh, Y.; Caulo, A.; van Beek, E. The 7th Lung Cancer TNM Classification and Staging System: Review of the Changes and Implications. World J. Radiol. 2012, 4, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Onishi, H.; Kawakami, H.; Marino, K.; Komiyama, T.; Kuriyama, K.; Araya, M.; Saito, R.; Aoki, S.; Araki, T. A Simple Respiratory Indicator for Irradiation during Voluntary Breath Holding: A One-Touch Device without Electronic Materials. Radiology 2010, 255, 917–923. [Google Scholar] [CrossRef]
- Parisi, G.; Ceschia, T.; Parisi, A. Stereotactic Body Radiation Therapy and Surgery for Early Lung Cancer “Two Sides of the Same Coin”. J. Thorac. Dis. 2019, 11, S271–S274. [Google Scholar] [CrossRef]
- Lin, A.; Abu-Isa, E.; Griffith, K.A.; Ben-Josef, E. Toxicity of Radiotherapy in Patients with Collagen Vascular Disease. Cancer 2008, 113, 648–653. [Google Scholar] [CrossRef]
- Shaikh, P.M.; Singh, S.A.; Alite, F.; Vargo, J.A.; Emami, B.; Wu, M.-J.; Jacobson, G.; Bakalov, V.; Small, W.; Dahshan, B.; et al. Radiation Toxicity in Patients with Collagen Vascular Disease: A Meta-Analysis of Case-Control Studies. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 1214–1226. [Google Scholar] [CrossRef]
- Gelbard, A.; Garnett, C.T.; Abrams, S.I.; Patel, V.; Gutkind, J.S.; Palena, C.; Tsang, K.-Y.; Schlom, J.; Hodge, J.W. Combination Chemotherapy and Radiation of Human Squamous Cell Carcinoma of the Head and Neck Augments CTL-Mediated Lysis. Clin. Cancer Res. 2006, 12, 1897–1905. [Google Scholar] [CrossRef]
- Takeshima, T.; Chamoto, K.; Wakita, D.; Ohkuri, T.; Togashi, Y.; Shirato, H.; Kitamura, H.; Nishimura, T. Local Radiation Therapy Inhibits Tumor Growth through the Generation of Tumor-Specific CTL: Its Potentiation by Combination with Th1 Cell Therapy. Cancer Res. 2010, 70, 2697–2706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, Y.; Mimura, K.; Yoshimoto, Y.; Watanabe, M.; Ohkubo, Y.; Izawa, S.; Murata, K.; Fujii, H.; Nakano, T.; Kono, K. Immunogenic Tumor Cell Death Induced by Chemoradiotherapy in Patients with Esophageal Squamous Cell Carcinoma. Cancer Res. 2012, 72, 3967–3976. [Google Scholar] [CrossRef] [Green Version]
- Gameiro, S.R.; Jammeh, M.L.; Wattenberg, M.M.; Tsang, K.Y.; Ferrone, S.; Hodge, J.W. Radiation-Induced Immunogenic Modulation of Tumor Enhances Antigen Processing and Calreticulin Exposure, Resulting in Enhanced T-Cell Killing. Oncotarget 2014, 5, 403–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, M.M.; Powell, S.N. Irradiation in the Setting of Collagen Vascular Disease: Acute and Late Complications. J. Clin. Oncol. 1997, 15, 2728–2735. [Google Scholar] [CrossRef]
- Ross, J.G.; Hussey, D.H.; Mayr, N.A.; Davis, C.S. Acute and Late Reactions to Radiation Therapy in Patients with Collagen Vascular Diseases. Cancer 1993, 71, 3744–3752. [Google Scholar] [CrossRef] [PubMed]
- Phan, C.; Mindrum, M.; Silverman, C.; Paris, K.; Spanos, W. Matched-Control Retrospective Study of the Acute and Late Complications in Patients with Collagen Vascular Diseases Treated with Radiation Therapy. Cancer J. 2003, 9, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Podlesnikar, T.; Berlot, B.; Dolenc, J.; Goričar, K.; Marinko, T. Radiotherapy-Induced Cardiotoxicity: The Role of Multimodality Cardiovascular Imaging. Front. Cardiovasc. Med. 2022, 9, 887705. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.D.; Paulus, R.; Komaki, R.; Masters, G.; Blumenschein, G.; Schild, S.; Bogart, J.; Hu, C.; Forster, K.; Magliocco, A.; et al. Standard-Dose versus High-Dose Conformal Radiotherapy with Concurrent and Consolidation Carboplatin plus Paclitaxel with or without Cetuximab for Patients with Stage IIIA or IIIB Non-Small-Cell Lung Cancer (RTOG 0617): A Randomised, Two-by-Two Factorial Phase 3 Study. Lancet Oncol. 2015, 16, 187–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dess, R.T.; Sun, Y.; Matuszak, M.M.; Sun, G.; Soni, P.D.; Bazzi, L.; Murthy, V.L.; Hearn, J.W.D.; Kong, F.-M.; Kalemkerian, G.P.; et al. Cardiac Events After Radiation Therapy: Combined Analysis of Prospective Multicenter Trials for Locally Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2017, 35, 1395–1402. [Google Scholar] [CrossRef]
- Wang, K.; Pearlstein, K.A.; Patchett, N.D.; Deal, A.M.; Mavroidis, P.; Jensen, B.C.; Lipner, M.B.; Zagar, T.M.; Wang, Y.; Lee, C.B.; et al. Heart Dosimetric Analysis of Three Types of Cardiac Toxicity in Patients Treated on Dose-Escalation Trials for Stage III Non-Small-Cell Lung Cancer. Radiother. Oncol. 2017, 125, 293–300. [Google Scholar] [CrossRef]
- Chan, S.T.; Ruan, D.; Shaverdian, N.; Raghavan, G.; Cao, M.; Lee, P. Effect of Radiation Doses to the Heart on Survival for Stereotactic Ablative Radiotherapy for Early-Stage Non-Small-Cell Lung Cancer: An Artificial Neural Network Approach. Clin. Lung Cancer 2020, 21, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Reshko, L.B.; Kalman, N.S.; Hugo, G.D.; Weiss, E. Cardiac Radiation Dose Distribution, Cardiac Events and Mortality in Early-Stage Lung Cancer Treated with Stereotactic Body Radiation Therapy (SBRT). J. Thorac. Dis. 2018, 10, 2346–2356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onishi, H.; Araki, T. Stereotactic Body Radiation Therapy for Stage I Non-Small-Cell Lung Cancer: A Historical Overview of Clinical Studies. Jpn. J. Clin. Oncol. 2013, 43, 345–350. [Google Scholar] [CrossRef]
- Lowell, D.; Tatter, S.B.; Bourland, J.D.; deGuzman, A.F.; Ekstrand, K.E.; Ellis, T.L.; Lovato, J.F.; McMullen, K.P.; Munley, M.T.; Shaw, E.G.; et al. Toxicity of Gamma Knife Radiosurgery in the Treatment of Intracranial Tumors in Patients With Collagen Vascular Diseases or Multiple Sclerosis. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, e519–e524. [Google Scholar] [CrossRef]
- Lin, D.; Lehrer, E.J.; Rosenberg, J.; Trifiletti, D.M.; Zaorsky, N.G. Toxicity after Radiotherapy in Patients with Historically Accepted Contraindications to Treatment (CONTRAD): An International Systematic Review and Meta-Analysis. Radiother. Oncol. 2019, 135, 147–152. [Google Scholar] [CrossRef]
- Jung, M.; Dimtchev, A.; Velena, A.; Dritschilo, A. Combining Radiation Therapy with Interstitial Radiation-Inducible TNF-α Expression for Locoregional Cancer Treatment. Cancer Gene Ther. 2011, 18, 189–195. [Google Scholar] [CrossRef]
- Gallagher, M.P.; Kelly, P.J.; Jardine, M.; Perkovic, V.; Cass, A.; Craig, J.C.; Eris, J.; Webster, A.C. Long-Term Cancer Risk of Immunosuppressive Regimens after Kidney Transplantation. J. Am. Soc. Nephrol. 2010, 21, 852–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food Safety Commission of Japan. Prednisolone. Food Saf. 2016, 4, 52–53. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Factor | Group | SAD Group | Control Group | p-Value |
|---|---|---|---|---|
| n | 12 | 36 | ||
| Patients | ||||
| Age (years) | <79 | 7 (58.3) | 24 (66.7) | 0.731 |
| ≥79 | 5 (41.7) | 12 (33.3) | ||
| Sex | Male | 8 (66.7) | 27 (75.0) | 0.710 |
| Female | 4 (33.3) | 9 (25.0) | ||
| KPS | ≥80 | 12 | 36 | - |
| Pathology | Adenocarcinoma | 5 | 18 | 0.835 |
| Squamous cell carcinoma | 4 | 9 | ||
| Other | 3 | 9 | ||
| T stage | T1 (T1a/T1b) | 7 | 27 | 0.294 |
| T2a | 5 | 9 | ||
| Cancer location | Peripheral | 12 | 31 | 0.312 |
| Central | 0 | 5 | ||
| Treatments | ||||
| Prescription dose | 48 Gy/4Fr | 7 | 27 | 0.093 |
| 50 Gy/4Fr | 0 | 3 | ||
| 55 Gy/4Fr | 1 | 3 | ||
| 60 Gy/10Fr | 2 | 3 | ||
| 70 Gy/10Fr | 2 | 3 |
| No. | Age | Sex | Pathology | T Stage | Location | Dose | Autoimmune Disease | Immunosuppressive Agent | Cancer Progression | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 77 | M | SCC | T2a | Right, peripheral | 60 Gy/10Fr | MPO-ANCA associated nephritis | Prednisolone | Yes | Cancer-related death |
| 2 | 72 | M | AC | T2a | Right, peripheral | 60 Gy/10Fr | Rheumatoid arthritis | Prednisolone | Yes | Cancer-related death |
| 3 | 68 | F | AC | T1a | Right, peripheral | 48 Gy/12Fr | Rheumatoid arthritis | Prednisolone, methotrexate | Yes | Cancer-related death |
| 4 | 66 | M | AC | T1a | Right, peripheral | 48 Gy/12Fr | Membranous nephropathy | Prednisolone | Yes | Death due to RP |
| 5 | 67 | M | SCC | T2a | Left, peripheral | 48 Gy/12Fr | Membranous nephropathy | Prednisolone | No | Non-cancer-related death |
| 6 | 82 | M | SCC | T1b | Right, peripheral | 48 Gy/12Fr | Rheumatoid arthritis | Prednisolone | Yes | Cancer-related death |
| 7 | 77 | M | AC | T1a | Right, peripheral | 48 Gy/12Fr | Microscopic polyangiitis | Prednisolone | Ye | Non-cancer-related death |
| 8 | 82 | M | SCC | T1a | Right, peripheral | 48 Gy/12Fr | Rheumatoid arthritis | Prednisolone | Yes | Non-cancer-related death |
| 9 | 82 | F | Other | T1a | Right, peripheral | 48 Gy/12Fr | Rheumatoid arthritis | Methotrexate | No | Non-cancer-related death |
| 10 | 80 | F | Other | T2a | Right, peripheral | 70 Gy/10Fr | Microscopic polyangiitis | Prednisolone | Yes | Cancer-related death |
| 11 | 81 | M | SCC | T2a | Right, peripheral | 55 Gy/4Fr | Membranous nephropathy | Prednisolone, ciclosporin | Yes | Alive |
| 12 | 65 | F | AC | T1a | Right, peripheral | 70 Gy/10Fr | Primary biliary cholangitis | N.A. | Yes | Cancer-related death |
| Outcomes | SAD Group | Control Group | HR (95% CI) | p-Value |
|---|---|---|---|---|
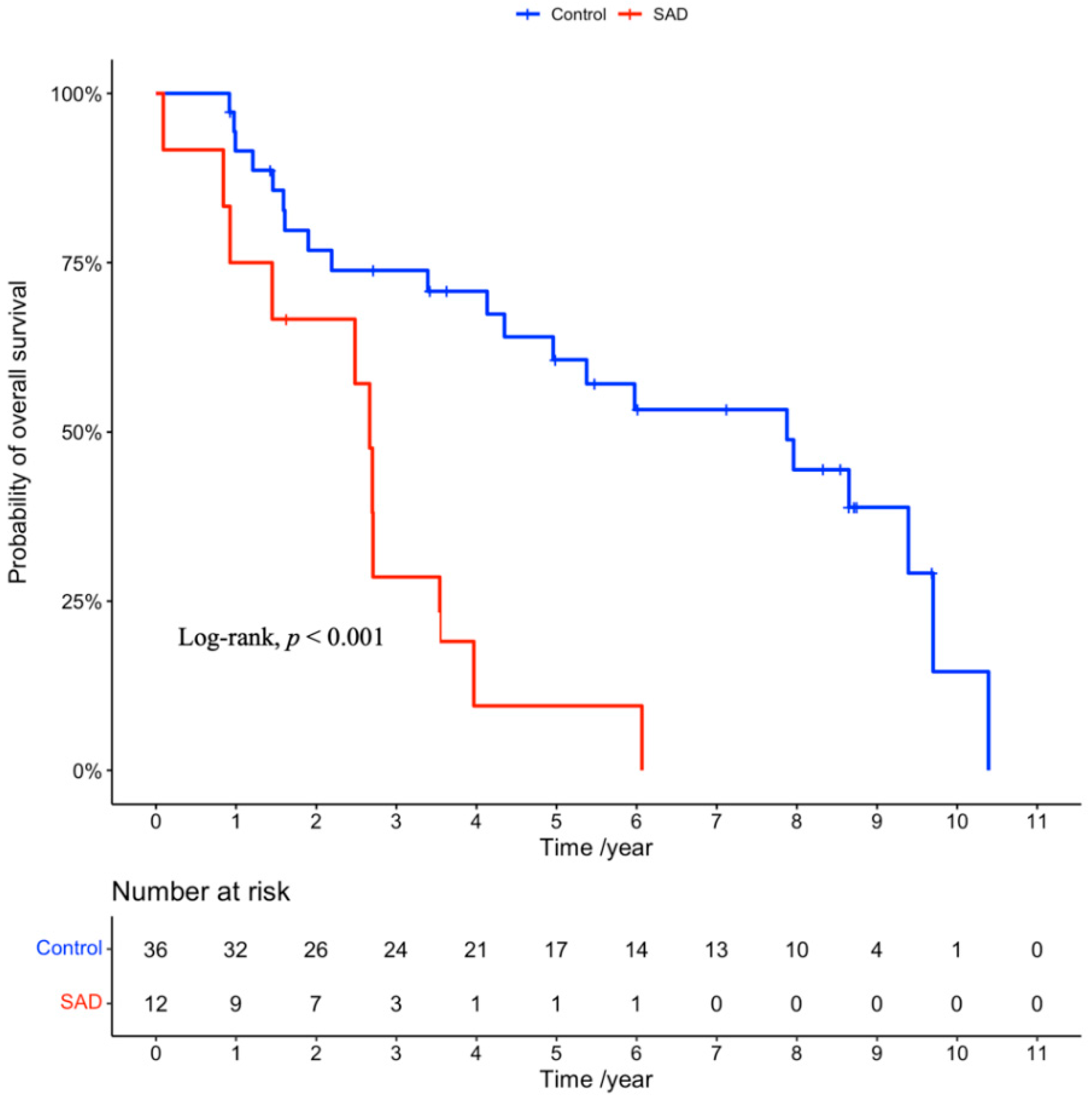
| Overall survival rate | 4.11 (1.82–9.27) | <0.001 | ||
| 3-year rate (%) | 28.6 | 73.9 | ||
| 5-year rate (%) | 9.5 | 60.7 | ||
| Median (years) | 2.7 | 7.9 | ||
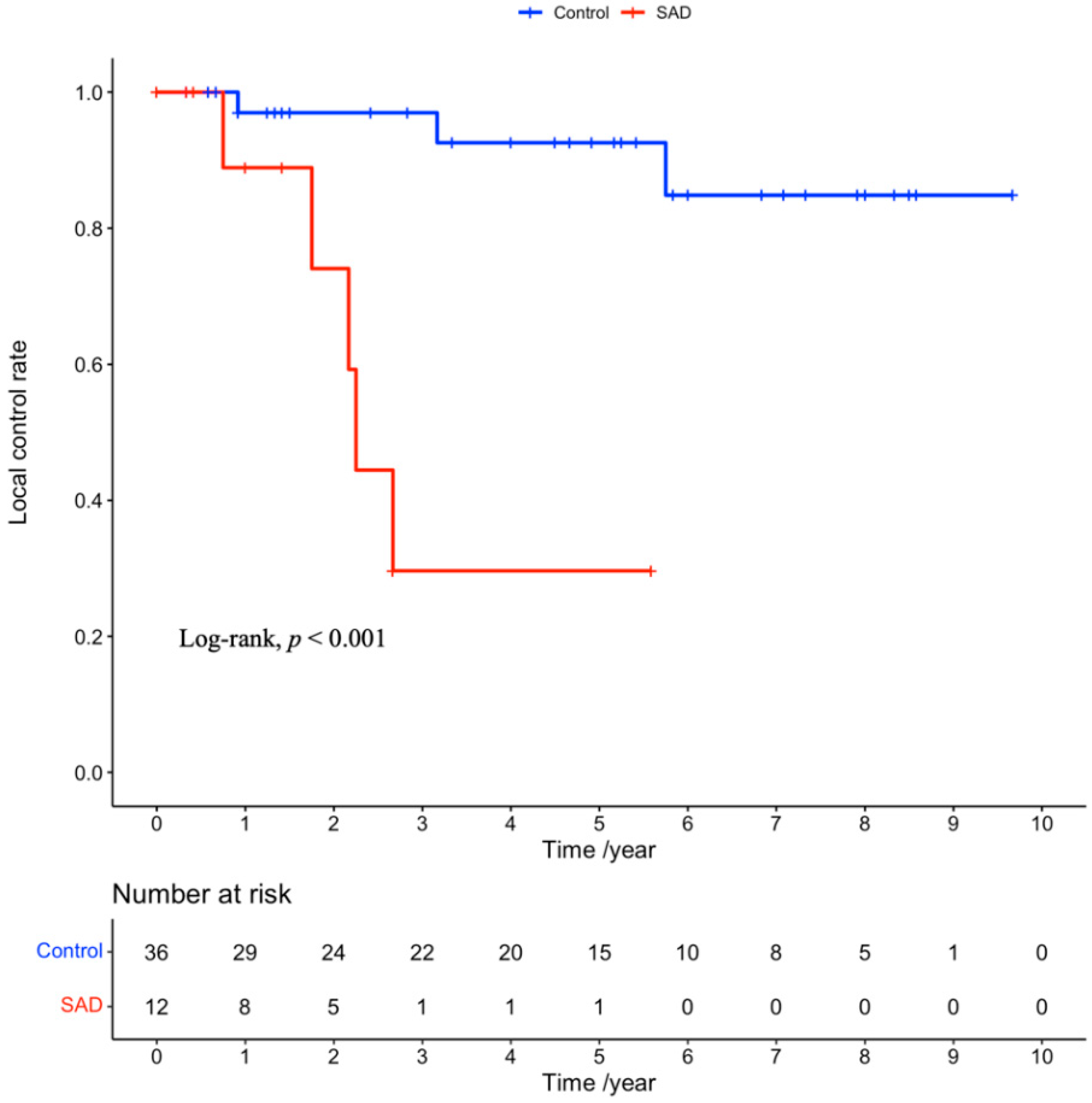
| Local recurrence rate | 15.97 (2.89–88.29) | <0.001 | ||
| 3-year rate (%) | 70.4 | 3.0 | ||
| 5-year rate (%) | 100 | 7.4 | ||
| Median (years) | 2.3 | Not estimated |
| Toxicities (%) | All Patients (n = 48) | SAD Group (n = 12) | Control Group (n = 36) | OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Acute | 0.38 (0.02–8.91) * | 0.550 | |||
| <G2 | 45 (93.8) | 12 (100) | 33 (91.7) | ||
| ≥G2 | 3 (6.2) | 0 (0) | 3 (6.2) | ||
| Late | 2.20 (0.32–15.10) | 0.422 | |||
| <G2 | 43 (89.6) | 10 (83.3) | 33 (91.7) | ||
| ≥G2 | 5 (10.4) | 2 (16.7) | 3 (8.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Nonaka, H.; Onishi, H.; Nakatani, E.; Oguri, M.; Saito, M.; Aoki, S.; Marino, K.; Komiyama, T.; Kuriyama, K.; et al. Impact of Systemic Autoimmune Diseases on Treatment Outcomes and Radiation Toxicities in Patients with Stage I Non-Small Cell Lung Cancer Receiving Stereotactic Body Radiation Therapy: A Matched Case-Control Analysis. Cancers 2022, 14, 5915. https://doi.org/10.3390/cancers14235915
Chen Z, Nonaka H, Onishi H, Nakatani E, Oguri M, Saito M, Aoki S, Marino K, Komiyama T, Kuriyama K, et al. Impact of Systemic Autoimmune Diseases on Treatment Outcomes and Radiation Toxicities in Patients with Stage I Non-Small Cell Lung Cancer Receiving Stereotactic Body Radiation Therapy: A Matched Case-Control Analysis. Cancers. 2022; 14(23):5915. https://doi.org/10.3390/cancers14235915
Chicago/Turabian StyleChen, Zhe, Hotaka Nonaka, Hiroshi Onishi, Eiji Nakatani, Mitsuhiko Oguri, Masahide Saito, Shinichi Aoki, Kan Marino, Takafumi Komiyama, Kengo Kuriyama, and et al. 2022. "Impact of Systemic Autoimmune Diseases on Treatment Outcomes and Radiation Toxicities in Patients with Stage I Non-Small Cell Lung Cancer Receiving Stereotactic Body Radiation Therapy: A Matched Case-Control Analysis" Cancers 14, no. 23: 5915. https://doi.org/10.3390/cancers14235915