
Anti-PD1 Consolidation in Patients with Hodgkin Lymphoma at High Risk of Relapse after Autologous Stem Cell Transplantation: A Multicenter Real-Life Study
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patients and Study Procedures
2.2. Efficacy and Toxicity Assessments
2.3. Statistical Methods and Analyses
3. Results
3.1. Patient Characteristics
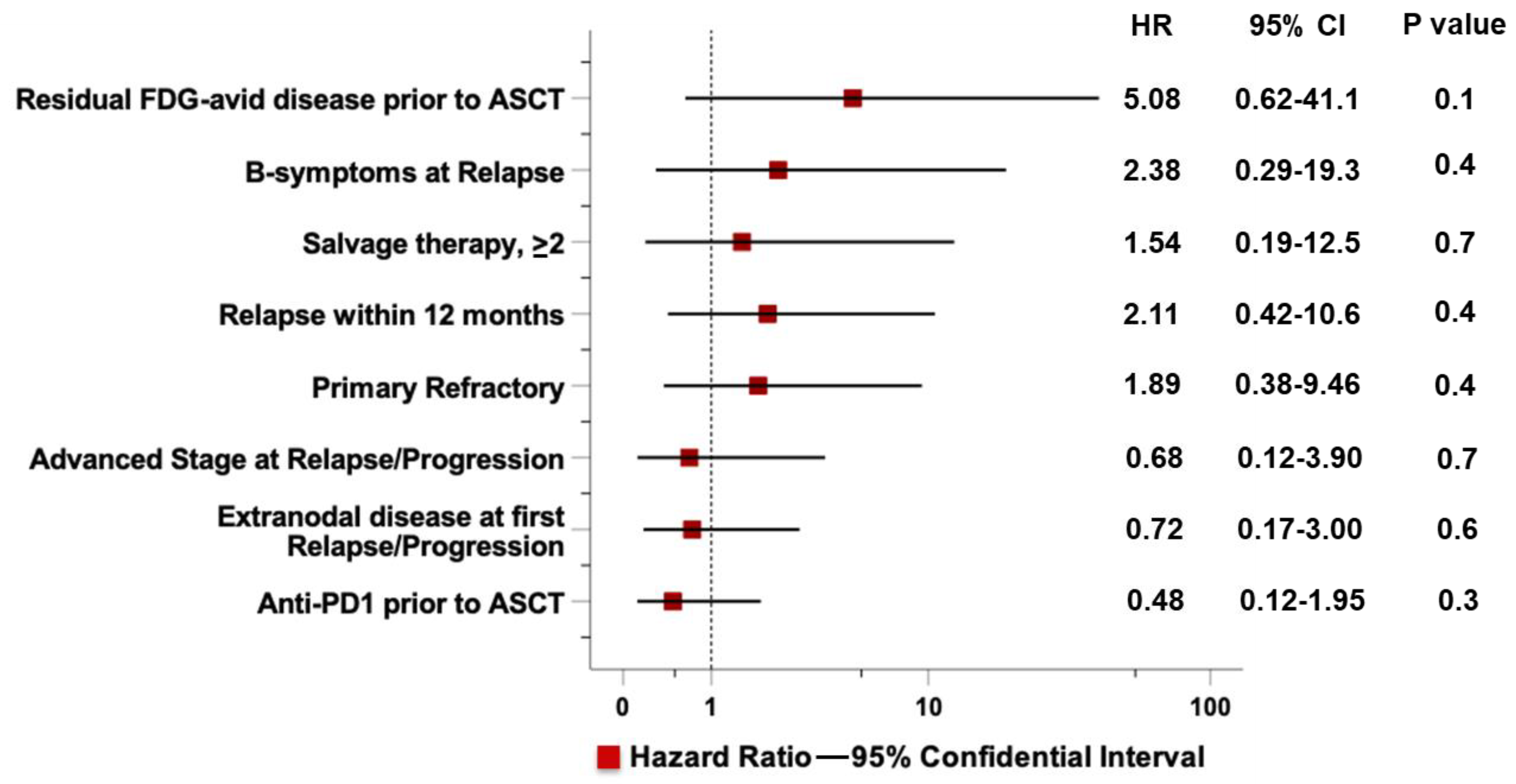
3.2. Risk factors for ASCT Failure
3.3. Pre-ASCT Exposure to BV and PD-1 Blockers
3.4. Disease Status at Transplant
3.5. Conditioning Regimens
3.6. Post-ASCT PD1-Blockade
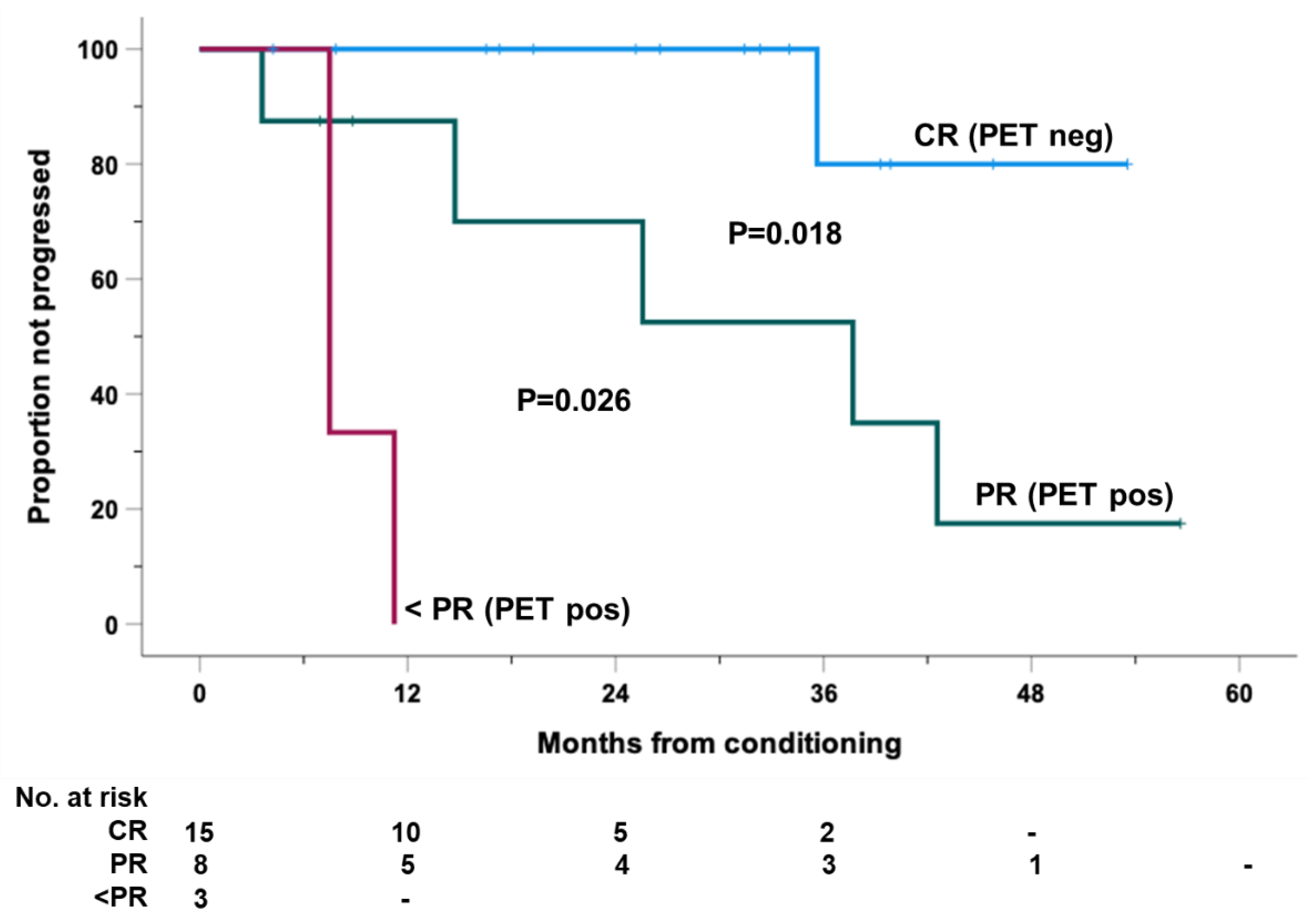
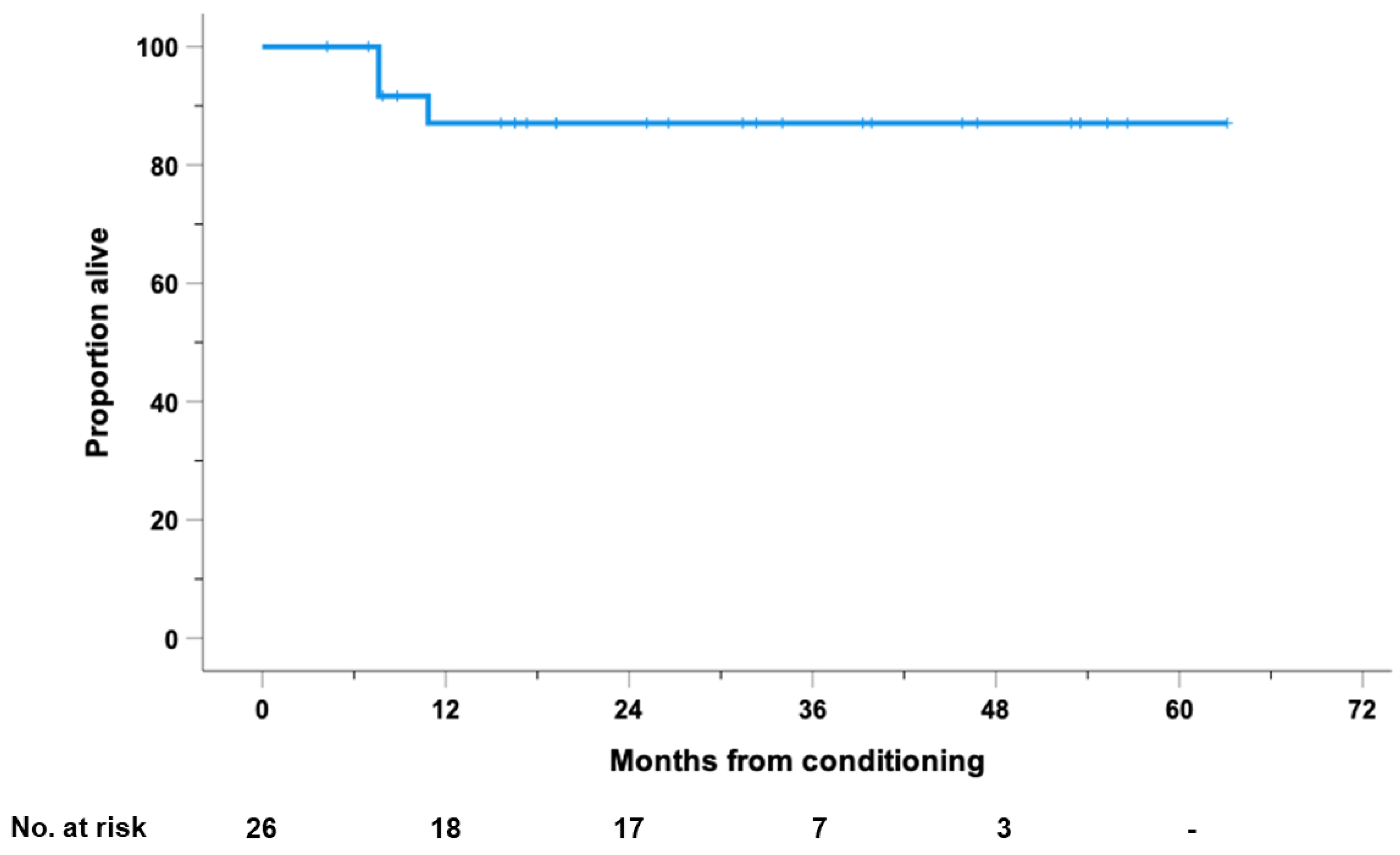
3.7. Survival Outcomes and Predictors
3.8. Safety Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoppe, R.T.; Advani, R.H.; Ai, W.Z.; Ambinder, R.F.; Armand, P.; Bello, C.M.; Benitez, C.M.; Chen, W.; Dabaja, B.; Daly, M.E.; et al. NCCN Guidelines® Insights: Hodgkin Lymphoma, Version 2.2022. J. Natl. Compr. Canc. Netw. 2022, 20, 322–334. [Google Scholar] [CrossRef] [PubMed]
- Rancea, M.; Monsef, I.; von Tresckow, B.; Engert, A.; Skoetz, N. High-dose chemotherapy followed by autologous stem cell transplantation for patients with relapsed/refractory Hodgkin lymphoma. Cochrane Database Syst. Rev. 2013, 6, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Horning, S.J.; Chao, N.J.; Negrin, R.S.; Hoppe, R.T.; Long, G.D.; Hu, W.W.; Wong, R.M.; Brown, B.W.; Blume, K.G. High-dose therapy and autologous hematopoietic progenitor cell transplantation for recurrent or refractory Hodgkin’s disease: Analysis of the Stanford University results and prognostic indices. Blood 1997, 89, 801–813. [Google Scholar] [CrossRef] [PubMed]
- Brice, P.; Bouabdallah, R.; Moreau, P.; Divine, M.; André, M.; Aoudjane, M.; Fleury, J.; Anglaret, B.; Baruchel, A.; Sensebe, L.; et al. Prognostic factors for survival after high-dose therapy and autologous stem cell transplantation for patients with relapsing Hodgkin’s disease: Analysis of 280 patients from the French registry. Société Française de Greffe de Moëlle. Bone Marrow Transplant. 1997, 20, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sureda, A.; Constans, M.; Iriondo, A.; Arranz, R.; Caballero, M.D.; Vidal, M.J.; Petit, J.; López, A.; Lahuerta, J.J.; Carreras, E.; et al. Grupo Español de Linfomas/Trasplante Autólogo de Médula Osea Cooperative Group. Prognostic factors affecting long-term outcome after stem cell transplantation in Hodgkin’s lymphoma autografted after a first relapse. Ann. Oncol. 2005, 16, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, C.H.; Matasar, M.J.; Zelenetz, A.D.; Nimer, S.D.; Gerecitano, J.; Hamlin, P.; Horwitz, S.; Moskowitz, A.J.; Noy, A.; Palomba, L.; et al. Normalization of pre-ASCT, FDG-PET imaging with second-line, non-cross-resistant, chemotherapy programs improves event-free survival in patients with Hodgkin lymphoma. Blood 2012, 119, 1665–1670. [Google Scholar] [CrossRef]
- Pinto, A.; Corradini, P.; Mussetti, A.; Zinzani, P.L. Recurrent Hodgkin lymphoma: Toward a new definition of candidates for autologous stem cell transplant in the era of positron emission tomography scan and novel agents. Leuk. Lymphoma 2015, 56, 1969–1974. [Google Scholar] [CrossRef] [PubMed]
- Shah, G.; Moskowitz, C. Transplant strategies in relapsed/refractory Hodgkins lymphoma. Blood 2018, 131, 1689–1697. [Google Scholar] [CrossRef]
- Moskowitz, C.H.; Nademanee, A.; Masszi, T.; Agura, E.; Holowiecki, J.; Abidi, M.H.; Chen, A.I.; Stiff, P.; Gianni, A.M.; Carella, A.; et al. Brentuximab vedotin as consolidation therapy after autologous stem-cell transplantation in patients with Hodgkin’s lymphoma at risk of relapse or progression (AETHERA): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2015, 385, 1853–1862. [Google Scholar] [CrossRef]
- Bröckelmann, P.J.; Müller, H.; Casasnovas, O.; Hutchings, M.; von Tresckow, B.; Jürgens, M.; McCall, S.J.; Morschhauser, F.; Fuchs, M.; Borchmann, P.; et al. Risk factors and a prognostic score for survival after autologous stem-cell transplantation for relapsed or refractory Hodgkin lymphoma. Ann. Oncol. 2017, 28, 1352–1358. [Google Scholar] [CrossRef]
- Bair, S.M.; Strelec, L.; Nagle, S.J.; Nasta, S.D.; Landsburg, D.J.; Mato, A.R.; Loren, A.W.; Schuster, S.J.; Stadtmauer, E.A.; Svoboda, J. Outcomes of patients with relapsed/refractory Hodgkin lymphoma progressing after autologous stem cell transplant in the current era of novel therapeutics: A retrospective analysis. Am. J. Hematol. 2017, 92, 879–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, H.; Jang, H.; Singh, P.; Kosti, J.; Kin, A.; Alavi, A.; Ratanatharathorn, V.; Ayash, L.; Uberti, J.; Ramchandren, R.; et al. Improved post-ASCT survival of relapsed/refractory classical Hodgkin lymphoma patients in the era of novel agents. Leuk. Lymphoma 2022, 63, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Bazarbachi, A.; Boumendil, A.; Finel, H.; Khvedelidze, I.; Romejko-Jarosinska, J.; Tanase, A.; Akhtar, S.; Ben Othman, T.; Ma’koseh, M.; Afanasyev, B.; et al. The outcome of patients with Hodgkin lymphoma and early relapse after autologous stem cell transplant has improved in recent years. Leukemia 2022, 36, 1646–1653. [Google Scholar] [CrossRef] [PubMed]
- Nieto, Y.; Gruschkus, S.; Valdez, B.C.; Jones, R.B.; Anderlini, P.; Hosing, C.; Popat, U.; Qazilbash, M.; Kebriaei, P.; Alousi, A.; et al. Improved outcomes of high-risk relapsed Hodgkin lymphoma patients after high-dose chemotherapy: A 15-year analysis. Haematologica 2022, 107, 899–908. [Google Scholar] [CrossRef]
- Satou, A.; Takahara, T.; Nakamura, S. An Update on the Pathology and Molecular Features of Hodgkin Lymphoma. Cancers 2022, 14, 2647. [Google Scholar] [CrossRef]
- Taylor, J.G.; Truelove, E.; Clear, A.; Calaminici, M.; Gribben, J.G. PDL1 shapes the classical Hodgkin lymphoma microenvironment without inducing T cell exhaustion. Haematologica 2022. [Google Scholar] [CrossRef]
- Kuruvilla, J.; Ramchandren, R.; Santoro, A.; Paszkiewicz-Kozik, E.; Gasiorowski, R.; Johnson, N.A.; Fogliatto, L.M.; Goncalves, I.; de Oliveira, J.; Buccheri, V.; et al. Pembrolizumab versus brentuximab vedotin in relapsed or refractory classical Hodgkin lymphoma (KEYNOTE-204): An interim analysis of a multicentre, randomised, open-label, phase 3 study. Lancet Oncol. 2021, 22, 512–524. [Google Scholar] [CrossRef]
- Ansell, S.M.; Bröckelmann, P.J.; von Keudell, G.; Lee, H.J.; Santoro, A.; Zinzani, P.L.; Collins, P.; Cohen, B.; De Boer, P.; Kuruvilla, J.; et al. Nivolumab for relapsed or refractory (r/r) classical hodgkin lymphoma (cHL) after autologous transplantation: 5-year overall survival from the phase 2 checkmate 205 study. Hematol. Oncol. 2021, 39 (Suppl. 2), 122–124. [Google Scholar] [CrossRef]
- Epperla, N.; Herrera, A.F. How I incorporate novel agents into the treatment of classical Hodgkin lymphoma. Blood 2021, 138, 520–530. [Google Scholar] [CrossRef]
- Moskowitz, A.J.; Schöder, H.; Yahalom, J.; McCall, S.J.; Fox, S.Y.; Gerecitano, J.; Grewal, R.; Hamlin, P.A.; Horwitz, S.; Kobos, R.; et al. PET-adapted sequential salvage therapy with brentuximab vedotin followed by augmented ifosamide, carboplatin, and etoposide for patients with relapsed and refractory Hodgkin’s lymphoma: A non-randomised, open-label, single-centre, phase 2 study. Lancet Oncol. 2015, 16, 284–292. [Google Scholar] [CrossRef]
- Mei, M.G.; Lee, H.J.; Palmer, J.M.; Chen, R.; Tsai, N.C.; Chen, L.; McBride, K.; Smith, D.L.; Melgar, I.; Song, J.Y.; et al. Response-adapted anti-PD-1-based salvage therapy for Hodgkin lymphoma with nivolumab alone or in combination with ICE. Blood 2022, 139, 3605–3616. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, A.J.; Shah, G.; Schöder, H.; Ganesan, N.; Drill, E.; Hancock, H.; Davey, T.; Perez, L.; Ryu, S.; Sohail, S.; et al. Phase II Trial of Pembrolizumab Plus Gemcitabine, Vinorelbine, and Liposomal Doxorubicin as Second-Line Therapy for Relapsed or Refractory Classical Hodgkin Lymphoma. J Clin Oncol. 2021, 39, 3109–3117. [Google Scholar] [CrossRef] [PubMed]
- Advani, R.H.; Moskowitz, A.J.; Bartlett, N.L.; Vose, J.M.; Ramchandren, R.; Feldman, T.A.; LaCasce, A.S.; Christian, B.A.; Ansell, S.M.; Moskowitz, C.H.; et al. Brentuximab vedotin in combination with nivolumab in relapsed or refractory Hodgkin lymphoma: 3-year study results. Blood 2021, 138, 427–438. [Google Scholar] [CrossRef]
- Moskowitz, C.H.; Walewski, J.; Nademanee, A.; Masszi, T.; Agura, E.; Holowiecki, J.; Abidi, M.H.; Chen, A.I.; Stiff, P.; Viviani, S.; et al. Five-year PFS from the AETHERA trial of brentuximab vedotin for Hodgkin lymphoma at high risk of progression or relapse. Blood 2018, 132, 2639–2642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armand, P.; Chen, Y.B.; Redd, R.A.; Joyce, R.M.; Bsat, J.; Jeter, E.; Merryman, R.W.; Coleman, K.C.; Dahi, P.B.; Nieto, Y.; et al. PD-1 blockade with pembrolizumab for classical Hodgkin lymphoma after autologous stem cell transplantation. Blood 2019, 134, 22–29. [Google Scholar] [CrossRef]
- Merryman, R.W.; Redd, R.; Jeter, E.; Wong, J.L.; McHugh, K.; Reynolds, C.; Nazzaro, M.; Varden, A.; Brown, J.R.; Crombie, J.L.; et al. Immune Reconstitution following High-Dose Chemotherapy and Autologous Stem Cell Transplantation with or without Pembrolizumab Maintenance Therapy in Patients with Lymphoma. Transpl. Cell Ther. 2022, 28, 32.e1–32.e10. [Google Scholar] [CrossRef]
- Herrera, A.F.; Chen, L.; Nieto, Y.; Holmberg, L.; Johnston, P.B.; Mei, M.; Popplewell, L.; Armenian, S.H.H.; Cao, T.; Farol, L.; et al. Consolidation with nivolumab and brentuximab vedotin after autologous hematopoietic cell transplantation in patients with high-risk Hodgkin lymphoma. Blood 2020, 136 (Suppl. 1), 19. [Google Scholar] [CrossRef]
- Bachier, C.; Schade, H.; Zoghi, B.; Ramakrishnan, A.; Shah, N.N. A Phase II Single Arm Study of Nivolumab As Maintenance Therapy after Autologous Stem Cell Transplantation in Patients with Hodgkin Lymphoma at Risk of Relapse or Progression. Blood 2021, 138, 2455–2456. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- De Filippi, R.; Morabito, F.; Santoro, A.; Tripepi, G.; D’Alò, F.; Rigacci, L.; Ricci, F.; Morelli, E.; Zinzani, P.L.; Pinto, A. Body mass index is not associated with survival outcomes and immune-related adverse events in patients with Hodgkin lymphoma treated with the immune checkpoint inhibitor nivolumab. J. Transl. Med. 2021, 19, 489. [Google Scholar] [CrossRef]
- Haanen, J.; Carbonnel, F.; Robert, C.; Kerr, K.M.; Peters, S.; Larkin, J.; Jordan, K. ESMO Guidelines Committee. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28 (Suppl. 4), iv119–iv142. [Google Scholar] [CrossRef] [PubMed]
- Calabretta, E.; Guidetti, A.; Ricci, F.; Di Trani, M.; Monfrini, C.; Magagnoli, M.; Bramanti, S.; Maspero, D.; Morello, L.; Merli, M.; et al. Chemotherapy after PD-1 inhibitors in relapsed/refractory Hodgkin lymphoma: Outcomes and clonal evolution dynamics. Br. J. Haematol. 2022, 198, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Casadei, B.; Argnani, L.; Morigi, A.; Lolli, G.; Broccoli, A.; Pellegrini, C.; Nanni, L.; Stefoni, V.; Coppola, P.E.; Carella, M.; et al. Effectiveness of chemotherapy after anti-PD-1 blockade failure for relapsed and refractory Hodgkin lymphoma. Cancer Med. 2020, 9, 7830–7836. [Google Scholar] [CrossRef] [PubMed]
- Carreau, N.A.; Pail, O.; Armand, P.; Merryman, R.; Advani, R.H.; Spinner, M.A.; Herrera, A.; Chen, R.; Tomassetti, S.; Ramchandren, R.; et al. Checkpoint blockade treatment may sensitize Hodgkin lymphoma to subsequent therapy. Oncologist 2020, 25, 878–885. [Google Scholar] [CrossRef]
- Merryman, R.W.; Redd, R.A.; Nishihori, T.; Chavez, J.; Nieto, Y.; Darrah, J.M.; Rao, U.; Byrne, M.T.; Bond, D.A.; Maddocks, K.J.; et al. Autologous stem cell transplantation after anti-PD-1 therapy for multiply relapsed or refractory Hodgkin lymphoma. Blood Adv. 2021, 5, 1648–1659. [Google Scholar] [CrossRef]
- Couey, M.A.; Bell, R.B.; Patel, A.A.; Romba, M.C.; Crittenden, M.R.; Curti, B.D.; Urba, W.J.; Leidner, R.S. Delayed immune-related events (DIRE) after discontinuation of immunotherapy: Diagnostic hazard of autoimmunity at a distance. J. Immunother. Cancer 2019, 7, 165. [Google Scholar] [CrossRef] [Green Version]
- Brahmer, J.R.; Drake, C.G.; Wollner, I.; Powderly, J.D.; Picus, J.; Sharfman, W.H.; Stankevich, E.; Pons, A.; Salay, T.M.; McMiller, T.L.; et al. Phase I study of single-agent anti-programmed Death-1 (MDX-1106) in refractory solid tumors: Safety, clinical activity, pharmacodynamics, and immunologic correlates. J. Clin. Oncol. 2010, 28, 3167–3175. [Google Scholar] [CrossRef]
- Manson, G.; Mear, J.B.; Herbaux, C.; Schiano, J.M.; Casasnovas, O.; Stamatoullas, A.; Deau, B.; Schmitt, A.; Garnier, G.; Regny, C.; et al. Long-term efficacy of anti-PD1 therapy in Hodgkin lymphoma with and without allogenic stem cell transplantation. Eur. J. Cancer 2019, 115, 47–56. [Google Scholar] [CrossRef]
- Manson, G.; Brice, P.; Herbaux, C.; Silva, M.G.; Bouabdallah, K.; Deau, B.; Bouteloup, J.; Schiano, J.M.; Nicolas-Virelizier, E.; Maerevoet, M.; et al. Risk of relapse after anti-PD1 discontinuation in patients with Hodgkin lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1144–1153. [Google Scholar] [CrossRef]
- Roemer, M.; Redd, R.A.; Cader, F.Z.; Pak, C.J.; Abdelrahman, S.; Ouyang, J.; Sasse, S.; Younes, A.; Fanale, M.; Santoro, A.; et al. Major histocompatibility complex class II and programmed death ligand 1 expression predict outcome after programmed death 1 blockade in classic Hodgkin Lymphoma. J. Clin. Oncol. 2018, 36, 942–950. [Google Scholar] [CrossRef]
- Song, Y.; Gao, Q.; Zhang, H.; Fan, L.; Zhou, J.; Zou, D.; Li, W.; Yang, H.; Liu, T.; Wang, Q.; et al. Tislelizumab for Relapsed/Refractory Classical Hodgkin Lymphoma: 3-Year Follow-up and Correlative Biomarker Analysis. Clin. Cancer Res. 2022, 28, 1147–1156. [Google Scholar] [CrossRef] [PubMed]
- Mohty, R.; Dulery, R.; Bazarbachi, A.H.; Savani, M.; Hamed, R.A.; Bazarbachi, A.; Mohty, M. Latest advances in the management of classical Hodgkin lymphoma: The era of novel therapies. Blood Cancer J. 2021, 11, 126. [Google Scholar] [CrossRef] [PubMed]
- Ansell, S.M.; Radford, J.; Connors, J.M.; Długosz-Danecka, M.; Kim, W.S.; Gallamini, A.; Ramchandren, R.; Friedberg, J.W.; Advani, R.; Hutchings, M.; et al. Overall Survival with Brentuximab Vedotin in Stage III or IV Hodgkin’s Lymphoma. N. Engl. J. Med. 2022, 387, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Samara, Y.; Mei, M. Autologous Stem Cell Transplantation in Hodgkin Lymphoma-Latest Advances in the Era of Novel Therapies. Cancers 2022, 14, 1738. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N° (%) |
|---|---|
| (N = 26) | |
| Age at transplant, (years) | |
| Median (range) | 30 (19–58) |
| Gender | |
| Male | 15 (58) |
| Female | 11 (42) |
| Frontline therapy | |
| ABVD | 25 (96) |
| Stanford V | 1 (4) |
| Consolidation radiotherapy | 10 (38) |
| Disease status after frontline therapy | |
| Primary refractory | 18 (69) |
| Relapse <12 months | 4 (15) |
| Failure after interim PET-driven escalation (BEACOPP esc) | 5 (19) |
| Extranodal disease at relapse | 17 (65) |
| B symptoms at relapse | 17 (65) |
| Advanced stage at relapse (stage IVA-B, IIIA-B) | 17 (65) |
| Number of salvage therapy lines | |
| Median (range) | 4 (1–5) |
| 1 line | 2 (8) |
| 2 lines | 5 (19) |
| >2 lines | 19 (73) |
| Exposure to BV pre-ASCT | 25 (96) |
| BV as single agent | 21 (84) |
| BV and Bendamustine | 4 (16) |
| Median number of BV cycles received (range) | 4 (2–8) |
| Exposure to anti-PD1 pre-ASCT | 16 (61) |
| Median number of anti-PD1 cycles received | 11 (4–32) |
| Exposure to BV and anti-PD1 pre-ASCT | 15 (58) |
| Best response to last salvage therapy pre-ASCT | |
| Not exposed to anti-PD1 | 10 (39) |
| CR | 1 (10) |
| PR | 7 (70) |
| SD/PD | 2 (20) |
| Anti-PD1 as last salvage line before ASCT | 16 (61) |
| CR | 9 (56) |
| PR | 7 (44) |
| SD/PD | --- |
| PET-CT status pre-ASCT | |
| Negative (DS 1–3) | 10 (38) |
| Positive (DS 4–5) | 16 (62) |
| Anti-PD1 post-ASCT Median number of days from ASCT to anti-PD1 initiation Median number of anti-PD1 cycles received Causes of anti-PD1 discontinuation (post-ASCT) | 44 (10–129) 13 (6–30) |
| CR (stop & follow-up) | 18 (69) |
| Toxicity | 0 |
| Disease progression/recurrence/stability | 5 (19) |
| Bridging to allo-SCT | 1 (4) |
| No discontinuation | 2 (8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Filippi, R.; Marcacci, G.; Derenzini, E.; Musso, M.; Donnarumma, D.; Morelli, E.; Patti, C.; Maraglino, A.M.E.; Scalone, R.; Simeone, L.; et al. Anti-PD1 Consolidation in Patients with Hodgkin Lymphoma at High Risk of Relapse after Autologous Stem Cell Transplantation: A Multicenter Real-Life Study. Cancers 2022, 14, 5846. https://doi.org/10.3390/cancers14235846
De Filippi R, Marcacci G, Derenzini E, Musso M, Donnarumma D, Morelli E, Patti C, Maraglino AME, Scalone R, Simeone L, et al. Anti-PD1 Consolidation in Patients with Hodgkin Lymphoma at High Risk of Relapse after Autologous Stem Cell Transplantation: A Multicenter Real-Life Study. Cancers. 2022; 14(23):5846. https://doi.org/10.3390/cancers14235846
Chicago/Turabian StyleDe Filippi, Rosaria, Gianpaolo Marcacci, Enrico Derenzini, Maurizio Musso, Daniela Donnarumma, Emanuela Morelli, Caterina Patti, Alessio Maria Edoardo Maraglino, Renato Scalone, Luigia Simeone, and et al. 2022. "Anti-PD1 Consolidation in Patients with Hodgkin Lymphoma at High Risk of Relapse after Autologous Stem Cell Transplantation: A Multicenter Real-Life Study" Cancers 14, no. 23: 5846. https://doi.org/10.3390/cancers14235846