
Tumors Involving the Infratemporal Fossa: A Systematic Review of Clinical Characteristics and Treatment Outcomes
 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Data Synthesis and Quality Assessment
2.5. Statistical Analysis
3. Results
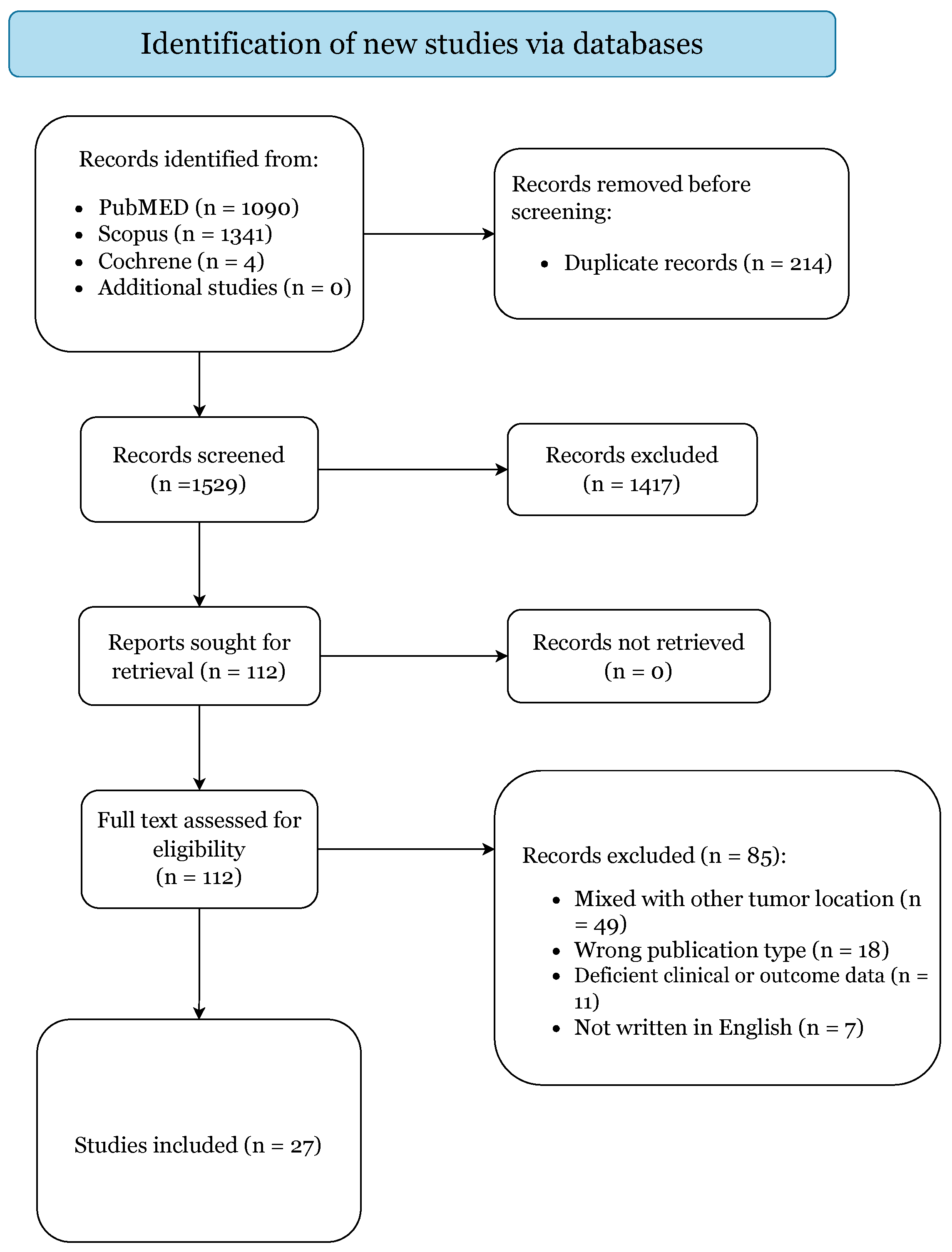
3.1. Study Selection
3.2. Demographics and Clinical Features
3.3. Management Paradigm and Postoperative Complications
3.4. Patient Clinical and Survival Outcomes
4. Discussion
4.1. Patient Clinical Characteristics
4.2. Management and Survival Outcomes
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Zhou, B.; Huang, Q.; Shen, P.-H.; Cui, S.-J.; Wang, C.-S.; Li, Y.-C.; Yu, Z.-K.; Chen, X.-H.; Ye, T. The Intranasal Endoscopic Removal of Schwannoma of the Pterygopalatine and Infratemporal Fossae via the Prelacrimal Recess Approach. J. Neurosurg. 2016, 124, 1068–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, M.; Shojima, M.; Kondo, K.; Hasegawa, H.; Hanakita, S.; Ito, A.; Kin, T.; Saito, N. Endoscopic Endonasal Craniofacial Surgery for Recurrent Skull Base Meningiomas Involving the Pterygopalatine Fossa, the Infratemporal Fossa, the Orbit, and the Paranasal Sinus. World Neurosurg. 2018, 112, E302–E312. [Google Scholar] [CrossRef] [PubMed]
- Nomura, F.; Kishimoto, S. Synovial Sarcoma of the Temporomandibular Joint and Infratemporal Fossa. Auris Nasus Larynx 2014, 41, 572–575. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.V.; Olsen, K.D.; McCaffrey, T.V. Parapharyngeal Space Neoplasms. Head Neck 1995, 17, 124–130. [Google Scholar] [CrossRef]
- Das, U.C.; Stephen, A.; Ross, A.; Chary, G.; Chand, A.K. Facial Translocation Approach to Infratemporal Fossa and Cranial Base in Extensive Angiofibroma: A Review of 7 Cases. Indian J. Otolaryngol. Head Neck Surg. 2005, 57, 17. [Google Scholar] [CrossRef]
- Murayama, S.; Suzuki, I.; Nagase, M.; Shingaki, S.; Kawasaki, T.; Nakajima, T.; Fukushima, M.; Ishiki, T. Chondrosarcoma of the Mandible. Report of Case and a Survey of 23 Cases in the Japanese Literature. J. Craniomaxillofac. Surg. 1988, 16, 287–292. [Google Scholar] [CrossRef]
- Shapshay, S.M.; Elber, E.; Strong, M.S. Occult Tumors of the Infratemporal Fossa: Report of Seven Cases Appearing as Preauricular Facial Pain. Arch. Otolaryngol. 1976, 102, 535–538. [Google Scholar] [CrossRef]
- Stippler, M.; Gardner, P.A.; Snyderman, C.H.; Carrau, R.L.; Prevedello, D.M.; Kassam, A.B. Endoscopic Endonasal Approach for Clival Chordomas. Neurosurgery 2009, 64, 268. [Google Scholar] [CrossRef]
- Wang, E.W.; Zanation, A.M.; Gardner, P.A.; Schwartz, T.H.; Eloy, J.A.; Adappa, N.D.; Bettag, M.; Bleier, B.S.; Cappabianca, P.; Carrau, R.L.; et al. ICAR: Endoscopic Skull-Base Surgery. Int. Forum Allergy Rhinol. 2019, 9, S145–S365. [Google Scholar] [CrossRef]
- Kassam, A.B.; Gardner, P.; Snyderman, C.; Mintz, A.; Carrau, R. Expanded Endonasal Approach: Fully Endoscopic, Completely Transnasal Approach to the Middle Third of the Clivus, Petrous Bone, Middle Cranial Fossa, and Infratemporal Fossa. Neurosurg. Focus 2005, 19, E6. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Hodgkinson, M. The Oxford 2011 Levels of Evidence. Oxford Centre Evidence-Based Medicine. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 15 March 2009).
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological Quality of Case Series Studies: An Introduction to the JBI Critical Appraisal Tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef]
- Wenig, B.M.; Abbondanzo, S.L.; Childers, E.L.; Kapadia, S.B.; Heffner, D.R. Extranodal Sinus Histiocytosis with Massive Lymphadenopathy (Rosai-Dorfman Disease) of the Head and Neck. Hum. Pathol. 1993, 24, 483–492. [Google Scholar] [CrossRef]
- Chung, J.W.; Ahn, J.H.; Kim, J.H.; Nam, S.Y.; Kim, C.-J.; Lee, K.-S. Facial Nerve Schwannomas: Different Manifestations and Outcomes. Surg. Neurol. 2004, 62, 245–252; discussion 452. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wan, S.; Abdelrehem, A.; Chen, M.; Yang, C. Benign Temporomandibular Joint Tumours with Extension to Infratemporal Fossa and Skull Base: Condyle Preserving Approach. Int. J. Oral Maxillofac. Surg. 2020, 49, 867–873. [Google Scholar] [CrossRef]
- Zhang, Q.; Feng, K.; Ge, C.; Hongchuan, G.; Mingchu, L. Endoscopic Endonasal Management of Trigeminal Schwannomas Extending into the Infratemporal Fossa. J. Clin. Neurosci. 2012, 19, 862–865. [Google Scholar] [CrossRef]
- Colmenero, C.; Perez Alvarez, M.; Alonso, A. Adenoid Cystic Carcinoma of the Infraspheno-Temporal Fossa. Latero-Facial Resection Combined with Multiple Osteotomies. J. Craniomaxillofac. Surg. 1991, 19, 212–216. [Google Scholar] [CrossRef]
- Galioto, S.; Valentini, V.; Fatone, F.M.G.; Rabagliati, M.; Autelitano, L.; Iannetti, G. Solitary Fibrous Tumours of the Infratemporal Fossa. Two Case Reports. J. Craniomaxillofac. Surg. 2006, 34, 494–501. [Google Scholar] [CrossRef]
- Chatni, S.S.; Sharan, R.; Patel, D.; Iyer, S.; Tiwari, R.M.; Kuriakose, M.A. Transmandibular Approach for Excision of Maxillary Sinus Tumors Extending to Pterygopalatine and Infratemporal Fossae. Oral Oncol. 2009, 45, 720–726. [Google Scholar] [CrossRef]
- Kakudo, N.; Kusumoto, K.; Takemoto, T.; Tanaka, Y.; Kurokawa, I.; Ogawa, Y. Dumbbell-Formed Lipomas under the Zygomatic Arch. J. Plast. Reconstr. Aesthet. Surg. 2008, 61, 107–110. [Google Scholar] [CrossRef]
- Morace, R.; Marongiu, A.; Vangelista, T.; Galasso, V.; Colonnese, C.; Giangaspero, F.; Innocenzi, G.; Esposito, V.; Cantore, G. Intracranial Capillary Hemangioma: A Description of Four Cases. World Neurosurg. 2012, 78, 191.E15–191.E21. [Google Scholar] [CrossRef]
- Wang, X.; Bao, Y.; Chen, G.; Guo, H.; Li, M.; Liang, J.; Bai, X.; Ling, F. Trigeminal Schwannomas in Middle Fossa Could Breach into Subdural Space: Report of 4 Cases and Review of Literature. World Neurosurg. 2019, 127, e534–e541. [Google Scholar] [CrossRef] [PubMed]
- Kekatpure, V.D.; Hedne, N.; Chavre, S.; Pillai, V.; Trivedi, N.; Kuriakose, M.A. Versatility of Adipofascial Anterolateral Thigh Flap for Reconstruction of Maxillary Defects with Infratemporal Fossa Extension. Craniomaxillofac. Trauma Reconstr. 2014, 7, 213–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnamurthy, S.; Holmes, B.; Powers, S.K. Schwannomas Limited to the Infratemporal Fossa: Report of Two Cases. J. Neuro-Oncol. 1998, 36, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Sun, X.; Hu, L.; Wang, J.; Wang, D.; Pasic, T.R.; Kern, R.C. Endoscopic Surgical Treatment of Neurogenic Tumor in Pterygopalatine and Infratemporal Fossae via Extended Medial Maxillectomy. Acta Otolaryngol. 2011, 131, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Deneuve, S.; Teissier, N.; Jouffroy, T.; Helfre, S.; Boissonnet, H.; Freneaux, P.; Peuchmaur, M.; Brisse, H.; Van Den Abbeele, T.; Orbach, D. Skull Base Surgery for Pediatric Parameningeal Sarcomas. Head Neck 2012, 34, 1057–1063. [Google Scholar] [CrossRef]
- Sichel, J.Y.; Monteil, J.P.; Elidan, J. Skull Base Chondroma of Extracranial Origin. Head Neck 1994, 16, 578–581. [Google Scholar] [CrossRef]
- Haidar, H.; Deveze, A.; Lavieille, J.P. Mini-Invasive Surgery of Infratemporal Fossa Schwannomas. J. Laryngol. Otol. 2015, 129, 187–193. [Google Scholar] [CrossRef]
- Dare, A.O.; Gibbons, K.J.; Proulx, G.M.; Fenstermaker, R.A. Resection Followed by Radiosurgery for Advanced Juvenile Nasopharyngeal Angiofibroma: Report of Two Cases. Neurosurgery 2003, 52, 1207–1211; discussion 1211. [Google Scholar]
- Folk, G.S.; Williams, S.B.; Foss, R.B.; Fanburg-Smith, J.C. Oral and Maxillofacial Sclerosing Epithelioid Fibrosarcoma: Report of Five Cases. Head Neck Pathol. 2007, 1, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Al-Daraji, W.; Lasota, J.; Foss, R.; Miettinen, M. Synovial Sarcoma Involving the Head: Analysis of 36 Cases with Predilection to the Parotid and Temporal Regions. Am. J. Surg. Pathol. 2009, 33, 1494–1503. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.T.; Suh, J.D.; Carrau, R.L.; Chu, M.W.; Chiu, A.G. Endoscopic Denker’s Approach for Resection of Lesions Involving the Anteroinferior Maxillary Sinus and Infratemporal Fossa. Laryngoscope 2017, 127, 556–560. [Google Scholar] [CrossRef]
- Buchanan, G. Two Rare Tumours Involving the Infratemporal Fossa: Alveolar Soft Part Sarcoma and Haemangiopericytoma. J. Laryngol. Otol. 1975, 89, 375–389. [Google Scholar] [CrossRef] [PubMed]
- Pieper, D.R.; Al-Mefty, O. Management of Intracranial Meningiomas Secondarily Involving the Infratemporal Fossa: Radiographic Characteristics, Pattern of Tumor Invasion, and Surgical Implications. Neurosurgery 1999, 45, 231–237. [Google Scholar] [CrossRef]
- Liu, D.Y.; Yuan, X.R.; Liu, Q.; Jiang, X.J.; Jiang, W.X.; Peng, Z.F.; Ding, X.P.; Luo, D.W.; Yuan, J. Large Medial Sphenoid Wing Meningiomas: Long-Term Outcome and Correlation with Tumor Size after Microsurgical Treatment in 127 Consecutive Cases. Turk. Neurosurg. 2012, 22, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, J.P.; Starke, R.M.; Kano, H.; Kaufmann, A.M.; Mathieu, D.; Zeiler, F.A.; West, M.; Chao, S.T.; Varma, G.; Chiang, V.L.S.; et al. Gamma Knife Radiosurgery for Sellar and Parasellar Meningiomas: A Multicenter Study. J. Neurosurg. 2015, 127, A1562–A1563, WE-Science Citation Index Expanded. [Google Scholar] [CrossRef]
- Mühl-Benninghaus, R.; Neumann, J. Malignant tumors of the skull base. Radiologe 2019, 59, 1064–1070. [Google Scholar] [CrossRef]
- Taylor, R.J.; Patel, M.R.; Wheless, S.A.; McKinney, K.A.; Stadler, M.E.; Sasaki-Adams, D.; Ewend, M.G.; Germanwala, A.V.; Zanation, A.M. Endoscopic Endonasal Approaches to Infratemporal Fossa Tumors: A Classification System and Case Series. Laryngoscope 2014, 124, 2443–2450. [Google Scholar] [CrossRef]
- Theodosopoulos, P.V.; Guthikonda, B.; Brescia, A.; Keller, J.T.; Zimmer, L.A. Endoscopic Approach to the Infratemporal Fossa: Anatomic Study. Neurosurgery 2010, 66, 196–202. [Google Scholar] [CrossRef]
- Longstreth, W.T.J.; Dennis, L.K.; McGuire, V.M.; Drangsholt, M.T.; Koepsell, T.D. Epidemiology of Intracranial Meningioma. Cancer 1993, 72, 639–648. [Google Scholar] [CrossRef]
- Wiemels, J.; Wrensch, M.; Claus, E.B. Epidemiology and Etiology of Meningioma. J. Neurooncol. 2010, 99, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, O.; Iyer, A.K.; Kano, H.; Talbott, E.O.; Lunsford, L.D. Epidemiology and Environmental Risk Factors Associated with Vestibular Schwannoma. World Neurosurg. 2015, 84, 1674–1680. [Google Scholar] [CrossRef] [PubMed]
- Cherekaev, V.A.; Korshunov, A.G.; Kornienko, V.N.; Bekiashev, A.K.; Belov, A.I.; Vinokurov, A.G.; Tsikarishvili, V.M.; Kadasheva, A.B.; Smirnov, R.A. Skull base meningiomas spreading into the infratemporal fossa: Clinical picture, diagnosis, and treatment policy. Zhurnal Vopr. Neirokhirurgii Im. NN Burd. 2004, 4, 6–11. [Google Scholar]
- Bouaziz, A.; Chabardes, E.; Laccourreye, O.; Menard, M.; Brasnu, D.; Laccourreye, H. Extension to the infratemporal fossa of malignant tumors of the face. Ann. Otolaryngol. Chir. Cervicofac. 1991, 108, 113–118. [Google Scholar]
- Paluzzi, A.; Gardner, P.; Fernandez-Miranda, J.C.; Snyderman, C. The Expanding Role of Endoscopic Skull Base Surgery. Br. J. Neurosurg. 2012, 26, 649–661. [Google Scholar] [CrossRef]
- Raza, S.M.; Amine, M.A.; Anand, V.; Schwartz, T.H. Endoscopic Endonasal Resection of Trigeminal Schwannomas. Neurosurg. Clin. N. Am. 2015, 26, 473–479. [Google Scholar] [CrossRef]
- Oakley, G.M.; Harvey, R.J. Endoscopic Resection of Pterygopalatine Fossa and Infratemporal Fossa Malignancies. Otolaryngol. Clin. N. Am. 2017, 50, 301–313. [Google Scholar] [CrossRef]
- Borg, A.; Kirkman, M.A.; Choi, D. Endoscopic Endonasal Anterior Skull Base Surgery: A Systematic Review of Complications During the Past 65 Years. World Neurosurg. 2016, 95, 383–391. [Google Scholar] [CrossRef]
- Gaillard, S. The Transition from Microscopic to Endoscopic Transsphenoidal Surgery in High-Caseload Neurosurgical Centers: The Experience of Foch Hospital. World Neurosurg. 2014, 82, S116–S120. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, Z.; Guo, H.; Yan, B.; Wang, Z.; Zhao, H.; Sahyouni, R.; Kuan, E.C. Direct Transcavernous Sinus Approach for Endoscopic Endonasal Resection of Intracavernous Sinus Tumors. World Neurosurg. 2019, 128, e478–e487. [Google Scholar] [CrossRef]
- Lucas, J.W.; Zada, G. Endoscopic Endonasal and Keyhole Surgery for the Management of Skull Base Meningiomas. Neurosurg. Clin. N. Am. 2016, 27, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Bander, E.D.; Singh, H.; Ogilvie, C.B.; Cusic, R.C.; Pisapia, D.J.; Tsiouris, A.J.; Anand, V.K.; Schwartz, T.H. Endoscopic Endonasal versus Transcranial Approach to Tuberculum Sellae and Planum Sphenoidale Meningiomas in a Similar Cohort of Patients. J. Neurosurg. 2018, 128, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, A.E.; Harrison Snyder, M.; Rabinovich, E.P.; Malkawi, D.; Chakravarti, S.; Wei, O.; Cheshire, M.; Carrie Price, M.L.S.; Khalafallah, A.M.; Rowan, N.R.; et al. Comparison and Evolution of Transcranial versus Endoscopic Endonasal Approaches for Suprasellar Meningiomas: A Systematic Review. J. Clin. Neurosci. 2022, 99, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Van Ngo, C.; Nguyen, H.; Aklinski, J.; Minh, L.H.N.; Le, H.H.; Nguyen, K.N.; Tran, U.H.; Le, N.; Huynh Le, P.; Tran, T.M. Reconstruction of Large Anterior Skull Base Defects After Resection of Sinonasal Tumors With Intracranial Extension by Using Pedicled Double Flap Techniques. J. Craniofac. Surg. 2022. [Google Scholar] [CrossRef]
- Qadeer, N.; Mehrara, B.J.; Cohen, M.; Tabar, V.; Shahzad, F. Endoscopic Endonasal Repair of Recurrent Cerebrospinal Fluid Leak With Adipofascial Anterolateral Thigh Free Flap: Case Report and Review of Literature. Eplasty 2022, 22, e32. [Google Scholar]
- Smith, P.G.; Grubb, R.L.; Kletzker, G.R.; Leonetti, J.P. Combined Pterional-Anterolateral Approaches to Cranial Base Tumors. Otolaryngol. Head Neck Surg. 1990, 103, 357–363. [Google Scholar] [CrossRef]
- Sekhar, L.N.; Schramm, V.L.J.; Jones, N.F.; Yonas, H.; Horton, J.; Latchaw, R.E.; Curtin, H. Operative Exposure and Management of the Petrous and Upper Cervical Internal Carotid Artery. Neurosurgery 1986, 19, 967–982. [Google Scholar] [CrossRef]
- Tysome, J.R.; Macfarlane, R.; Durie-Gair, J.; Donnelly, N.; Mannion, R.; Knight, R.; Harris, F.; Vanat, Z.H.; Tam, Y.C.; Burton, K.; et al. Surgical Management of Vestibular Schwannomas and Hearing Rehabilitation in Neurofibromatosis Type 2. Otol. Neurotol. 2012, 33, 466–472. [Google Scholar] [CrossRef]
- Nowak, A.; Dziedzic, T.; Czernicki, T.; Kunert, P.; Morawski, K.; Niemczyk, K.; Marchel, A. Strategy for the Surgical Treatment of Vestibular Schwannomas in Patients with Neurofibromatosis Type 2. Neurol. Neurochir. Pol. 2015, 49, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Samii, M.; Gerganov, V.; Samii, A. Microsurgery Management of Vestibular Schwannomas in Neurofibromatosis Type 2: Indications and Results. Prog. Neurol. Surg. 2008, 21, 169–175. [Google Scholar] [CrossRef]
- Johnson, S.; Kano, H.; Faramand, A.; Pease, M.; Nakamura, A.; Hassib, M.; Spencer, D.; Sisterson, N.; Faraji, A.H.; Arai, Y.; et al. Long Term Results of Primary Radiosurgery for Vestibular Schwannomas. J. Neurooncol. 2019, 145, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Ogino, A.; Lunsford, L.D.; Long, H.; Johnson, S.; Faramand, A.; Niranjan, A.; Flickinger, J.C.; Kano, H. Stereotactic Radiosurgery as the First-Line Treatment for Intracanalicular Vestibular Schwannomas. J. Neurosurg. 2021, 135, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Ogino, A.; Lunsford, L.D.; Long, H.; Johnson, S.; Faramand, A.; Niranjan, A.; Flickinger, J.C.; Kano, H. Stereotactic Radiosurgery as the Primary Management for Patients with Koos Grade IV Vestibular Schwannomas. J. Neurosurg. 2021, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bunevicius, A.; Anand, R.K.; Suleiman, M.; Nabeel, A.M.; Reda, W.A.; Tawadros, S.R.; Abdelkarim, K.; El-Shehaby, A.M.N.; Emad, R.M.; Chytka, T.; et al. Stereotactic Radiosurgery for Perioptic Meningiomas: An International, Multicenter Study. Neurosurgery 2021, 88, 828–837. [Google Scholar] [CrossRef] [PubMed]
- Bin-Alamer, O.; Alnefaie, N.; Qedair, J.; Chaudhary, A.; Hallak, H.; Abdulbaki, A.; Mallela, A.N.; Palmisciano, P.; Gersey, Z.C.; Legarreta, A.D.; et al. Single Session versus Multisession Stereotactic Radiosurgery for the Management of Intracranial Meningiomas: A Systematic Review and Meta-Analysis. J. Neurooncol. 2022. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Age, years | 46 (IQR, 32–55) |
| Male sex | 63 (59.4%) |
| Tumor size, cm3 | 24.3 (15.2–42) |
| Involved structures | n = 111 |
| Pterygopalatine fossa | 29 (26.1%) |
| Temporomandibular Joint | 14 (12.6%) |
| The orbit | 14 (12.6%) |
| Maxilla | 12 (10.8%) |
| Cavernous sinus | 10 (9.0%) |
| Middle cranial fossa | 10 (9.0%) |
| Nasopharynx | 9 (8.1%) |
| Paranasal sinus | 6 (5.4%) |
| Zygomatic arch | 3 (2.7%) |
| Hard and soft palate | 1 (0.9%) |
| Temporomandibular fossa | 1 (0.9%) |
| Petroclival region | 1 (0.9%) |
| Oropharynx | 1 (0.9%) |
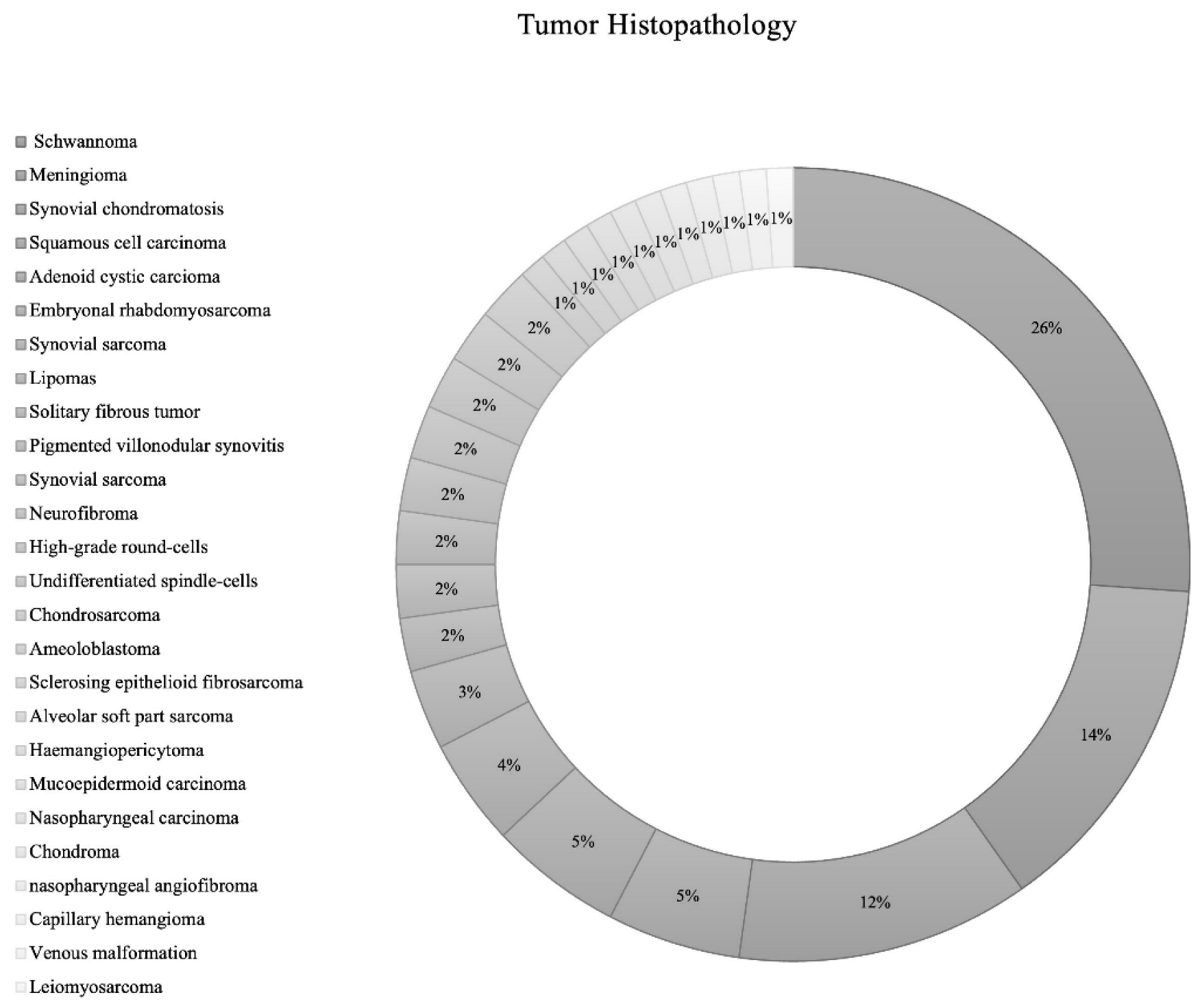
| Histopathology | n = 92 |
| Schwannoma | 24 (26.1%) |
| Meningioma | 13 (14.1%) |
| Synovial chondromatosis | 11 (12.0%) |
| Squamous cell carcinoma | 5 (5.4%) |
| Adenoid cystic carcinoma | 5 (5.4%) |
| Embryonal rhabdomyosarcoma | 4 (4.4%) |
| Synovial sarcoma | 3 (3.3%) |
| Lipomas | 2 (2.2%) |
| Solitary fibrous tumor | 2 (2.2%) |
| Pigmented villonodular synovitis | 2 (2.2%) |
| Synovial sarcoma | 2 (2.2%) |
| Neurofibroma | 2 (2.2%) |
| High-grade round-cells | 2 (2.2%) |
| Undifferentiated spindle-cells | 2 (2.2%) |
| Chondrosarcoma | 2 (2.2%) |
| Ameloblastoma | 1 (1.1%) |
| Sclerosing epithelioid fibrosarcoma | 1 (1.1%) |
| Alveolar soft part sarcoma | 1 (1.1%) |
| Hemangiopericytoma | 1 (1.1%) |
| Mucoepidermoid carcinoma | 1 (1.1%) |
| Nasopharyngeal carcinoma | 1 (1.1%) |
| Chondroma | 1 (1.1%) |
| Nasopharyngeal angiofibroma | 1 (1.1%) |
| Capillary hemangioma | 1 (1.1%) |
| Venous malformation a | 1 (1.1%) |
| Leiomyosarcoma | 1 (1.1%) |
| Presentation symptoms | n = 119 |
| Facial hypoesthesia | 22 (18.5%) |
| Auricular/preauricular pain | 20 (16.8%) |
| Headaches | 11 (9.2%) |
| Jaw deviation | 11 (9.2%) |
| Hearing loss | 9 (7.6%) |
| Facial pain | 8 (6.7%) |
| Trismus | 6 (5.0%) |
| Temporomandibular Joint pain | 4 (3.4%) |
| Diplopia | 3 (2.5%) |
| Decreased vision | 3 (2.5%) |
| Nasal obstruction/congestion | 2 (1.7%) |
| Vertigo | 2 (1.7%) |
| Trigeminal neuralgia | 2 (1.7%) |
| Exophthalmos | 2 (1.7%) |
| Otitis media | 1 (0.8%) |
| Dysarthria | 1 (0.8%) |
| Dysphagia | 1 (0.8%) |
| Dementia | 1 (0.8%) |
| Ptosis | 1 (0.8%) |
| Involved cranial nerves | n = 15 |
| CN III | 2 (13.3%) |
| CN IV | 1 (6.7%) |
| CN V | 7 (46.7%) |
| CN VI | 3 (20.0%) |
| CN VII | 1 (6.7%) |
| CN IX | 1 (6.7%) |
| Patients had surgical resection | 97 (95.1%) |
| Surgical approach | n = 95 * |
| TCS | 70 (73.7%) |
| EES | 25 (26.3%) |
| Mandibulotomy approach | 16 (17.8%) |
| Condylotomy with posterior disc attachment release | 14 (15.6%) |
| Unspecified endoscopic endonasal approach | 13 (14.4%) |
| Middle fossa/zygomatic approach | 9 (10.0%) |
| Endoscopic prelacrimal recess approach | 6 (6.7%) |
| Endoscopic extended medial maxillectomy | 5 (5.6%) |
| Cervical approach | 3 (3.3%) |
| Transmandibular approach | 3 (3.3%) |
| Submandibular and preauricular approach | 2 (2.2%) |
| Latero-facial approach | 2 (2.2%) |
| Degloving approach | 2 (2.2%) |
| Parotidectomy incision | 2 (2.2%) |
| Submandibular cutaneous incision | 1 (1.1%) |
| Preauricular subtemporal approach | 1 (1.1%) |
| Orbito-zygomatic approach | 1 (1.1%) |
| Left temporal craniotomy | 1 (1.1%) |
| Temporal and buccal incision | 1 (1.1%) |
| Weber Fergusson approach | 1 (1.1%) |
| Transzygomatic arch approach | 1 (1.1%) |
| Transcochlear approach | 1 (1.1%) |
| Orbito-zygomatic osteotomy | 1 (1.1%) |
| Zygomatic osteotomy | 1 (1.1%) |
| Antero-lateral, transcraniofacial, subtemporal, extradural approach | 1 (1.1%) |
| Coronal approach | 1 (1.1%) |
| Endoscopic Denker’s approach | 1 (1.1%) |
| Extent of surgical resection | n = 84 |
| Gross-total resection | 62 (73.8%) |
| Subtotal resection | 17 (20.2%) |
| Biopsy | 5 (6.0%) |
| Surgical complications | |
| All complications | 35 (33.0%) |
| Lingual nerve complication | 8 (22.9%) |
| Inferior alveolar nerve complication | 7 (20.0%) |
| Facial paresis | 7 (20.0%) |
| Partial facial numbness | 3 (8.6%) |
| Facial pain | 2 (5.7%) |
| Deep vein thrombosis | 2 (5.7%) |
| CN III Deficit | 1 (2.9%) |
| CN VI Deficit | 2 (5.7%) |
| CN VII Deficit | 1 (2.9%) |
| CN VIIII Deficit | 1 (2.9%) |
| Wound dehiscence | 1 (2.9%) |
| Reconstruction techniques and material | n = 8 |
| Adipofascial antero-lateral thigh flap | 4 (50%) |
| Latissimus dorsi free flap | 3 (37.5%) |
| Antero-lateral thigh flap | 1 (12.5%) |
| Adjuvant chemotherapy | n = 14 (13.2%) |
| Methotrexate | 1 (7.1%) |
| Cisplatin | 1 (7.1%) |
| Ifosfamide | 1 (7.1%) |
| Doxorubicin | 1 (7.1%) |
| Unknown | 10 (71.4%) |
| Adjuvant radiotherapy | n = 16 (15.1%) |
| EBRT | 3 (18.8%) |
| GKRS | 2 (12.5%) |
| Proton beam therapy | 1 (6.3%) |
| Unknown | 10 (62.5%) |
| Recurrence | 15 (14.2%) |
| Status | n = 97 |
| Alive | 88 (83.0%) |
| Dead | 18 (17.0%) |
| Survival rates | |
| 5-year OS | 20% |
| 5-year PFS | 61% |
| Median follow-up time in months (IQR) | 28 months (12.3–45.8) |
| Surgical Access Based on Tumor Histology | Number of Patients with Available Data | Endonasal Access No. (%) | p-Value ^ |
|---|---|---|---|
| Trigeminal schwannoma | 22 | 19 (86%) | <0.01 |
| Grade 1 meningioma | 12 | 2 (16.7%) | |
| Squamous cell carcinoma | 3 | 1 (33%) | |
| Grade 2 meningioma | 1 | 1 (100%) | |
| The rest | 54 | 0 | |
| Complication Based on Surgical Access | Total Number of Patients with Each Access | Complications No. (%) | p-Value ^ |
| Transcranial access | 70 | 33 (47.1%) | 0.01 |
| Endonasal access | 25 | 2 (8.0%) | |
| Complication Based on Surgical Approach | Total Number of Patients with Each Approach | Complications No. (%) | p-Value ^ |
| Parotidectomy incision | 2 | 2 (100.0%) | <0.01 |
| Transzygomatic arch approach | 1 | 1 (100.0%) | |
| Latero-facial approach | 2 | 2 (100.0%) | |
| Mandibulotomy approach | 16 | 9 (56.3%) | |
| Middle fossa/zygomatic approach | 9 | 3 (33.3%) | |
| Endoscopic prelacrimal recess | 6 | 1 (16.7%) | |
| Cervical approach | 3 | 1 (33.3%) | |
| Condylotomy with posterior disc attachment release | 14 | 2 (14.3%) | |
| Endoscopic endonasal approach | 13 | 1 (7.7%) | |
| Recurrence Rate Based on Tumor Histology | Total Number of Patients | Death No. (%) | p-Value ^ |
| Trigeminal schwannoma | 22 | 1 (5%) | 0.04 |
| Grade 1 meningioma | 12 | 3 (25%) | |
| Adenoid cystic carcinoma | 5 | 2 (40%) | |
| Squamous cell carcinoma | 5 | 1 (20%) | |
| Synovial sarcoma | 5 | 3 (60%) | |
| Alveolar soft part sarcoma | 1 | 1 (100%) | |
| Sclerosing epithelioid fibrosarcoma | 1 | 1 (100%) | |
| Grade 2 meningioma | 1 | 1 (100%) | |
| Capillary hemangioma | 1 | 1 (100%) | |
| The rest | 39 | 0 | |
| Mortality Rates Based on Tumor Histology | Total Number of Patients | Death No. (%) | p-Value ^ |
| Trigeminal schwannoma | 22 | 3 (13.6%) | <0.01 |
| Grade 1 meningioma | 12 | 1 (8.3%) | |
| Adenoid cystic carcinoma | 5 | 1 (20%) | |
| Synovial sarcoma | 5 | 4 (80%) | |
| Neurofibroma | 2 | 2 (100%) | |
| Undifferentiated spindle cells | 2 | 2 (100%) | |
| Alveolar soft part sarcoma | 1 | 1 (100%) | |
| Sclerosing epithelioid fibrosarcoma | 1 | 1 (100%) | |
| The rest | 42 | 0 |
| Variable | Overall Survival | |||
|---|---|---|---|---|
| Univariable Analysis | Multivariable Analysis | |||
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | 1.0 (0.9–1.0) | 0.4 | 1.0 (1.0–1.0) | 0.45 |
| Male sex | 0.9 (0.5–1.4) | 0.6 | 1.4 (0.6–3.4) | 0.42 |
| Schwannoma | 0.6 (0.3–1.1) | 0.09 | NA | NA |
| Meningioma | 1.5 (0.6–3.8) | 0.4 | NA | NA |
| Tumor volume cc | 1.0 (0.9–1.0) | 0.3 | 1.0 (1.0–1.0) | 0.09 |
| EES (Vs. TCS) | 0.7 (0.4–1.1) | 0.2 | NA | NA |
| GTR (Vs. STR) | 1.1 (0.8–1.6) | 0.2 | 6.5 (1.4–29.0) | 0.02 |
| Adjuvant chemotherapy | 0.6 (0.3–1.2) | 0.1 | 0.6 (0–52.4) | 0.82 |
| Adjuvant radiotherapy | 0.9 (0.4–1.9) | 0.7 | NA | NA |
| Variable | Progression-Free Survival | |||
|---|---|---|---|---|
| Univariable Analysis | Multivariable Analysis | |||
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | 0.9 (0.9–1.0) | 0.6 | 1 (0.9–1.2) | 0.6 |
| Male sex | 0.8 (0.3–2.1) | 0.6 | 9.37 × 108 (0-inf) | 1 |
| Schwannoma | 0.0 (0-inf) | 1 | 2.2 (0-inf) | 1 |
| Meningioma | 0.31 (0.1–1.0) | 0.04 | NA | NA |
| Tumor volume cc | 1.0 (1.0–1.0) | 0.9 | 1.0 (1.0–1.0) | 0.8 |
| EES (Vs. TCS) | 3.7 (0.8–16.4) | 0.08 | 2.66 × 108 (0-inf) | 1 |
| GTR (Vs. STR) | 2.5 (1.5–4.1) | <0.01 | 2.70 × 10−5 (0-inf) | 1 |
| Adjuvant chemotherapy | 0.26 (0.1–0.7) | <0.01 | 9.50 × 10−11 (0-inf) | 1 |
| Adjuvant radiotherapy | 0.32 (0.1–0.9) | 0.02 | NA | NA |
| Variable | Complications | |||
|---|---|---|---|---|
| Univariable Analysis | Multivariable Analysis | |||
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age > 46 years | 2.4 (0.7–9.8) | 0.2 | 5.58 × 108 (1.59 × 10−209-NA) | 1.0 |
| Male sex | 0.3 (0.1–1.1) | 0.09 | 5.58 × 108 (0–1) | 0.1 |
| Tumor volume > 24.3 cc | 2.1 (0.19–48.4) | 0.6 | 2.6 (0.1–236.5) | 0.6 |
| EES (Vs. TCS) | 4.1 (1.1–27.1) | 0.07 | 0.4 (0–16.9) | 0.6 |
| GTR (Vs. STR) | 1.5 (0.8–2.7) | 0.18 | 4.5 (0–1.6 × 1095) | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bin-Alamer, O.; Bhenderu, L.S.; Palmisciano, P.; Balasubramanian, K.; Upadhyay, P.; Ferini, G.; Viola, A.; Zagardo, V.; Yu, K.; Cohen-Gadol, A.A.; et al. Tumors Involving the Infratemporal Fossa: A Systematic Review of Clinical Characteristics and Treatment Outcomes. Cancers 2022, 14, 5420. https://doi.org/10.3390/cancers14215420
Bin-Alamer O, Bhenderu LS, Palmisciano P, Balasubramanian K, Upadhyay P, Ferini G, Viola A, Zagardo V, Yu K, Cohen-Gadol AA, et al. Tumors Involving the Infratemporal Fossa: A Systematic Review of Clinical Characteristics and Treatment Outcomes. Cancers. 2022; 14(21):5420. https://doi.org/10.3390/cancers14215420
Chicago/Turabian StyleBin-Alamer, Othman, Lokeshwar S. Bhenderu, Paolo Palmisciano, Kishore Balasubramanian, Prashant Upadhyay, Gianluca Ferini, Anna Viola, Valentina Zagardo, Kenny Yu, Aaron A. Cohen-Gadol, and et al. 2022. "Tumors Involving the Infratemporal Fossa: A Systematic Review of Clinical Characteristics and Treatment Outcomes" Cancers 14, no. 21: 5420. https://doi.org/10.3390/cancers14215420