

Transarterial Yttrium-90 Radioembolization in Intrahepatic Cholangiocarcinoma Patients: Outcome Assessment Applying a Prognostic Score
 , ,
, ,  , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Cohort
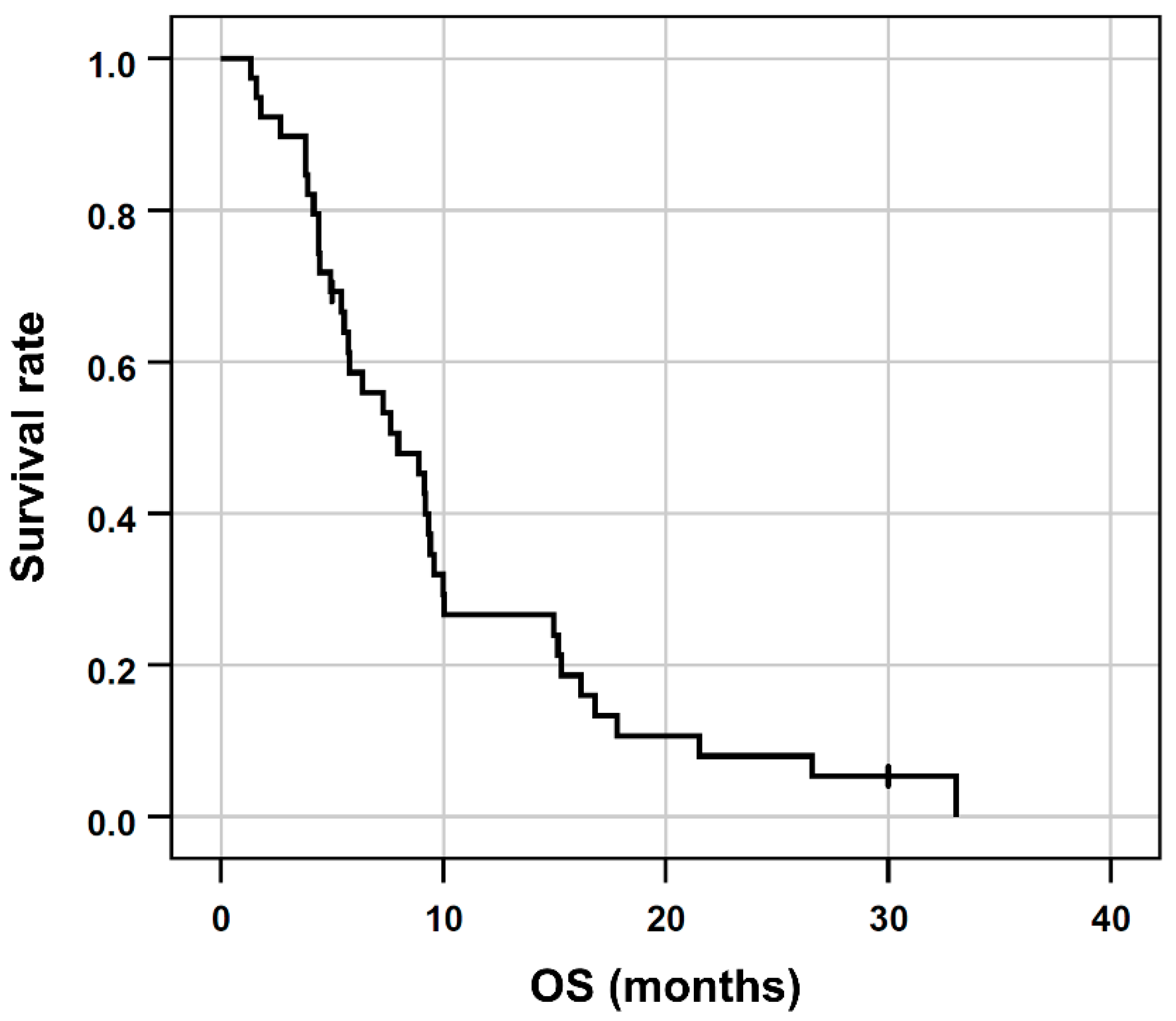
2.2. Overall Survival and Therapy Response
2.3. Treatment and Toxicity
2.4. Univariable Cox Regression
2.5. Multivariable Cox Regression
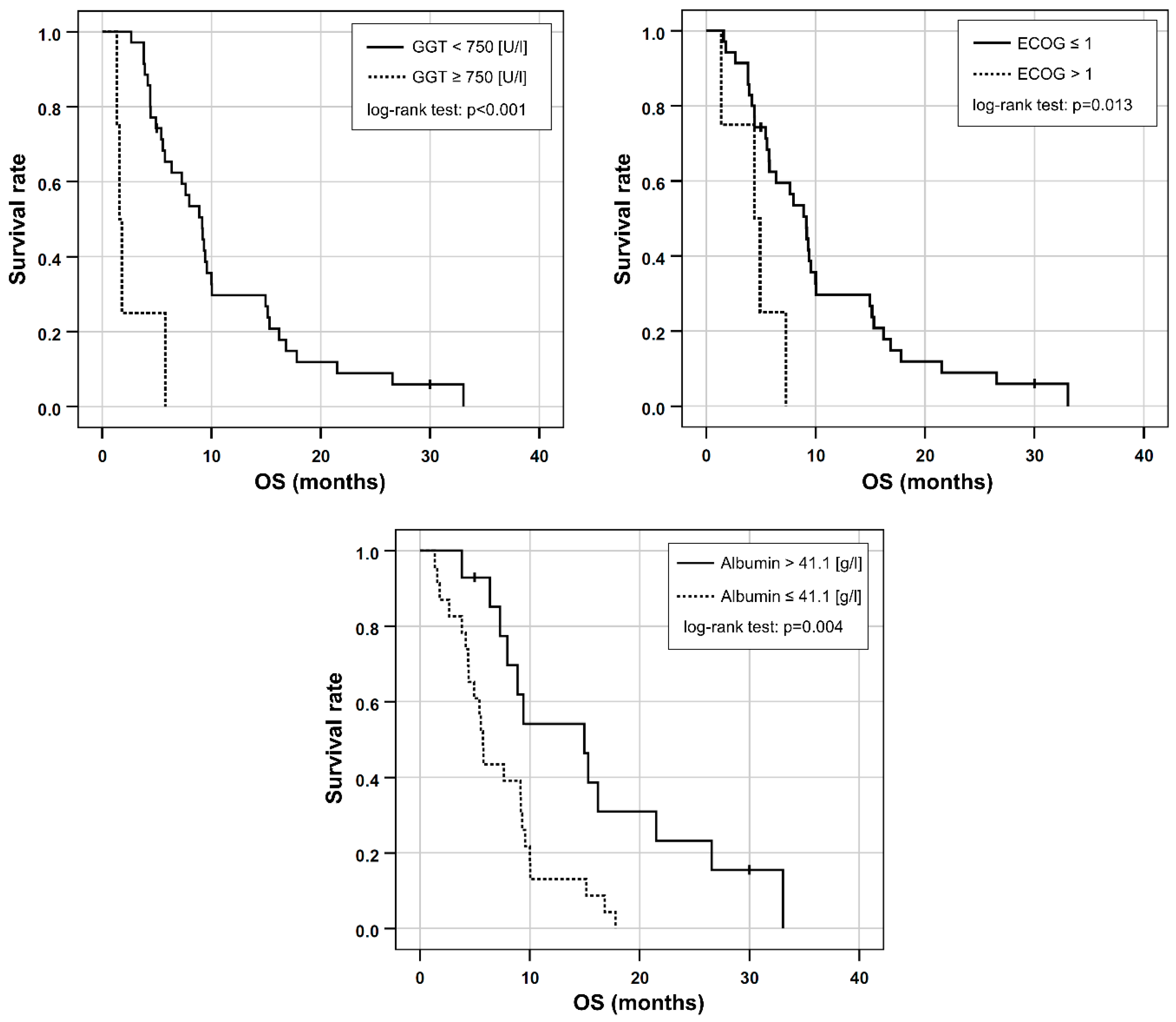
2.6. Combined Prognostic Score
3. Discussion
4. Materials and Methods
4.1. Study Design and Eligibility Criteria
4.2. Radioembolization
4.3. Assessment of Toxicity and Survival
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef] [Green Version]
- Roayaie, S.; Guarrera, J.V.; Ye, M.Q.; Thung, S.N.; Emre, S.; Fishbein, T.M.; Guy, S.R.; Sheiner, P.A.; Miller, C.M.; Schwartz, M.E. Aggressive surgical treatment of intrahepatic cholangiocarcinoma: Predictors of outcomes. J. Am. Coll. Surg. 1998, 187, 365–372. [Google Scholar] [CrossRef]
- Al-Adra, D.P.; Gill, R.S.; Axford, S.J.; Shi, X.; Kneteman, N.; Liau, S.S. Treatment of unresectable intrahepatic cholangiocarcinoma with yttrium-90 radioembolization: A systematic review and pooled analysis. Eur. J. Surg. Oncol. 2015, 41, 120–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippi, L.; Schillaci, O.; Cianni, R.; Bagni, O. Yttrium-90 resin microspheres and their use in the treatment of intrahepatic cholangiocarcinoma. Future Oncol. 2018, 14, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A.; Coldwell, D.; Sangro, B.; Wasan, H.; Salem, R. Radioembolization for the treatment of liver tumors general principles. Am. J. Clin. Oncol. 2012, 35, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Levillain, H.; Duran Derijckere, I.; Ameye, L.; Guiot, T.; Braat, A.; Meyer, C.; Vanderlinden, B.; Reynaert, N.; Hendlisz, A.; Lam, M.; et al. Personalised radioembolization improves outcomes in refractory intra-hepatic cholangiocarcinoma: A multicenter study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2270–2279. [Google Scholar] [CrossRef] [PubMed]
- Sangro, B.; Gil-Alzugaray, B.; Rodriguez, J.; Sola, I.; Martinez-Cuesta, A.; Viudez, A.; Chopitea, A.; Iñarrairaegui, M.; Arbizu, J.; Bilbao, J.I. Liver disease induced by radioembolization of liver tumors: Description and possible risk factors. Cancer 2008, 112, 1538–1546. [Google Scholar] [CrossRef]
- Braat, M.N.; van Erpecum, K.J.; Zonnenberg, B.A.; van den Bosch, M.A.; Lam, M.G. Radioembolization-induced liver disease: A systematic review. Eur. J. Gastroenterol. Hepatol. 2017, 29, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Levillain, H.; Bagni, O.; Deroose, C.M.; Dieudonné, A.; Gnesin, S.; Grosser, O.S.; Kappadath, S.C.; Kennedy, A.; Kokabi, N.; Liu, D.M.; et al. International recommendations for personalised selective internal radiation therapy of primary and metastatic liver diseases with yttrium-90 resin microspheres. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1570–1584. [Google Scholar] [CrossRef] [PubMed]
- Kis, B.; El-Haddad, G.; Sheth, R.A.; Parikh, N.S.; Ganguli, S.; Shyn, P.B.; Choi, J.; Brown, K.T. Liver-Directed Therapies for Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. Cancer Control. 2017, 24, 1073274817729244. [Google Scholar] [CrossRef] [PubMed]
- Antkowiak, M.; Gabr, A.; Das, A.; Ali, R.; Kulik, L.; Ganger, D.; Moore, C.; Abecassis, M.; Katariya, N.; Mouli, S.; et al. Prognostic Role of Albumin, Bilirubin, and ALBI Scores: Analysis of 1000 Patients with Hepatocellular Carcinoma Undergoing Radioembolization. Cancers 2019, 11, 879. [Google Scholar] [CrossRef] [Green Version]
- Damm, R.; Seidensticker, R.; Ulrich, G.; Breier, L.; Steffen, I.G.; Seidensticker, M.; Garlipp, B.; Mohnike, K.; Pech, M.; Amthauer, H.; et al. Y90 Radioembolization in chemo-refractory metastastic, liver dominant colorectal cancer patients: Outcome assessment applying a predictive scoring system. BMC Cancer 2016, 16, 509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.A.; Jang, H.; Choi, N.R.; Nam, J.Y.; Lee, Y.B.; Cho, E.J.; Lee, J.H.; Yu, S.J.; Kim, H.C.; Chung, J.W.; et al. Yttrium-90 Radioembolization Is Associated with Better Clinical Outcomes in Patients with Hepatocellular Carcinoma Compared with Conventional Chemoembolization: A Propensity Score-Matched Study. J. Hepatocell. Carcinoma 2021, 8, 1565–1577. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.Y.; Lee, Y.B.; Lee, J.H.; Yu, S.J.; Kim, H.C.; Chung, J.W.; Yoon, J.H.; Kim, Y.J. A Prognostic Prediction Model of Transarterial Radioembolization in Hepatocellular Carcinoma: SNAP-HCC. Dig. Dis. Sci. 2022, 67, 329–336. [Google Scholar] [CrossRef]
- Schatka, I.; Tschernig, M.; Rogasch, J.M.M.; Bluemel, S.; Graef, J.; Furth, C.; Sehouli, J.; Blohmer, J.U.; Gebauer, B.; Fehrenbach, U.; et al. Selective Internal Radiation Therapy in Breast Cancer Liver Metastases: Outcome Assessment Applying a Prognostic Score. Cancers 2021, 13, 3777. [Google Scholar] [CrossRef] [PubMed]
- Op den Winkel, M.; Nagel, D.; de la Torre Aláez, M.A.; Hempe, S.; De Toni, E.N.; Paprottka, K.J.; Op den Winkel, P.; Stecher, S.S.; Bourhis, H.; Gerbes, A.L.; et al. A Simple Prognostic Scoring System for Hepatocellular Carcinoma Treated with Selective Internal Radiation Therapy. Dig. Dis. 2022, 40, 322–334. [Google Scholar] [CrossRef] [PubMed]
- Soydal, C.; Keskin, O.; Kucuk, O.N.; Ozkan, E.; Bilgic, S.; Idilman, R.; Kir, M.K. Prognostic factors for prediction of survival of hepatocellular cancer patients after selective internal radiation therapy. Ann. Nucl. Med. 2015, 29, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Spreafico, C.; Sposito, C.; Vaiani, M.; Cascella, T.; Bhoori, S.; Morosi, C.; Lanocita, R.; Romito, R.; Chiesa, C.; Maccauro, M.; et al. Development of a prognostic score to predict response to Yttrium-90 radioembolization for hepatocellular carcinoma with portal vein invasion. J. Hepatol. 2018, 68, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Bargellini, I.; Scalise, P.; Boni, G.; Traino, C.A.; Bozzi, E.; Lorenzoni, G.; Crocetti, L.; Cioni, R. Yttrium-90 Radioembolization for Hepatocellular Carcinoma with Portal Vein Invasion: Validation of the Milan Prognostic Score. J. Vasc. Interv. Radiol. 2020, 31, 2028–2032. [Google Scholar] [CrossRef]
- Hoffmann, R.T.; Paprottka, P.M.; Schön, A.; Bamberg, F.; Haug, A.; Dürr, E.M.; Rauch, B.; Trumm, C.T.; Jakobs, T.F.; Helmberger, T.K.; et al. Transarterial hepatic yttrium-90 radioembolization in patients with unresectable intrahepatic cholangiocarcinoma: Factors associated with prolonged survival. Cardiovasc. Intervent. Radiol. 2012, 35, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.; Khan, S.A.; Hallemeier, C.L.; Kelley, R.K.; Gores, G.J. Cholangiocarcinoma—Evolving concepts and therapeutic strategies. Nat. Rev. Clin. Oncol. 2018, 15, 95–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarnagin, W.R.; Fong, Y.; DeMatteo, R.P.; Gonen, M.; Burke, E.C.; Bodniewicz, B.J.; Youssef, B.M.; Klimstra, D.; Blumgart, L.H. Staging, resectability, and outcome in 225 patients with hilar cholangiocarcinoma. Ann. Surg. 2001, 234, 507–517, discussion 517–509. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Wang, H.; Ning, Z.; Xu, L.; Zhuang, L.; Wang, P.; Meng, Z. Serum liver enzymes serve as prognostic factors in patients with intrahepatic cholangiocarcinoma. Onco. Targets Ther. 2017, 10, 1441–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.S.; Miao, R.C.; Zhang, L.Q.; Wang, R.T.; Qu, K.; Pang, Q.; Liu, C. Model Based on Alkaline Phosphatase and Gamma-Glutamyltransferase for Gallbladder Cancer Prognosis. Asian Pac. J. Cancer Prev. 2015, 16, 6255–6259. [Google Scholar] [CrossRef] [Green Version]
- Yao, D.F.; Dong, Z.Z. Hepatoma-related gamma-glutamyl transferase in laboratory or clinical diagnosis of hepatocellular carcinoma. Hepatobiliary Pancreat. Dis. Int. 2007, 6, 9–11. [Google Scholar] [PubMed]
- Yin, X.; Zheng, S.S.; Zhang, B.H.; Zhou, Y.; Chen, X.H.; Ren, Z.G.; Qiu, S.J.; Fan, J. Elevation of serum γ-glutamyltransferase as a predictor of aggressive tumor behaviors and unfavorable prognosis in patients with intrahepatic cholangiocarcinoma: Analysis of a large monocenter study. Eur. J. Gastroenterol. Hepatol. 2013, 25, 1408–1414. [Google Scholar] [CrossRef]
- Jia, Z.; Paz-Fumagalli, R.; Frey, G.; Sella, D.M.; McKinney, J.M.; Wang, W. Resin-based Yttrium-90 microspheres for unresectable and failed first-line chemotherapy intrahepatic cholangiocarcinoma: Preliminary results. J. Cancer Res. Clin. Oncol. 2017, 143, 481–489. [Google Scholar] [CrossRef]
- Saxena, A.; Bester, L.; Chua, T.C.; Chu, F.C.; Morris, D.L. Yttrium-90 radiotherapy for unresectable intrahepatic cholangiocarcinoma: A preliminary assessment of this novel treatment option. Ann. Surg. Oncol. 2010, 17, 484–491. [Google Scholar] [CrossRef]
- Ibrahim, S.M.; Mulcahy, M.F.; Lewandowski, R.J.; Sato, K.T.; Ryu, R.K.; Masterson, E.J.; Newman, S.B.; Benson, A., 3rd; Omary, R.A.; Salem, R. Treatment of unresectable cholangiocarcinoma using yttrium-90 microspheres: Results from a pilot study. Cancer 2008, 113, 2119–2128. [Google Scholar] [CrossRef]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar] [CrossRef]
- Lai, C.C.; You, J.F.; Yeh, C.Y.; Chen, J.S.; Tang, R.; Wang, J.Y.; Chin, C.C. Low preoperative serum albumin in colon cancer: A risk factor for poor outcome. Int. J. Colorectal. Dis. 2011, 26, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Tanriverdi, O.; Avci, N.; Oktay, E.; Kalemci, S.; Pilanci, K.N.; Cokmert, S.; Menekse, S.; Kocar, M.; Sen, C.A.; Akman, T.; et al. Pretreatment Serum Albumin Level is an Independent Prognostic Factor in Patients with Stage IIIB Non-Small Cell Lung Cancer: A Study of the Turkish Descriptive Oncological Researches Group. Asian Pac. J. Cancer Prev. 2015, 16, 5971–5976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waghray, A.; Sobotka, A.; Marrero, C.R.; Estfan, B.; Aucejo, F.; Narayanan Menon, K.V. Serum albumin predicts survival in patients with hilar cholangiocarcinoma. Gastroenterol. Rep. 2017, 5, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Ramacciato, G.; Di Benedetto, F.; Cautero, N.; Masetti, M.; Mercantini, P.; Corigliano, N.; Nigri, G.; Lauro, A.; Ercolani, G.; Del Gaudio, M.; et al. [Prognostic factors and long term outcome after surgery for hilar cholangiocarcinoma. Univariate and multivariate analysis]. Chir. Ital. 2004, 56, 749–759. [Google Scholar]
- Swinburne, N.C.; Biederman, D.M.; Besa, C.; Tabori, N.E.; Fischman, A.M.; Patel, R.S.; Nowakowski, F.S.; Gunasekaran, G.; Schwartz, M.E.; Lookstein, R.A.; et al. Radioembolization for Unresectable Intrahepatic Cholangiocarcinoma: Review of Safety, Response Evaluation Criteria in Solid Tumors 1.1 Imaging Response and Survival. Cancer Biother. Radiopharm. 2017, 32, 161–168. [Google Scholar] [CrossRef]
- Bouvry, C.; Palard, X.; Edeline, J.; Ardisson, V.; Loyer, P.; Garin, E.; Lepareur, N. Transarterial Radioembolization (TARE) Agents beyond (90)Y-Microspheres. Biomed. Res. Int. 2018, 2018, 1435302. [Google Scholar] [CrossRef] [Green Version]
- Mosconi, C.; Gramenzi, A.; Ascanio, S.; Cappelli, A.; Renzulli, M.; Pettinato, C.; Brandi, G.; Monari, F.; Cucchetti, A.; Trevisani, F.; et al. Yttrium-90 radioembolization for unresectable/recurrent intrahepatic cholangiocarcinoma: A survival, efficacy and safety study. Br. J. Cancer 2016, 115, 297–302. [Google Scholar] [CrossRef]
- Edeline, J.; Du, F.L.; Rayar, M.; Rolland, Y.; Beuzit, L.; Boudjema, K.; Rohou, T.; Latournerie, M.; Campillo-Gimenez, B.; Garin, E.; et al. Glass Microspheres 90Y Selective Internal Radiation Therapy and Chemotherapy as First-Line Treatment of Intrahepatic Cholangiocarcinoma. Clin. Nucl. Med. 2015, 40, 851–855. [Google Scholar] [CrossRef]
- Rafi, S.; Piduru, S.M.; El-Rayes, B.; Kauh, J.S.; Kooby, D.A.; Sarmiento, J.M.; Kim, H.S. Yttrium-90 radioembolization for unresectable standard-chemorefractory intrahepatic cholangiocarcinoma: Survival, efficacy, and safety study. Cardiovasc. Intervent. Radiol. 2013, 36, 440–448. [Google Scholar] [CrossRef]
- Soydal, C.; Kucuk, O.N.; Bilgic, S.; Ibis, E. Radioembolization with 90Y resin microspheres for intrahepatic cholangiocellular carcinoma: Prognostic factors. Ann. Nucl. Med. 2016, 30, 29–34. [Google Scholar] [CrossRef]
- Levillain, H.; Duran Derijckere, I.; Marin, G.; Guiot, T.; Vouche, M.; Reynaert, N.; Hendlisz, A.; Vanderlinden, B.; Flamen, P. (90)Y-PET/CT-based dosimetry after selective internal radiation therapy predicts outcome in patients with liver metastases from colorectal cancer. EJNMMI Res. 2018, 8, 60. [Google Scholar] [CrossRef] [PubMed]
- D’Arienzo, M.; Pimpinella, M.; Capogni, M.; De Coste, V.; Filippi, L.; Spezi, E.; Patterson, N.; Mariotti, F.; Ferrari, P.; Chiaramida, P.; et al. Phantom validation of quantitative Y-90 PET/CT-based dosimetry in liver radioembolization. EJNMMI Res. 2017, 7, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ritis, F.; Coltorti, M.; Giusti, G. An enzymic test for the diagnosis of viral hepatitis; the transaminase serum activities. Clin. Chim. Acta 1957, 2, 70–74. [Google Scholar] [CrossRef]
- Salem, R.; Lewandowski, R.J.; Gates, V.L.; Nutting, C.W.; Murthy, R.; Rose, S.C.; Soulen, M.C.; Geschwind, J.F.; Kulik, L.; Kim, Y.H.; et al. Research reporting standards for radioembolization of hepatic malignancies. J. Vasc. Interv. Radiol. 2011, 22, 265–278. [Google Scholar] [CrossRef] [Green Version]
- Lüdemann, W.; Kahn, J.; Pustelnik, D.; Hardt, J.; Böning, G.; Jonczyk, M.; Amthauer, H.; Gebauer, B.; Hamm, B.; Wieners, G. Yttrium-90 radioembolization for unresectable hepatocellular carcinoma: Predictive modeling strategies to anticipate tumor response and improve patient selection. Eur. Radiol. 2022, 32, 4687–4698. [Google Scholar] [CrossRef]
- Gibbs, P.; Gebski, V.; Van Buskirk, M.; Thurston, K.; Cade, D.N.; Van Hazel, G.A. Selective Internal Radiation Therapy (SIRT) with yttrium-90 resin microspheres plus standard systemic chemotherapy regimen of FOLFOX versus FOLFOX alone as first-line treatment of non-resectable liver metastases from colorectal cancer: The SIRFLOX study. BMC Cancer 2014, 14, 897. [Google Scholar] [CrossRef] [Green Version]
- Hazel, G.A.V.; Heinemann, V.; Sharma, N.K.; Findlay, M.P.N.; Ricke, J.; Peeters, M.; Perez, D.; Robinson, B.A.; Strickland, A.H.; Ferguson, T.; et al. SIRFLOX: Randomized Phase III Trial Comparing First-Line mFOLFOX6 (Plus or Minus Bevacizumab) Versus mFOLFOX6 (Plus or Minus Bevacizumab) Plus Selective Internal Radiation Therapy in Patients With Metastatic Colorectal Cancer. J. Clin. Oncol.-N. Y. 2016, 34, 1723–1731. [Google Scholar] [CrossRef]
- Dutton, S.J.; Kenealy, N.; Love, S.B.; Wasan, H.S.; Sharma, R.A. FOXFIRE protocol: An open-label, randomised, phase III trial of 5-fluorouracil, oxaliplatin and folinic acid (OxMdG) with or without interventional Selective Internal Radiation Therapy (SIRT) as first-line treatment for patients with unresectable liver-only or liver-dominant metastatic colorectal cancer. BMC Cancer 2014, 14, 497. [Google Scholar] [CrossRef] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Fendler, W.P.; Lechner, H.; Todica, A.; Paprottka, K.J.; Paprottka, P.M.; Jakobs, T.F.; Michl, M.; Bartenstein, P.; Lehner, S.; Haug, A.R. Safety, Efficacy, and Prognostic Factors After Radioembolization of Hepatic Metastases from Breast Cancer: A Large Single-Center Experience in 81 Patients. J. Nucl. Med. 2016, 57, 517–523. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Number (%) or Median (IQR; Range) |
|---|---|
| RE procedures | 42 (100) |
| Age [years] | 61 (IQR, 56–69; range, 32–82) |
| Female/male sex | 26/13 (100) |
| ECOG performance status | |
| - 0 | 19 (49) |
| - 1 | 16 (41) |
| - 2 | 4 (10) |
| Baseline laboratory parameters | |
| - Total bilirubin [mg/dL] | 0.5 (IQR, 0.4–0.7; range, 0.1–1.4) |
| - AST [U/L] - ALT [U/L] | 41 (IQR, 35–65; range, 25–394) 25 (IQR, 17–38; range, 12–128) |
| - AST/ALT ratio | 1.8 (IQR, 1.4–2.5; range, 0.73–5.13 |
| - GGT [U/L] - Albumin [g/L] - INR - Ammonia [µmol/L] - CA19-9 [U/mL] | 222 (IQR, 91–383; range, 24–1210) 40.6 (IQR, 37.2–42.9; range, 31–47) 1.06 (IQR, 1–1.1; range, 0.92–1.9) 36.2 (IQR, 28.9–52.6; range, 20.2–83.1) 72 (IQR, 8.7–259.8; range, 1.9–36249) |
| Presence of | |
| - Extrahepatic tumor manifestation | 20 (51) |
| - Thrombosis of the portal vein | 8 (21) |
| - Ascites - Sequential RE | 6 (15) 3 (8) |
| Baseline hepatic tumor burden | |
| - unilobar | 20 (51) |
| - bilobar - Liver volume [mL] - Hepatic tumor burden [mL] - Total tumor burden [%] ≤25% 26–50% >50% | 19 (49) 1804 (IQR, 1477–2229; range, 947–3560) 316 (IQR, 75–589; range, 22–1838) 14.5 (IQR, 4.5–29.9; range, 1.9–51.6) 27 (69) 10 (256) 2 (5) |
| Hepatopulmonary shunt [%] | 9.8 (IQR, 6.6–12.3; range, 2.6–18.7) |
| Prior treatment | 36 (92) |
| - Chemotherapy - Hepatic surgery - Local hepatic therapy | 29 (74) 21 (54) 8 (21) |
| - Intraarterial therapy | 3 (8) |
| Variable | HR (95% CI) | p-Value |
|---|---|---|
| Age [years] | 1.01 (0.97–1.04) | 0.755 |
| ECOG performance status | 0.005 | |
| - 1 vs. 0 | 1.30 (0.7–2.7) | 0.44 |
| - 2 vs. 0 | 4.27 (1.3–13.8) | 0.015 |
| - 2 vs. < 2 | 3.76 (1.2–11.6) | 0.021 |
| Baseline laboratory parameters | ||
| - Total bilirubin [mg/dL] | 0.632 (0.19–2.09) | 0.45 |
| - AST [U/l] | 1.003 (1.00–1.01) | 0.33 |
| - ALT [U/l] - AST/ALT ratio - GGT [U/L] - AP [U/L] - Albumin [g/L] - INR - Ammonia [µmol/L] - CA19-9 [U/ml] | 0.999 (0.98–1.02) 1.586 (1.08–2.33) 1.002 (1.00–1.00) 1.002 (1.00–1.00) 0.927 (0.86–1.00) 1.487 (0.21–10.77) 1.005 (0.98–1.04 1.000 (1.00–1.00) | 0.88 0.018 0.016 0.77 0.045 0.695 0.763 0.021 |
| Hepatopulmonary shunt [%] | 1.08 (0.99–1.19) | 0.09 |
| Dose reduction | ||
| - 20 vs. 0% | 1.28 (0.6–2.6) | 0.53 |
| - 40 vs. 0% | 4.12 (1.2–13.9) | 0.022 |
| - 40 vs. 0–20% | 3.74 (1.2–12.1) | 0.027 |
| - Total tumor burden [%] | 1.01 (0.99–1.03) | 0.37 |
| - Tumor burden treated lobe [%] | 1.01 (0.99–1.03) | 0.28 |
| Presence vs. absence of - Bilobar manifestation | 1.12 (0.55–2.08) | 0.84 |
| - Extrahepatic tumor manifestation | 1.45 (0.74–2.84) | 0.29 |
| - Thrombosis of the portal vein | 1.08 (0.45–2.39) | 0.85 |
| - Ascites - Sequential RE - Chemotherapy - Liver surgery - Local liver therapy - Intraarterial therapy | 1.99 (0.80–4.94 0.61 (0.19–1.99) 0.92 (0.49–2.22 0.72 (0.37–1.39) 0.86 (0.37–1.97) 0.39 (0.09–1.68) | 0.14 0.41 0.92 0.33 0.71 0.21 |
| Variable | HR (95% CI) | p-Value |
|---|---|---|
| GGT ≥ 750 [U/L] | 7.96 (2.3–28.1) | 0.001 |
| ECOG > 1 | 6.34 (1.8–21.8) | 0.003 |
| Albumin ≤ 41.1 [g/L] | 2.8 (1.2–6.3) | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schatka, I.; Jochens, H.V.; Rogasch, J.M.M.; Walter-Rittel, T.C.; Pelzer, U.; Benckert, J.; Graef, J.; Feldhaus, F.W.; Gebauer, B.; Amthauer, H. Transarterial Yttrium-90 Radioembolization in Intrahepatic Cholangiocarcinoma Patients: Outcome Assessment Applying a Prognostic Score. Cancers 2022, 14, 5324. https://doi.org/10.3390/cancers14215324
Schatka I, Jochens HV, Rogasch JMM, Walter-Rittel TC, Pelzer U, Benckert J, Graef J, Feldhaus FW, Gebauer B, Amthauer H. Transarterial Yttrium-90 Radioembolization in Intrahepatic Cholangiocarcinoma Patients: Outcome Assessment Applying a Prognostic Score. Cancers. 2022; 14(21):5324. https://doi.org/10.3390/cancers14215324
Chicago/Turabian StyleSchatka, Imke, Hans V. Jochens, Julian M. M. Rogasch, Thula C. Walter-Rittel, Uwe Pelzer, Julia Benckert, Josefine Graef, Felix W. Feldhaus, Bernhard Gebauer, and Holger Amthauer. 2022. "Transarterial Yttrium-90 Radioembolization in Intrahepatic Cholangiocarcinoma Patients: Outcome Assessment Applying a Prognostic Score" Cancers 14, no. 21: 5324. https://doi.org/10.3390/cancers14215324