
Association of Non-Steroidal Anti-Inflammatory Drugs, Genetic Risk, and Environmental Risk Factors with Incidence of Colorectal Cancer
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Polygenic Risk Score
2.3. Environmental Risk Score
2.4. Ascertainment of CRC Incidence
2.5. Statistical Analyses
3. Results
3.1. Relationships of NSAID Use, Genetic Risk, Environmental Risk Factors and Population-Attributable Fractions with CRC Incidence
3.2. Relationship of Environmental Risk Factors with CRC Incidence According to the Genetic Risk
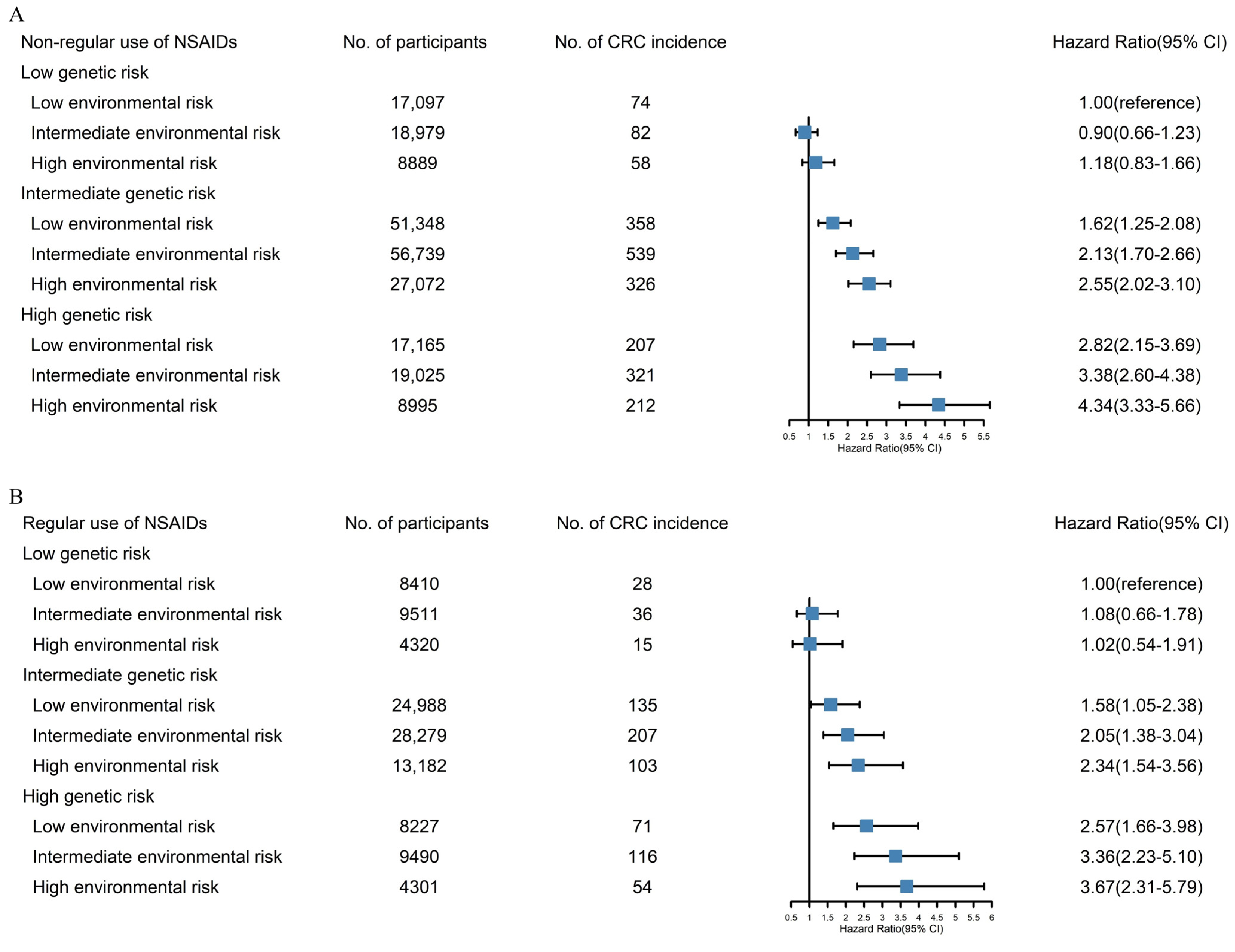
3.3. Relationship of Genetic Risk and Environmental Risk Factors with CRC Incidence Stratified by Non-Regular and Regular NSAID Use
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| CRC | Colorectal Cancer |
| DASH | Dietary Approaches to Stop Hypertension |
| GWAS | Genome-Wide Association Studies |
| ICD | International Classification of Diseases |
| IQR | Interquartile Range |
| NHS | National Health Service |
| NSAIDs | Non-Steroidal Anti-Inflammatory Drugs |
| PAF | Population Attributable Fraction |
| PRS | Polygenic Risk Score |
| RCT | Randomized Controlled Trial |
| SD | Standard Deviation |
| SNP | Single Nucleotide Polymorphisms |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Umezawa, S.; Higurashi, T.; Komiya, Y.; Arimoto, J.; Horita, N.; Kaneko, T.; Iwasaki, M.; Nakagama, H.; Nakajima, A. Chemoprevention of colorectal cancer: Past, present, and future. Cancer Sci. 2019, 110, 3018–3026. [Google Scholar] [CrossRef] [PubMed]
- Doubeni, C.A.; Fedewa, S.A.; Levin, T.R.; Jensen, C.D.; Saia, C.; Zebrowski, A.M.; Quinn, V.P.; Rendle, K.A.; Zauber, A.G.; Becerra-Culqui, T.A.; et al. Modifiable Failures in the Colorectal Cancer Screening Process and Their Association With Risk of Death. Gastroenterology 2019, 156, 63–74.e6. [Google Scholar] [CrossRef] [Green Version]
- Kaminski, M.F.; Robertson, D.J.; Senore, C.; Rex, D.K. Optimizing the Quality of Colorectal Cancer Screening Worldwide. Gastroenterology 2020, 158, 404–417. [Google Scholar] [CrossRef]
- Katona, B.W.; Weiss, J.M. Chemoprevention of Colorectal Cancer. Gastroenterology 2020, 158, 368–388. [Google Scholar] [CrossRef] [PubMed]
- Friis, S.; Riis, A.H.; Erichsen, R.; Baron, J.A.; Sørensen, H.T. Low-Dose Aspirin or Nonsteroidal Anti-inflammatory Drug Use and Colorectal Cancer Risk: A Population-Based, Case-Control Study. Ann. Intern. Med. 2015, 163, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, J.C.; Jacobs, E.J.; Newton, C.C.; Guinter, M.A.; Cance, W.G.; Campbell, P.T. Associations of Aspirin and Non-Aspirin Non-Steroidal Anti-Inflammatory Drugs With Colorectal Cancer Mortality After Diagnosis. J. Natl. Cancer Inst. 2021, 113, 833–840. [Google Scholar] [CrossRef]
- Tomić, T.; Domínguez-López, S.; Barrios-Rodríguez, R. Non-aspirin non-steroidal anti-inflammatory drugs in prevention of colorectal cancer in people aged 40 or older: A systematic review and meta-analysis. Cancer Epidemiol. 2019, 58, 52–62. [Google Scholar] [CrossRef]
- Lanas, Á.; Carrera-Lasfuentes, P.; Arguedas, Y.; García, S.; Bujanda, L.; Calvet, X.; Ponce, J.; Perez-Aísa, Á.; Castro, M.; Muñoz, M.; et al. Risk of upper and lower gastrointestinal bleeding in patients taking nonsteroidal anti-inflammatory drugs, antiplatelet agents, or anticoagulants. Clin. Gastroenterol. Hepatol. 2015, 13, 906–912.e2. [Google Scholar] [CrossRef]
- Nan, H.; Hutter, C.M.; Lin, Y.; Jacobs, E.J.; Ulrich, C.M.; White, E.; Baron, J.A.; Berndt, S.I.; Brenner, H.; Butterbach, K.; et al. Association of aspirin and NSAID use with risk of colorectal cancer according to genetic variants. JAMA 2015, 313, 1133–1142. [Google Scholar] [CrossRef] [Green Version]
- Jiao, S.; Peters, U.; Berndt, S.; Bezieau, S.; Brenner, H.; Campbell, P.T.; Chan, A.T.; Chang-Claude, J.; Lemire, M.; Newcomb, P.A.; et al. Powerful Set-Based Gene-Environment Interaction Testing Framework for Complex Diseases. Genet. Epidemiol. 2015, 39, 609–618. [Google Scholar] [CrossRef] [Green Version]
- Huyghe, J.R.; Bien, S.A.; Harrison, T.A.; Kang, H.M.; Chen, S.; Schmit, S.L.; Conti, D.V.; Qu, C.; Jeon, J.; Edlund, C.K.; et al. Discovery of common and rare genetic risk variants for colorectal cancer. Nat. Genet. 2019, 51, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Khera, A.V.; Chaffin, M.; Aragam, K.G.; Haas, M.E.; Roselli, C.; Choi, S.H.; Natarajan, P.; Lander, E.S.; Lubitz, S.A.; Ellinor, P.T.; et al. Genome-wide polygenic scores for common diseases identify individuals with risk equivalent to monogenic mutations. Nat. Genet. 2018, 50, 1219–1224. [Google Scholar] [CrossRef] [PubMed]
- Cornish, A.J.; Law, P.J.; Timofeeva, M.; Palin, K.; Farrington, S.M.; Palles, C.; A Jenkins, M.; Casey, G.; Brenner, H.; Chang-Claude, J.; et al. Modifiable pathways for colorectal cancer: A mendelian randomisation analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Kwak, K.; Paek, D.; Zoh, K.E. Exposure to asbestos and the risk of colorectal cancer mortality: A systematic review and meta-analysis. Occup. Environ. Med. 2019, 76, 861–871. [Google Scholar] [CrossRef]
- Zanders, M.M.; Vissers, P.A.; Haak, H.R.; van de Poll-Franse, L.V. Colorectal cancer, diabetes and survival: Epidemiological insights. Diabetes Metab. 2014, 40, 120–127. [Google Scholar] [CrossRef]
- Carr, P.R.; Weigl, K.; Jansen, L.; Walter, V.; Erben, V.; Chang-Claude, J.; Brenner, H.; Hoffmeister, M. Healthy lifestyle factors associated with lower risk of colorectal cancer irrespective of genetic risk. Gastroenterology 2018, 155, 1805–1815.e5. [Google Scholar] [CrossRef]
- Choi, J.; Jia, G.; Wen, W.; Shu, X.O.; Zheng, W. Healthy lifestyles, genetic modifiers, and colorectal cancer risk: A prospective cohort study in the UK Biobank. Am. J. Clin. Nutr. 2021, 113, 810–820. [Google Scholar] [CrossRef]
- Bycroft, C.; Freeman, C.; Petkova, D.; Band, G.; Elliott, L.T.; Sharp, K.; Motyer, A.; Vukcevic, D.; Delaneau, O.; O’Connell, J.; et al. The UK Biobank resource with deep phenotyping and genomic data. Nature 2018, 562, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.; Sakoda, L.C.; Hoffmeister, M.; Rosenthal, E.A.; Lee, J.K.; van Duijnhoven, F.J.; Platz, E.A.; Wu, A.H.; Dampier, C.H.; de la Chapelle, A.; et al. Genome-wide Modeling of Polygenic Risk Score in Colorectal Cancer Risk. Am. J. Hum. Genet. 2020, 107, 432–444. [Google Scholar] [CrossRef]
- Purcell, S.; Neale, B.; Todd-Brown, K.; Thomas, L.; Ferreira, M.A.R.; Bender, D.; Maller, J.; Sklar, P.; de Bakker, P.I.W.; Daly, M.J.; et al. PLINK: A tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 2007, 81, 559–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weigl, K.; Chang-Claude, J.; Knebel, P.; Hsu, L.; Hoffmeister, M.; Brenner, H. Strongly enhanced colorectal cancer risk stratification by combining family history and genetic risk score. Clin. Epidemiol. 2018, 10, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, J.; Du, M.; Schoen, R.E.; Hoffmeister, M.; Newcomb, P.A.; Berndt, S.I.; Caan, B.; Campbell, P.T.; Chan, A.T.; Chang-Claude, J.; et al. Determining Risk of Colorectal Cancer and Starting Age of Screening Based on Lifestyle, Environmental, and Genetic Factors. Gastroenterology 2018, 154, 2152–2164.e19. [Google Scholar] [CrossRef]
- Jiao, L.; Mitrou, P.N.; Reedy, J.; Graubard, B.I.; Hollenbeck, A.R.; Schatzkin, A.; Stolzenberg-Solomon, R. A combined healthy lifestyle score and risk of pancreatic cancer in a large cohort study. Arch. Intern. Med. 2009, 169, 764–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoenfeld, D. Partial residuals for the proportional hazards regression model. Biometrika 1982, 69, 239–241. [Google Scholar] [CrossRef]
- Imamura, F.; O’Connor, L.; Ye, Z.; Mursu, J.; Hayashino, Y.; Bhupathiraju, S.N.; Forouhi, N.G. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. BMJ 2015, 351, h3576. [Google Scholar] [CrossRef] [Green Version]
- Carr, P.R.; Weigl, K.; Edelmann, D.; Jansen, L.; Chang-Claude, J.; Brenner, H.; Hoffmeister, M. Estimation of Absolute Risk of Colorectal Cancer Based on Healthy Lifestyle, Genetic Risk, and Colonoscopy Status in a Population-Based Study. Gastroenterology 2020, 159, 129–138.e9. [Google Scholar] [CrossRef]
- Frampton, M.J.; Law, P.; Litchfield, K.; Morris, E.J.; Kerr, D.; Turnbull, C.; Tomlinson, I.P.; Houlston, R.S. Implications of polygenic risk for personalised colorectal cancer screening. Ann. Oncol. 2016, 27, 429–434. [Google Scholar] [CrossRef]
- Chen, X.; Guo, F.; Hoffmeister, M.; Chang-Claude, J.; Brenner, H. Non-steroidal anti-inflammatory drugs, polygenic risk score and colorectal cancer risk. Aliment. Pharmacol. Ther. 2021, 54, 167–175. [Google Scholar] [CrossRef]
- Drew, D.A.; Cao, Y.; Chan, A.T. Aspirin and colorectal cancer: The promise of precision chemoprevention. Nat. Rev. Cancer 2016, 16, 173–186. [Google Scholar] [CrossRef]
- Cheung, K.S.; Chen, L.; Chan, E.W.; Seto, W.K.; Wong, I.C.K.; Leung, W.K. Nonsteroidal anti-inflammatory drugs but not aspirin are associated with a lower risk of post-colonoscopy colorectal cancer. Aliment. Pharmacol. Ther. 2020, 51, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, C.M.; Bigler, J.; Potter, J.D. Non-steroidal anti-inflammatory drugs for cancer prevention: Promise, perils and pharmacogenetics. Nat. Rev. Cancer 2006, 6, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Seufert, B.L.; Poole, E.M.; Whitton, J.; Xiao, L.; Makar, K.W.; Campbell, P.T.; Kulmacz, R.J.; Baron, J.A.; Newcomb, P.A.; Slattery, M.L.; et al. IkappaBKbeta and NFkappaB1, NSAID use and risk of colorectal cancer in the Colon Cancer Family Registry. Carcinogenesis 2013, 34, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Wang, C.; Dong, H.; Wang, X.; Gao, F.; Zhang, S.; Zhang, X. Aspirin has a better effect on PIK3CA mutant colorectal cancer cells by PI3K/Akt/Raptor pathway. Mol. Med. 2020, 26, 14. [Google Scholar] [CrossRef] [Green Version]
- Arfè, A.; Scotti, L.; Varas-Lorenzo, C.; Nicotra, F.; Zambon, A.; Kollhorst, B.; Schink, T.; Garbe, E.; Herings, R.; Straatman, H.; et al. Non-steroidal anti-inflammatory drugs and risk of heart failure in four European countries: Nested case-control study. BMJ 2016, 354, i4857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNeil, J.J.; Nelson, M.R.; Woods, R.L.; Lockery, J.E.; Wolfe, R.; Reid, C.M.; Kirpach, B.; Shah, R.C.; Ives, D.G.; Storey, E.; et al. Effect of aspirin on all-cause mortality in the healthy elderly. N. Engl. J. Med. 2018, 379, 1519–1528. [Google Scholar] [CrossRef]
- Guo, C.G.; Ma, W.; Drew, D.A.; Cao, Y.; Nguyen, L.H.; Joshi, A.D.; Ng, K.; Ogino, S.; Meyerhardt, J.A.; Song, M.; et al. Aspirin Use and Risk of Colorectal Cancer Among Older Adults. JAMA Oncol. 2021, 7, 428–435. [Google Scholar] [CrossRef]
- Zhang, Y.; Chan, A.T.; Meyerhardt, J.A.; Giovannucci, E.L. Timing of Aspirin Use in Colorectal Cancer Chemoprevention: A Prospective Cohort Study. J. Natl. Cancer Inst. 2021, 113, 841–851. [Google Scholar] [CrossRef]
- Bibbins-Domingo, K.; U.S. Preventive Services Task Force. Aspirin use for the primary prevention of cardiovascular disease and colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2016, 164, 836–845. [Google Scholar] [CrossRef] [Green Version]
- Brenner, H.; Stock, C.; Hoffmeister, M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: Systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ 2014, 348, g2467. [Google Scholar] [CrossRef]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Chadeau-Hyam, M.; Bodinier, B.; Vermeulen, R.; Karimi, M.; Zuber, V.; Castagné, R.; Elliott, J.; Muller, D.; Petrovic, D.; Whitaker, M.; et al. Education, biological ageing, all-cause and cause-specific mortality and morbidity: UK biobank cohort study. EClinicalMedicine 2020, 29, 100658. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Chiuve, S.E.; McCulloguh, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, T.T.; Hu, F.B.; Wu, K.; Chiuve, S.E.; Fuchs, C.S.; Giovannucci, E. The Mediterranean and Dietary Approaches to Stop Hypertension (DASH) diets and colorectal cancer. Am. J. Clin. Nutr. 2010, 92, 1429–1435. [Google Scholar] [CrossRef] [Green Version]
- Tsoi, K.K.; Pau, C.Y.; Wu, W.K.; Chan, F.K.; Griffiths, S.; Sung, J.J. Cigarette smoking and the risk of colorectal cancer: A meta-analysis of prospective cohort studies. Clin. Gastroenterol. Hepatol. 2009, 7, 682–688.e1-5. [Google Scholar] [CrossRef]
- Walter, V.; Jansen, L.; Hoffmeister, M.; Ulrich, A.; Chang-Claude, J.; Brenner, H. Smoking and survival of colorectal cancer patients: Population-based study from Germany. Int. J. Cancer 2015, 137, 1433–1445. [Google Scholar] [CrossRef]
- DeSalvo, K.B.; Olson, R.; Casavale, K.O. Dietary Guidelines for Americans. JAMA 2016, 315, 457–458. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]


{kind=link}
| Characteristics | Incident CRC (n = 2942) No. (%) | Non-Incident CRC (n = 333,075) No. (%) | p Value |
|---|---|---|---|
| Age, mean (SD), years | 60.8 (6.4) | 56.5 (8.0) | <0.001 |
| Male, n (%) | 1752 (59.6) | 157,299 (47.2) | <0.001 |
| Education, n (%) | 0.004 | ||
| Lower qualification | 1522 (51.7) | 163,397 (49.1) | |
| Higher qualification | 1420 (48.3) | 169,678 (50.9) | |
| Household income, n (%), GBP | <0.001 | ||
| <18,000 | 697 (23.7) | 64,805 (19.5) | |
| 18,000–30,999 | 868 (29.5) | 86,547 (26.0) | |
| 31,000–51,999 | 785 (26.7) | 94,591 (28.3) | |
| 52,000–100,000 | 466 (15.8) | 69,973 (21.0) | |
| >100,000 | 126 (4.3) | 17,159 (5.2) | |
| Townsend deprivation index, median (IQR) | −2.4 (−3.8, 0.1) | −2.3 (−3.7, 0.2) | 0.056 |
| Screening history of CRC, n (%) | 730 (24.8) | 88,931 (26.7) | 0.021 |
| Family history of CRC, n (%) | 419 (14.2) | 35,659 (10.7) | <0.001 |
| BMI, n (%), kg/m2 | <0.001 | ||
| 18.5–24.9 | 833 (28.3) | 109,131 (32.7) | |
| 25.0–29.9 | 1333 (45.3) | 143,092 (43.0) | |
| ≥30.0 | 776 (26.4) | 80,852 (24.3) | |
| DASH score, mean (SD) | 23.3 (3.1) | 23.5 (3.1) | 0.008 |
| Smoking, n (%) | <0.001 | ||
| Never or former (<30 pack years) | 2114 (71.9) | 270,906 (81.3) | |
| Current or former (≥30 pack years) | 828 (28.1) | 62,169 (18.7) | |
| Alcohol consumption, n (%), g/day | <0.001 | ||
| 0 | 423 (14.4) | 50,005 (15.0) | |
| Men: 0.1–28; women: 0.1–14 | 1894 (64.4) | 224,262 (67.3) | |
| Men: >28; women: >14 | 625 (21.2) | 58,808 (17.7) | |
| Occupational exposure, n (%) | <0.001 | ||
| Rarely/never | 2335 (79.3) | 274,679 (82.5) | |
| Sometimes | 529 (18.0) | 51,330 (15.4) | |
| Often | 78 (2.7) | 7066 (2.1) | |
| Regular physical activity, n (%) | 1492 (50.7) | 178,243 (53.5) | 0.002 |
| History of type 2 diabetes, n (%) | 220 (7.5) | 16,660 (5.0) | <0.001 |
| Regular use of NSAIDs, n (%) | 765 (26.0) | 109,943 (33.0) | <0.001 |
| Genetic risk category, n (%) | <0.001 | ||
| Low | 293 (10.0) | 66,913 (20.1) | |
| Intermediate | 1668 (56.7) | 199,940 (60.0) | |
| High | 981 (33.3) | 66,222 (19.9) | |
| Environmental risk category, n (%) | <0.001 | ||
| Low | 873 (29.7) | 126,362 (37.9) | |
| Intermediate | 1301 (44.2) | 140,722 (42.3) | |
| High | 768 (26.1) | 65,991 (19.8) |
| No. of Participants | No. of Cases (%) /Person Years | HR (95% CI) b | p Value | p Value for Trend c | |
|---|---|---|---|---|---|
| Genetic risk categories | |||||
| Low | 67,206 | 293 (0.44)/593,593 | 1 [reference] | <0.001 | |
| Intermediate | 201,608 | 1668 (0.83)/1,781,989 | 1.87 (1.65–2.12) | <0.001 | |
| High | 67,203 | 981 (1.46)/572,123 | 3.28 (2.88–3.74) | <0.001 | |
| Environmental risk categories | |||||
| Low | 127,235 | 873 (0.69)/1,125,921 | 1 [reference] | <0.001 | |
| Intermediate | 142,023 | 1301 (0.92)/1,253,727 | 1.20 (1.10–1.31) | <0.001 | |
| High | 66,759 | 768 (1.15)/568,057 | 1.38 (1.25–1.52) | <0.001 | |
| Regular use of NSAIDs | |||||
| No | 225,309 | 2177 (0.97)/1,965,614 | 1 [reference] | -- | |
| Yes | 110,708 | 765 (0.69)/982,091 | 0.64 (0.59–0.70) | <0.001 | |
| Population-attributable fraction (%) | |||||
| Regular use of NSAIDs | 110,708 | 765 (0.69)/982,091 | 1 [reference] | -- | |
| Non-regular use of NSAIDs | 225,309 | 2177 (0.97)/1,965,614 | 21.1 (16.2–25.8) | -- | |
| NSAIDs Use | Genetic Risk | No. of Participants | No. of CRC Incidence (%)/Person Years | HR (95% CI) b | p Value | p Value for Trend c | p Value for Interaction |
|---|---|---|---|---|---|---|---|
| Non-regular use | Low risk | 44,965 | 214 (0.48)/394,384 | 1 [reference] | <0.001 | 0.190 | |
| Non-regular use | Intermediate risk | 135,159 | 1223 (0.90)/1,187,550 | 1.86 (1.61–2.15) | <0.001 | ||
| Non-regular use | High risk | 45,185 | 740 (1.64)/383,680 | 3.33 (2.86–3.88) | <0.001 | ||
| Regular use | Low risk | 22,241 | 79 (0.36)/199,209 | 1 [reference] | <0.001 | ||
| Regular use | Intermediate risk | 66,449 | 445 (0.67)/594,439 | 1.85 (1.46–2.35) | <0.001 | ||
| Regular use | High risk | 22,018 | 241 (1.09)/188,443 | 3.03 (2.35–3.90) | <0.001 | ||
| NSAIDs Use | Environmental Risk | No. of Participants | No. of CRC Incidence (%)/Person Years | HR (95% CI) b | p Value | p Value for Trend c | p Value for Interaction |
|---|---|---|---|---|---|---|---|
| Non-regular use | Low risk | 85,610 | 639 (0.75)/753,254 | 1 [reference] | <0.001 | 0.740 | |
| Non-regular use | Intermediate risk | 94,743 | 942 (0.99)/829,898 | 1.25 (1.11–1.42) | 0.001 | ||
| Non-regular use | High risk | 44,956 | 596 (1.33)/382,462 | 1.46 (1.23–1.74) | <0.001 | ||
| Regular use | Low risk | 41,625 | 234 (0.56)/372,667 | 1 [reference] | 0.249 | ||
| Regular use | Intermediate risk | 47,280 | 359 (0.76)/423,829 | 1.25 (0.91–1.71) | 0.169 | ||
| Regular use | High risk | 21,803 | 172 (0.79)/185,595 | 1.29 (1.03–1.62) | 0.027 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, J.; Zhang, P.; Li, Z.; Zhang, X.; Zhong, W.; Song, W.; Wang, X.; Gao, P.; Mao, C. Association of Non-Steroidal Anti-Inflammatory Drugs, Genetic Risk, and Environmental Risk Factors with Incidence of Colorectal Cancer. Cancers 2022, 14, 5138. https://doi.org/10.3390/cancers14205138
Ren J, Zhang P, Li Z, Zhang X, Zhong W, Song W, Wang X, Gao P, Mao C. Association of Non-Steroidal Anti-Inflammatory Drugs, Genetic Risk, and Environmental Risk Factors with Incidence of Colorectal Cancer. Cancers. 2022; 14(20):5138. https://doi.org/10.3390/cancers14205138
Chicago/Turabian StyleRen, Jiaojiao, Peidong Zhang, Zhihao Li, Xiru Zhang, Wenfang Zhong, Weiqi Song, Xing Wang, Pingming Gao, and Chen Mao. 2022. "Association of Non-Steroidal Anti-Inflammatory Drugs, Genetic Risk, and Environmental Risk Factors with Incidence of Colorectal Cancer" Cancers 14, no. 20: 5138. https://doi.org/10.3390/cancers14205138