
Oral Contraceptive Use and Breast Cancer Risk for BRCA1 and BRCA2 Mutation Carriers: Systematic Review and Meta-Analysis of Case–Control Studies

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Quality Assessment
2.3. Statistical Analysis
3. Results
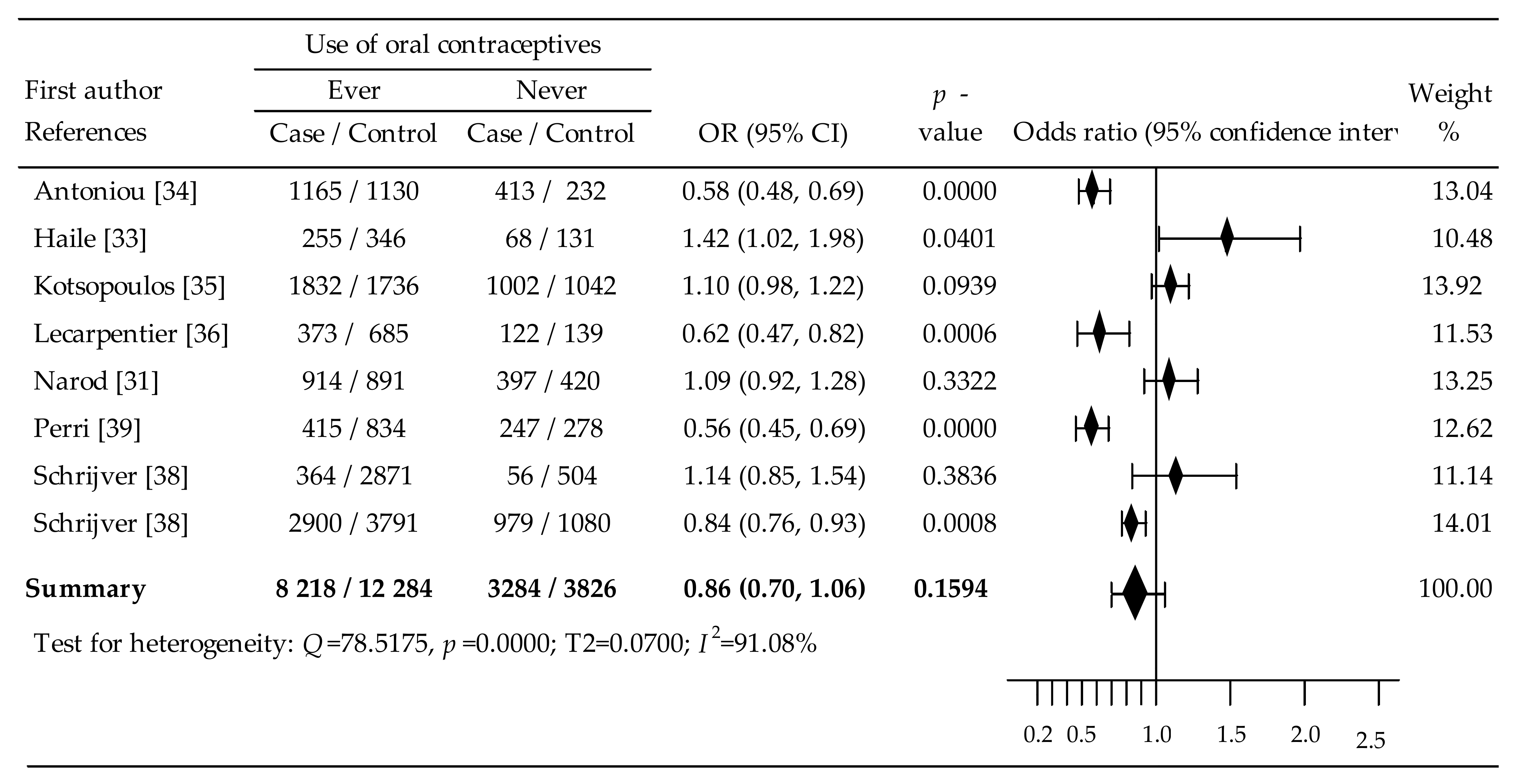
3.1. Oral Contraceptives and Breast Cancer in BRCA1/2 Mutation Carriers
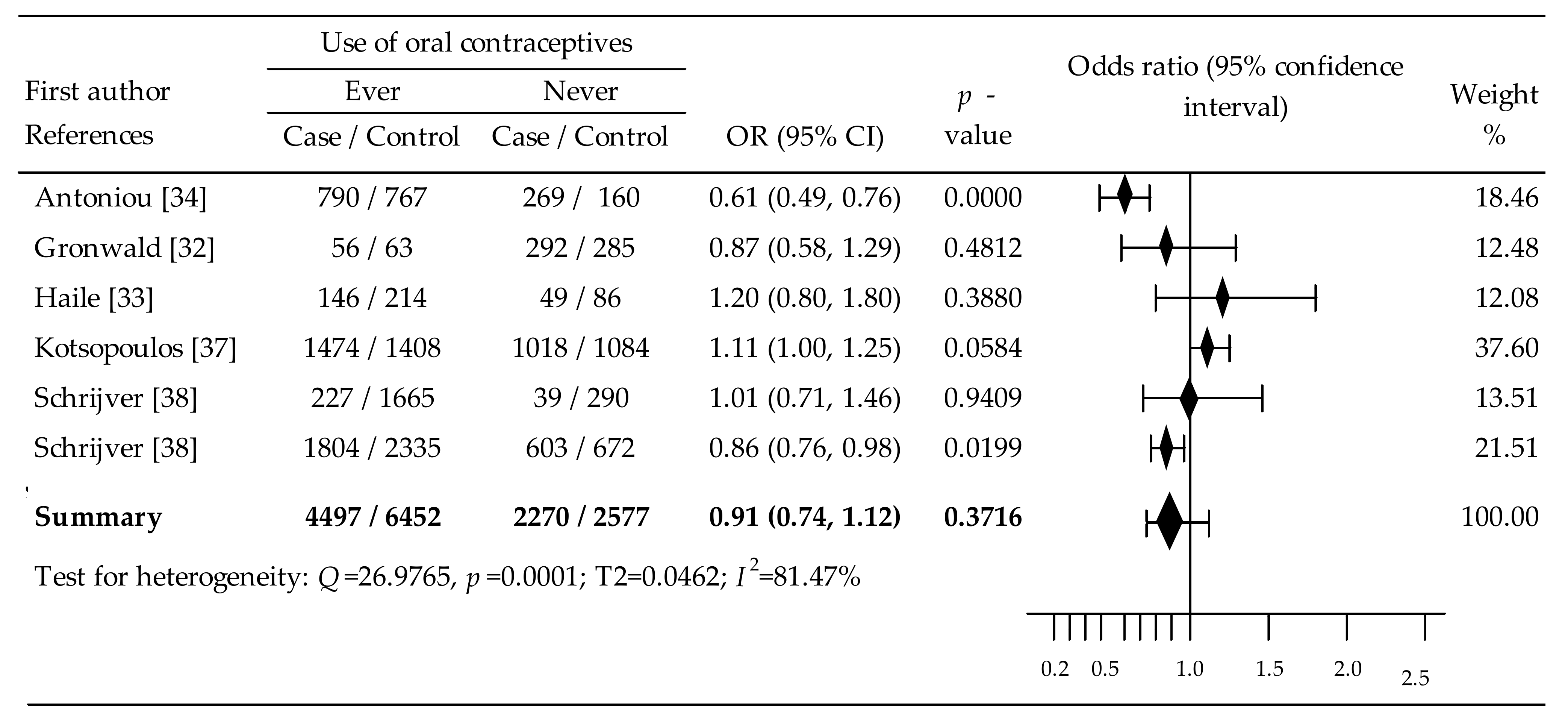
3.2. Oral Contraceptives and Breast Cancer in BRCA1 Mutation Carriers
3.3. Oral Contraceptives and Breast Cancer in BRCA2 Mutation Carriers
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, S.; Piatti, P.; Motto, M.; Rossi, V. Chromatin and DNA modifications in the Opaque2-mediated regulation of gene transcription during maize endosperm development. Plant Cell 2009, 21, 1410–1427. [Google Scholar] [CrossRef] [PubMed]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.-A.; Mooij, T.M.; Roos-Blom, M.-J.; Jervis, S.; Van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef]
- Shiovitz, S.; Korde, L.A. Genetics of breast cancer: A topic in evolution. Ann. Oncol. 2015, 26, 1291–1299. [Google Scholar] [CrossRef]
- Angeli, D.; Salvi, S.; Tedaldi, G. Genetic Predisposition to Breast and Ovarian Cancers: How Many and Which Genes to Test? Int. J. Mol. Sci. 2020, 21, 1128. [Google Scholar] [CrossRef]
- Lenoir, G.M. Familial breast-ovarian cancer locus on chromosome 17q12-q23. Lancet 1991, 338, 82–83. [Google Scholar] [CrossRef]
- Wooster, R.; Neuhausen, S.L.; Mangion, J.; Quirk, Y.; Ford, D.; Collins, N.; Nguyen, K.; Seal, S.; Tran, T.; Averill, D.; et al. Localization of a Breast Cancer Susceptibility Gene, BRCA2, to Chromosome 13q12-13. Science 1994, 265, 2088–2090. [Google Scholar] [CrossRef]
- Yoshida, K.; Miki, Y. Role of BRCA1 and BRCA2 as regulators of DNA repair, transcription, and cell cycle in response to DNA damage. Cancer Sci. 2004, 95, 866–871. [Google Scholar] [CrossRef]
- Fu, X.; Tan, W.; Song, Q.; Pei, H.; Li, J. BRCA1 and Breast Cancer: Molecular Mechanisms and Therapeutic Strategies. Front. Cell Dev. Biol. 2022, 10, 813457. [Google Scholar] [CrossRef]
- Chen, S.; Parmigiani, G. Meta-Analysis of BRCA1 and BRCA2 Penetrance. J. Clin. Oncol. 2007, 25, 1329–1333. [Google Scholar] [CrossRef]
- Baretta, Z.; Mocellin, S.; Goldin, E.; Olopade, O.I.; Huo, D. Effect of BRCA germline mutations on breast cancer prognosis. Medicine 2016, 95, e4975. [Google Scholar] [CrossRef]
- Liu, M.; Xie, F.; Liu, M.; Zhang, Y.; Wang, S. Association between BRCA mutational status and survival in patients with breast cancer: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2021, 186, 591–605. [Google Scholar] [CrossRef]
- Sekine, M.; Nishino, K.; Enomoto, T. Differences in Ovarian and Other Cancers Risks by Population and BRCA Mutation Location. Genes 2021, 12, 1050. [Google Scholar] [CrossRef]
- Doren, A.; Vecchiola, A.; Aguirre, B.; Villaseca, P. Gynecological–endocrinological aspects in women carriers of BRCA1/2 gene mutations. Climacteric 2018, 21, 529–535. [Google Scholar] [CrossRef]
- Kotsopoulos, J.; Lubinski, J.; Salmena, L.; Lynch, H.T.; Kim-Sing, C.; Foulkes, W.D.; Ghadirian, P.; Neuhausen, S.L.; Demsky, R.; Tung, N.; et al. Breastfeeding and the risk of breast cancer in BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. 2012, 14, R42. [Google Scholar] [CrossRef]
- Rieder, V.; Salama, M.; Glöckner, L.; Muhr, D.; Berger, A.; Tea, M.-K.; Pfeiler, G.; Rappaport-Fuerhauser, C.; Gschwantler-Kaulich, D.; Weingartshofer, S.; et al. Effect of lifestyle and reproductive factors on the onset of breast cancer in female BRCA 1 and 2 mutation carriers. Mol. Genet. Genom. Med. 2015, 4, 172–177. [Google Scholar] [CrossRef]
- Momenimovahed, Z.; Salehiniya, H. Epidemiological characteristics of and risk factors for breast cancer in the world. Breast Cancer Targets Ther. 2019, 11, 151–164. [Google Scholar] [CrossRef]
- Kanadys, W.; Barańska, A.; Malm, M.; Błaszczuk, A.; Polz-Dacewicz, M.; Janiszewska, M.; Jędrych, M. Use of Oral Contraceptives as a Potential Risk Factor for Breast Cancer: A Systematic Review and Meta-Analysis of Case-Control Studies Up to 2010. Int. J. Environ. Res. Public Health 2021, 18, 4638. [Google Scholar] [CrossRef]
- Barańska, A.; Błaszczuk, A.; Kanadys, W.; Malm, M.; Drop, K.; Polz-Dacewicz, M. Oral Contraceptive Use and Breast Cancer Risk Assessment: A Systematic Review and Meta-Analysis of Case-Control Studies, 2009–2020. Cancers 2021, 13, 5654. [Google Scholar] [CrossRef]
- Iodice, S.; Barile, M.; Rotmensz, N.; Feroce, I.; Bonanni, B.; Radice, P.; Bernard, L.; Maisonneuve, P.; Gandini, S. Oral contraceptive use and breast or ovarian cancer risk in BRCA1/2 carriers: A meta-analysis. Eur. J. Cancer 2010, 46, 2275–2284. [Google Scholar] [CrossRef]
- Friebel, T.M.; Domchek, S.M.; Rebbeck, T.R. Modifiers of Cancer Risk in BRCA1 and BRCA2 Mutation Carriers: Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2014, 106, dju091. [Google Scholar] [CrossRef]
- Schrijver, L.H.; Mooij, T.M.; Pijpe, A.; Sonke, G.S.; Mourits, E.M.J.; Andrieu, N.; Antoniou, A.C.; Easton, D.F.; Engel, C.; Goldgar, D.; et al. Oral Contraceptive Use in BRCA1 and BRCA2 Mutation Carriers: Absolute Cancer Risks and Benefits. JNCI J. Natl. Cancer Inst. 2022, 114, 540–552. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley and Sons, Ltd.: Chichester, UK, 2019; pp. 143–176. [Google Scholar]
- Narod, S.A.; Dubé, M.-P.; Klijn, J.; Lubinski, J.; Lynch, H.T.; Ghadirian, P.; Provencher, D.; Heimdal, K.; Moller, P.; Robson, M.; et al. Oral Contraceptives and the Risk of Breast Cancer in BRCA1 and BRCA2 Mutation Carriers. JNCI J. Natl. Cancer Inst. 2002, 94, 1773–1779. [Google Scholar] [CrossRef]
- Gronwald, J.; Byrski, T.; Huzarski, T.; Cybulski, C.; Sun, P.; Tulman, A.; Narod, S.A.; Lubinski, J. Influence of selected lifestyle factors on breast and ovarian cancer risk in BRCA1 mutation carriers from Poland. Breast Cancer Res. Treat. 2005, 95, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Haile, R.W.; Thomas, D.C.; McGuire, V.; Felberg, A.; John, E.M.; Milne, R.L.; Hopper, J.L.; Jenkins, M.A.; Levine, A.J.; Daly, M.M.; et al. BRCA1 and BRCA2 mutation carriers, oral contraceptive use, and breast cancer before age 50. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1863–1870. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, A.C.; Rookus, M.; Andrieu, N.; Brohet, R.; Chang-Claude, J.; Peock, S.; Cook, M.; Evans, D.G.; Eeles, R.; Nogues, C.; et al. Reproductive and Hormonal Factors, and Ovarian Cancer Risk for BRCA1 and BRCA2 Mutation Carriers: Results from the International BRCA1/2 Carrier Cohort Study. Cancer Epidemiol. Biomark. Prev. 2009, 18, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Kotsopoulos, J.; Lubinski, J.; Lynch, H.T.; Kim-Sing, C.; Neuhausen, S.; Demsky, R.; Foulkes, W.D.; Ghadirian, P.; Tung, N.; Ainsworth, P.; et al. Oophorectomy after Menopause and the Risk of Breast Cancer in BRCA1 and BRCA2 Mutation Carriers. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1089–1096. [Google Scholar] [CrossRef]
- LeCarpentier, J.; Noguès, C.; Mouret-Fourme, E.; Gauthier-Villars, M.; Lasset, C.; Fricker, J.-P.; Caron, O.; Stoppa-Lyonnet, M.; Berthet, P.; Faivre, L.; et al. Variation in breast cancer risk associated with factors related to pregnancies according to truncating mutation location, in the French National BRCA1 and BRCA2 mutations carrier cohort (GENEPSO). Breast Cancer Res. 2012, 14, R99. [Google Scholar] [CrossRef]
- Kotsopoulos, J.; Lubinski, J.; Moller, P.; Lynch, H.T.; Singer, C.F.; Eng, C.; Neuhausen, S.L.; Karlan, B.; Kim-Sing, C.; Huzarski, T.; et al. Timing of oral contraceptive use and the risk of breast cancer in BRCA1 mutation carriers. Breast Cancer Res. Treat. 2014, 143, 579–586. [Google Scholar] [CrossRef]
- Schrijver, L.H.; Olsson, H.; Phillips, K.-A.; Terry, M.B.; Goldgar, E.D.; Kast, K.; Engel, C.; Mooij, T.M.; Adlard, J.; Barrowdale, D.; et al. Oral Contraceptive Use and Breast Cancer Risk: Retrospective and Prospective Analyses From a BRCA1 and BRCA2 Mutation Carrier Cohort Study. JNCI Cancer Spectr. 2018, 2, pky023. [Google Scholar] [CrossRef]
- Perri, T.; Naor-Revel, S.; Eliassi-Revivo, P.; Lifshitz, D.; Friedman, E.; Korach, J. Fertility treatments and breast cancer risk in Jewish Israeli BRCA mutation carriers. Fertil. Steril. 2021, 116, 538–545. [Google Scholar] [CrossRef]
- Brohet, R.M.; Goldgar, D.E.; Easton, D.F.; Antoniou, A.C.; Andrieu, N.; Chang-Claude, J.; Peock, S.; Eeles, R.A.; Cook, M.; Chu, C.; et al. Oral Contraceptives and Breast Cancer Risk in the International BRCA1/2 Carrier Cohort Study: A Report From EMBRACE, GENEPSO, GEO-HEBON, and the IBCCS Collaborating Group. J. Clin. Oncol. 2007, 25, 3831–3836. [Google Scholar] [CrossRef]
- Moorman, P.G.; Havrilesky, L.J.; Gierisch, J.M.; Coeytaux, R.R.; Lowery, W.J.; Urrutia, R.P.; Dinan, M.; McBroom, A.J.; Hasselblad, V.; Sanders, G.D.; et al. Oral Contraceptives and Risk of Ovarian Cancer and Breast Cancer Among High-Risk Women: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2013, 31, 4188–4198. [Google Scholar] [CrossRef]
- Huber, D.; Seitz, S.; Kast, K.; Emons, G.; Ortmann, O. Use of oral contraceptives in BRCA mutation carriers and risk for ovarian and breast cancer: A systematic review. Arch. Gynecol. Obstet. 2020, 301, 875–884. [Google Scholar] [CrossRef]
- Britt, K.L.; Cuzick, J.; Phillips, K.-A. Key steps for effective breast cancer prevention. Nat. Cancer 2020, 20, 1–20. [Google Scholar] [CrossRef]
- Renehan, A.G.; Pegington, M.; Harvie, M.N.; Sperrin, M.; Astley, S.M.; Brentnall, A.R.; Howell, A.; Cuzick, J.; Evans, D.G. Young adulthood body mass index, adult weight gain and breast cancer risk: The PROCAS Study (United Kingdom). Br. J. Cancer 2020, 122, 1552–1561. [Google Scholar] [CrossRef]
- Munsell, M.F.; Sprague, B.L.; Berry, D.A.; Chisholm, G.; Trentham-Dietz, A. Body Mass Index and Breast Cancer Risk According to Postmenopausal Estrogen-Progestin Use and Hormone Receptor Status. Epidemiol. Rev. 2014, 36, 114–136. [Google Scholar] [CrossRef]
- Seitz, H.K.; Pelucchi, C.; Bagnardi, V.; La Vecchia, C. Epidemiology and Pathophysiology of Alcohol and Breast Cancer: Update 2012. Alcohol Alcohol. 2012, 47, 204–212. [Google Scholar] [CrossRef]
- Neilson, H.K.; Farris, M.S.; Stone, C.R.; Vaska, M.M.; Brenner, D.R.; Friedenreich, C.M. Moderate–vigorous recreational physical activity and breast cancer risk, stratified by menopause status: A systematic review and meta-analysis. Menopause 2017, 24, 322–344. [Google Scholar] [CrossRef]
- Łukasiewicz, S.; Czeczelewski, M.; Forma, A.; Baj, J.; Sitarz, R.; Stanisławek, A. Breast Cancer—Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies—An Updated Review. Cancers 2021, 13, 4287. [Google Scholar] [CrossRef]
- Tremont, A.; Lu, J.; Cole, J.T. Endocrine Therapy for Early Breast Cancer: Updated Review. Ochsner J. 2017, 17, 405–411. [Google Scholar]
- Mayer, E.L.; Burstein, H.J. Postmenopausal breast cancer: A best endocrine strategy? Lancet 2015, 386, 1317–1319. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in early breast cancer: Patient-level meta-analysis of the randomised trials. Lancet 2015, 386, 1341–1352. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Autor Pub Year [Ref.] | Study Name Setting | Study Year | Study Populations of Mutation Carriers Cancer N (n, %) Unaffected N (n, %) | NOS Scale |
|---|---|---|---|---|
| Narod et al. 2002 [31] | International study 11 countries a | 1977–2001 | Cases: 1311 BRCA1/2 (69.7) Controls: 1311 BRCA1/2 (68.0) | 5 |
| Gronwald et al. 2006 [32] | Poland | 1988–2005 | Cases: 348 BRCA1 (16.1) Controls: 348 BRCA1 (18.1) | 8 |
| Haile et al. 2006 [33] | Australia, Canada, USA and Utah | Cases: 195 BRCA1 (74.9); 128 BRCA2 (85.2) Controls: 302 BRCA1 (70.9);179 BRCA2 (73.4) | 6 | |
| Anatoniou et al. 2009 [34] | IBCCS 15 countries b | 1997–2005 | Cases: 1100 BRCA1 (71.2); 531 BRCA2 (70.6) Controls: 970 BRCA1 (79.1); 455 BRCA2 (79.8) | 6 |
| Kotsopoulos et al. 2012 [35] | International 5 countries c | Cases: 2584 BRCA1/2 (64.6) Controls: 2584 BRCA1/2 (63.3) | 7 | |
| Lecarpentier et al. 2012 [36] | GEBESPO France | 2000–2010 | Cases: 499 BRCA1/2 (74.7) Controls: 838 BRCA1/2 (81.7) | 8 |
| Kotsopoulos et al. 2014 [37] | HBCCSG 13 countries d | Cases: 2,492 BRCA1 (59.2) Controls: 2,492 BRCA1 (56.5) | ||
| Schrijver 2018 [38] | EMBRACE, BCFR, IBCCS, kConFab, Othere 14 countries e | a. Prospective cohort: Cases: 2,544 BRCA1 (71.5); 1,560 BRCA2 (70.9) Controls: 3,163 BRCA1 (77.4); 1,965 BRCA2 (73.9) b. Retrospective full cohort: Cases: 269 BRCA1 (84.0); 157 BRCA2 (86.6) Controls: 2,007 BRCA1 (82.7); 1.453 BRCA2 (82.7) | 8 | |
| Perri et al. 2021 [39] | Israel | 1995–2019 | Case: 687 BRCA1/2 (64.0) Controls: 1,137 BRCA1/2 (75.5) | 8 |
| Subgroup | n | OR | 95% CI | p | I2 (%) | Begg’s Test | Egger’s Test | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcoms | Tau-b | Z | p | b0 | 95% CI | T | p | |||||
| BRCA1/2 carriers mutations | ||||||||||||
| Oral contraceptives (OCs) use [31,33,34,35,36,38,39] | ||||||||||||
| Ever | 8 | 0.86 | 0.70 to 1.06 | 0.159 | 91.08 | 1.000 | 2.038 | 0.041 | −1.205 | −8.955 to 6.545 | −0.380 | 0.717 |
| Never | 8 | Referent | ||||||||||
| Age at first use the OCs [33,38] | ||||||||||||
| <20 years | 3 | 1.06 | 0.70 to 1.60 | 0.798 | 87.90 | Inaccessible | 4.492 | −6.114 to 15.099 | 5.382 | 0.117 | ||
| ≥20 years | 3 | 1.21 | 1.07 to 1.36 | 0.002 | 0.00 | 1.000 | 1.567 | 0.117 | 1.206 | −1.0270 to 3.438 | 6.862 | 0.092 |
| <20 years/≥20 years | 3 | 0.81 | 0.60 to 1.08 | 0.154 | 77.92 | Inaccessible | 3.777 | −6.130 to 13.684 | 4.844 | 0.130 | ||
| Duration of OCs use [33,34,38] | ||||||||||||
| ≥5 years | 4 | 0.84 | 0.67 to 1.06 | 0.149 | 71.55 | Inaccessible | 2.244 | −8.367 to 12.855 | 0.910 | 0.459 | ||
| <5 years | 4 | 0.94 | 0.67 to 1.33 | 0.723 | 90.23 | Inaccessible | 3.487 | −12.020 to 18.994 | 0.967 | 0.435 | ||
| ≥5 years/<5 years | 4 | 1.05 | 0.86 to 1.27 | 0.655 | 73.91 | Inaccessible | 3.348 | −7.767 to 14.464 | 1.296 | 0.324 | ||
| Years since last use of OCs prior to diagnosis [33,38] | ||||||||||||
| <10 years | 3 | 0.92 | 0.65 to 1.29 | 0.623 | 80.01 | Inaccessible | 3.579 | −0.597 to 12.755 | 4.956 | 0.127 | ||
| ≥10 years | 3 | 1.27 | 0.84 to 1.29 | 0.249 | 85.60 | Inaccessible | 4.3770 | −7.437 to 16.19 | 4.708 | 0.133 | ||
| <10 years/≥10 years | 3 | 0.75 | 0.68 to 0.83 | 0.000 | 0.00 | −1.000 | −1.567 | 0.117 | −1.050 | −7.761 to 5.660 | −1.989 | 0.297 |
| BRCA1 carriers mutations | ||||||||||||
| Oral contraceptives (OCs) use [32,33,34,37,38] | ||||||||||||
| Ever | 6 | 0.90 | 0.75 to 1.10 | 0.359 | 79.36 | 0.667 | 1.359 | 0.174 | −0.756 | −6.507 to 4.995 | −0.365 | 0.733 |
| Never | 6 | Referent | ||||||||||
| Age at first use the OCs [33,37,38] | ||||||||||||
| <20 years | 4 | 1.02 | 0.77 to 1.35 | 0.880 | 84.45 | Inaccessible | 1.284 | −13.214 to 15.782 | 0.381 | 0.740 | ||
| ≥20 years | 4 | 1.28 | 1.04 to 1.57 | 0.019 | 62.00 | Inaccessible | −1.420 | −9.347 to 6.506 | −0.771 | 0.521 | ||
| <20 years/≥20 years | 4 | 0.78 | 0.69 to 0.89 | 0.000 | 27.10 | 0.667 | 1.359 | 0.174 | 1.967 | −2.548 to 6.482 | 1.874 | 0.202 |
| Duration of OCs use [33,34,37,38] | ||||||||||||
| <5 years | 5 | 0.85 | 0.70 to 1.04 | 0.115 | 67.86 | 0.333 | 0.522 | 0.601 | −1.140 | −7.653 to 5.373 | −0.557 | 0.616 |
| ≥5 years | 5 | 0.90 | 0.74 to 1.10 | 0.298 | 75.60 | 1.000 | 1.567 | 0.117 | 0.499 | −7.157 to 8.156 | 0.208 | 0.849 |
| ≥5 years/<5 years | 5 | 1.03 | 0.91 to 1.16 | 0.653 | 36.70 | 0.600 | 1.470 | 0.142 | 1.927 | −2.732 to 6.587 | 1.316 | 0.280 |
| Years since last use of OCs prior to diagnosis [33,37,38] | ||||||||||||
| <10 years | 4 | 0.84 | 0.74 to 0.96 | 0.009 | 11.61 | Inaccessible | 1.740 | −2.004 to 5.484 | 1.999 | 0.184 | ||
| ≥10 years | 4 | 1.08 | 0.90 to 1.31 | 0.394 | 63.25 | Inaccessible | 1.326 | −6.600 to 9.252 | 0.720 | 0.546 | ||
| <10 years/≥10 years | 4 | 0.83 | 0.73 to 0.93 | 0.002 | 11.19 | −1.000 | −2.038 | 0.041 | −1.711 | −6.826 to 3.403 | −1.440 | 0.287 |
| BRCA2 carriers mutation | ||||||||||||
| Oral contraceptives (OCs) use [33,34,38] | ||||||||||||
| Ever | 4 | 0.98 | 0.62 to 1.55 | 0.924 | 85.51 | Inaccessible | 0.733 | −10.121 to 14.662 | 0.788 | 0.513 | ||
| Never | 4 | Referent | ||||||||||
| Age at first use the OCs [33,38] | ||||||||||||
| <20 years | 3 | 1.23 | 0.61 to 2.50 | 0.563 | 87.41 | Inaccessible | 4.192 | −7.113 to 15.498 | 4.712 | 0.133 | ||
| ≥20 years | 3 | 1.42 | 1.04 to 1.93 | 0.027 | 30.59 | Inaccessible | 1.892 | −4.307 to 8.092 | 3.878 | 0.161 | ||
| <20 years/>−20 years | 3 | 0.76 | 0.50 to 1.14 | 0.187 | 73.79 | Inaccessible | 3.109 | −20.053 to 26.272 | 1.706 | 0.338 | ||
| Duration of OCs use [33,34,38] | ||||||||||||
| <5 years | 4 | 0.93 | 0.63 to 1.36 | 0.709 | 71.21 | Inaccessible | 2.115 | −7.863 to 12.094 | 0.912 | 0.458 | ||
| ≥5 years | 4 | 0.98 | 0.59 to 1.63 | 0.936 | 86.33 | Inaccessible | 3.106 | 8.484 to 14.696 | 1.153 | 0.368 | ||
| ≥5 years/<5 years | 4 | 0.94 | 0.74 to 1.20 | 0.635 | 56.69 | 1.000 | 1.567 | 0.117 | 3.034 | −4.326 to 10.394 | 1.774 | 0.218 |
| Years since last use of OCs prior to diagnosis [33,38] | ||||||||||||
| <10 years | 3 | 1,00 | 0.51 to 1.96 | 0.995 | 83.93 | Inaccessible | 3.663 | −14.208 to 21.534 | 2.604 | 0.233 | ||
| ≥10 years | 3 | 1.46 | 0.83 to 2.57 | 0.187 | 77.67 | Inaccessible | 3.393 | 0.990 to 5.796 | 17.941 | 0.035 | ||
| <10 years/≥10 years | 3 | 0.65 | 0.55 to 0.76 | 0.000 | 0.00 | 0.333 | 0.522 | 0.601 | 0.534 | −16.921 to 17.990 | 0.389 | 0.764 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barańska, A.; Kanadys, W. Oral Contraceptive Use and Breast Cancer Risk for BRCA1 and BRCA2 Mutation Carriers: Systematic Review and Meta-Analysis of Case–Control Studies. Cancers 2022, 14, 4774. https://doi.org/10.3390/cancers14194774
Barańska A, Kanadys W. Oral Contraceptive Use and Breast Cancer Risk for BRCA1 and BRCA2 Mutation Carriers: Systematic Review and Meta-Analysis of Case–Control Studies. Cancers. 2022; 14(19):4774. https://doi.org/10.3390/cancers14194774
Chicago/Turabian StyleBarańska, Agnieszka, and Wiesław Kanadys. 2022. "Oral Contraceptive Use and Breast Cancer Risk for BRCA1 and BRCA2 Mutation Carriers: Systematic Review and Meta-Analysis of Case–Control Studies" Cancers 14, no. 19: 4774. https://doi.org/10.3390/cancers14194774