
Characteristics and Outcomes of Adult Patients in the PETHEMA Registry with Relapsed or Refractory FLT3-ITD Mutation-Positive Acute Myeloid Leukemia

 , , , , , , , , , , ,
, , , , , , , , , , ,  ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Main Inclusion Criteria
2.3. Data Extraction
2.4. Treatment Schedules
2.5. Endpoints and Outcome Measures
2.6. Statistical Analyses
3. Results
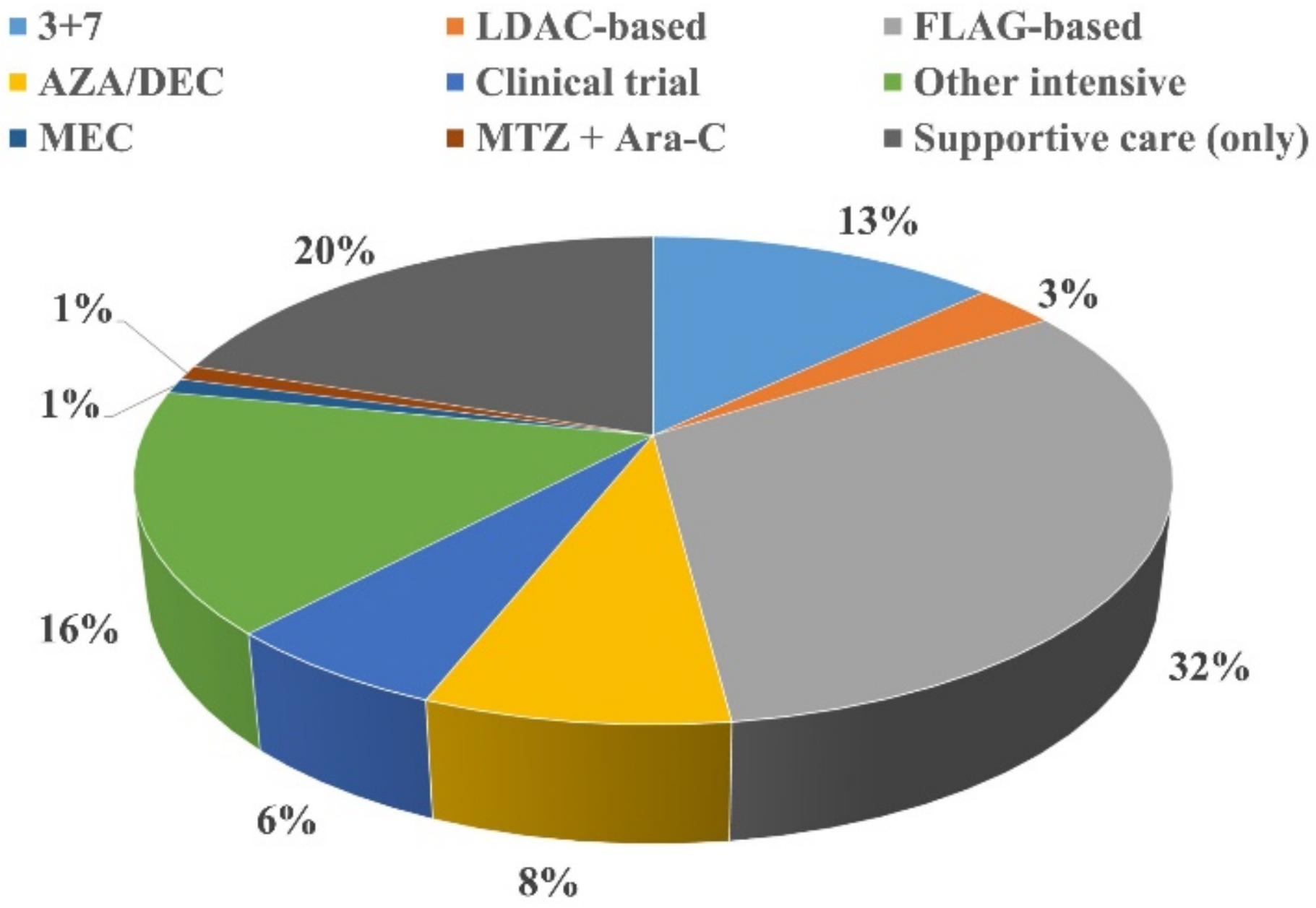
3.1. First-Line Therapy
3.2. Salvage Therapy
3.3. Stem Cell Transplantation in Second-Line Therapy
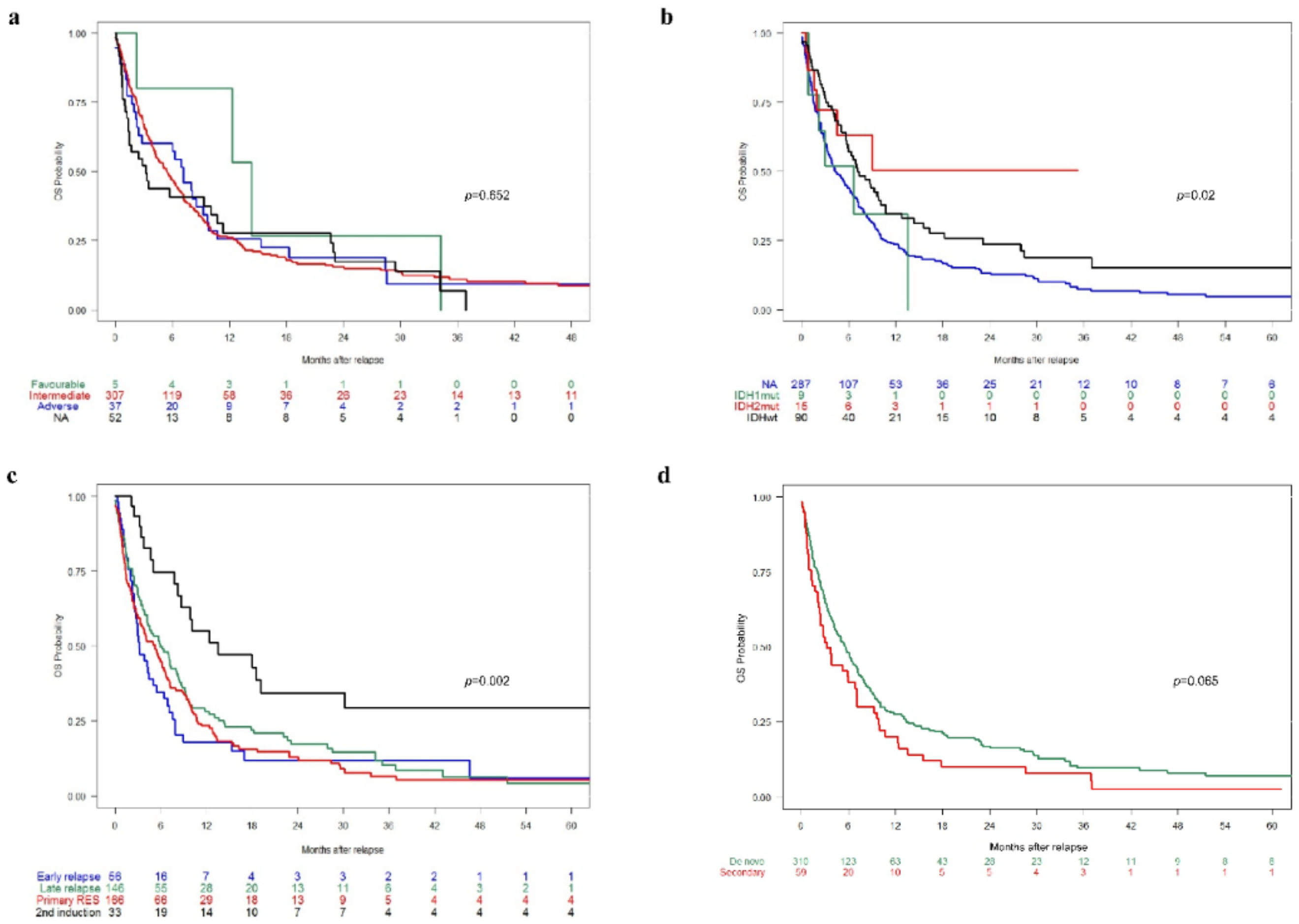
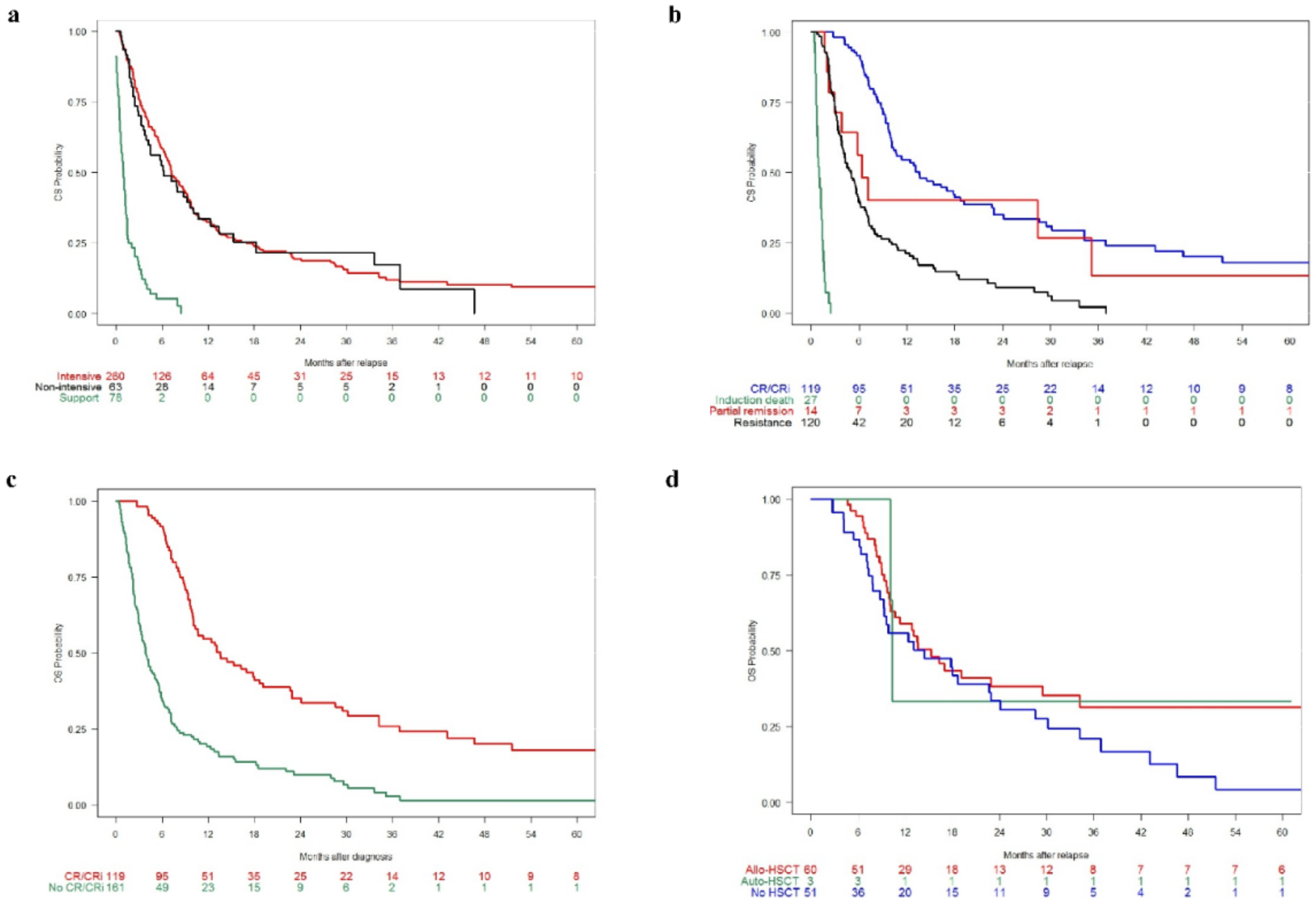
3.4. Survival Analysis
Multivariate Analysis of Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Döhner, H.; Estey, E.H.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Burnett, A.K.; Dombret, H.; Fenaux, P.; Grimwade, D.; Larson, R.A.; et al. Diagnosis and management of acute myeloid leukemia in adults: Recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood 2010, 115, 453–474. [Google Scholar] [CrossRef] [PubMed]
- Forman, S.J.; Rowe, J.M. The myth of the second remission of acute leukemia in the adult. Blood 2013, 121, 1077–1082. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, F.; Lessi, F.; Vitagliano, O.; Birkenghi, E.; Rossi, G. Current therapeutic results and treatment options for older patients with relapsed acute myeloid leukemia. Cancers 2019, 11, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [Green Version]
- Fey, M.F.; Buske, C.; ESMO Guidelines Working Group. Acute myeloblastic leukaemias in adult patients: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi138–vi143. [Google Scholar] [CrossRef] [PubMed]
- Ossenkoppele, G.J.; Stussi, G.; Maertens, J.; van Montfort, K.; Biemond, B.J.; Breems, D.; Ferrant, A.; Graux, C.; de Greef, G.E.; Halkes, C.J.; et al. Addition of bevacizumab to chemotherapy in acute myeloid leukemia at older age: A randomized phase 2 trial of the Dutch-Belgian Cooperative Trial Group for Hemato-Oncology (HOVON) and the Swiss Group for Clinical Cancer Research (SAKK). Blood 2012, 120, 4706–4711. [Google Scholar] [CrossRef] [Green Version]
- Popescu, B.; Sheela, S.; Thompson, J.; Grasmeder, S.; Intrater, T.; DeStefano, C.B.; Hourigan, C.S.; Lai, C. Timed sequential salvage chemotherapy for relapsed or refractory acute myeloid leukemia. Clin. Hematol. Int. 2020, 2, 27–31. [Google Scholar] [CrossRef] [Green Version]
- National Comprehensive Cancer Network. Acute Myeloid Leukemia. Version 3.2020. 2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/aml.pdf (accessed on 19 February 2020).
- Daver, N.; Schlenk, R.F.; Russell, N.H.; Levis, M.J. Targeting FLT3 mutations in AML: Review of current knowledge and evidence. Leukemia 2019, 33, 299–312. [Google Scholar] [CrossRef] [Green Version]
- Astellas Pharma Europe B.V. Xospata 40 mg Film-Coated Tablets: Summary of Product Characteristics. 2019. Available online: https://www.ema.europa.eu/en/documents/product-information/xospata-epar-product-information_en.pdf (accessed on 19 February 2020).
- Astellas Pharma US Inc. XOSPATA® (Gilteritinib) Tablets, for Oral Use: Highlights of Prescribing Information. 2018. Available online: https://www.astellas.com/us/system/files/xospata.pdf (accessed on 19 February 2020).
- Cortes, J.E.; Khaled, S.; Martinelli, G.; Perl, A.E.; Ganguly, S.; Russell, N.; Kramer, A.; Dombret, H.; Hogge, D.; Jonas, B.A.; et al. Quizartinib versus salvage chemotherapy in relapsed or refractory FLT3-ITD acute myeloid leukaemia (QuANTUM-R): A multicentre, randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 984–997. [Google Scholar] [CrossRef]
- Perl, A.E.; Martinelli, G.; Cortes, J.E.; Neubauer, A.; Berman, E.; Paolini, S.; Montesinos, P.; Baer, M.R.; Larson, R.A.; Ustun, C.; et al. Gilteritinib or chemotherapy for relapsed or refractory FLT3-mutated AML. N. Engl. J. Med. 2019, 381, 1728–1740. [Google Scholar] [CrossRef]
- Amadori, S.; Arcese, W.; Isacchi, G.; Meloni, G.; Petti, M.C.; Monarca, B.; Testi, A.M.; Mandelli, F. Mitoxantrone, etoposide, and intermediate-dose cytarabine: An effective and tolerable regimen for the treatment of refractory acute myeloid leukemia. J. Clin. Oncol. 1991, 9, 1210–1214. [Google Scholar] [CrossRef] [PubMed]
- Daenen, S.; Löwenberg, B.; Sonneveld, P.; van Putten, W.L.; Verhoef, G.; Verdonck, L.F.; van Veldhoven, M.; Huijgens, P.C. Efficacy of etoposide and mitoxantrone in patients with acute myelogenous leukemia refractory to standard induction therapy and intermediate-dose cytarabine with amsidine. Dutch Hematology-Oncology Working Group for Adults (HOVON). Leukemia 1994, 8, 6–10. [Google Scholar]
- Ho, A.D.; Lipp, T.; Ehninger, G.; Illiger, H.J.; Meyer, P.; Freund, M.; Hunstein, W. Combination of mitoxantrone and etoposide in refractory acute myelogenous leukemia—An active and well-tolerated regimen. J. Clin. Oncol. 1988, 6, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Karanes, C.; Kopecky, K.J.; Head, D.R.; Grever, M.R.; Hynes, H.E.; Kraut, E.H.; Vial, R.H.; Lichtin, A.; Nand, S.; Samlowski, W.E.; et al. A phase III comparison of high dose ARA-C (HIDAC) versus HIDAC plus mitoxantrone in the treatment of first relapsed or refractory acute myeloid leukemia Southwest Oncology Group Study. Leuk. Res. 1999, 23, 787–794. [Google Scholar] [CrossRef]
- Martin, M.G.; Welch, J.S.; Augustin, K.; Hladnik, L.; DiPersio, J.F.; Abboud, C.N. Cladribine in the treatment of acute myeloid leukemia: A single-institution experience. Clin. Lymphoma Myeloma 2009, 9, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Bergua, J.M.; Montesinos, P.; Martinez-Cuadrón, D.; Fernández-Abellán, P.; Serrano, J.; Sayas, M.J.; Prieto-Fernandez, J.; García, R.; García-Huerta, A.J.; Barrios, M.; et al. A prognostic model for survival after salvage treatment with FLAG-Ida +/− gemtuzumab-ozogamicine in adult patients with refractory/relapsed acute myeloid leukaemia. Br. J. Haematol. 2016, 174, 700–710. [Google Scholar] [CrossRef]
- Jackson, G.; Taylor, P.; Smith, G.M.; Marcus, R.; Smith, A.; Chu, P.; Littlewood, T.J.; Duncombe, A.; Hutchinson, M.; Mehta, A.B.; et al. A multicentre, open, non-comparative phase II study of a combination of fludarabine phosphate, cytarabine and granulocyte colony-stimulating factor in relapsed and refractory acute myeloid leukaemia and de novo refractory anaemia with excess of blasts in transformation. Br. J. Haematol. 2001, 112, 127–137. [Google Scholar]
- Lee, S.R.; Yang, D.H.; Ahn, J.S.; Kim, Y.K.; Lee, J.J.; Choi, Y.J.; Shin, H.J.; Chung, J.S.; Cho, Y.Y.; Chae, Y.S.; et al. The clinical outcome of FLAG chemotherapy without idarubicin in patients with relapsed or refractory acute myeloid leukemia. J. Korean Med. Sci. 2009, 24, 498–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montillo, M.; Mirto, S.; Petti, M.C.; Latagliata, R.; Magrin, S.; Pinto, A.; Zagonel, V.; Mele, G.; Tedeschi, A.; Ferrara, F. Fludarabine, cytarabine, and G-CSF (FLAG) for the treatment of poor risk acute myeloid leukemia. Am. J. Hematol. 1998, 58, 105–109. [Google Scholar] [CrossRef]
- Chevallier, P.; Delaunay, J.; Turlure, P.; Pigneux, A.; Hunault, M.; Garand, R.; Guillaume, T.; Avet-Loiseau, H.; Dmytruk, N.; Girault, S.; et al. Long-term disease-free survival after gemtuzumab, intermediate-dose cytarabine, and mitoxantrone in patients with CD33+ primary resistant or relapsed acute myeloid leukemia. J. Clin. Oncol. 2008, 26, 5192–5197. [Google Scholar] [CrossRef] [PubMed]
- Grimwade, D.; Hills, R.K.; Moorman, A.V.; Walker, H.; Chatters, S.; Goldstone, A.H.; Wheatley, K.; Harrison, C.J.; Burnett, A.K.; National Cancer Research Institute Adult Leukaemia Working, G. Refinement of cytogenetic classification in acute myeloid leukemia: Determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood 2010, 116, 354–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheson, B.D.; Bennett, J.M.; Kopecky, K.J.; Büchner, T.; Willman, C.L.; Estey, E.H.; Schiffer, C.A.; Doehner, H.; Tallman, M.S.; Lister, T.A.; et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J. Clin. Oncol. 2003, 21, 4642–4649. [Google Scholar] [CrossRef]
- Dumas, P.Y.; Bertoli, S.; Bérard, E.; Largeaud, L.; Bidet, A.; Delabesse, E.; Leguay, T.; Leroy, H.; Gadaud, N.; Rieu, J.B.; et al. Real-world outcomes of patients with refractory or relapsed FLT3-ITD acute myeloid leukemia: A Toulouse-Bordeaux DATAML registry study. Cancers 2020, 12, 2044. [Google Scholar] [CrossRef] [PubMed]
- Chua, C.C.; Grigg, A.; Singh, J.; Droogleever, M.P.; Zhang, L.; Lim, A.; Fong, C.Y.; Ting, S.B.; Schwarer, A.; Tiong, I.S.; et al. Treatment practice and outcomes in FLT3-mutant acute myeloid leukemia in the pre-midostaurin era: A real-world experience from Australian tertiary hospitals. Leuk. Lymphoma 2020, 61, 848–854. [Google Scholar] [CrossRef]
- Medeiros, B.C.; Pandya, B.J.; Hadfield, A.; Pike, J.; Wilson, S.; Mueller, C.; Bui, C.N.; Flanders, S.C.; Rider, A.; Horvath Walsh, L.E. Treatment patterns in patients with acute myeloid leukemia in the United States: A cross-sectional, real-world survey. Curr. Med. Res. Opin. 2019, 35, 927–935. [Google Scholar] [CrossRef] [Green Version]
- Almeida, A.M.; Ramos, F. Acute myeloid leukemia in the older adults. Leuk. Res. Rep. 2016, 6, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Lazarevic, V.L.; Bredberg, A.; Lorenz, F.; Öhlander, E.; Antunovic, P.; Cammenga, J.; Wennström, L.; Möllgård, L.; Deneberg, S.; Derolf, A.; et al. Acute myeloid leukemia in very old patients. Haematologica 2018, 103, e578–e580. [Google Scholar] [CrossRef] [PubMed]
- Yanada, M.; Naoe, T. Acute myeloid leukemia in older adults. Int. J. Hematol. 2012, 96, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Wattad, M.; Weber, D.; Döhner, K.; Krauter, J.; Gaidzik, V.I.; Paschka, P.; Heuser, M.; Thol, F.; Kindler, T.; Lübbert, M.; et al. Impact of salvage regimens on response and overall survival in acute myeloid leukemia with induction failure. Leukemia 2017, 31, 1306–1313. [Google Scholar] [CrossRef]
- Gamper, E.M.; Cottone, F.; Sommer, K.; Norman, R.; King, M.; Breccia, M.; Caocci, G.; Patriarca, A.; Palumbo, G.A.; Stauder, R.; et al. The EORTC QLU-C10D was more efficient in detecting clinical known group differences in myelodysplastic syndromes than the EQ-5D-3L. J. Clin. Epidemiol. 2021, 137, 31–44. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Aged ≥18 years when diagnosed with AML Relapsed or refractory AML Tested positive for an FLT3-ITD mutation during the study period using a locally available test Received active therapy † in first line | Acute promyelocytic leukemia (M3 AML) or mixed phenotype AML |
| Characteristic at Initial Diagnosis | Total (N = 404) | Intensive (N = 261) | Non-Intensive (N = 63) | Supportive Care Only (N = 80) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Median (Range) | n (%) | Median (Range) | n (%) | Median (Range) | n (%) | Median (Range) | n (%) | ||
| Age (years) | 59 (18–86) | 404 (100) | 52 (18–76) | 261 (100) | 72 (33–83) | 63 (100) | 68 (37–86) | 80 (100) | <0.001 * |
| <60 | 208 (51) | 180 (69) | 12 (19) | 16 (20) | <0.001 | ||||
| ≥60 | 196 (49) | 81 (31) | 51 (81) | 64 (80) | |||||
| Sex | 402 (100) | 261 (100) | 61 (100) | 80 (100) | |||||
| Male | 196 (49) | 126 (48) | 34 (56) | 36 (45) | 0.4 | ||||
| Female | 206 (51) | 135 (52) | 27 (44) | 44 (55) | |||||
| Type of AML | 372 (100) | 238 (100) | 62 (100) | 72 (100) | |||||
| De novo | 313 (84) | 210 (88) | 45 (73) | 58 (81) | 0.007 | ||||
| Secondary | 59 (16) | 28 (12) | 17 (27) | 14 (19) | |||||
| Therapy-related AML | 367 (100) | 234 (100) | 62 (100) | 71 (100) | |||||
| Yes | 26 (7) | 13 (6) | 8 (13) | 5 (7) | |||||
| No | 341 (93) | 221 (94) | 54 (87) | 66 (93) | 0.13 | ||||
| Secondary to MDS/MPS | 367 (100) | 234 (100) | 62 (100) | 71 (100) | |||||
| Yes | 28 (8) | 11 (5) | 9 (15) | 8 (11) | 0.02 | ||||
| No | 339 (92) | 223 (95) | 53 (85) | 63 (89) | |||||
| FAB subtype | 404 (100) | 261 (100) | 63 (100) | 80 (100) | |||||
| M0 | 23 (6) | 17 (7) | 4 (6) | 2 (2) | 0.16 | ||||
| M1 | 69 (17) | 43 (16) | 14 (22) | 12 (15) | |||||
| M2 | 46 (11) | 27 (10) | 6 (10) | 13 (16) | |||||
| M4 | 107 (26) | 68 (26) | 14 (22) | 25 (31) | |||||
| M5 | 65 (16) | 51 (20) | 9 (14) | 5 (6) | |||||
| M6 | 5 (1) | 2 (1) | 2 (3) | 1 (1) | |||||
| M7 | 2 (1) | 1 (0) | 1 (2) | 0 (0) | |||||
| NA | 87 (22) | 52 (20) | 13 (21) | 22 (27) | |||||
| Extramedullary disease | 285 (100) | 174 (100) | 55 (100) | 56 (100) | |||||
| Yes | 75 (26) | 58 (33) | 8 (15) | 9 (16) | |||||
| No | 210 (74) | 116 (67) | 47 (85) | 47 (84) | 0.003 | ||||
| WBC, ×109/L | 51.4 (0.6–365.5) | 379 (100) | 51.2 (0.9–65.5) | 247 (100) | 26 (0.6–384.4) | 59 (100) | 67.5 (0.9–292.3) | 73 (100) | 0.02* |
| ≤10 | 70 (18) | 45 (18) | 15 (25) | 10 (14) | 0.22 | ||||
| >10 | 309 (82) | 202 (82) | 44 (75) | 63 (86) | |||||
| Cytogenetics | 404 (100) | 261 (100) | 63 (100) | 80 (100) | |||||
| Normal | 253 (630) | 168 (64) | 42 (67) | 43 (54) | 0.31 | ||||
| Abnormal | 95 (24) | 63 (24) | 13 (21) | 19 (24) | |||||
| No metaphases | 33 (8) | 16 (6) | 6 (10) | 11 (14) | |||||
| NA | 23 (6) | 14 (5) | 2 (3) | 7 (9) | |||||
| MRC cytogenetic risk | 404 (100) | 261 (100) | 63 (100) | 80 (100) | |||||
| Favorable | 5 (1) | 3 (1) | 2 (3) | 0 (0) | 0.23 | ||||
| Intermediate | 309 (76) | 204 (78) | 51 (81) | 54 (67) | |||||
| Adverse | 38 (9) | 24 (9) | 4 (6) | 10 (13) | |||||
| NA | 52 (13) | 30 (12) | 6 (10) | 16 (20) | |||||
| FLT3-ITD mutation | 403 (100) † | 261 (100) | 63 (100) | 79 (100) † | |||||
| Positive | 395 (98) | 259 (99) | 59 (94) | 77 (97) | 0.02 | ||||
| Negative | 8 (2) # | 2 (1) # | 4 (6) # | 2 (3) # | |||||
| FLT3-ITD allelic ratio | 0.65 (0–10.55) | 281 (100) | 0.7 (0–10.55) | 166 (100) | 0.4 (0–7.4) | 57 (100) | 0.58 (0–4.7) | 58 (100) | |
| <0.06 | 23 (8) | 4 (2) | 11 (19) | 8 (14) | 0.004 * | ||||
| ≥0.06–0.5 | 93 (33) | 53 (32) | 22 (39) | 18 (31) | |||||
| ≥0.5–0.8 | 63 (22) | 39 (23) | 10 (18) | 14 (24) | <0.001 | ||||
| ≥0.8 | 102 (36) | 70 (42) | 14 (25) | 18 (31) | |||||
| NPM1 mutation status | 404 (100) | 261 (100) | 63 (100) | 80 (100) | |||||
| Positive | 205 (51) | 127 (49) | 39 (62) | 39 (49) | 0.18 | ||||
| Negative | 155 (38) | 100 (38) | 20 (32) | 35 (44) | |||||
| NA | 44 (11) | 34 (13) | 4 (6) | 6 (7) | |||||
| CEBPA mutation status | 404 (100) | 261 (100) | 55 (100) | 80 (100) | |||||
| Positive | 11 (3) | 9 (3) | 1(2) | 1 (1) | 0.32 | ||||
| Negative | 78 (19) | 44 (17) | 13 (24) | 21 (26) | |||||
| NA | 315 (78) | 208 (80) | 41 (75) | 58 (72) | |||||
| IDH mutation status | 404 (100) | 261 (100) | 63 (100) | 80 (100) | |||||
| IDH1 positive | 9 (2) | 6 (2) | 2 (3) | 1 (1) | |||||
| IDH2 positive | 15 (4) | 6 (2) | 7 (11) | 2 (2) | |||||
| Negative | 92 (23) | 57 (22) | 21 (33) | 14 (17) | |||||
| NA | 288 (71) | 192 (74) | 33 (52) | 63 (79) | 0.003 | ||||
| Characteristic | Total (N = 404) | Intensive (N = 261) | Non-Intensive (N = 63) | Supportive Care Only (N = 80) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Median (Range) | n (%) | Median (Range) | n (%) | Median (Range) | n (%) | Median (Range) | n (%) | ||
| Time to R/R, † (months) | 4.99 (1.58–79.48) | 4.25 (1.81–127.3) | 5.91 (1.87–104.5) | 5.44 (1.58–79.48) | 0.23 | ||||
| Age (years) | 60 (18–86) | 401 (100) | 52 (18–77) | 259 (100) | 73 (34–84) | 63 (100) | 69 (37–86) | 77 (100) | |
| <60 | 190 (47) | 167 (64) | 10 (16) | 13 (17) | <0.001 * | ||||
| ≥60 | 211 (53) | 93 (36) | 53 (84) | 65 (83) | <0.001 | ||||
| ECOG PS | 1 (0–4) | 126 (100) | 1 (0–4) | 79 (100) | 1 (0–2) | 26 (100) | 1 (0–4) | 21 (100) | 0.001 * |
| 0 | 43 (34) | 31 (39) | 10 (38) | 2 (10) | 0.02 | ||||
| 1 | 58 (46) | 36 (46) | 13 (50) | 9 (43) | |||||
| 2 | 16 (13) | 8 (10) | 3 (12) | 5 (24) | |||||
| 3 | 6 (5) | 3 (4) | 0 (0) | 3 (14) | |||||
| 4 | 3 (2) | 1 (1) | 0 (0) | 2 (10) | |||||
| WBC, ×109/L | 5.3 (0.2–283) | 114 (100) | 6.5 (0.4–269) | 67 (100) | 3.4 (0.6–108) | 26 (100) | 5.4 (0.2–282) | 21 (100) | 0.06 * |
| ≤10 | 71 (62) | 40 (60) | 18 (69) | 13 (62) | 0.7 | ||||
| >10 | 43 (38) | 27 (40) | 8 (31) | 8 (38) | |||||
| Hemoglobin, g/dL | 10 (4.6–16.1) | 113 (100) | 9.7 (4.6–16.1) | 67 (100) | 10.8 (7.8–15.3) | 25 (100) | 9.6 (6.6–13.5) | 21 (100) | 0.14 * |
| ≤10 | 59 (52) | 38 (57) | 9 (36) | 12 (57) | 0.18 | ||||
| >10 | 54 (48) | 29 (43) | 26 (64) | 9 (43) | |||||
| Platelet count, ×109/L | 81 (1.5–984) | 113 (100) | 82 (1.5–984) | 67 (100) | 101 (10–467) | 25 (100) | 61 (12–294) | 21 (100) | 0.25 * |
| ≤50 | 44 (39) | 26 (39) | 8 (32) | 10 (48) | |||||
| >50 | 69 (61) | 41 (61) | 17 (68) | 11 (52) | 0.56 | ||||
| PB blasts, % | 15 (0–100) | 115 (100) | 17 (0–100) | 68 (100) | 11 (0–96) | 26 (100) | 17 (0–100) | 21 (100) | 0.70 * |
| ≤50 | 81 (70) | 44 (65) | 21 (81) | 16 (76) | 0.25 | ||||
| >50 | 34 (30) | 24 (35) | 5 (19) | 5 (24) | |||||
| BM blasts, % | 45 (0–100) | 121 (100) | 40 (0–100) | 78 (100) | 45 (5–99) | 25 (100) | 46 (9–100) | 18 (100) | 0.32 * |
| ≤50 | 68 (56) | 44 (56) | 14 (56) | 10 (56) | 0.99 | ||||
| >50 | 53 (44) | 34 (44) | 11 (44) | 8 (44) | |||||
| Previous SCT | 403 (100) | 261 (100) | 63 (100) | 79 (100) | |||||
| No | 318 (79) | 195 (75) | 56 (89) | 67 (85) | 0.08 | ||||
| Autologous | 33 (8) | 26 (10) | 2 (3) | 5 (6) | |||||
| Allogeneic | 52 (13) | 40 (15) | 5 (8) | 7 (9) | |||||
| Clinical trial salvage | 404 (100) | 261 (100) | 63 (100) | - | <0.001 | ||||
| Yes | 24 (6) | 4 (2) | 20 (32) | - | |||||
| No | 380 (94) | 257 (98) | 43 (68) | - | |||||
| Variable | All Patients (N = 404) | Intensive (N = 261) | Non-Intensive (N = 63) | Supportive (N = 80) | p-Value * |
|---|---|---|---|---|---|
| Response, n (%) | n = 280 | n = 223 | n = 57 | - | |
| ORR (CR + CRi) | 119 (42) | 108 (48) | 11 (19) | - | <0.001 |
| CR | 110 (39) | 101 (45) | 9 (15) | - | |
| CRi | 9 (3) | 7 (3) | 2 (4) | - | |
| PR | 14 (5) | 12 (5) | 2 (4) | - | |
| Resistance | 120 (43) | 82 (37) | 38 (67) | - | |
| Induction death | 27 (10) | 21 (9) | 6 (11) | - | |
| OS, months | n = 401 | n = 260 | n = 63 | n = 78 | |
| Median (95% CI) | 5.5 (4.2–6.7) | 7.2 (6.6–9.3) | 6.2 (4.2–10.7) | 1.0 (0.6–1.2) | <0.001 |
| OS, % | |||||
| At 1 year (95% CI) | 25 (20–30) | 34 (28–42) | 33 (23–49) | - | |
| At 2 years (95% CI) | 16 (11–20) | 20 (15–27) | 22 (12–39) | - | |
| At 5 years (95% CI) | 7 (2–4) | 9 (6–16) | - | - | |
| EFS, months | n = 280 | n = 223 | n = 57 | - | |
| Median (95% CI) | 0.03 (0.03–0.03) | 0.03 (0.03–1.6) | 0.03 (0.03–0.03) | - | 0.008 |
| EFS, % | |||||
| At 1 year (95% CI) | 17(13–22) | 20 (15–26) | 10 (5–22) | - | |
| At 2 years (95% CI) | 11 (7–15) | 14 (9–20) | 8 (3–20) | - | |
| At 5 years (95% CI) | 7 (3–11) | 8 (4–14) | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Cuadrón, D.; Serrano, J.; Mariz, J.; Gil, C.; Tormo, M.; Martínez-Sánchez, P.; Rodríguez-Arbolí, E.; García-Boyero, R.; Rodríguez-Medina, C.; Martínez-Chamorro, C.; et al. Characteristics and Outcomes of Adult Patients in the PETHEMA Registry with Relapsed or Refractory FLT3-ITD Mutation-Positive Acute Myeloid Leukemia. Cancers 2022, 14, 2817. https://doi.org/10.3390/cancers14112817
Martínez-Cuadrón D, Serrano J, Mariz J, Gil C, Tormo M, Martínez-Sánchez P, Rodríguez-Arbolí E, García-Boyero R, Rodríguez-Medina C, Martínez-Chamorro C, et al. Characteristics and Outcomes of Adult Patients in the PETHEMA Registry with Relapsed or Refractory FLT3-ITD Mutation-Positive Acute Myeloid Leukemia. Cancers. 2022; 14(11):2817. https://doi.org/10.3390/cancers14112817
Chicago/Turabian StyleMartínez-Cuadrón, David, Josefina Serrano, José Mariz, Cristina Gil, Mar Tormo, Pilar Martínez-Sánchez, Eduardo Rodríguez-Arbolí, Raimundo García-Boyero, Carlos Rodríguez-Medina, Carmen Martínez-Chamorro, and et al. 2022. "Characteristics and Outcomes of Adult Patients in the PETHEMA Registry with Relapsed or Refractory FLT3-ITD Mutation-Positive Acute Myeloid Leukemia" Cancers 14, no. 11: 2817. https://doi.org/10.3390/cancers14112817