
New Therapy Options for Neuroendocrine Carcinoma of the Pancreas—The Emergent Substance GP-2250 and Gemcitabine Prove to Be Highly Effective without the Development of Secondary Resistances In Vitro and In Vivo

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cells and Tissue
2.2. Reagents
2.3. MTT
2.4. Xenograft QGP-1 and Patient Derived Xenograft Bo99
2.5. Ethics Approval and Consent to Participate
2.6. Statistical Analysis
3. Results
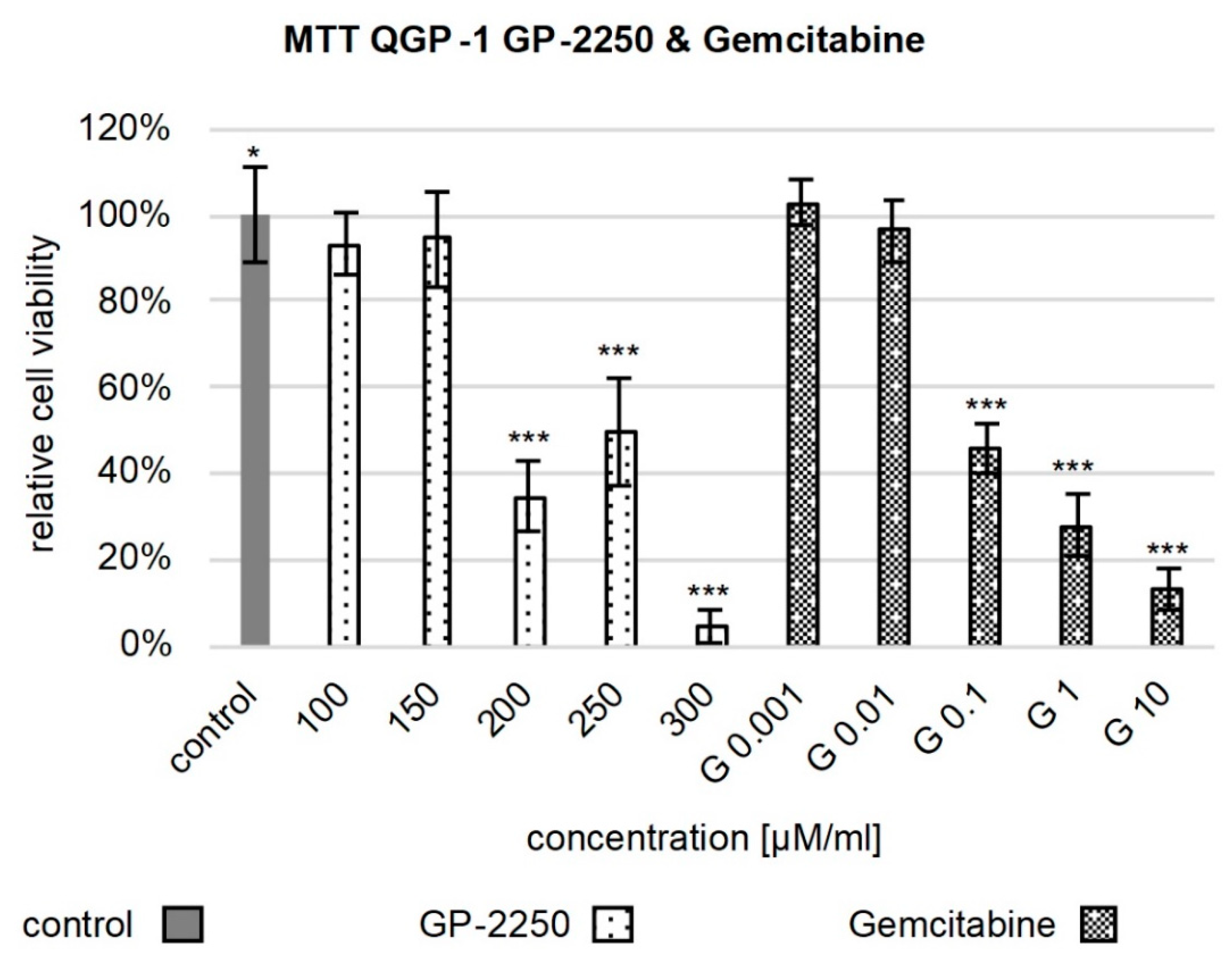
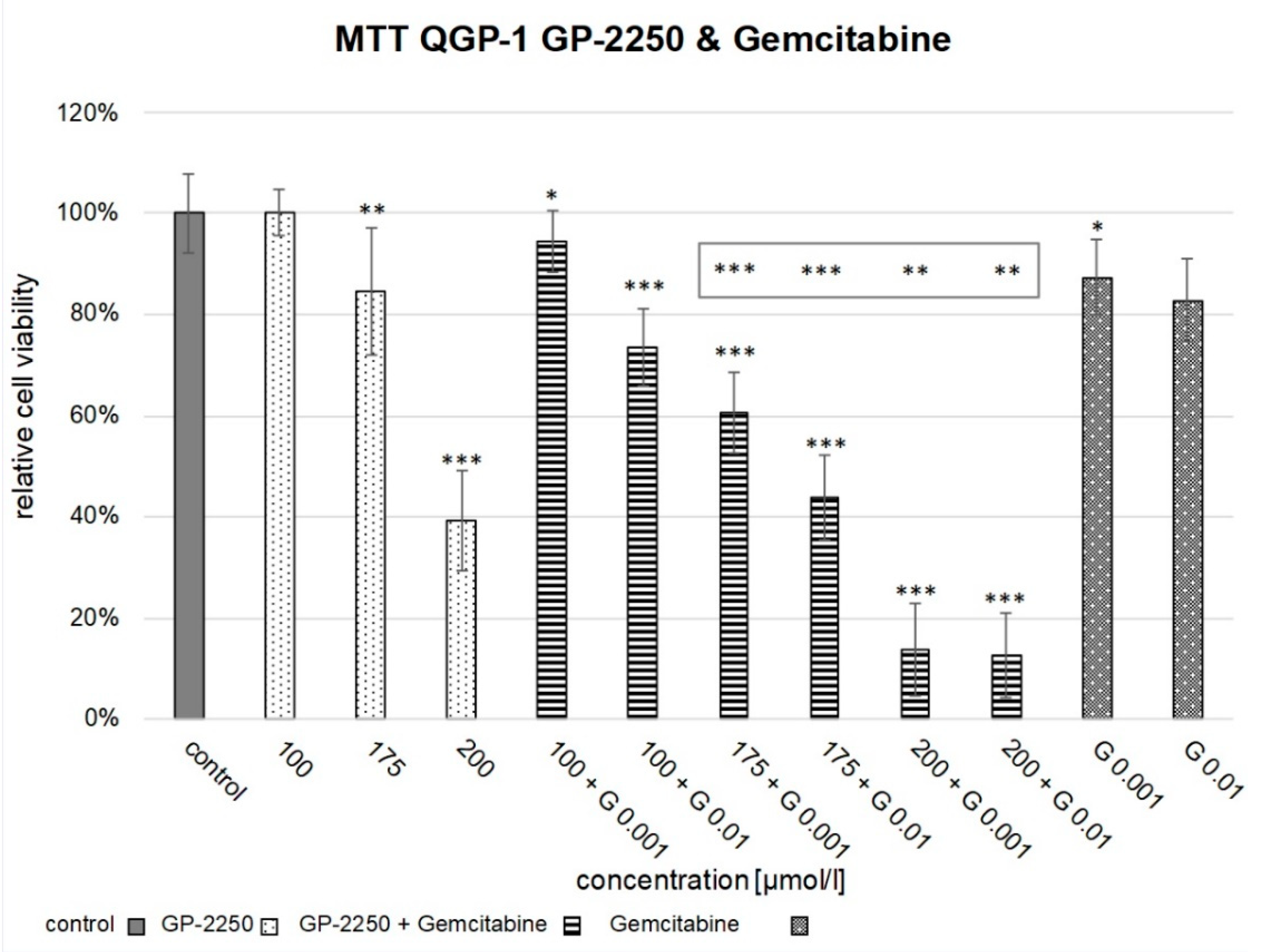
3.1. MTT
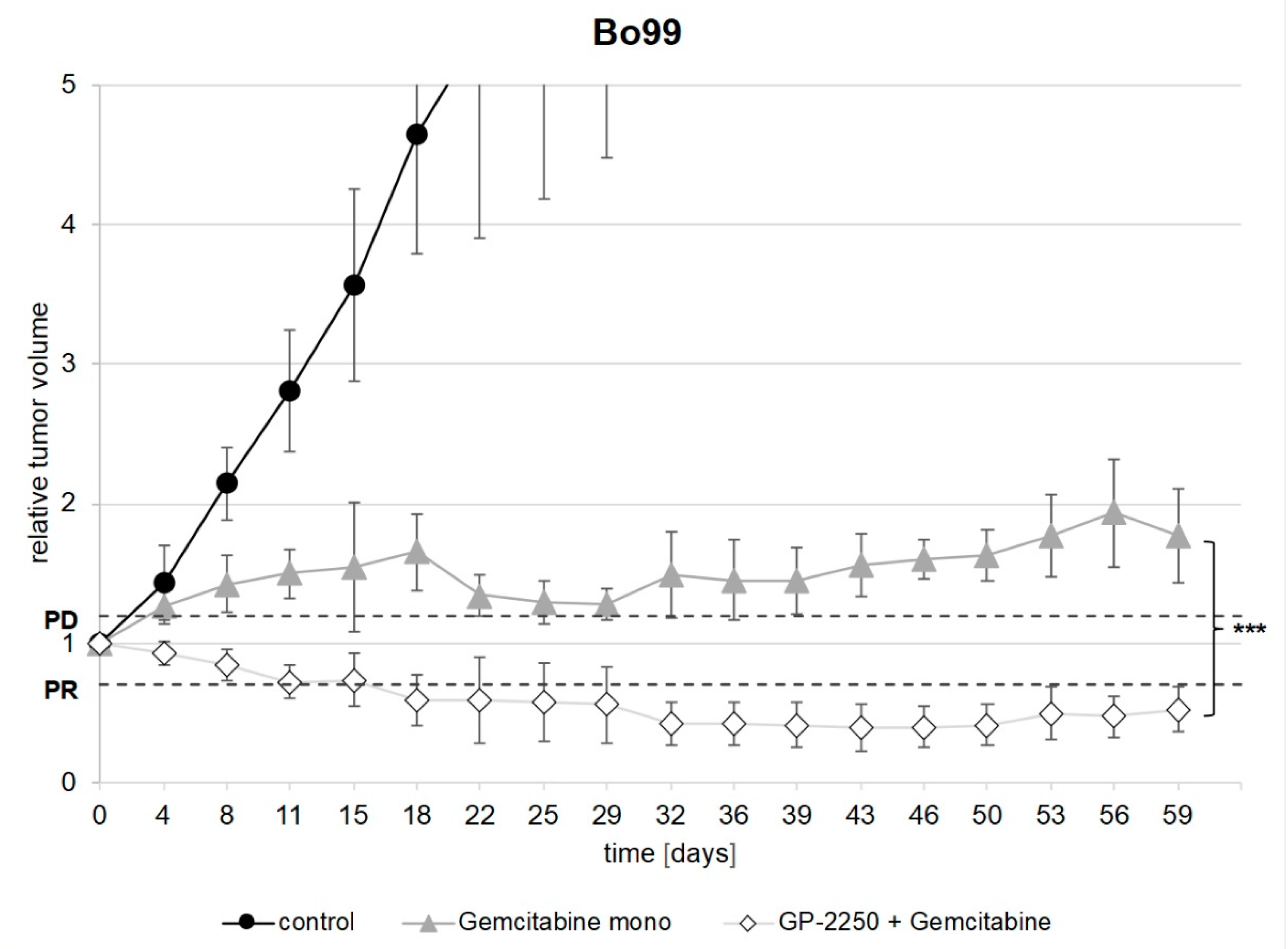
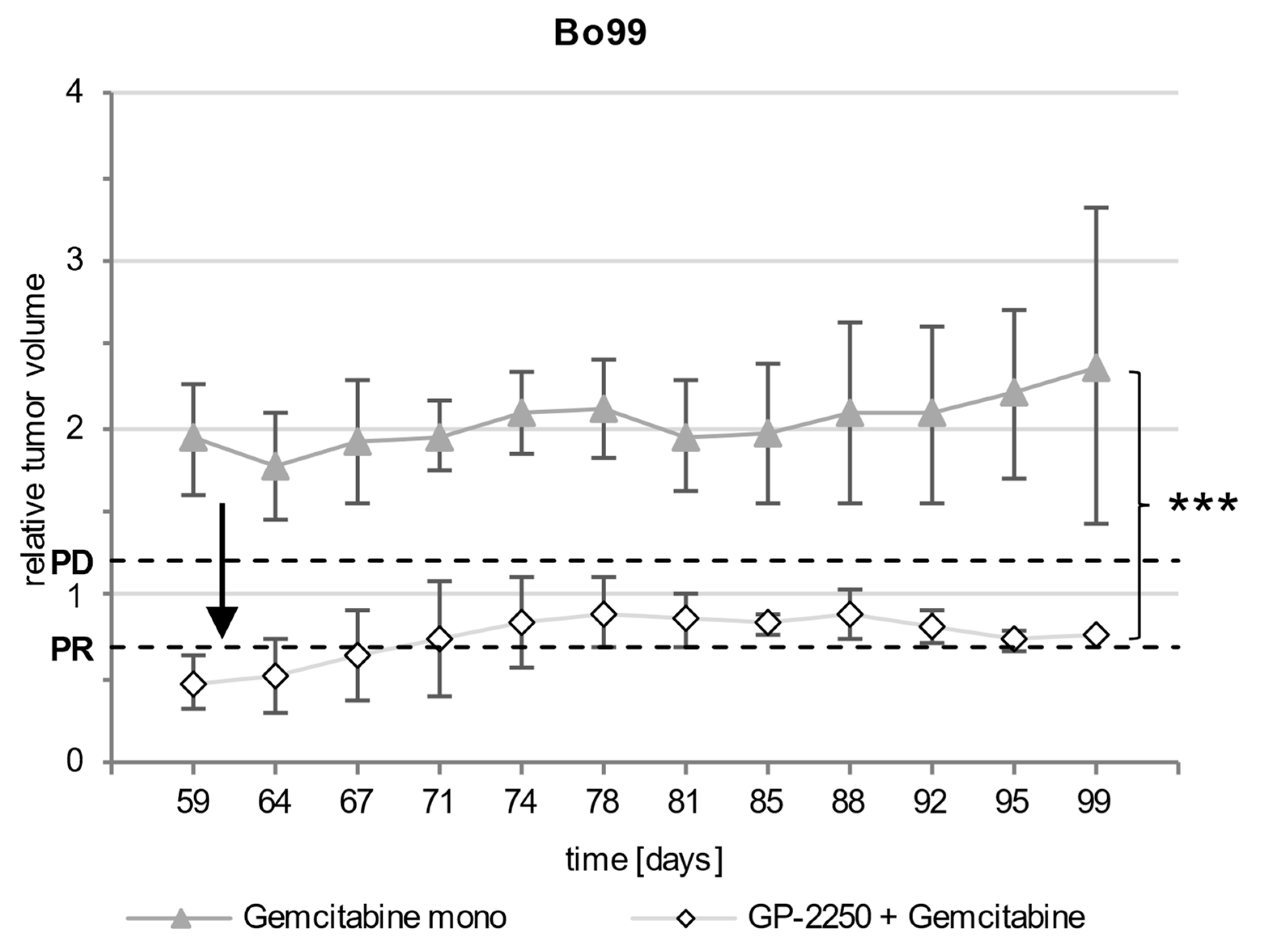
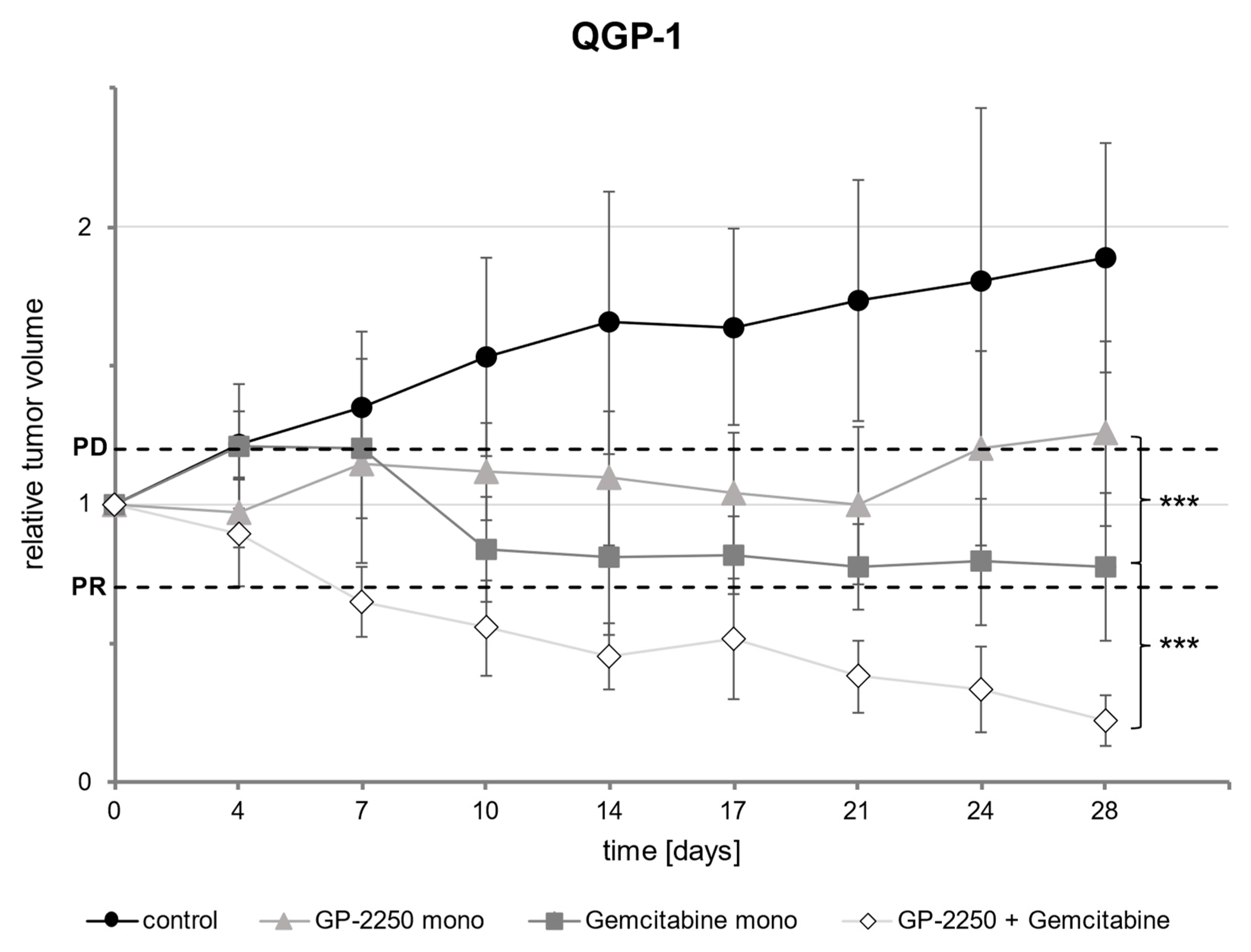
3.2. PDX and Xenograft
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| FCS | fetal calf serum |
| FOLFIRI | folinic acid, 5-Fluorouracil, Irinotecan |
| FOLFOX | folinic acid, 5-Fluorouracil, Oxaliplatin |
| Gemmono | monotherapy with Gemcitabine |
| GP-2250mono | monotherapy with GP-2250 |
| ddH20 | double distilled water |
| DMEM | Dulbecco’s Modified Eagle Medium |
| DMSO | dimethylsulfoxide |
| kgBW | kilogram body weight |
| µM | micromole per liter |
| MTT | 3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyltetrazoliumbromid |
| NEC | neuroendocrine carcinoma |
| NET | neuroendocrine tumor |
| PD | progressive disease |
| PDAC | pancreatic ductal adenocarcinoma |
| PDX | patient derived xenograft |
| pNEC | pancreatic neuroendocrine carcinoma |
| pNET | pancreatic neuroendocrine tumor |
| PR | partial response |
| RECIST | Response Evaluation Criteria in Solid Tumors |
| SCLC | small cell lung carcinoma |
References
- Scott, A.T.; Howe, J.R. Evaluation and management of neuroendocrine tumors of the pancreas. Surg. Clin. N. Am. 2019, 99, 793–814. [Google Scholar] [CrossRef]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Boyar Cetinkaya, R.; Aagnes, B.; Thiis-Evensen, E.; Tretli, S.; Bergestuen, D.S.; Hansen, S. Trends in incidence of neuroendocrine neoplasms in Norway: A report of 16,075 cases from 1993 through 2010. Neuroendocrinology 2017, 104, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Lee, L.; Hijioka, M.; Kawabe, K.; Kato, M.; Nakamura, K.; Ueda, K.; Ohtsuka, T.; Igarashi, H. The up-to-date review of epidemiological pancreatic neuroendocrine tumors in Japan. J. Hepato-Biliary-Pancreat. Sci. 2015, 22, 574–577. [Google Scholar] [CrossRef]
- Korse, C.M.; Taal, B.G.; van Velthuysen, M.-L.F.; Visser, O. Incidence and survival of neuroendocrine tumours in the Netherlands according to histological grade: Experience of two decades of cancer registry. Eur. J. Cancer 2013, 49, 1975–1983. [Google Scholar] [CrossRef]
- Lepage, C.; Rachet, B.; Coleman, M.P. Survival from malignant digestive endocrine tumors in England and Wales: A population-based study. Gastroenterology 2007, 132, 899–904. [Google Scholar] [CrossRef]
- Klöppel, G.; Couvelard, A.; Hruban, R.H.; Klimstra, D.S.; Komminoth, P.; Osamura, R.Y.; Perren, A.; Rindi, G. Neoplasms of the neuroendocrine pancreas. In WHO Classification of Tumours of Endocrine Organs, 4th ed.; Lloyd, R.V., Osamura, R.Y., Klöppel, G., Rosai, J., Eds.; International Agency for Research on Cancer: Lyon, France, 2017; ISBN 978-92-832-44936. [Google Scholar]
- Yang, M.; Tian, B.; Zhang, Y.; Su, A.-P.; Yue, P.-J.; Xu, S.; Wang, L. Evaluation of the World Health Organization 2010 grading system in surgical outcome and prognosis of pancreatic neuroendocrine tumors. Pancreas 2014, 43, 1003–1008. [Google Scholar] [CrossRef]
- Sorbye, H.; Welin, S.; Langer, S.W.; Vestermark, L.W.; Holt, N.; Osterlund, P.; Dueland, S.; Hofsli, E.; Guren, M.G.; Ohrling, K.; et al. Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3): The NORDIC NEC study. Ann. Oncol. 2013, 24, 152–160. [Google Scholar] [CrossRef]
- Barnes, B. (Ed.) Bericht zum Krebsgeschehen in Deutschland 2016; Robert Koch-Institut: Berlin, Germany, 2016; ISBN 978-3-89606-279-6. [Google Scholar]
- Izbicki, J.R.; Perez, D. (Eds.) Expertise Allgemein-und Viszeralchirurgie Pankreas; Georg Thieme Verlag: Stuttgart, Germany, 2018; ISBN 9783132407220. [Google Scholar]
- Garcia-Carbonero, R.; Capdevila, J.; Crespo-Herrero, G.; Díaz-Pérez, J.A.; Del Martínez Prado, M.P.; Alonso Orduña, V.; Sevilla-García, I.; Villabona-Artero, C.; Beguiristain-Gómez, A.; Llanos-Muñoz, M.; et al. Incidence, patterns of care and prognostic factors for outcome of gastroenteropancreatic neuroendocrine tumors (GEP-NETs): Results from the National Cancer Registry of Spain (RGETNE). Ann. Oncol. 2010, 21, 1794–1803. [Google Scholar] [CrossRef]
- Bösch, F.; Belyaev, O.; Brunner, M.; Müller-Debus, C.F.; Grützmann, R.; Keck, T.; Uhl, W.; Witzigmann, H.; Werner, J. Operationsindikationen bei neuroendokrinen Neoplasien des Pankreas. Zentralbl. Chir. 2020, 145, 365–373. [Google Scholar] [CrossRef]
- Rink, A.; Wiedenmann, B.; Auernhammer, C.; Bartenstein, P.; Bartsch, D.; Begum, N.; Faiss, S.; Fottner, C.; Gebauer, B.; Goretzki, P.; et al. Practice guideline neuroendocrine tumors-AWMF-Reg. 021-27. Z. fur Gastroenterol. 2018, 56, 583–681. [Google Scholar] [CrossRef] [Green Version]
- Moertel, C.G.; Kvols, L.K.; O’Connell, M.J.; Rubin, J. Treatment of neuroendocrine carcinomas with combined etoposide and cisplatin. Evidence of major therapeutic activity in the anaplastic variants of these neoplasms. Cancer 1991, 68, 227–232. [Google Scholar] [CrossRef]
- Ghosh, S. Cisplatin: The first metal based anticancer drug. Bioorg. Chem. 2019, 88, 102925. [Google Scholar] [CrossRef]
- Amptoulach, S.; Tsavaris, N. Neurotoxicity caused by the treatment with platinum analogues. Chemother. Res. Pract. 2011, 2011, 843019. [Google Scholar] [CrossRef]
- Sinkule, J.A. Etoposide: A semisynthetic epipodophyllotoxin. Chemistry, pharmacology, pharmacokinetics, adverse effects and use as an antineoplastic agent. Pharmacotherapy 1984, 4, 61–73. [Google Scholar] [CrossRef]
- Buchholz, M.; Majchrzak-Stiller, B.; Hahn, S.; Vangala, D.; Pfirrmann, R.W.; Uhl, W.; Braumann, C.; Chromik, A.M. Innovative substance 2250 as a highly promising anti-neoplastic agent in malignant pancreatic carcinoma—In vitro and in vivo. BMC Cancer 2017, 17, 216. [Google Scholar] [CrossRef] [Green Version]
- Braumann, C.; Buchholz, M.; Majchrzak-Stiller, B.; Hahn, S.; Uhl, W.; Kasi, A.; Mueller, T. Metabolism-based GP-2250 in combination with gemcitabine as a novel approach to pancreatic cancer: A mouse xenograft study. J. Clin. Oncol. 2020, 38, e16750. [Google Scholar] [CrossRef]
- Buchholz, M. Vergleichende Anti-neoplastische Charakterisierung der Substanz 2250 Mit Ihrer Muttersubstanz Taurolidin: In Vivo und in Vitro. Dissertation, Ruhr-Universität Bochum, Bochum, Germany, 2016. Available online: https://hss-opus.ub.ruhr-uni-bochum.de/opus4/frontdoor/index/index/start/0/rows/10/sortfield/score/sortorder/desc/searchtype/simple/query/Buchholz%2C+Marie/docId/4904. (accessed on 25 May 2022).
- van Meerloo, J.; Kaspers, G.J.L.; Cloos, J. Cell sensitivity assays: The MTT assay. Methods Mol. Biol. 2011, 731, 237–245. [Google Scholar] [CrossRef]
- Benten, D.; Behrang, Y.; Unrau, L.; Weissmann, V.; Wolters-Eisfeld, G.; Burdak-Rothkamm, S.; Stahl, F.R.; Anlauf, M.; Grabowski, P.; Möbs, M.; et al. Establishment of the first well-differentiated human pancreatic neuroendocrine tumor model. Mol. Cancer Res. 2018, 16, 496–507. [Google Scholar] [CrossRef] [Green Version]
- Mazur, P.K.; Herner, A.; Mello, S.S.; Wirth, M.; Hausmann, S.; Sánchez-Rivera, F.J.; Lofgren, S.M.; Kuschma, T.; Hahn, S.A.; Vangala, D.; et al. Combined inhibition of BET family proteins and histone deacetylases as a potential epigenetics-based therapy for pancreatic ductal adenocarcinoma. Nat. Med. 2015, 21, 1163–1171. [Google Scholar] [CrossRef] [Green Version]
- Hidalgo, M.; Amant, F.; Biankin, A.V.; Budinská, E.; Byrne, A.T.; Caldas, C.; Clarke, R.B.; de Jong, S.; Jonkers, J.; Mælandsmo, G.M.; et al. Patient-derived xenograft models: An emerging platform for translational cancer research. Cancer Discov. 2014, 4, 998–1013. [Google Scholar] [CrossRef] [Green Version]
- Früh, M.; de Ruysscher, D.; Popat, S.; Crinò, L.; Peters, S.; Felip, E. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi99–vi105. [Google Scholar] [CrossRef]
- McKenna, L.R.; Edil, B.H. Update on pancreatic neuroendocrine tumors. Gland Surg. 2014, 3, 258–275. [Google Scholar] [CrossRef]
- Yao, J.C.; Phan, A.T.; Chang, D.Z.; Wolff, R.A.; Hess, K.; Gupta, S.; Jacobs, C.; Mares, J.E.; Landgraf, A.N.; Rashid, A.; et al. Efficacy of RAD001 (everolimus) and octreotide LAR in advanced low- to intermediate-grade neuroendocrine tumors: Results of a phase II study. J. Clin. Oncol. 2008, 26, 4311–4318. [Google Scholar] [CrossRef]
- Yao, J.C.; Shah, M.H.; Ito, T.; Bohas, C.L.; Wolin, E.M.; van Cutsem, E.; Hobday, T.J.; Okusaka, T.; Capdevila, J.; de Vries, E.G.E.; et al. Everolimus for advanced pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Ducreux, M.; Cuhna, A.S.; Caramella, C.; Hollebecque, A.; Burtin, P.; Goéré, D.; Seufferlein, T.; Haustermans, K.; van Laethem, J.L.; Conroy, T.; et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, v56–v68. [Google Scholar] [CrossRef]
- Esmo. Cancer of the Pancreas Treatment Recommendations. Available online: https://www.esmo.org/guidelines/gastrointestinal-cancers/pancreatic-cancer/eupdate-cancer-of-the-pancreas-treatment-recommendations (accessed on 2 June 2021).
- Cormier, Y.; Eisenhauer, E.; Muldal, A.; Gregg, R.; Ayoub, J.; Goss, G.; Stewart, D.; Tarasoff, P.; Wong, D. Gemcitabine is an active new agent in previously untreated extensive small cell lung cancer (SCLC). A study of the National Cancer Institute of Canada Clinical Trials Group. Ann. Oncol. 1994, 5, 283–285. [Google Scholar] [CrossRef]
- van der Lee, I.; Smit, E.F.; van Putten, J.W.; Groen, H.J.; Schlösser, N.J.; Postmus, P.E.; Schramel, F.M. Single-agent gemcitabine in patients with resistant small-cell lung cancer. Ann. Oncol. 2001, 12, 557–561. [Google Scholar] [CrossRef]
- Kulke, M.H.; Kim, H.; Clark, J.W.; Enzinger, P.C.; Lynch, T.J.; Morgan, J.A.; Vincitore, M.; Michelini, A.; Fuchs, C.S. A Phase II trial of gemcitabine for metastatic neuroendocrine tumors. Cancer 2004, 101, 934–939. [Google Scholar] [CrossRef]
- Saif, M.W.; Kaley, K.; Rodriguez, T.; Garcon, M.C. Gemcitabine as salvage treatment in patients with poorly differentiated pancreatic neuroendocrine tumors: A case series. JOP. J. Pancreas 2014, 15, 38–41. [Google Scholar] [CrossRef]
- Nakazuru, S.; Yoshio, T.; Suemura, S.; Itoh, M.; Araki, M.; Yoshioka, C.; Ohta, M.; Sueyoshi, Y.; Ohta, T.; Hasegawa, H.; et al. Poorly differentiated endocrine carcinoma of the pancreas responded to gemcitabine: Case report. World J. Gastroenterol. 2010, 16, 3853–3856. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Miyagawa, K.; Hiura, M.; Taguchi, M.; Kihara, Y.; Abe, S.; Shimajiri, S.; Harada, M. Poorly differentiated neuroendocrine carcinoma of the pancreas responsive to combination therapy with gemcitabine and S-1. Intern. Med. 2012, 51, 727–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasuya, K.; Nagakawa, Y.; Suzuki, M.; Suzuki, Y.; Kyo, B.; Suzuki, S.; Matsudo, T.; Itoi, T.; Tsuchida, A.; Aoki, T. Combination therapy of gemcitabine or oral S-1 with the anti-VEGF monoclonal antibody bevacizumab for pancreatic neuroendocrine carcinoma. Exp. Ther. Med. 2012, 3, 599–602. [Google Scholar] [CrossRef] [Green Version]
- Geistlich Pharma, A.G.; Translational Drug Development. A Phase 1/2 Trial of GP-2250 in Combination with Gemcitabine in Pancreatic Adenocarcinoma After FOLFIRINOX Chemotherapy: NCT03854110, GP-2250-1001. Available online: https://clinicaltrials.gov/ct2/show/NCT03854110 (accessed on 12 April 2021).
- Chamberlain, C.E.; German, M.S.; Yang, K.; Wang, J.; VanBrocklin, H.; Regan, M.; Shokat, K.M.; Ducker, G.S.; Kim, G.E.; Hann, B.; et al. A Patient-derived xenograft model of pancreatic neuroendocrine tumors identifies sapanisertib as a possible new treatment for everolimus-resistant tumors. Mol. Cancer Ther. 2018, 17, 2702–2709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, Y.; Zhen, L.; Bai, J.; Mei, Y.; Li, Z.; Lin, A.; Li, X. Anticancer effects of baicalein in pancreatic neuroendocrine tumors in vitro and in vivo. Pancreas 2017, 46, 1076–1081. [Google Scholar] [CrossRef] [Green Version]
- Binenbaum, Y.; Na’ara, S.; Gil, Z. Gemcitabine resistance in pancreatic ductal adenocarcinoma. Drug Resist. Updat. 2015, 23, 55–68. [Google Scholar] [CrossRef]
- Chen, Y.-W.; Liu, J.-Y.; Lin, S.-T.; Li, J.-M.; Huang, S.-H.; Chen, J.-Y.; Wu, J.-Y.; Kuo, C.-C.; Wu, C.-L.; Lu, Y.-C.; et al. Proteomic analysis of gemcitabine-induced drug resistance in pancreatic cancer cells. Mol. BioSyst. 2011, 7, 3065–3074. [Google Scholar] [CrossRef]
- Arlt, A.; Gehrz, A.; Müerköster, S.; Vorndamm, J.; Kruse, M.-L.; Fölsch, U.R.; Schäfer, H. Role of NF-kappaB and Akt/PI3K in the resistance of pancreatic carcinoma cell lines against gemcitabine-induced cell death. Oncogene 2003, 22, 3243–3251. [Google Scholar] [CrossRef] [Green Version]
- Quiñonero, F.; Mesas, C.; Doello, K.; Cabeza, L.; Perazzoli, G.; Jimenez-Luna, C.; Rama, A.R.; Melguizo, C.; Prados, J. The challenge of drug resistance in pancreatic ductal adenocarcinoma: A current overview. Cancer Biol. Med. 2019, 16, 688–699. [Google Scholar] [CrossRef]
- Sliutz, G.; Karlseder, J.; Tempfer, C.; Orel, L.; Holzer, G.; Simon, M.M. Drug resistance against gemcitabine and topo-tecan mediated by constitutive hsp70 overexpression in vitro: Implication of quercetin as sensitiser in chemotherapy. Br. J. Cancer 1996, 74, 172–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozinn, S.I.; Harty, N.J.; Delong, J.M.; Deliyiannis, C.; Logvinenko, T.; Summerhayes, I.C.; Libertino, J.A.; Holway, A.H.; Rieger-Christ, K.M. MicroRNA Profile to Predict Gemcitabine Resistance in Bladder Carcinoma Cell Lines. Genes Cancer 2013, 4, 61–69. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buchholz, M.; Strotmann, J.; Majchrzak-Stiller, B.; Hahn, S.; Peters, I.; Horn, J.; Müller, T.; Höhn, P.; Uhl, W.; Braumann, C. New Therapy Options for Neuroendocrine Carcinoma of the Pancreas—The Emergent Substance GP-2250 and Gemcitabine Prove to Be Highly Effective without the Development of Secondary Resistances In Vitro and In Vivo. Cancers 2022, 14, 2685. https://doi.org/10.3390/cancers14112685
Buchholz M, Strotmann J, Majchrzak-Stiller B, Hahn S, Peters I, Horn J, Müller T, Höhn P, Uhl W, Braumann C. New Therapy Options for Neuroendocrine Carcinoma of the Pancreas—The Emergent Substance GP-2250 and Gemcitabine Prove to Be Highly Effective without the Development of Secondary Resistances In Vitro and In Vivo. Cancers. 2022; 14(11):2685. https://doi.org/10.3390/cancers14112685
Chicago/Turabian StyleBuchholz, Marie, Johanna Strotmann, Britta Majchrzak-Stiller, Stephan Hahn, Ilka Peters, Julian Horn, Thomas Müller, Philipp Höhn, Waldemar Uhl, and Chris Braumann. 2022. "New Therapy Options for Neuroendocrine Carcinoma of the Pancreas—The Emergent Substance GP-2250 and Gemcitabine Prove to Be Highly Effective without the Development of Secondary Resistances In Vitro and In Vivo" Cancers 14, no. 11: 2685. https://doi.org/10.3390/cancers14112685