
Immune Checkpoint Inhibitors as a Neoadjuvant/Adjuvant Treatment of Muscle-Invasive Bladder Cancer: A Systematic Review

 ,
,  , , ,
, , ,  ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
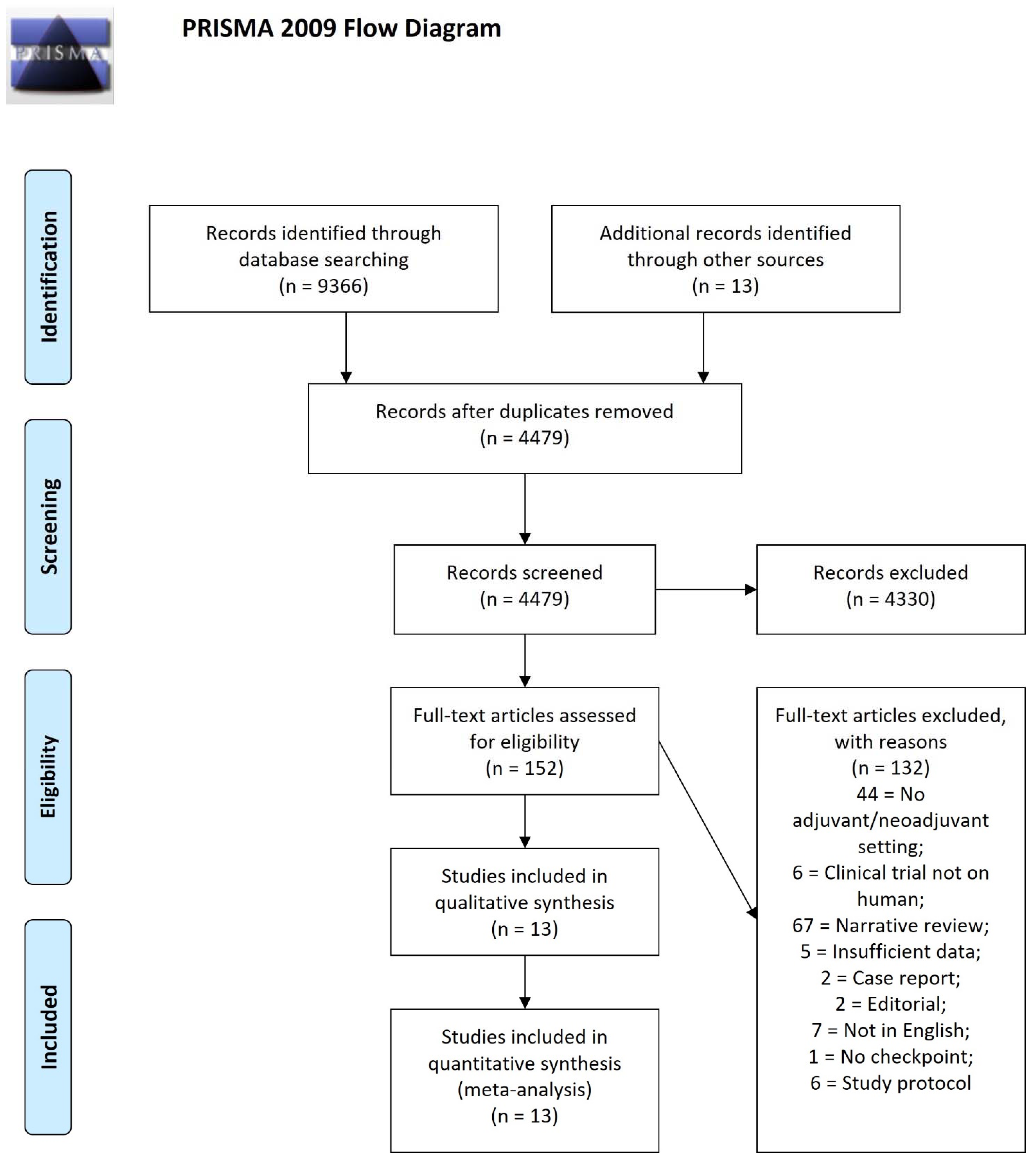
2. Methods
3. Rationale for Immune Checkpoint Inhibitors Use
4. Neoadjuvant Setting
5. Adjuvant Setting
6. Predictive Biomarkers
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Greiman, A.K.; Rosoff, J.S.; Prasad, S.M. Association of Human Development Index with global bladder, kidney, prostate and testis cancer incidence and mortality. BJU Int. 2017, 120, 799–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, D.S. Cancer epidemiology and prevention. Chronic Dis. Inj. Can. 1997, 18, 1G. [Google Scholar]
- Noon, A.P.; Pickvance, S.M.; Catto, J.W. Occupational exposure to crack detection dye penetrants and the potential for bladder cancer. Occup. Environ. Med. 2012, 69, 300–301. [Google Scholar] [CrossRef]
- Rushton, L.; Bagga, S.; Bevan, R.; Brown, T.; Cherrie, J.; Holmes, P.; Fortunato, L.; Slack, R.; Van Tongeren, M.; Young, C. Occupation and cancer in Britain. Br. J. Cancer 2010, 102, 1428–1437. [Google Scholar] [CrossRef]
- Crocetto, F.; Pandolfo, S.D.; Aveta, A.; Martino, R.; Trama, F.; Caputo, V.F.; Barone, B.; Abate, M.; Sicignano, E.; Cilio, S.; et al. A Comparative Study of the Triglycerides/HDL Ratio and Pseudocholinesterase Levels in Patients with Bladder Cancer. Diagnostics 2022, 12, 431. [Google Scholar] [CrossRef]
- Chang, S.S.; Bochner, B.H.; Chou, R.; Dreicer, R.; Kamat, A.M.; Lerner, S.P.; Lotan, Y.; Meeks, J.J.; Michalski, J.M.; Morgan, T.M. Treatment of nonmetastatic muscle-invasive bladder cancer: American Urological Association/American Society of Clinical Oncology/American Society for Radiation Oncology/Society of Urologic Oncology clinical practice guideline summary. J. Oncol. Pract. 2017, 13, 621–625. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [Green Version]
- Brandau, S.; Suttmann, H. Thirty years of BCG immunotherapy for non-muscle invasive bladder cancer: A success story with room for improvement. Biomed. Pharmacother. 2007, 61, 299–305. [Google Scholar] [CrossRef]
- Ferro, M.; Tătaru, O.S.; Musi, G.; Lucarelli, G.; Abu Farhan, A.R.; Cantiello, F.; Damiano, R.; Hurle, R.; Contieri, R.; Busetto, G.M.; et al. Modified Glasgow Prognostic Score as a Predictor of Recurrence in Patients with High Grade Non-Muscle Invasive Bladder Cancer Undergoing Intravesical Bacillus Calmette-Guerin Immunotherapy. Diagnostics 2022, 12, 586. [Google Scholar] [CrossRef] [PubMed]
- Pettenati, C.; Ingersoll, M.A. Mechanisms of BCG immunotherapy and its outlook for bladder cancer. Nat. Rev. Urol. 2018, 15, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.; Chiujdea, S.; Musi, G.; Lucarelli, G.; Del Giudice, F.; Hurle, R.; Damiano, R.; Cantiello, F.; Mari, A.; Minervini, A.; et al. Impact of Age on Outcomes of Patients With Pure Carcinoma In Situ of the Bladder: Multi-Institutional Cohort Analysis. Clin. Genitourin. Cancer 2021, 20, e166–e172. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Xu, L.; Yi, M.; Yu, S.; Wu, K.; Luo, S. Novel immune checkpoint targets: Moving beyond PD-1 and CTLA-4. Mol. Cancer 2019, 18, 155. [Google Scholar] [CrossRef] [PubMed]
- Schadendorf, D.; Nghiem, P.; Bhatia, S.; Hauschild, A.; Saiag, P.; Mahnke, L.; Hariharan, S.; Kaufman, H.L. Immune evasion mechanisms and immune checkpoint inhibition in advanced merkel cell carcinoma. Oncoimmunology 2017, 6, e1338237. [Google Scholar] [CrossRef]
- Iacovino, M.L.; Miceli, C.C.; De Felice, M.; Barone, B.; Pompella, L.; Chiancone, F.; Di Zazzo, E.; Tirino, G.; Della Corte, C.M.; Imbimbo, C.; et al. Novel Therapeutic Opportunities in Neoadjuvant Setting in Urothelial Cancers: A New Horizon Opened by Molecular Classification and Immune Checkpoint Inhibitors. Int. J. Mol. Sci. 2022, 23, 1133. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Larissa Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Gonzalez, H.; Hagerling, C.; Werb, Z. Roles of the immune system in cancer: From tumor initiation to metastatic progression. Genes Dev. 2018, 32, 1267–1284. [Google Scholar] [CrossRef] [Green Version]
- Tay, R.E.; Richardson, E.K.; Toh, H.C. Revisiting the role of CD4+ T cells in cancer immunotherapy—New insights into old paradigms. Cancer Gene Ther. 2020, 28, 5–17. [Google Scholar] [CrossRef]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor-Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno-Oncology Biomarkers Working Group: Part 2: TILs in Melanoma, Gastrointestinal Tract Carcinomas, Non-Small Cell Lung Carcinoma and Mesothelioma, Endometrial and Ovarian Carcinomas, Squamous Cell Carcinoma of the Head and Neck, Genitourinary Carcinomas, and Primary Brain Tumors. Adv. Anat. Pathol. 2017, 24, 311–335. [Google Scholar] [CrossRef] [PubMed]
- Farhood, B.; Najafi, M.; Mortezaee, K. CD8(+) cytotoxic T lymphocytes in cancer immunotherapy: A review. J. Cell. Physiol. 2019, 234, 8509–8521. [Google Scholar] [CrossRef] [PubMed]
- Vinay, D.S.; Ryan, E.P.; Pawelec, G.; Talib, W.H.; Stagg, J.; Elkord, E.; Lichtor, T.; Decker, W.K.; Whelan, R.L.; Kumara, H.M.C.S.; et al. Immune evasion in cancer: Mechanistic basis and therapeutic strategies. Semin. Cancer Biol. 2015, 35, S185–S198. [Google Scholar] [CrossRef] [PubMed]
- Callahan, M.K.; Wolchok, J.D. At the bedside: CTLA-4- and PD-1-blocking antibodies in cancer immunotherapy. J. Leukoc. Biol. 2013, 94, 41–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchbinder, E.I.; Desai, A. CTLA-4 and PD-1 Pathways: Similarities, Differences, and Implications of Their Inhibition. Am. J. Clin. Oncol. 2016, 39, 98–106. [Google Scholar] [CrossRef] [Green Version]
- Intlekofer, A.M.; Thompson, C.B. At the bench: Preclinical rationale for CTLA-4 and PD-1 blockade as cancer immunotherapy. J. Leukoc. Biol. 2013, 94, 25–39. [Google Scholar] [CrossRef] [Green Version]
- Contardi, E.; Palmisano, G.L.; Tazzari, P.L.; Martelli, A.M.; Falà, F.; Fabbi, M.; Kato, T.; Lucarelli, E.; Donati, D.; Polito, L.; et al. CTLA-4 is constitutively expressed on tumor cells and can trigger apoptosis upon ligand interaction. Int. J. Cancer 2005, 117, 538–550. [Google Scholar] [CrossRef]
- Zhang, W.; Shi, L.; Zhao, Z.; Du, P.; Ye, X.; Li, D.; Cai, Z.; Han, J.; Cai, J. Disruption of CTLA-4 expression on peripheral blood CD8 + T cell enhances anti-tumor efficacy in bladder cancer. Cancer Chemother. Pharmacol. 2019, 83, 911–920. [Google Scholar] [CrossRef]
- Darvin, P.; Toor, S.M.; Sasidharan Nair, V.; Elkord, E. Immune checkpoint inhibitors: Recent progress and potential biomarkers. Exp. Mol. Med. 2018, 50, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.L.; et al. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421. [Google Scholar] [CrossRef] [Green Version]
- Donin, N.M.; Lenis, A.T.; Holden, S.; Drakaki, A.; Pantuck, A.; Belldegrun, A.; Chamie, K. Immunotherapy for the treatment of urothelial carcinoma. J. Urol. 2017, 197, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.; de Cobelli, O.; Musi, G.; Lucarelli, G.; Terracciano, D.; Pacella, D.; Muto, T.; Porreca, A.; Busetto, G.M.; Del Giudice, F.; et al. Three vs. Four Cycles of Neoadjuvant Chemotherapy for Localized Muscle Invasive Bladder Cancer Undergoing Radical Cystectomy: A Retrospective Multi-Institutional Analysis. Front. Oncol. 2021, 11, 651745. [Google Scholar] [CrossRef] [PubMed]
- Bada, M.; De Concilio, B.; Crocetto, F.; Creta, M.; Silvestri, T.; Di Mauro, M.; Celia, A. Laparoscopic radical cystectomy with extracorporeal urinary diversion: An Italian single-center experience with 10-year outcomes. Minerva Urol. Nefrol. 2020, 72, 641–643. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.; Babă, D.-F.; Cobelli, O.d.; Musi, G.; Lucarelli, G.; Terracciano, D.; Porreca, A.; Busetto, G.M.; Giudice, F.D.; Soria, F. Neutrophil percentage-to-albumin ratio predicts mortality in bladder cancer patients treated with neoadjuvant chemotherapy followed by radical cystectomy. Future Sci. OA 2021, 7, FSO709. [Google Scholar] [CrossRef]
- Raphael, M.J.; Booth, C.M. Neoadjuvant chemotherapy for muscle-invasive bladder cancer: Underused across the 49th parallel. Can. Urol. Assoc. J. 2019, 13, 29–31. [Google Scholar] [CrossRef]
- Scafuri, L.; Sciarra, A.; Crocetto, F.; Ferro, M.; Buonerba, C.; Ugliano, F.; Guerra, G.; Sanseverino, R.; Lorenzo, G.D. Does perioperative systemic therapy represent the optimal therapeutic paradigm in organ-confined, muscle-invasive urothelial carcinoma? Future Sci. OA 2021, 7, Fso770. [Google Scholar] [CrossRef]
- Huo, J.; Ray-Zack, M.D.; Shan, Y.; Chamie, K.; Boorjian, S.A.; Kerr, P.; Jana, B.; Freedland, S.J.; Kamat, A.M.; Mehta, H.B.; et al. Discerning Patterns and Quality of Neoadjuvant Chemotherapy Use Among Patients with Muscle-invasive Bladder Cancer. Eur. Urol. Oncol. 2019, 2, 497–504. [Google Scholar] [CrossRef]
- Grimm, M.O.; Bex, A.; De Santis, M.; Ljungberg, B.; Catto, J.W.F.; Rouprêt, M.; Hussain, S.A.; Bellmunt, J.; Powles, T.; Wirth, M.; et al. Safe Use of Immune Checkpoint Inhibitors in the Multidisciplinary Management of Urological Cancer: The European Association of Urology Position in 2019. Eur. Urol. 2019, 76, 368–380. [Google Scholar] [CrossRef] [Green Version]
- Carthon, B.C.; Wolchok, J.D.; Yuan, J.; Kamat, A.; Ng Tang, D.S.; Sun, J.; Ku, G.; Troncoso, P.; Logothetis, C.J.; Allison, J.P.; et al. Preoperative CTLA-4 blockade: Tolerability and immune monitoring in the setting of a presurgical clinical trial. Clin. Cancer Res. 2010, 16, 2861–2871. [Google Scholar] [CrossRef] [Green Version]
- Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Vuky, J.; Powles, T.; Plimack, E.R.; Hahn, N.M.; de Wit, R.; Pang, L.; et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 1483–1492. [Google Scholar] [CrossRef]
- Crist, M.; Iyer, G.; Hsu, M.; Huang, W.C.; Balar, A.V. Pembrolizumab in the treatment of locally advanced or metastatic urothelial carcinoma: Clinical trial evidence and experience. Ther. Adv. Urol. 2019, 11, 1756287219839285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandini, M.; Ross, J.S.; Raggi, D.; Gallina, A.; Colecchia, M.; Lucianò, R.; Giannatempo, P.; Farè, E.; Pederzoli, F.; Bianchi, M.; et al. Predicting the pathologic complete response after neoadjuvant pembrolizumab in muscle-invasive bladder cancer. J. Natl. Cancer Inst. 2020, 113, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Necchi, A.; Anichini, A.; Raggi, D.; Briganti, A.; Massa, S.; Lucianò, R.; Colecchia, M.; Giannatempo, P.; Mortarini, R.; Bianchi, M.; et al. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J. Clin. Oncol. 2018, 36, 3353–3360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Necchi, A.; Raggi, D.; Gallina, A.; Ross, J.S.; Farè, E.; Giannatempo, P.; Marandino, L.; Colecchia, M.; Lucianò, R.; Bianchi, M.; et al. Impact of Molecular Subtyping and Immune Infiltration on Pathological Response and Outcome Following Neoadjuvant Pembrolizumab in Muscle-invasive Bladder Cancer. Eur. Urol. 2020, 77, 701–710. [Google Scholar] [CrossRef]
- Necchi, A.; Raggi, D.; Gallina, A.; Madison, R.; Colecchia, M.; Lucianò, R.; Montironi, R.; Giannatempo, P.; Farè, E.; Pederzoli, F.; et al. Updated Results of PURE-01 with Preliminary Activity of Neoadjuvant Pembrolizumab in Patients with Muscle-invasive Bladder Carcinoma with Variant Histologies. Eur. Urol. 2020, 77, 439–446. [Google Scholar] [CrossRef]
- Epaillard, N.; Parent, P.; Loriot, Y.; Lavaud, P.; Vera-Cea, E.-B.; Martinez-Chanza, N.; Rodriguez-Vida, A.; Dumont, C.; Lozano, R.; Llácer, C.; et al. Treatments Outcomes in Histological Variants and Non-Urothelial Bladder Cancer: Results of a Multicenter Retrospective Study. Front. Oncol. 2021, 11, 1750. [Google Scholar] [CrossRef]
- Philip, E.J.; Wright, F.; Kim, D.M.; Kwon, D.; Ho, H.; Ho, S.; Cheung, E.; Chan, E.; Porten, S.P.; Wong, A.C.; et al. Efficacy of immune checkpoint inhibitors (ICIs) in rare histological variants of bladder cancer. J. Clin. Oncol. 2020, 38, 502. [Google Scholar] [CrossRef]
- Miller, N.J.; Khaki, A.R.; Diamantopoulos, L.N.; Bilen, M.A.; Santos, V.; Agarwal, N.; Morales-Barrera, R.; Devitt, M.; Nelson, A.; Hoimes, C.J.; et al. Histological Subtypes and Response to PD-1/PD-L1 Blockade in Advanced Urothelial Cancer: A Retrospective Study. J. Urol. 2020, 204, 63–70. [Google Scholar] [CrossRef]
- Daneshmand, S.; Nazemi, A. Neoadjuvant Chemotherapy in Variant Histology Bladder Cancer: Current Evidence. Eur. Urol. Focus 2020, 6, 639–641. [Google Scholar] [CrossRef]
- Briganti, A.; Necchi, A.; Raggi, D.; Giannatempo, P.; Bianchi, M.; Freschi, M.; Colecchia, M.; Fossati, N.; Gandaglia, G.; Salonia, A.; et al. 370—Early surgical safety outcomes from PURE-01: Secondary analysis from a phase 2 open-label study of neoadjuvant pembrolizumab (pembro) before radical cystectomy for muscle-invasive urothelial bladder carcinoma (MIUC). Eur. Urol. Suppl. 2018, 17, e523–e524. [Google Scholar] [CrossRef]
- Briganti, A.; Gandaglia, G.; Scuderi, S.; Gallina, A.; Colombo, R.; Fossati, N.; Barletta, F.; Pellegrino, A.; Nocera, L.; Montorsi, F.; et al. Surgical Safety of Radical Cystectomy and Pelvic Lymph Node Dissection Following Neoadjuvant Pembrolizumab in Patients with Bladder Cancer: Prospective Assessment of Perioperative Outcomes from the PURE-01 Trial. Eur. Urol. 2020, 77, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, A.; Jimeno, A. Atezolizumab: A novel PD-L1 inhibitor in cancer therapy with a focus in bladder and non-small cell lung cancers. Drugs Today 2017, 53, 217–237. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Kockx, M.; Rodriguez-Vida, A.; Duran, I.; Crabb, S.J.; Van Der Heijden, M.S.; Szabados, B.; Pous, A.F.; Gravis, G.; Herranz, U.A.; et al. Clinical efficacy and biomarker analysis of neoadjuvant atezolizumab in operable urothelial carcinoma in the ABACUS trial. Nat. Med. 2019, 25, 1706–1714. [Google Scholar] [CrossRef] [PubMed]
- Hoimes, C.; Albany, C.; Hoffman-Censits, J.; Fleming, M.; Trabulsi, E.; Picus, J.; Cary, C.; Koch, M.; Walling, R.; Kelly, W.; et al. LBA33A phase Ib/II study of neoadjuvant pembrolizumab (pembro) and chemotherapy for locally advanced urothelial cancer (UC). Ann. Oncol. 2018, 29, viii726. [Google Scholar] [CrossRef]
- Kaimakliotis, H.Z.; Adra, N.; Kelly, W.K.; Trabulsi, E.J.; Lauer, R.C.; Picus, J.; Smith, Z.L.; Walling, R.; Masterson, T.A.; Calaway, A.C.; et al. Phase II neoadjuvant (N-) gemcitabine (G) and pembrolizumab (P) for locally advanced urothelial cancer (laUC): Interim results from the cisplatin (C)-ineligible cohort of GU14-188. J. Clin. Oncol. 2020, 38, 5019. [Google Scholar] [CrossRef]
- van Dijk, N.; Gil-Jimenez, A.; Silina, K.; Hendricksen, K.; Smit, L.A.; de Feijter, J.M.; van Montfoort, M.L.; van Rooijen, C.; Peters, D.; Broeks, A.; et al. Preoperative ipilimumab plus nivolumab in locoregionally advanced urothelial cancer: The NABUCCO trial. Nat. Med. 2020, 26, 1839–1844. [Google Scholar] [CrossRef]
- Gupta, S.; Sonpavde, G.; Weight, C.J.; McGregor, B.A.; Gupta, S.; Maughan, B.L.; Wei, X.X.; Gibb, E.; Thyagarajan, B.; Einstein, D.J.; et al. Results from BLASST-1 (Bladder Cancer Signal Seeking Trial) of nivolumab, gemcitabine, and cisplatin in muscle invasive bladder cancer (MIBC) undergoing cystectomy. J. Clin. Oncol. 2020, 38, 439. [Google Scholar] [CrossRef]
- Witjes, J.A.; Bruins, M.; Cathomas, R.; Compérat, E.; Cowan, N.C.; Gakis, G.; Hernández, V.; Lorch, A.; Ribal, M.J.; Thalmann, G.N.; et al. EAU Guidelines on Muscle-invasive and metastatic Bladder Cancer 2020. In European Association of Urology Guidelines. 2020 Edition; Volume presented at the EAU Annual Congress Amsterdam 2020; European Association of Urology Guidelines Office: Arnhem, The Netherlands, 2020. [Google Scholar]
- Kim, H.S.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. Adjuvant chemotherapy for muscle-invasive bladder cancer: A systematic review and network meta-analysis of randomized clinical trials. Oncotarget 2017, 8, 81204–81214. [Google Scholar] [CrossRef] [Green Version]
- Sternberg, C.N.; Donat, S.M.; Bellmunt, J.; Millikan, R.E.; Stadler, W.; De Mulder, P.; Sherif, A.; von der Maase, H.; Tsukamoto, T.; Soloway, M.S. Chemotherapy for bladder cancer: Treatment guidelines for neoadjuvant chemotherapy, bladder preservation, adjuvant chemotherapy, and metastatic cancer. Urology 2007, 69, 62–79. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Bellmunt, J.; Sonpavde, G.; Siefker-Radtke, A.O.; Stadler, W.M.; Bajorin, D.F.; Dreicer, R.; George, D.J.; Milowsky, M.I.; Theodorescu, D.; et al. ICUD-EAU International Consultation on Bladder Cancer 2012: Chemotherapy for urothelial carcinoma-neoadjuvant and adjuvant settings. Eur. Urol. 2013, 63, 58–66. [Google Scholar] [CrossRef]
- Seisen, T.; Jamzadeh, A.; Leow, J.J.; Rouprêt, M.; Cole, A.P.; Lipsitz, S.R.; Kibel, A.S.; Nguyen, P.L.; Sun, M.; Menon, M.; et al. Adjuvant Chemotherapy vs Observation for Patients With Adverse Pathologic Features at Radical Cystectomy Previously Treated With Neoadjuvant Chemotherapy. JAMA Oncol. 2018, 4, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.H.A.; Powles, T.; Albers, P.; Castellano, D.; Daneshmand, S.; Gschwend, J.; Nishiyama, H.; Oudard, S.; Tayama, D.; Davarpanah, N.N.; et al. IMvigor010: Primary analysis from a phase III randomized study of adjuvant atezolizumab (atezo) versus observation (obs) in high-risk muscle-invasive urothelial carcinoma (MIUC). J. Clin. Oncol. 2020, 38, 5000. [Google Scholar] [CrossRef]
- Bellmunt, J.; Hussain, M.; Gschwend, J.E.; Albers, P.; Oudard, S.; Castellano, D.; Daneshmand, S.; Nishiyama, H.; Majchrowicz, M.; Degaonkar, V.; et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021, 22, 525–537. [Google Scholar] [CrossRef]
- Bajorin, D.F.; Witjes, J.A.; Gschwend, J.E.; Schenker, M.; Valderrama, B.P.; Tomita, Y.; Bamias, A.; Lebret, T.; Shariat, S.F.; Park, S.H. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N. Engl. J. Med. 2021, 384, 2102–2114. [Google Scholar] [CrossRef]
- Ilie, M.; Khambata-Ford, S.; Copie-Bergman, C.; Huang, L.; Juco, J.; Hofman, V.; Hofman, P. Use of the 22C3 anti-PD-L1 antibody to determine PD-L1 expression in multiple automated immunohistochemistry platforms. PLoS ONE 2017, 12, e0183023. [Google Scholar] [CrossRef] [Green Version]
- Davis, A.A.; Patel, V.G. The role of PD-L1 expression as a predictive biomarker: An analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 278. [Google Scholar] [CrossRef]
- Khunger, M.; Hernandez, A.V.; Pasupuleti, V.; Rakshit, S.; Pennell, N.A.; Stevenson, J.; Mukhopadhyay, S.; Schalper, K.; Velcheti, V. Programmed Cell Death 1 (PD-1) Ligand (PD-L1) Expression in Solid Tumors As a Predictive Biomarker of Benefit From PD-1/PD-L1 Axis Inhibitors: A Systematic Review and Meta-Analysis. JCO Precis. Oncol. 2017, 1, 1–15. [Google Scholar] [CrossRef]
- Lopez-Beltran, A.; López-Rios, F.; Montironi, R.; Wildsmith, S.; Eckstein, M. Immune Checkpoint Inhibitors in Urothelial Carcinoma: Recommendations for Practical Approaches to PD-L1 and Other Potential Predictive Biomarker Testing. Cancers 2021, 13, 1424. [Google Scholar] [CrossRef]
- Goodman, A.M.; Kato, S.; Bazhenova, L.; Patel, S.P.; Frampton, G.M.; Miller, V.; Stephens, P.J.; Daniels, G.A.; Kurzrock, R. Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers. Mol. Cancer Ther. 2017, 16, 2598–2608. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Samstein, R.M.; Valero, C.; Chan, T.A.; Morris, L.G.T. Tumor mutational burden as a predictive biomarker for checkpoint inhibitor immunotherapy. Hum. Vaccines Immunother. 2020, 16, 112–115. [Google Scholar] [CrossRef]
- Voutsadakis, I.A. Urothelial Bladder Carcinomas with High Tumor Mutation Burden Have a Better Prognosis and Targetable Molecular Defects beyond Immunotherapies. Curr. Oncol. 2022, 29, 1390–1407. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Qian, W.-l.; Yan, W.-f.; Pang, T.; Gong, Y.-l.; Yang, Z.-g. Radiomic assessment as a method for predicting tumor mutation burden (TMB) of bladder cancer patients: A feasibility study. BMC Cancer 2021, 21, 823. [Google Scholar] [CrossRef] [PubMed]
- Hugo, W.; Zaretsky, J.M.; Sun, L.; Song, C.; Moreno, B.H.; Hu-Lieskovan, S.; Berent-Maoz, B.; Pang, J.; Chmielowski, B.; Cherry, G.; et al. Genomic and Transcriptomic Features of Response to Anti-PD-1 Therapy in Metastatic Melanoma. Cell 2016, 165, 35–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayers, M.; Lunceford, J.; Nebozhyn, M.; Murphy, E.; Loboda, A.; Kaufman, D.R.; Albright, A.; Cheng, J.D.; Kang, S.P.; Shankaran, V.; et al. IFN-γ-related mRNA profile predicts clinical response to PD-1 blockade. J. Clin. Investig. 2017, 127, 2930–2940. [Google Scholar] [CrossRef] [PubMed]
- Crocetto, F.; Barone, B.; Ferro, M.; Busetto, G.M.; La Civita, E.; Buonerba, C.; Di Lorenzo, G.; Terracciano, D.; Schalken, J.A. Liquid biopsy in bladder cancer: State of the art and future perspectives. Crit. Rev. Oncol./Hematol. 2022, 170, 103577. [Google Scholar] [CrossRef] [PubMed]
- Martins, I.; Ribeiro, I.P.; Jorge, J.; Gonçalves, A.C.; Sarmento-Ribeiro, A.B.; Melo, J.B.; Carreira, I.M. Liquid Biopsies: Applications for Cancer Diagnosis and Monitoring. Genes 2021, 12, 349. [Google Scholar] [CrossRef]
- Crocetto, F.; Cimmino, A.; Ferro, M.; Terracciano, D. Circulating tumor cells in bladder cancer: A new horizon of liquid biopsy for precision medicine. J. Basic Clin. Physiol. Pharmacol. 2021. [Google Scholar] [CrossRef]
- Kuziora, M.; Higgs, B.W.; Brohawn, P.Z.; Raja, R.; Bais, C.; Ranade, K. Association of early reduction in circulating tumor DNA (ctDNA) with improved progression-free survival (PFS) and overall survival (OS) of patients (pts) with urothelial bladder cancer (UBC) treated with durvalumab (D). J. Clin. Oncol. 2017, 35, 11538. [Google Scholar] [CrossRef]
- Vandekerkhove, G.; Lavoie, J.-M.; Annala, M.; Murtha, A.J.; Sundahl, N.; Walz, S.; Sano, T.; Taavitsainen, S.; Ritch, E.; Fazli, L.; et al. Plasma ctDNA is a tumor tissue surrogate and enables clinical-genomic stratification of metastatic bladder cancer. Nat. Commun. 2021, 12, 184. [Google Scholar] [CrossRef]
- Raja, R.; Kuziora, M.; Brohawn, P.Z.; Higgs, B.W.; Gupta, A.; Dennis, P.A.; Ranade, K. Early Reduction in ctDNA Predicts Survival in Patients with Lung and Bladder Cancer Treated with Durvalumab. Clin. Cancer Res. 2018, 24, 6212–6222. [Google Scholar] [CrossRef] [Green Version]
- Vandekerkhove, G.; Todenhöfer, T.; Annala, M.; Struss, W.J.; Wong, A.; Beja, K.; Ritch, E.; Brahmbhatt, S.; Volik, S.V.; Hennenlotter, J.; et al. Circulating Tumor DNA Reveals Clinically Actionable Somatic Genome of Metastatic Bladder Cancer. Clin. Cancer Res. 2017, 23, 6487–6497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powles, T.; Assaf, Z.J.; Davarpanah, N.; Banchereau, R.; Szabados, B.E.; Yuen, K.C.; Grivas, P.; Hussain, M.; Oudard, S.; Gschwend, J.E.; et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature 2021, 595, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Feng, J.; Weng, Y.; Xu, Z.; Jin, Y.; Wang, P.; Cui, X.; Ruan, P.; Luo, R.; Li, N.; et al. The Prognostic Value of ctDNA and bTMB on Immune Checkpoint Inhibitors in Human Cancer. Front. Oncol. 2021, 11, 706910. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| NCT Number | Other Names | Drug | Phase | Population | Dates |
|---|---|---|---|---|---|
| NCT04506554 | GU-176 | Nivolumab + AMVAC | II | 71 | Study Start: August 2020 Study Completion: August 2023 |
| NCT04383743 | RG1006206 | Pembrolizumab ± Cisplatin ± Doxorubicin ± Methotrexate ± Pegfilgrastim | II | 17 | Study Start: September 2020 Study Completion: February 2023 |
| NCT04289779 | ABATE | Atezolizumab + Cabozantinib | II | 42 | Study Start: May 2020 Study Completion: March 2023 |
| NCT04099589 | NCC2121 | Toripalimab | II | 64 | Study Start: October 2019 Study Completion: October 2022 |
| NCT03978624 | LCCC1827 | Pembrolizumab ± Entinostat | II | 20 | Study Start: March 2020 Study Completion: November 2022 |
| NCT03912818 | IRB-48062 | Durvalumab ± Carboplatin ± Cisplatin ± Doxorubicin ± Gemcitabine ± Methotrexate ± Vinblastine | II | 24 | Study Start: April 2019 Study Completion: August 2022 |
| NCT03832673 | PECULIAR | Pembrolizumab + Epacadostat | II | 38 | Study Start: April 2019 Study Completion: April 2020 |
| NCT03773666 | BLASTT-2 | Durvalumab ± Oleclumab | I | 24 | Study Start: February 2019 Study Completion: July 31 2022 |
| NCT03674424 | AURA | Avelumab | II | 166 | Study Start: June 2018 Study Completion: December 2022 |
| NCT03577132 | SeoulNUHUro_Ate | Atezolizumab | I | 20 | Study Start: August 2018 Study Completion: May 2022 |
| NCT03558087 | HCRN GU16-257 | Nivolumab + Gemcitabine + Cisplatin | II | 76 | Study Start: July 2018 Study Completion: August 2023 |
| NCT03549715 | NEMIO | Durvalumab + Tremelimumab + Methotrexate + Vinblastine + Adryamicin + Cisplatin | II | 120 | Study Start: December 2018 Study Completion: September 2025 |
| NCT03534492 | NEODURVARIB | Durvalumab + Olaparib | II | 29 | Study Start: November 2018 Study Completion: March 16, 2020 |
| NCT03532451 | PrE0807 | Nivolumab ± Lirilumab | I | 43 | Study Start: March 2019 Study Completion: September 2022 |
| NCT03529890 | RACE IT | Nivolumab | II | 33 | Study Start: February 2019 Study Completion: August 2022 |
| NCT03520491 | 18-042 | Nivolumab ± Ipilimumab | II | 45 | Study Start: April 2018 Study Completion: January 2021 |
| NCT03518320 | TAR-200-104 | Nivolumab + Gemcitabine | I | 13 | Study Start: January 2019 Study Completion: December 2019 |
| NCT03498196 | H-41207 | Avelumab | II | 1 | Study Start: December 2018 Study Completion: December 2019 |
| NCT03472274 | DUTRENEO | Durvalumab + Tremelimumab | II | 99 | Study Start: October 2018 Study Completion: December 2022 |
| NCT03319745 | P30CA016672 | Pembrolizumab | II | 20 | Study Start: January 2018 Study Completion: November 2020 |
| NCT03234153 | NITIMIB | Durvalumab + Tremelimumab | II | 6 | Study Start: July 2018 Study Completion: May 2020 |
| NCT03212651 | PANDORE | Pembrolizumab | II | 41 | Study Start: October 2017 Study Completion: October 2019 |
| NCT02989584 | 16-1428 | Atezolizumab + Gemcitabine + Cisplatin | II | 54 | Study Start: December 2016 Study Completion: December 2021 |
| NCT02845323 | J1682 | Nivolumab ± Urelumab | II | 44 | Study Start: May 2017 Study Completion: January 2021 |
| NCT02812420 | P30CA016672 | Durvalumab + Tremelimumab | I | 54 | Study Start: March 2017 Study Completion: March 2022 |
| NCT02690558 | LCCC 1520 | Pembrolizumab + Gemcitabine + Cisplatin | II | 19 | Study Start: May 2016 Study Completion: September 2025 |
| NCT02451423 | 14524 | Atezolizumab | II | 42 | Study Start: June 2016 Study Completion: December 2021 |
| NCT02891161 | DUART | Durvalumab | II | 26 | Study Start: November 2016 Study Completion: November 2021 |
| NCT03406650 | SAKK 06/17 | Durvalumab | II | 61 | Study Start: May 2018 Study Completion: April 2026 |
| NCT03732677 | NIAGARA | Durvalumab ± Gemcitabine ± Cisplatin | III | 1050 | Study Start: November 2018 Study Completion: December 2025 |
| NCT03661320 | CA017-078 | Nivolumab ± BMS-986205 ± Gemcitabine ± Cisplatin | III | 1200 | Study Start: October 2018 Study Completion: December 2026 |
| NCT03924856 | KEYNOTE-866 | Pembrolizumab ± Gemcitabine + Cisplatin | III | 790 | Study Start: June 2019 Study Completion: January 2025 |
| NCT03924895 | KEYNOTE-905 | Pembrolizumab ± Enfortumab Vedotin | III | 836 | Study Start: July 2019 Study Completion: February 2026 |
| NCT Number | Other Names | Drug | Phase | Population | Dates |
|---|---|---|---|---|---|
| NCT04138628 | TOMBOLA | Atezolizumab | II | 262 | Study Start: March 2020 Study Completion: November 2024 |
| NCT03768570 | BL13 | Durvalumab | II | 238 | Study Start: December 2018 Study Completion: December 2024 |
| NCT03620435 | ML-39576 | Atezolizumab | II | 25 | Study Start: May 2018 Study Completion: December 2020 |
| NCT03359239 | GCO 16-1387 | Atezolizumab + PGV001 + Poly ICLC | I | 15 | Study Start: May 2019 Study Completion: January 2022 |
| NCT03244384 | AMBASSADOR | Pembrolizumab | III | 739 | Study Start: September 2017 Study Completion: June 2025 |
| NCT03171025 | NEXT | Nivolumab | II | 28 | Study Start: July 2017 Study Completion: June 2024 |
| NCT02897765 | NT-001 | NEO- PV-01 + Nivolumab | I | 55 | Study Start: October 2016 Study Completion: May 2020 |
| NCT02450331 | IMvigor010 | Atezolizumab | III | 809 | Study Start: October 2015 Study Completion: May 2022 |
| NCT02632409 | CheckMate 274 | Nivolumab | III | 700 | Study Start: February 2016 Study Completion: November 2026 |
| NCT Number | Title | Other Names | Drug | Phase | Population | Dates |
|---|---|---|---|---|---|---|
| NCT03387761 | Neo-Adjuvant Bladder Urothelial Carcinoma Combination-immunotherapy | NABUCCO | Ipilimumab + Nivolumab | I | 54 | Study Start: January 2018 Study Completion: June 2021 |
| NCT02662309 | Preoperative MPDL3280A in Transitional Cell Carcinoma of the Bladder | ABACUS | Atezolizumab | II | 96 | Study Start: February 2016 Study Completion: July 2020 |
| NCT02736266 | Neoadjuvant Pembrolizumab for Muscle-invasive Urothelial Bladder Carcinoma | PURE-01 | Pembrolizumab | II | 90 | Study Start: February 2017 Study Completion: December 2019 |
| NCT02365766 | Neoadjuvant Pembrolizumab in Combination With Gemcitabine Therapy in Cis-eligible/Ineligible UC Subjects | GU14-188 | Pembrolizumab ± Gemcitabine ± Cisplatin | I | 83 | Study Start: May 2015 Study Completion: July 2021 |
| NCT03294304 | BLASST-1 (Bladder Cancer Signal Seeking Trial): Nivolumab, Gemcitabine and Cisplatin in Treatment of Muscle Invasive Bladder Cancer (MIBC) Undergoing Cystectomy | BLASST-1 | Nivolumab + Gemcitabine + Cisplatin | II | 43 | Study Start: January 2018 Study Completion: December 2020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barone, B.; Calogero, A.; Scafuri, L.; Ferro, M.; Lucarelli, G.; Di Zazzo, E.; Sicignano, E.; Falcone, A.; Romano, L.; De Luca, L.; et al. Immune Checkpoint Inhibitors as a Neoadjuvant/Adjuvant Treatment of Muscle-Invasive Bladder Cancer: A Systematic Review. Cancers 2022, 14, 2545. https://doi.org/10.3390/cancers14102545
Barone B, Calogero A, Scafuri L, Ferro M, Lucarelli G, Di Zazzo E, Sicignano E, Falcone A, Romano L, De Luca L, et al. Immune Checkpoint Inhibitors as a Neoadjuvant/Adjuvant Treatment of Muscle-Invasive Bladder Cancer: A Systematic Review. Cancers. 2022; 14(10):2545. https://doi.org/10.3390/cancers14102545
Chicago/Turabian StyleBarone, Biagio, Armando Calogero, Luca Scafuri, Matteo Ferro, Giuseppe Lucarelli, Erika Di Zazzo, Enrico Sicignano, Alfonso Falcone, Lorenzo Romano, Luigi De Luca, and et al. 2022. "Immune Checkpoint Inhibitors as a Neoadjuvant/Adjuvant Treatment of Muscle-Invasive Bladder Cancer: A Systematic Review" Cancers 14, no. 10: 2545. https://doi.org/10.3390/cancers14102545