
Impact of HER2 Status on Pathological Response after Neoadjuvant Chemotherapy in Early Triple-Negative Breast Cancer

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
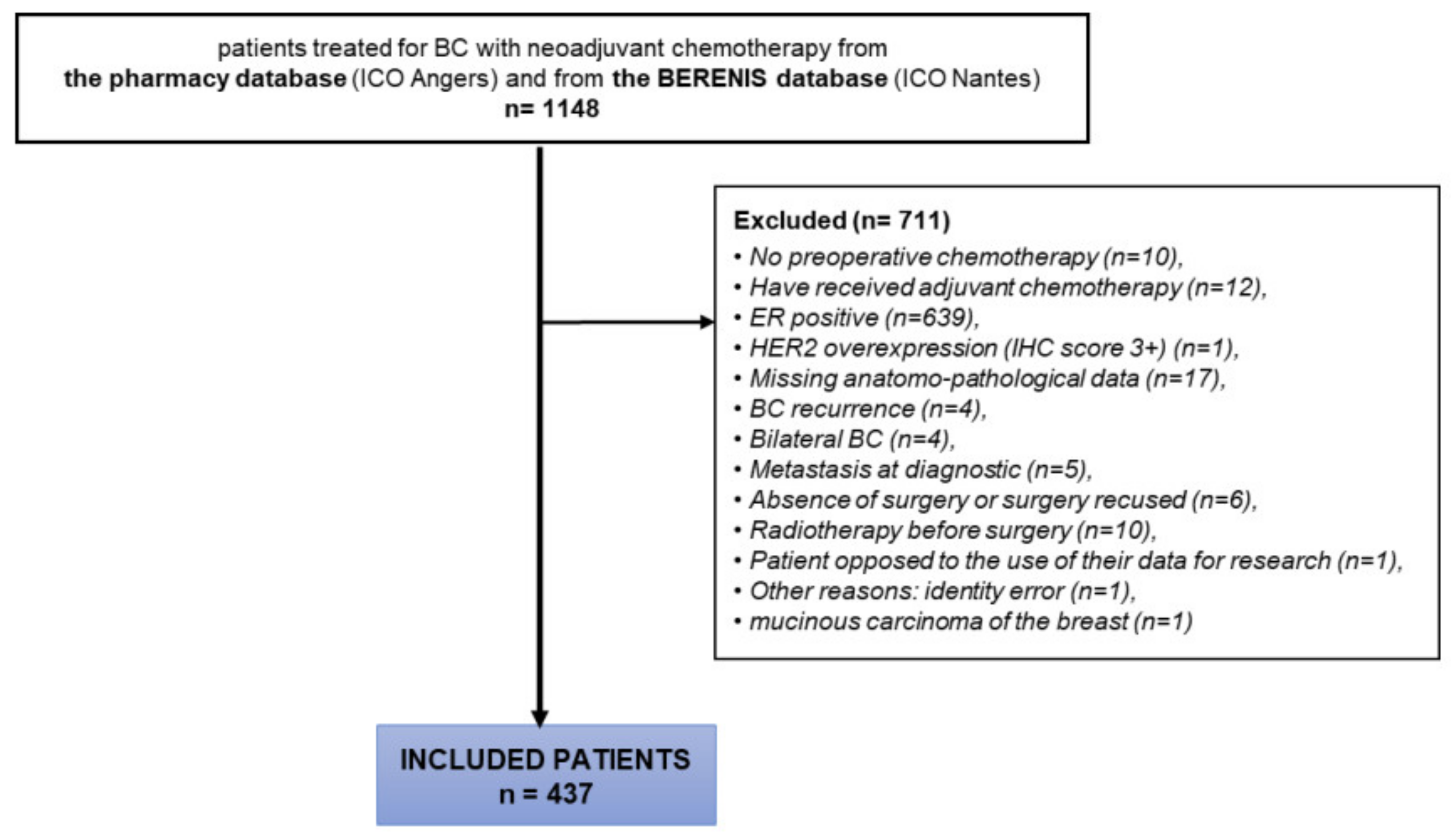
2.1. Study Design
2.2. Definition of the End Points
2.3. Statistical Analysis
3. Results
3.1. Patient and Tumour Characteristics
3.2. Predictive Value of HER2 Status on pCR
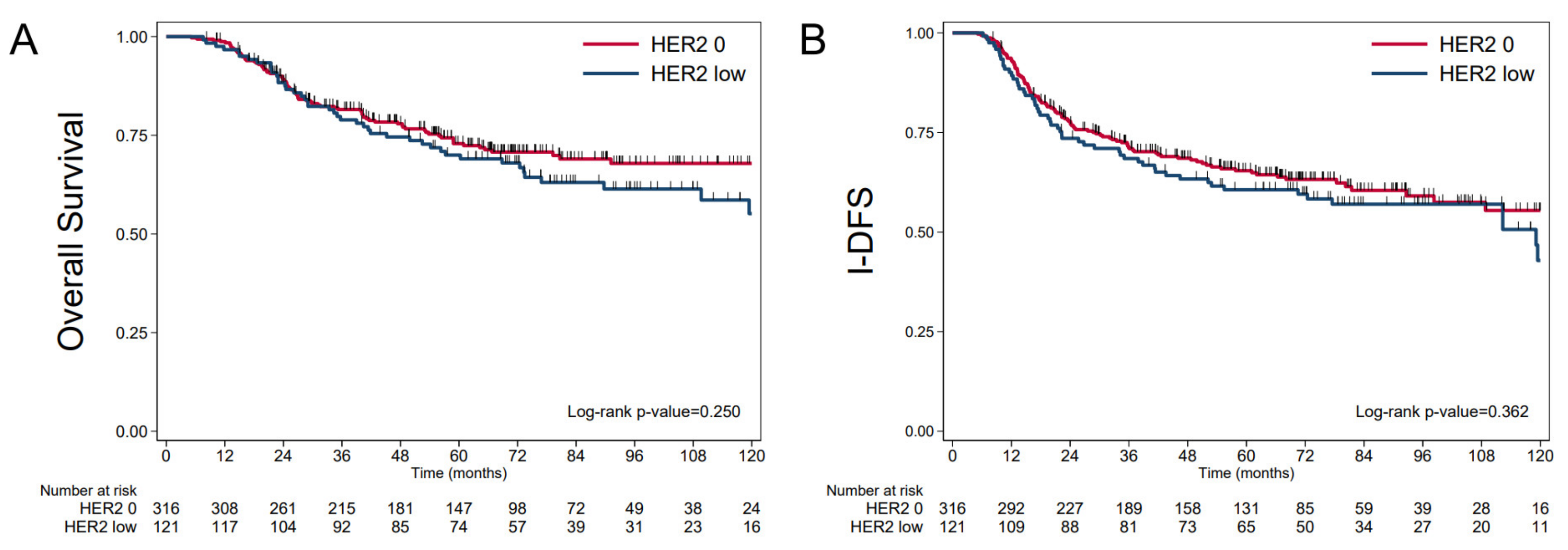
3.3. Prognostic Value of HER2 Status
3.4. Prognostic Value of PLR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Freres, P.; Collignon, J.; Gennigens, C.; Scagnol, I.; Rorive, A.; Barbeaux, A.; Coucke, P.A. Jérusalem Gle cancer du sein «triple né-gatif». Rev. Med. Liège 2010, 65, 120–126. [Google Scholar]
- Miller, K.; Wang, M.; Gralow, J.; Dickler, M.; Cobleigh, M.; Perez, E.A.; Shenkier, T.; Cella, D.; Davidson, N.E. Paclitaxel plus Bevacizumab versus Paclitaxel Alone for Metastatic Breast Cancer. N. Engl. J. Med. 2007, 357, 2666–2676. [Google Scholar] [CrossRef] [Green Version]
- Nabholtz, J.M.; Abrial, C.; Mouret-Reynier, M.-A.; Dauplat, M.M.; Weber, B.; Gligorov, J.; Forest, A.M.; Tredan, O.; Vanlemmens, L.; Petit, T.; et al. Multicentric neoadjuvant phase II study of panitumumab combined with an anthracycline/taxane-based chemotherapy in operable triple-negative breast cancer: Identification of biologically defined signatures predicting treatment impact. Ann. Oncol. 2014, 25, 1570–1577. [Google Scholar] [CrossRef]
- Mateo, J.; Lord, C.J.; Serra, V.; Tutt, A.; Balmaña, J.; Castroviejo-Bermejo, M.; Cruz, C.; Oaknin, A.; Kaye, S.B.; de Bono, J.S. A decade of clinical development of PARP inhibitors in perspective. Ann. Oncol. 2019, 30, 1437–1447. [Google Scholar] [CrossRef] [Green Version]
- Tutt, A.N.; Garber, J.E.; Kaufman, B.; Viale, G.; Fumagalli, D.; Rastogi, P.; Gelber, R.D.; de Azambuja, E.; Fielding, A.; Balmaña, J.; et al. Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer. N. Engl. J. Med. 2021, 384, 2394–2405. [Google Scholar] [CrossRef]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; Van De Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef]
- Sorlie, T.; Perou, C.M.; Tibshirani, R.; Aas, T.; Geisler, S.; Johnsen, H.; Hastie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl. Acad. Sci. USA 2001, 98, 10869–10874. [Google Scholar] [CrossRef] [Green Version]
- Foulkes, W.D.; Smith, I.E.; Reis-Filho, J.S. Triple-Negative Breast Cancer. N. Engl. J. Med. 2010, 363, 1938–1948. [Google Scholar] [CrossRef] [Green Version]
- Deconstructing the Molecular Portraits of Breast Cancer—Prat A and Perou CM—2011—Molecular Oncology—Wiley Online Library. Available online: https://febs.onlinelibrary.wiley.com/doi/full/10.1016/j.molonc.2010.11 (accessed on 9 May 2021).
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J. Clin. Investig. 2011, 121, 2750–2767. [Google Scholar] [CrossRef] [Green Version]
- Farmer, P.; Bonnefoi, H.; Becette, V.; Tubiana-Hulin, M.; Fumoleau, P.; Larsimont, D.; MacGrogan, G.; Bergh, J.; Cameron, D.; Goldstein, D.; et al. Identification of molecular apocrine breast tumours by microarray analysis. Oncogene 2005, 24, 4660–4671. [Google Scholar] [CrossRef] [Green Version]
- Jézéquel, P.; Kerdraon, O.; Hondermarck, H.; Guérin-Charbonnel, C.; Lasla, H.; Gouraud, W.; Canon, J.-L.; Gombos, A.; Dalenc, F.; Delaloge, S.; et al. Identification of three subtypes of triple-negative breast cancer with potential therapeutic implications. Breast Cancer Res. 2019, 21, 65. [Google Scholar] [CrossRef]
- Schettini, F.; Chic, N.; Brasó-Maristany, F.; Paré, L.; Pascual, T.; Conte, B.; Martínez-Sáez, O.; Adamo, B.; Vidal, M.; Barnadas, E.; et al. Clinical, pathological, and PAM50 gene expression features of HER2-low breast cancer. NPJ Breast Cancer 2021, 7, 1. [Google Scholar] [CrossRef]
- Tarantino, P.; Hamilton, E.; Tolaney, S.M.; Cortes, J.; Morganti, S.; Ferraro, E.; Marra, A.; Viale, G.; Trapani, D.; Cardoso, F.; et al. HER2-Low Breast Cancer: Pathological and Clinical Landscape. J. Clin. Oncol. 2020, 38, 1951–1962. [Google Scholar] [CrossRef]
- Takegawa, N.; Tsurutani, J.; Kawakami, H.; Yonesaka, K.; Kato, R.; Haratani, K.; Hayashi, H.; Takeda, M.; Nonagase, Y.; Maenishi, O.; et al. [fam-] trastuzumab deruxtecan, antitumor activity is dependent on HER2 expression level rather than on HER2 amplification. Int. J. Cancer 2019, 145, 3414–3424. [Google Scholar] [CrossRef]
- Modi, S.; Park, H.; Murthy, R.K.; Iwata, H.; Tamura, K.; Tsurutani, J.; Moreno-Aspitia, A.; Doi, T.; Sagara, Y.; Redfern, C.; et al. Antitumor Activity and Safety of Trastuzumab Deruxtecan in Patients With HER2-Low–Expressing Advanced Breast Cancer: Results From a Phase Ib Study. J. Clin. Oncol. 2020, 38, 1887–1896. [Google Scholar] [CrossRef]
- Pernas, S.; Tolaney, S.M. Targeting HER2 heterogeneity in early-stage breast cancer. Curr. Opin. Oncol. 2020, 32, 545–554. [Google Scholar] [CrossRef]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Esserman, L.J.; Berry, D.A.; Cheang, M.C.U.; Yau, C.; Perou, C.M.; Carey, L.; DeMichele, A.; Gray, J.W.; Conway-Dorsey, K.; Lenburg, M.E.; et al. Chemotherapy response and recurrence-free survival in neoadjuvant breast cancer depends on biomarker profiles: Results from the I-SPY 1 TRIAL (CALGB 150007/150012; ACRIN 6657). Breast Cancer Res. Treat. 2011, 132, 1049–1062. [Google Scholar] [CrossRef] [Green Version]
- Liedtke, C.; Mazouni, C.; Hess, K.R.; André, F.; Tordai, A.; Mejia, J.A.; Symmans, W.F.; Gonzalez-Angulo, A.M.; Hennessy, B.; Green, M.; et al. Response to Neoadjuvant Therapy and Long-Term Survival in Patients With Triple-Negative Breast Cancer. J. Clin. Oncol. 2008, 26, 1275–1281. [Google Scholar] [CrossRef]
- Masuda, H.; Baggerly, K.A.; Wang, Y.; Zhang, Y.; Gonzalez-Angulo, A.M.; Meric-Bernstam, F.; Valero, V.; Lehmann, B.D.; Pietenpol, J.A.; Hortobagyi, G.N.; et al. Differential Response to Neoadjuvant Chemotherapy Among 7 Triple-Negative Breast Cancer Molecular Subtypes. Clin. Cancer Res. 2013, 19, 5533–5540. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Xu, B.; Yuan, P.; Li, Q.; Zhang, P.; Cai, R.; Ma, F.; Fan, Y.; Luo, Y. HER2 as a Predictive Factor for Successful Neoadjuvant Anthracycline Chemotherapy of Locally Advanced and Early Breast Cancer. Int. J. Biol. Markers 2014, 29, 187–192. [Google Scholar] [CrossRef]
- Templeton, A.J.; Ace, O.; McNamara, M.G.; Al-Mubarak, M.; Vera-Badillo, F.E.; Hermanns, T.; Seruga, B.; Ocana, A.; Tannock, I.F.; Amir, E. Prognostic role of platelet to lymphocyte ratio in solid tumors: A systematic review and meta-analysis. Cancer Epidemiol. Prev. Biomark. 2014, 23, 1204–1212. [Google Scholar] [CrossRef] [Green Version]
- Asano, Y.; Kashiwagi, S.; Onoda, N.; Noda, S.; Kawajiri, H.; Takashima, T.; Ohsawa, M.; Kitagawa, S.; Hirakawa, K. Predictive Value of Neutrophil/Lymphocyte Ratio for Efficacy of Preoperative Chemotherapy in Triple-Negative Breast Cancer. Ann. Surg. Oncol. 2015, 23, 1104–1110. [Google Scholar] [CrossRef] [Green Version]
- Huszno, J.; Kolosza, Z. Prognostic value of the neutrophil-lymphocyte, platelet-lymphocyte and monocyte-lymphocyte ratio in breast cancer patients. Oncol. Lett. 2019, 18, 6275–6283. [Google Scholar] [CrossRef]
- Liu, C.; Huang, Z.; Wang, Q.; Sun, B.; Ding, L.; Meng, X.; Wu, S. Usefulness of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in hormone-receptor-negative breast cancer. OncoTargets Ther. 2016, 9, 4653–4660. [Google Scholar] [CrossRef] [Green Version]
- Losada, B.; Guerra, J.A.; Malón, D.; Jara, C.; Rodriguez, L.; Del Barco, S. Pretreatment neutrophil/lymphocyte, platelet/lymphocyte, lymphocyte/monocyte, and neutrophil/monocyte ratios and outcome in elderly breast cancer patients. Clin. Transl. Oncol. 2018, 21, 855–863. [Google Scholar] [CrossRef]
- Cuello-López, J.; Fidalgo-Zapata, A.; López-Agudelo, L.; Vasquez-Trespalacios, E.M. Platelet-to-lymphocyte ratio as a predictive factor of complete pathologic response to neoadjuvant chemotherapy in breast cancer. PLoS ONE 2018, 13, e0207224. [Google Scholar] [CrossRef] [Green Version]
- Asano, Y.; Kashiwagi, S.; Onoda, N.; Noda, S.; Kawajiri, H.; Takashima, T.; Ohsawa, M.; Kitagawa, S.; Hirakawa, K. Platelet–Lymphocyte Ratio as a Useful Predictor of the Therapeutic Effect of Neoadjuvant Chemotherapy in Breast Cancer. PLoS ONE 2016, 11, e0153459. [Google Scholar] [CrossRef] [Green Version]
- Wiranata, S.; Anjani, I.A.W.; Saputra, I.P.G.S.; Sadvika, I.G.A.S.; Prabawa, I.P.Y.; Supadmanaba, I.G.; Wihandani, D.M.; Adiputra, P.A.T.; Sudarsa, I.W.; Lestari, A.A.W. Pretreatment Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio as a Stage Determination in Breast Cancer. Open Access Maced. J. Med Sci. 2020, 8, 1058–1063. [Google Scholar] [CrossRef]
- Research C for DE and Pathological Complete Response in Neoadjuvant Treatment of High-Risk EarlyStage Breast Cancer: Use as an Endpoint to Support Accelerated Approval. In U.S. Food and Drug Administration. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/pathologicalcomplete-response-neoadjuvant-treatment-high-risk-early-stage-breast-cancer-use (accessed on 10 May 2022).
- Gourgou-Bourgade, S.; Cameron, D.; Poortmans, P.; Asselain, B.; Azria, D.; Cardoso, F.; A’Hern, R.; Bliss, J.; Bogaerts, J.; Bonnefoi, H.; et al. Guidelines for time-to-event end point definitions in breast cancer trials: Results of the DATECAN initiative (Definition for the Assessment of Time-to-event Endpoints in CANcer trials). Ann. Oncol. 2015, 26, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.R.; Cain, K.C.; Gelber, R.D. Analysis of Survival by Tumor Response and Other Comparisons of Time-to-Event by Outcome Variables. J. Clin. Oncol. 2008, 26, 3913–3915. [Google Scholar] [CrossRef] [PubMed]
- Scott, M.; Vandenberghe, M.E.; Scorer, P.; Boothman, A.-M.; Barker, C. Prevalence of HER2 low in breast cancer subtypes using the VENTANA anti-HER2/neu (4B5) assay. J. Clin. Oncol. 2021, 39, 1021. [Google Scholar] [CrossRef]
- Brasó-Maristany, F.; Paré, L.; Chic, N.; Martínez-Sáez, O.; Pascual, T.; Mallafré-Larrosa, M.; Schettini, F.; González-Farré, B.; Sanfeliu, E.; Martínez, D.; et al. Gene expression profiles of breast cancer metastasis according to organ site. Mol. Oncol. 2021, 16, 69–87. [Google Scholar] [CrossRef] [PubMed]
- Prat, A.; Adamo, B.; Cheang, M.C.U.; Anders, C.K.; Carey, L.A.; Perou, C.M. Molecular Characterization of Basal-Like and Non-Basal-Like Triple-Negative Breast Cancer. Oncologist 2013, 18, 123–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehmann, B.D.; Pietenpol, J.A. Identification and use of biomarkers in treatment strategies for triple-negative breast cancer subtypes. J. Pathol. 2014, 232, 142–150. [Google Scholar] [CrossRef]
- Huober, J.; Von Minckwitz, G.; Denkert, C.; Tesch, H.; Weiss, E.; Zahm, D.M.; Belau, A.; Khandan, F.; Hauschild, M.; Thomssen, C.; et al. Effect of neoadjuvant anthracycline–taxane-based chemotherapy in different biological breast cancer phenotypes: Overall results from the GeparTrio study. Breast Cancer Res. Treat. 2010, 124, 133–140. [Google Scholar] [CrossRef]
- Gonçalves, A. Chimiothérapie néo-adjuvante des cancers du sein HER2-positifs et triple-négatifs. Bull. Cancer 2016, 103, S76–S89. [Google Scholar] [CrossRef]
- Wang, J.; Xu, B.; Yuan, P.; Zhang, P.; Li, Q.; Ma, F.; Fan, Y. TOP2A amplification in breast cancer is a predictive marker of anthracycline-based neoadjuvant chemotherapy efficacy. Breast Cancer Res. Treat. 2012, 135, 531–537. [Google Scholar] [CrossRef]
- Santonja, A.; Sánchez-Muñoz, A.; Lluch, A.; Chica-Parrado, M.R.; Albanell, J.; Chacón, J.I.; Antolín, S.; Jerez, J.M.; De La Haba, J.; De Luque, V.; et al. Triple negative breast cancer subtypes and pathologic complete response rate to neoadjuvant chemotherapy. Oncotarget 2018, 9, 26406–26416. [Google Scholar] [CrossRef] [Green Version]
- Echavarria, I.; López-Tarruella, S.; Picornell, A.C.; García-Saenz, J.; Jerez-Gilarranz, Y.; Hoadley, K.A.; Gómez, H.L.; Moreno, F.; Del Monte-Millan, M.; Márquez-Rodas, I.; et al. Pathological Response in a Triple-Negative Breast Cancer Cohort Treated with Neoadjuvant Carboplatin and Docetaxel According to Lehmann’s Refined Classification. Clin. Cancer Res. 2018, 24, 1845–1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denkert, C.; Seither, F.; Schneeweiss, A.; Link, T.; Blohmer, J.-U.; Just, M.; Wimberger, P.; Forberger, A.; Tesch, H.; Jackisch, C.; et al. Clinical and molecular characteristics of HER2-low-positive breast cancer: Pooled analysis of individual patient data from four prospective, neoadjuvant clinical trials. Lancet Oncol. 2021, 22, 1151–1161. [Google Scholar] [CrossRef]
- Leite, L.D.M.; Cesca, M.G.; Tavares, M.C.; Santana, D.M.; Saldanha, E.F.; Guimarães, P.T.; Sá, D.D.S.; Simões, M.F.E.; Viana, R.L.; Rocha, F.G.; et al. HER2-low status and response to neoadjuvant chemotherapy in HER2 negative early breast cancer. Breast Cancer Res. Treat. 2021, 190, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Reinert, T.; Sartori, G.P.; AB Souza, A.; Pellegrini, R.; Rosa, M.L.; Rossatto, N.; Coelho, G.P.; Litvin, I.E.; Zerwes, F.; Millen, E.; et al. Abstract PS4-22: Prevalence of HER2-low and HER2-zero subgroups and correlation with response to neoadjuvant chemotherapy (NACT) in patients with HER2-negative breast cancer. Cancer Res. 2021, 81, PS4-22. [Google Scholar] [CrossRef]
- Rossi, V.; Sarotto, I.; Maggiorotto, F.; Berchialla, P.; Kubatzki, F.; Tomasi, N.; Redana, S.; Martinello, R.; Valabrega, G.; Aglietta, M.; et al. Moderate Immunohistochemical Expression of HER-2 (2+) Without HER-2 Gene Amplification Is a Negative Prognostic Factor in Early Breast Cancer. Oncologist 2012, 17, 1418–1425. [Google Scholar] [CrossRef] [Green Version]
- De Azambuja, E.; Cardoso, F.; De Castro, G.; Colozza, M.; Mano, M.S.; Durbecq, V.; Sotiriou, C.; Larsimont, D.; Piccart-Gebhart, M.; Paesmans, M. Ki-67 as prognostic marker in early breast cancer: A meta-analysis of published studies involving 12 155 patients. Br. J. Cancer 2007, 96, 1504–1513. [Google Scholar] [CrossRef] [Green Version]
- Colozza, M.; Azambuja, E.; Cardoso, F.; Sotiriou, C.; Larsimont, D.; Piccart, M.J. Proliferative markers as prognostic and predictive tools in early breast cancer: Where are we now? Ann. Oncol. 2005, 16, 1723–1739. [Google Scholar] [CrossRef]
- Zhu, X.; Chen, L.; Huang, B.; Wang, Y.; Ji, L.; Wu, J.; Di, G.; Liu, G.; Yu, K.; Shao, Z.; et al. The prognostic and predictive potential of Ki-67 in triple-negative breast cancer. Sci. Rep. 2020, 10, 225. [Google Scholar] [CrossRef] [Green Version]
- Denkert, C.; Loibl, S.; Müller, B.M.; Eidtmann, H.; Schmitt, W.; Eiermann, W.; Gerber, B.; Tesch, H.; Hilfrich, J.; Huober, J.; et al. Ki67 levels as predictive and prognostic parameters in pretherapeutic breast cancer core biopsies: A translational investigation in the neoadjuvant GeparTrio trial. Ann. Oncol. 2013, 24, 2786–2793. [Google Scholar] [CrossRef]
- Seretis, C.; Seretis, F.; Lagoudianakis, E.; Politou, M.; Gemenetzis, G.; Salemis, N.S. Enhancing the Accuracy of Platelet to Lymphocyte Ratio after Adjustment for Large Platelet Count: A Pilot Study in Breast Cancer Patients. Int. J. Surg. Oncol. 2012, 2012, 653608. [Google Scholar] [CrossRef] [Green Version]
- Krenn-Pilko, S.; Langsenlehner, T.; Thurner, E.-M.; Stojakovic, T.; Pichler, M.; Gerger, A.; Kapp, K.S. The elevated preoperative platelet-to-lymphocyte ratio predicts poor prognosis in breast cancer patients. Br. J. Cancer 2014, 110, 2524–2530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.-Y.; Jung, E.J.; Kim, J.-M.; Lee, H.S.; Kwag, S.-J.; Park, J.-H.; Park, T.; Jeong, S.-H.; Jeong, C.-Y.; Ju, Y.-T. Dynamic changes of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio predicts breast cancer prognosis. BMC Cancer 2020, 20, 1206. [Google Scholar] [CrossRef] [PubMed]
- Marchiò, C.; Annaratone, L.; Marques, A.; Casorzo, L.; Berrino, E.; Sapino, A. Evolving concepts in HER2 evaluation in breast cancer: Heterogeneity, HER2-low carcinomas and beyond. Semin. Cancer Biol. 2020, 72, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Sapino, A.; Goia, M.; Recupero, D.; Marchiò, C. Current Challenges for HER2 Testing in Diagnostic Pathology: State of the Art and Controversial Issues. Front. Oncol. 2013, 3, 129. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.; Gao, R.; Sei, E.; Brandt, R.; Hartman, J.; Hatschek, T.; Crosetto, N.; Foukakis, T.; Navin, N.E. Chemoresistance Evolution in Triple-Negative Breast Cancer Delineated by Single-Cell Sequencing. Cell 2018, 173, 879–893.e13. [Google Scholar] [CrossRef] [Green Version]
- Garrido-Castro, A.C.; Lin, N.U.; Polyak, K. Insights into Molecular Classifications of Triple-Negative Breast Cancer: Improving Patient Selection for Treatment. Cancer Discov. 2019, 9, 176–198. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| HER2-0 (n = 316) | HER2-Low (n = 121) | p-Value | Total (n = 437) | |
|---|---|---|---|---|
| Age at diagnostic | ||||
| Median (range) | 51.0 (25–89) | 52.0 (22–89) | 51.0 (22–89) | |
| Histological type | ||||
| Non-specific | 304 (96.2%) | 112 (92.6%) | 416 (95.2%) | |
| Invasive lobular | 4 (1.3%) | 3 (2.5%) | 7 (1.6%) | |
| Apocrine | 1 (0.3%) | 2 (1.7%) | 3 (0.7%) | |
| Other histological type | 7 (2.2%) | 4 (3.2%) | 11 (2.5%) | |
| Stage T | p = 0.053 | |||
| T0-T1 | 15 (4.7%) | 15 (12.4%) | 30 (6.7%) | |
| T2 | 178 (56.3%) | 66 (54.5%) | 252 (56.1%) | |
| T3 | 81 (25.6%) | 26 (21.5%) | 110 (24.5%) | |
| T4 | 42 (13.3%) | 14 (11.6%) | 57 (12.7%) | |
| Stage N | p = 0.662 | |||
| N0 | 122/315 (38.7%) | 50/121 (41.3%) | 172 (39.4%) | |
| N+ | 193/315 (61.3%) | 71/121 (58.7%) | 264 (60.6%) | |
| RE | ||||
| 0 | 295/315 (93.7%) | 116/120 (96.7%) | 423/447 (94.5%) | |
| 1–10% | 20/315 (6.3%) | 4/120 (3.3%) | 24/447 (5.5%) | |
| HER2 status | ||||
| 1+ | 0 | 90/119 (76.3%) | ||
| 2+ | 0 | 28/119 (23.7%) | ||
| mSBR grade | p = 0.452 | |||
| Grade II | 72/313 (23%) | 32/120 (26.7%) | 104/433 (24%) | |
| Grade III | 241/313 (77%) | 88/120 (73.3%) | 329/433 (76%) | |
| Mitotic index (/mm2) | ||||
| Median (range) | 8.1 (1.1–31.5) | 8.8 (0.0, 30.0) | 8.3 (0.0, 31.5) | |
| Missing | 254 | 99 | 353 | |
| Ki67 (%) | p = 0.011 | |||
| Median (range) | 50.0 (10.0, 90.0) | 64.0 (10.0, 95.0) | 52.0 (10.0, 95.0) | |
| Missing | 199 | 85 | 284 | |
| Neoadjuvant chemotherapy | p = 0.013 | |||
| Anthracycline-taxane (A-T) | 301/316 (95,3%) | 114/121 (94,2%) | 415/437 (95%) | |
| A-T dose dense regimen | 48/316 (15.2%) | 9/121 (7.4%) | 57/437 (13%) | |
| Platinum salts | 33/316 (10.4%) | 5/121(4.1%) | 38/448 (8.7%) | |
| Mammary surgery | p = 0.226 | |||
| Mastectomy | 107 (33.1%) | 50 (39.7%) | 157 (35.0%) | |
| Conservative | 216 (66.9%) | 76 (60.3%) | 292 (65.0%) | |
| Germline mutation | ||||
| Number of screened patients | 125 | 48 | 173 | |
| BRCA1 | 18 (14.4%) | 8 (16.7%) | 26 (15.0%) | |
| BRCA2 | 9 (7.2%) | 1 (2.1%) | 10 (5.8%) | |
| PALB2 | 1 (0.8%) | 0 (0.0%) | 1 (0.6%) | |
| No identified mutation | 97 (77.6%) | 39 (81.3%) | 136 (78.6%) | |
| HER2-0 | HER2-Low | Total | ||||
|---|---|---|---|---|---|---|
| (n = 316) | (n = 121) | (n = 449) | ||||
| pCR (i.e., ypT0 ypN0) | p = 0.192 | |||||
| No | 181 (57.3%) | 78 (64.5%) | 259 (59.3%) | |||
| Yes | 135 (42.7%) | 43 (35.5%) | 178 (40.7%) | |||
| Univariate | Multivariate (n = 432) | |||||
| OR | IC 95% | p-value | OR | IC 95% | p-value | |
| HER2 | ||||||
| HER2 0 | 1.00 | 1.00 | ||||
| HER 1+ or 2+ | 0.74 | [0.48;1.14] | 0.172 | 0.66 | [0.42; 1.03] | 0.066 |
| Stade N | ||||||
| N0 | 1.00 | 1.00 | ||||
| N+ | 1.01 | [0.68; 1.49] | 0.965 | 1.08 | [0.42; 1.03] | 0.700 |
| Stade T | ||||||
| T0-T1 | 1.00 | 1.00 | ||||
| T2 | 0.61 | [0.28; 1.31] | 0.201 | 0.60 | [0.27; 1.32] | 0.207 |
| T3-T4 | 0.37 | [0.17; 0.81] | 0.014 | 0.35 | [0.16; 0.80] | 0.012 |
| mSBR grade (biopsy) | ||||||
| Grade II | 1.00 | 1.00 | ||||
| Grade III | 1.08 | [0.69; 1.70] | 0.729 | 1.07 | [0.72; 1.78] | 0.773 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domergue, C.; Martin, E.; Lemarié, C.; Jézéquel, P.; Frenel, J.-S.; Augereau, P.; Campone, M.; Patsouris, A. Impact of HER2 Status on Pathological Response after Neoadjuvant Chemotherapy in Early Triple-Negative Breast Cancer. Cancers 2022, 14, 2509. https://doi.org/10.3390/cancers14102509
Domergue C, Martin E, Lemarié C, Jézéquel P, Frenel J-S, Augereau P, Campone M, Patsouris A. Impact of HER2 Status on Pathological Response after Neoadjuvant Chemotherapy in Early Triple-Negative Breast Cancer. Cancers. 2022; 14(10):2509. https://doi.org/10.3390/cancers14102509
Chicago/Turabian StyleDomergue, Camille, Elodie Martin, Camille Lemarié, Pascal Jézéquel, Jean-Sebastien Frenel, Paule Augereau, Mario Campone, and Anne Patsouris. 2022. "Impact of HER2 Status on Pathological Response after Neoadjuvant Chemotherapy in Early Triple-Negative Breast Cancer" Cancers 14, no. 10: 2509. https://doi.org/10.3390/cancers14102509