
Clinical Outcome Assessment in Cancer Rehabilitation and the Central Role of Patient-Reported Outcomes

 , , , ,
, , , ,  , and
, and 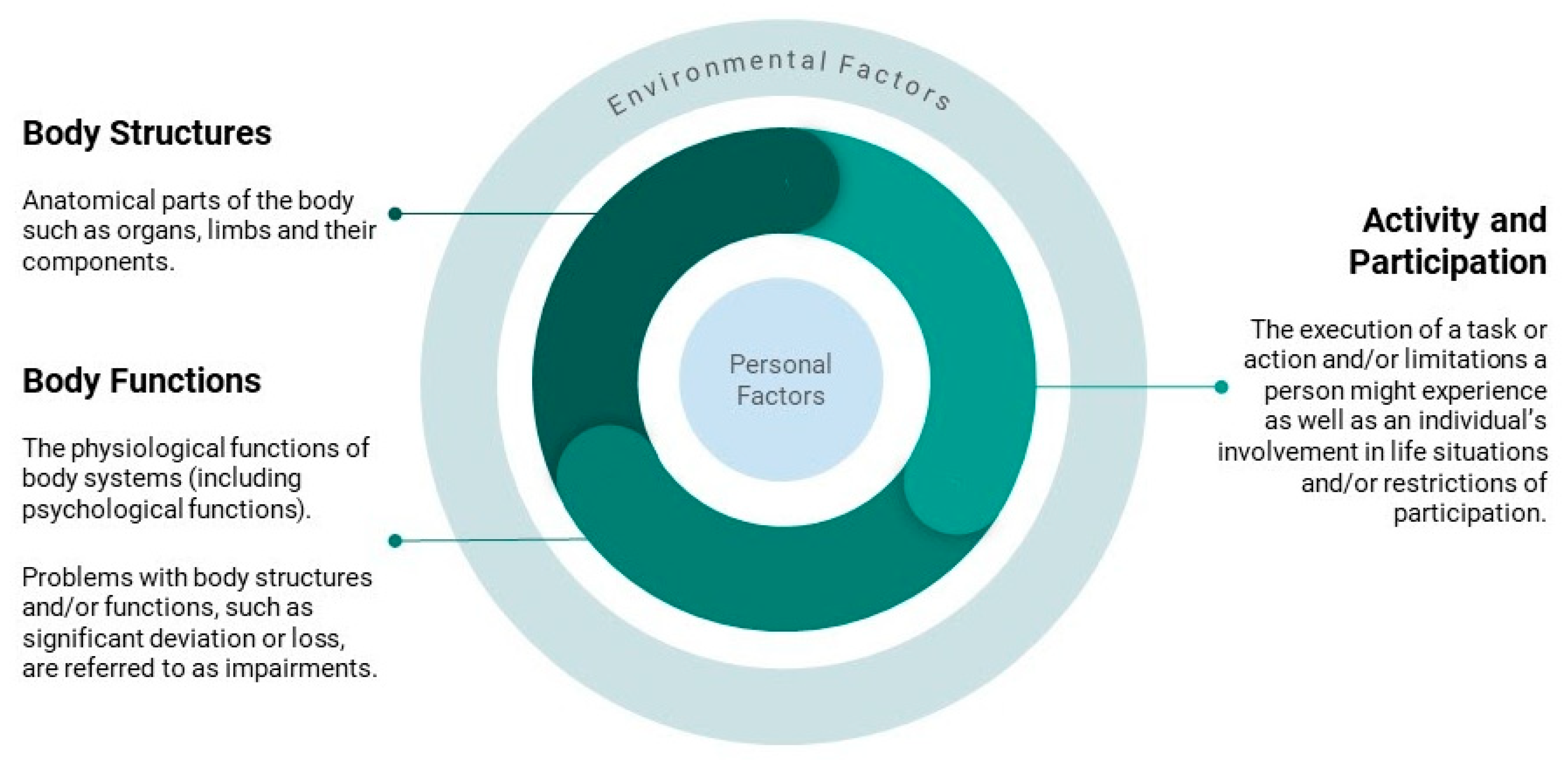{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Outcome Assessments in Cancer Rehabilitation
2.1. Functioning, Disability, Health, and Quality of Life as Outcomes of Interest
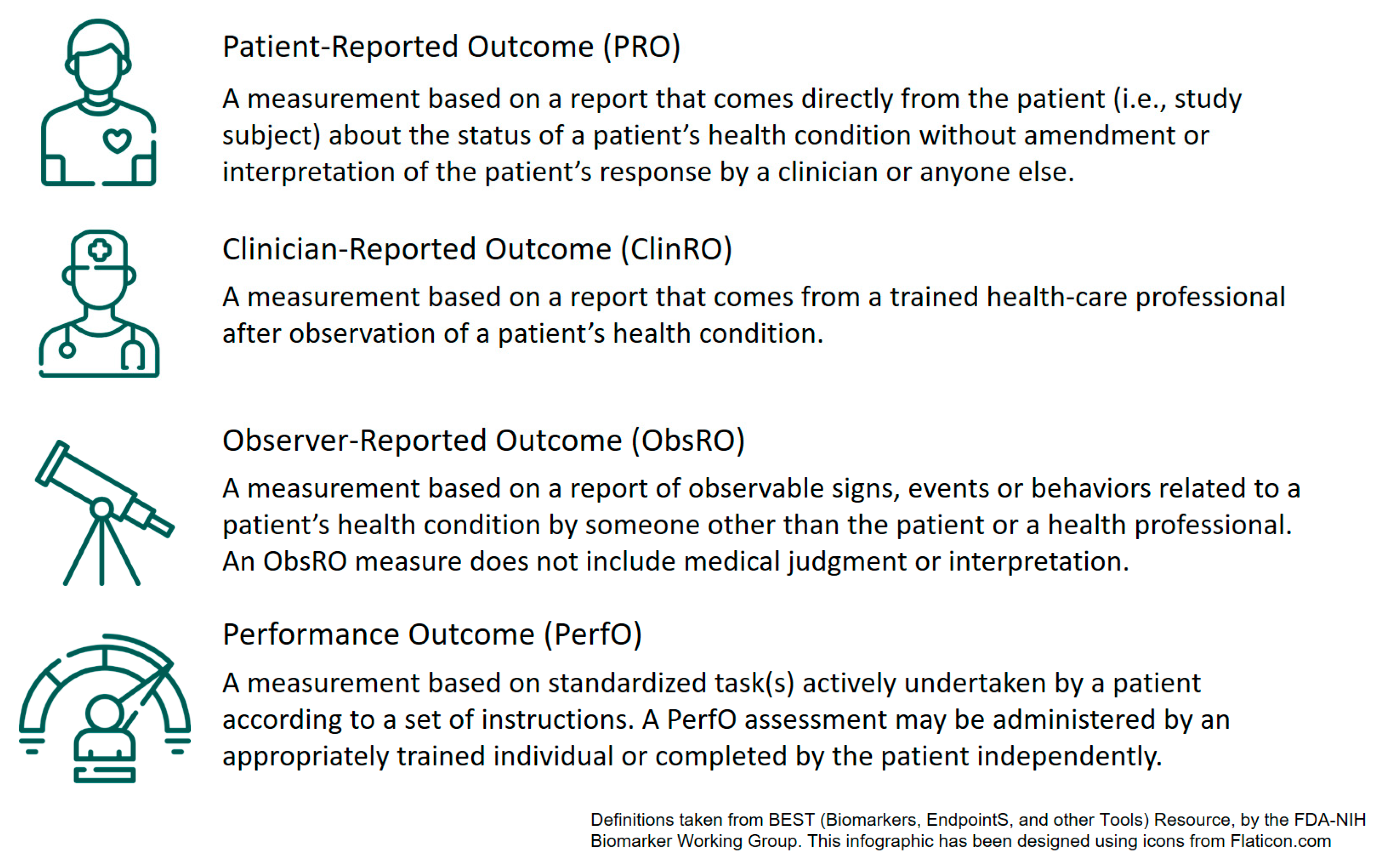
2.2. Different Types of Clinical Outcome Assessments (COAs)
3. PROMs for Cancer Rehabilitation
4. PROM Usage in Cancer Rehabilitation Research
5. Moving to PROs to Benchmark Value-Based Care
6. Standardized Outcome Sets and Recommendations for PROM Selection
7. Integration of (Electronic) PROs into the Rehabilitation Setting
7.1. Barriers to Successful Implementation
7.2. Integrating ePROs into the Rehabilitation Pathway
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer Treatment and Survivorship Statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Arnold, M.; Rutherford, M.J.; Bardot, A.; Ferlay, J.; Andersson, T.M.-L.; Myklebust, T.Å.; Tervonen, H.; Thursfield, V.; Ransom, D.; Shack, L.; et al. Progress in Cancer Survival, Mortality, and Incidence in Seven High-Income Countries 1995-2014 (ICBP SURVMARK-2): A Population-Based Study. Lancet Oncol. 2019, 20, 1493–1505. [Google Scholar] [CrossRef] [Green Version]
- Truant, T.L.; Fitch, M.I.; O’Leary, C.; Stewart, J. Global Perspectives on Cancer Survivorship: From Lost in Transition to Leading into the Future. Can. Oncol. Nurs. J. 2017, 27, 287–294. [Google Scholar]
- Götze, H.; Taubenheim, S.; Dietz, A.; Lordick, F.; Mehnert, A. Comorbid Conditions and Health-Related Quality of Life in Long-Term Cancer Survivors-Associations with Demographic and Medical Characteristics. J. Cancer Surviv. 2018, 12, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Stein, K.D.; Syrjala, K.L.; Andrykowski, M.A. Physical and Psychological Long-Term and Late Effects of Cancer. Cancer 2008, 112, 2577–2592. [Google Scholar] [CrossRef]
- Macmillan Cancer Support. Two Million Reasons: The Cancer Survivorship Agenda; Macmillan Cancer Support: London, UK, 2008. [Google Scholar]
- World Health Organization. Rehabilitation Competency Framework; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Stout, N.L.; Mina, D.S.; Lyons, K.D.; Robb, K.; Silver, J.K. A Systematic Review of Rehabilitation and Exercise Recommendations in Oncology Guidelines. CA A Cancer J. Clin. 2021, 71, 149–175. [Google Scholar] [CrossRef]
- Stout, N.L.; Silver, J.K.; Raj, V.S.; Rowland, J.; Gerber, L.; Cheville, A.; Ness, K.K.; Radomski, M.; Nitkin, R.; Stubblefield, M.D.; et al. Toward a National Initiative in Cancer Rehabilitation: Recommendations From a Subject Matter Expert Group. Arch. Phys. Med. Rehabil. 2016, 97, 2006–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Driscoll, J.J.; Rixe, O. Overall Survival: Still the Gold Standard: Why Overall Survival Remains the Definitive End Point in Cancer Clinical Trials. Cancer J. 2009, 15, 401–405. [Google Scholar] [CrossRef]
- Karimi, M.; Brazier, J. Health, Health-Related Quality of Life, and Quality of Life: What Is the Difference? PharmacoEconomics 2016, 34, 645–649. [Google Scholar] [CrossRef]
- Moons, P.; Budts, W.; De Geest, S. Critique on the Conceptualisation of Quality of Life: A Review and Evaluation of Different Conceptual Approaches. Int. J. Nurs. Stud. 2006, 43, 891–901. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability, and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- WHOQOL Group. The World Health Organization Quality of Life Assessment (WHOQOL): Position Paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and Response Criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Schag, C.C.; Heinrich, R.L.; Ganz, P.A. Karnofsky Performance Status Revisited: Reliability, Validity, and Guidelines. J. Clin. Oncol. 1984, 2, 187–193. [Google Scholar] [CrossRef]
- Parsons, S.K.; Fairclough, D.L.; Wang, J.; Hinds, P.S. Comparing Longitudinal Assessments of Quality of Life by Patient and Parent in Newly Diagnosed Children with Cancer: The Value of Both Raters’ Perspectives. Qual. Life Res. 2012, 21, 915–923. [Google Scholar] [CrossRef]
- Eiser, C.; Morse, R. Can Parents Rate Their Child’s Health-Related Quality of Life? Results of a Systematic Review. Qual. Life Res. 2001, 10, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Kilgour, R.D.; Vigano, A.; Trutschnigg, B.; Lucar, E.; Borod, M.; Morais, J.A. Handgrip Strength Predicts Survival and Is Associated with Markers of Clinical and Functional Outcomes in Advanced Cancer Patients. Support Care Cancer 2013, 21, 3261–3270. [Google Scholar] [CrossRef] [PubMed]
- Jansen, C.E.; Miaskowski, C.A.; Dodd, M.J.; Dowling, G.A. A Meta-Analysis of the Sensitivity of Various Neuropsychological Tests Used to Detect Chemotherapy-Induced Cognitive Impairment in Patients with Breast Cancer. Oncol. Nurs. Forum. 2007, 34, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Jette, A.M.; Haley, S.M. Contemporary Measurement Techniques for Rehabilitation Outcomes Assessment. J. Rehabil. Med. 2005, 37, 339–345. [Google Scholar] [CrossRef] [Green Version]
- Meyers, C.A.; Hess, K.R.; Yung, W.K.; Levin, V.A. Cognitive Function as a Predictor of Survival in Patients with Recurrent Malignant Glioma. J. Clin. Oncol. 2000, 18, 646–650. [Google Scholar] [CrossRef]
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and Other Tools) Resource; Food and Drug Administration (US): Silver Spring, MD, USA, 2016.
- U.S. Food and Drug Administration Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/patient-reported-outcome-measures-use-medical-product-development-support-labeling-claims (accessed on 5 August 2020).
- European Medicines Agency. Appendix 2 to the Guideline on the Evaluation of Anticancer Medicinal Products in Man: The Use of Patient-Reported Outcome (PRO) Measures in Oncology Studies; European Medicines Agency: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Basch, E.; Iasonos, A.; McDonough, T.; Barz, A.; Culkin, A.; Kris, M.G.; Scher, H.I.; Schrag, D. Patient versus Clinician Symptom Reporting Using the National Cancer Institute Common Terminology Criteria for Adverse Events: Results of a Questionnaire-Based Study. Lancet Oncol. 2006, 7, 903–909. [Google Scholar] [CrossRef]
- Atkinson, T.M.; Rogak, L.J.; Heon, N.; Ryan, S.J.; Shaw, M.; Stark, L.P.; Bennett, A.V.; Basch, E.; Li, Y. Exploring Differences in Adverse Symptom Event Grading Thresholds between Clinicians and Patients in the Clinical Trial Setting. J. Cancer Res. Clin. Oncol. 2017, 143, 735–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkinson, T.M.; Andreotti, C.F.; Roberts, K.E.; Saracino, R.M.; Hernandez, M.; Basch, E. The Level of Association between Functional Performance Status Measures and Patient-Reported Outcomes in Cancer Patients: A Systematic Review. Support Care Cancer 2015, 23, 3645–3652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratford, P.W.; Kennedy, D.; Pagura, S.M.C.; Gollish, J.D. The Relationship between Self-Report and Performance-Related Measures: Questioning the Content Validity of Timed Tests. Arthritis Rheum. 2003, 49, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, S.; Dijkstra, P.; Stewart, R.; Göeken, L.; Groothoff, J.; Geertzen, J. Comparing Self-Report, Clinical Examination and Functional Testing in the Assessment of Work-Related Limitations in Patients with Chronic Low Back Pain. Disabil. Rehabil. 2005, 27, 999–1005. [Google Scholar] [CrossRef]
- de Boer, A.G.E.M.; Taskila, T.; Ojajärvi, A.; van Dijk, F.J.H.; Verbeek, J.H.A.M. Cancer Survivors and Unemployment: A Meta-Analysis and Meta-Regression. JAMA 2009, 301, 753–762. [Google Scholar] [CrossRef]
- Isernhagen, S.J.; Hart, D.L.; Matheson, L.M. Reliability of Independent Observer Judgments of Level of Lift Effort in a Kinesiophysical Functional Capacity Evaluation. Work 1999, 12, 145–150. [Google Scholar]
- Frank, M.; Hallak, G.; Stahl, C.; Wölke, G.; Ekkernkamp, A. Evaluation der funktionellen Leistungsfähigkeit nach Isernhagen. Trauma Berufskrankh. 2011, 13, 18–22. [Google Scholar] [CrossRef]
- Weiss, D.J.; Dawis, R.V.; England, G.W. Manual for the Minnesota Satisfaction Questionnaire. Minn. Stud. Vocat. Rehabil. 1967, 22, 120. [Google Scholar]
- Smith, W.A.; Li, Z.; Loftin, M.; Carlyle, B.E.; Hudson, M.M.; Robison, L.L.; Ness, K.K. Measured versus Self-Reported Physical Function in Adult Survivors of Childhood Cancer. Med. Sci. Sports Exerc. 2014, 46, 211–218. [Google Scholar] [CrossRef] [Green Version]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Snaith, R.P. The Hospital Anxiety And Depression Scale. Health Qual. Life Outcomes 2003, 1, 29. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Gould, R.; Ilmarinen, J.; Järvisalo, J.; Koskinen, S. Dimensions of Work Ability: Results of the Health 2000 Survey; Innish Centre for Pensions (ETK), The Social Insurance Institution (Kela), National Public Health Institute (KTL), Finnish Institute of Occupational Health: Helsinki, Finland, 2008. [Google Scholar]
- Tuomi, K.; Ilmarinen, J.; Jahkola, A.; Katajarinne, L.; Tulkki, A. Work Ability Index; Finnish Institute of Occupational Health Helsinki: Helsinki, Finland, 1998; Volume 19. [Google Scholar]
- Kingsley, C.; Patel, S. Patient-Reported Outcome Measures and Patient-Reported Experience Measures. BJA Educ. 2017, 17, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Brédart, A.; Kop, J.-L.; Efficace, F.; Beaudeau, A.; Brito, T.; Dolbeault, S.; Aaronson, N. EORTC Quality of Life Group Quality of Care in the Oncology Outpatient Setting from Patients’ Perspective: A Systematic Review of Questionnaires’ Content and Psychometric Performance. Psychooncology 2015, 24, 382–394. [Google Scholar] [CrossRef]
- Brédart, A.; Anota, A.; Young, T.; Tomaszewski, K.A.; Arraras, J.I.; Moura De Albuquerque Melo, H.; Schmidt, H.; Friend, E.; Bergenmar, M.; Costantini, A.; et al. Phase III Study of the European Organisation for Research and Treatment of Cancer Satisfaction with Cancer Care Core Questionnaire (EORTC PATSAT-C33) and Specific Complementary Outpatient Module (EORTC OUT-PATSAT7). Eur. J. Cancer Care 2018, 27, e12786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulis, D.; Bottomley, A.; Whittaker, C.; van de Poll-Franse, L.; Darlington, A.; Holzner, B.; Koller, M.; Reijneveld, J.C.; Tomaszewski, K.; Grønvold, M. The Use of The Eortc Item Library To Supplement Eortc Quality of Life Instruments. Value Health 2017, 20, A775. [Google Scholar] [CrossRef]
- Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). Available online: https://healthcaredelivery.cancer.gov/pro-ctcae/ (accessed on 27 August 2021).
- PROMIS. Available online: https://www.healthmeasures.net/explore-measurement-systems/promis (accessed on 27 August 2021).
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and Preliminary Testing of the New Five-Level Version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pickard, A.S.; Wilke, C.T.; Lin, H.-W.; Lloyd, A. Health Utilities Using the EQ-5D in Studies of Cancer. Pharmacoeconomics 2007, 25, 365–384. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E. SF-36 Health Survey Update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.F.; Tulsky, D.S.; Gray, G.; Sarafian, B.; Linn, E.; Bonomi, A.; Silberman, M.; Yellen, S.B.; Winicour, P.; Brannon, J. The Functional Assessment of Cancer Therapy Scale: Development and Validation of the General Measure. J. Clin. Oncol. 1993, 11, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Coombes, L.; Bristowe, K.; Ellis-Smith, C.; Aworinde, J.; Fraser, L.K.; Downing, J.; Bluebond-Langner, M.; Chambers, L.; Murtagh, F.E.M.; Harding, R. Enhancing Validity, Reliability and Participation in Self-Reported Health Outcome Measurement for Children and Young People: A Systematic Review of Recall Period, Response Scale Format, and Administration Modality. Qual. Life Res. 2021, 30, 1803–1832. [Google Scholar] [CrossRef] [PubMed]
- Arbuckle, R.; Abetz-Webb, L. “Not Just Little Adults”: Qualitative Methods to Support the Development of Pediatric Patient-Reported Outcomes. Patient 2013, 6, 143–159. [Google Scholar] [CrossRef]
- Sodergren, S.C.; Husson, O.; Robinson, J.; Rohde, G.E.; Tomaszewska, I.M.; Vivat, B.; Dyar, R.; Darlington, A.-S. EORTC Quality of Life Group Systematic Review of the Health-Related Quality of Life Issues Facing Adolescents and Young Adults with Cancer. Qual. Life Res. 2017, 26, 1659–1672. [Google Scholar] [CrossRef] [Green Version]
- Sodergren, S.C.; Husson, O.; Rohde, G.E.; Tomaszewska, I.M.; Vivat, B.; Yarom, N.; Griffiths, H.; Darlington, A.-S. A Life Put on Pause: An Exploration of the Health-Related Quality of Life Issues Relevant to Adolescents and Young Adults with Cancer. J. Adolesc. Young Adult Oncol. 2018, 7, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Burwinkle, T.M.; Katz, E.R.; Meeske, K.; Dickinson, P. The PedsQL in Pediatric Cancer: Reliability and Validity of the Pediatric Quality of Life Inventory Generic Core Scales, Multidimensional Fatigue Scale, and Cancer Module. Cancer 2002, 94, 2090–2106. [Google Scholar] [CrossRef]
- Reeve, B.B.; McFatrich, M.; Mack, J.W.; Maurer, S.H.; Jacobs, S.S.; Freyer, D.R.; Withycombe, J.S.; Baker, J.N.; Castellino, S.M.; Lin, L.; et al. Validity and Reliability of the Pediatric Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events. J. Natl. Cancer Inst. 2020, 112, 1143–1152. [Google Scholar] [CrossRef] [PubMed]
- DeWalt, D.A.; Gross, H.E.; Gipson, D.S.; Selewski, D.T.; DeWitt, E.M.; Dampier, C.D.; Hinds, P.S.; Huang, I.-C.; Thissen, D.; Varni, J.W. PROMIS® Pediatric Self-Report Scales Distinguish Subgroups of Children within and across Six Common Pediatric Chronic Health Conditions. Qual. Life Res. 2015, 24, 2195–2208. [Google Scholar] [CrossRef] [Green Version]
- Husson, O.; Sodergren, S.C.; Darlington, A.-S. The Importance of a Collaborative Health-Related Quality of Life Measurement Strategy for Adolescents and Young Adults with Cancer. Cancer 2021, 127, 1712–1713. [Google Scholar] [CrossRef] [PubMed]
- Haley, S.M.; Andres, P.L.; Coster, W.J.; Kosinski, M.; Ni, P.; Jette, A.M. Short-Form Activity Measure for Post-Acute Care. Arch. Phys. Med. Rehabil. 2004, 85, 649–660. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.R.; Vargo, M.; Zucker, D.S.; Henderson, M.; Shahpar, S.; Wisotzky, E.M.; Custodio, C.; Basford, J.; Jay, G.; Gerber, L.; et al. The Cancer Rehabilitation Medicine Metrics Consortium: A Path to Enhanced, Multi-Site Outcome Assessment to Enhance Care and Demonstrate Value. Front. Oncol. 2020, 10, 625700. [Google Scholar] [CrossRef]
- Schag, C.A.; Heinrich, R.L. Development of a Comprehensive Quality of Life Measurement Tool: CARES. Oncology (Williston Park NY) 1990, 4, 135–138, discussion 147. [Google Scholar]
- Ganz, P.A.; Schag, C.A.; Lee, J.J.; Sim, M.S. The CARES: A Generic Measure of Health-Related Quality of Life for Patients with Cancer. Qual. Life Res. 1992, 1, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Ganz, P.A. Cancer Rehabilitation Evaluation System (CARES) and CARES-SF Now Publicly Available. J. Clin. Oncol. 2012, 30, 4046–4047. [Google Scholar] [CrossRef]
- Duijts, S.F.A.; Faber, M.M.; Oldenburg, H.S.A.; van Beurden, M.; Aaronson, N.K. Effectiveness of Behavioral Techniques and Physical Exercise on Psychosocial Functioning and Health-Related Quality of Life in Breast Cancer Patients and Survivors—A Meta-Analysis. Psychooncology 2011, 20, 115–126. [Google Scholar] [CrossRef]
- van Leeuwen, M.; Husson, O.; Alberti, P.; Arraras, J.I.; Chinot, O.L.; Costantini, A.; Darlington, A.-S.; Dirven, L.; Eichler, M.; Hammerlid, E.B.; et al. Understanding the Quality of Life (QOL) Issues in Survivors of Cancer: Towards the Development of an EORTC QOL Cancer Survivorship Questionnaire. Health Qual. Life Outcomes 2018, 16, 114. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Portier, K.; Stein, K.; Baker, F.; Smith, T. Exploratory Factor Analysis of the Cancer Problems in Living Scale: A Report from the American Cancer Society’s Studies of Cancer Survivors. J. Pain Symptom Manag. 2009, 37, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Zebrack, B.J.; Ganz, P.A.; Bernaards, C.A.; Petersen, L.; Abraham, L. Assessing the Impact of Cancer: Development of a New Instrument for Long-Term Survivors. Psychooncology 2006, 15, 407–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrell, B.R.; Dow, K.H.; Grant, M. Measurement of the Quality of Life in Cancer Survivors. Qual. Life Res. 1995, 4, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Avis, N.E.; Smith, K.W.; McGraw, S.; Smith, R.G.; Petronis, V.M.; Carver, C.S. Assessing Quality of Life in Adult Cancer Survivors (QLACS). Qual. Life Res. 2005, 14, 1007–1023. [Google Scholar] [CrossRef]
- Muzzatti, B.; Annunziata, M.A. Assessing Quality of Life in Long-Term Cancer Survivors: A Review of Available Tools. Support Care Cancer 2013, 21, 3143–3152. [Google Scholar] [CrossRef]
- Survivorship: EORTC–Quality of Life. Available online: https://qol.eortc.org/questionnaire/surv111/ (accessed on 30 September 2021).
- Gudbergsson, S.B.; Dahl, A.A.; Loge, J.H.; Thorsen, L.; Oldervoll, L.M.; Grov, E.K. What Is Covered by “Cancer Rehabilitation” in PubMed? A Review of Randomized Controlled Trials 1990-2011. J. Rehabil. Med. 2015, 47, 97–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mewes, J.C.; Steuten, L.M.G.; Ijzerman, M.J.; van Harten, W.H. Effectiveness of Multidimensional Cancer Survivor Rehabilitation and Cost-Effectiveness of Cancer Rehabilitation in General: A Systematic Review. Oncologist 2012, 17, 1581–1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, S.I.; Scherer, R.W.; Geigle, P.M.; Berlanstein, D.R.; Topaloglu, O.; Gotay, C.C.; Snyder, C. Exercise Interventions on Health-related Quality of Life for Cancer Survivors. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Licht, T.; Nickels, A.; Rumpold, G.; Holzner, B.; Riedl, D. Evaluation by Electronic Patient-Reported Outcomes of Cancer Survivors’ Needs and the Efficacy of Inpatient Cancer Rehabilitation in Different Tumor Entities. Support Care Cancer 2021, 29, 5853–5864. [Google Scholar] [CrossRef]
- Riedl, D.; Giesinger, J.M.; Wintner, L.M.; Loth, F.L.; Rumpold, G.; Greil, R.; Nickels, A.; Licht, T.; Holzner, B. Improvement of Quality of Life and Psychological Distress after Inpatient Cancer Rehabilitation: Results of a Longitudinal Observational Study. Wien. Klin. Wochenschr. 2017, 129, 692–701. [Google Scholar] [CrossRef]
- Nottelmann, L.; Groenvold, M.; Vejlgaard, T.B.; Petersen, M.A.; Jensen, L.H. Early, Integrated Palliative Rehabilitation Improves Quality of Life of Patients with Newly Diagnosed Advanced Cancer: The Pal-Rehab Randomized Controlled Trial. Palliat. Med. 2021, 35, 1344–1355. [Google Scholar] [CrossRef]
- Leclerc, A.-F.; Foidart-Dessalle, M.; Tomasella, M.; Coucke, P.; Devos, M.; Bruyère, O.; Bury, T.; Deflandre, D.; Jerusalem, G.; Lifrange, E.; et al. Multidisciplinary Rehabilitation Program after Breast Cancer: Benefits on Physical Function, Anthropometry and Quality of Life. Eur. J. Phys. Rehabil. Med. 2017, 53, 633–642. [Google Scholar] [CrossRef]
- Keeney, T.; Kumar, A.; Erler, K.S.; Karmarkar, A.M. Making the Case for Patient-Reported Outcome Measures in Big-Data Rehabilitation Research: Implications for Optimizing Patient-Centered Care. Arch. Phys. Med. Rehabil. 2021. [Google Scholar] [CrossRef]
- Porter, M.E. What Is Value in Health Care? N. Engl. J. Med. 2010, 363, 2477–2481. [Google Scholar] [CrossRef]
- Anatchkova, M.; Donelson, S.M.; Skalicky, A.M.; McHorney, C.A.; Jagun, D.; Whiteley, J. Exploring the Implementation of Patient-Reported Outcome Measures in Cancer Care: Need for More Real-World Evidence Results in the Peer Reviewed Literature. J. Patient Rep. Outcomes 2018, 2, 64. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Wilfong, L.; Schrag, D. Adding Patient-Reported Outcomes to Medicare’s Oncology Value-Based Payment Model. JAMA 2020, 323, 213–214. [Google Scholar] [CrossRef] [PubMed]
- Nübling, R.; Kaluscha, R.; Krischak, G.; Kriz, D.; Martin, H.; Müller, G.; Renzland, J.; Reuss-Borst, M.; Schmidt, J.; Kaiser, U.; et al. Ergebnisqualität medizinischer Rehabilitation: Zum Zusammenhang zwischen „Patient Reported Outcomes“ (PROs) und geleisteten Sozialversicherungsbeiträgen. Die Rehabilitation 2017, 56, 22–30. [Google Scholar] [CrossRef]
- Stamm, T.; Bott, N.; Thwaites, R.; Mosor, E.; Andrews, M.; Borgdorff, J.; Cossio-Gil, Y.; de Portu, S.; Ferrante, M.; Fischer, F.; et al. Building a Value-Based Care Infrastructure in Europe: The Health Outcomes Observatory. NEJM Catal. Innov. Care Deliv. 2021, 2. Available online: https://catalyst.nejm.org/doi/full/10.1056/CAT.21.0146 (accessed on 1 November 2021).
- Grote, V.; Unger, A.; Böttcher, E.; Muntean, M.; Puff, H.; Marktl, W.; Mur, E.; Kullich, W.; Holasek, S.; Hofmann, P.; et al. General and Disease-Specific Health Indicator Changes Associated with Inpatient Rehabilitation. J. Am. Med. Dir. Assoc. 2020, 21, 2017.e10–2017.e27. [Google Scholar] [CrossRef]
- Zdravkovic, A.; Grote, V.; Pirchl, M.; Stockinger, M.; Crevenna, R.; Fischer, M.J. Comparison of Patient- and Clinician-Reported Outcome Measures in Lower Back Rehabilitation: Introducing a New Integrated Performance Measure (T2D). Qual. Life Res. 2021. [Google Scholar] [CrossRef]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes; Oxford University Press: Oxford, UK, 2015; ISBN 0-19-164358-0. [Google Scholar]
- Norman, R.; Viney, R.; Aaronson, N.K.; Brazier, J.E.; Cella, D.; Costa, D.S.J.; Fayers, P.M.; Kemmler, G.; Peacock, S.; Pickard, A.S.; et al. Using a Discrete Choice Experiment to Value the QLU-C10D: Feasibility and Sensitivity to Presentation Format. Qual. Life Res. 2016, 25, 637–649. [Google Scholar] [CrossRef]
- King, M.T.; Costa, D.S.J.; Aaronson, N.K.; Brazier, J.E.; Cella, D.F.; Fayers, P.M.; Grimison, P.; Janda, M.; Kemmler, G.; Norman, R.; et al. QLU-C10D: A Health State Classification System for a Multi-Attribute Utility Measure Based on the EORTC QLQ-C30. Qual. Life Res. 2016, 25, 625–636. [Google Scholar] [CrossRef]
- Gamper, E.M.; King, M.T.; Norman, R.; Efficace, F.; Cottone, F.; Holzner, B.; Kemmler, G. European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Group EORTC QLU-C10D Value Sets for Austria, Italy, and Poland. Qual. Life Res. 2020, 29, 2485–2495. [Google Scholar] [CrossRef]
- Deutsche Rentenversicherung Bund. Deutsche Rentenversicherung Reha Bericht 2018: Die Medizinische Und Berufliche Rehabilitation Der Rentenversicherung Im Licht Der Statistik; Deutsche Rentenversicherung Bund: Berlin, Germany, 2018. [Google Scholar]
- Sibert, N.T.; Pfaff, H.; Breidenbach, C.; Wesselmann, S.; Kowalski, C. Different Approaches for Case-Mix Adjustment of Patient-Reported Outcomes to Compare Healthcare Providers-Methodological Results of a Systematic Review. Cancers 2021, 13, 3964. [Google Scholar] [CrossRef] [PubMed]
- Squitieri, L.; Bozic, K.J.; Pusic, A.L. The Role of Patient-Reported Outcome Measures in Value-Based Payment Reform. Value Health 2017, 20, 834–836. [Google Scholar] [CrossRef] [Green Version]
- Young, G.; Schleicher, S.M.; Dickson, N.R.; Lyss, A.J. Insights From the Oncology Care First Proposal—Where We’ve Been and Where We’re Going in Value-Based Care. JCO Oncol. Pract. 2020, 16, 151–153. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C.W. The COSMIN Study Reached International Consensus on Taxonomy, Terminology, and Definitions of Measurement Properties for Health-Related Patient-Reported Outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz Rivera, S.; Mercieca-Bebber, R.; Aiyegbusi, O.L.; Scott, J.; Hunn, A.; Fernandez, C.; Ives, J.; Ells, C.; Price, G.; Draper, H.; et al. The Need for Ethical Guidance for the Use of Patient-Reported Outcomes in Research and Clinical Practice. Nat. Med. 2021, 27, 572–573. [Google Scholar] [CrossRef]
- Ramsey, I.; de Rooij, B.H.; Mols, F.; Corsini, N.; Horevoorts, N.J.E.; Eckert, M.; van de Poll-Franse, L.V. Cancer Survivors Who Fully Participate in the PROFILES Registry Have Better Health-Related Quality of Life than Those Who Drop Out. J. Cancer Surviv. 2019, 13, 829–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsey, I.; Eckert, M.; Hutchinson, A.D.; Marker, J.; Corsini, N. Core Outcome Sets in Cancer and Their Approaches to Identifying and Selecting Patient-Reported Outcome Measures: A Systematic Review. J. Patient-Rep. Outcomes 2020, 4, 77. [Google Scholar] [CrossRef]
- Prinsen, C.A.C.; Vohra, S.; Rose, M.R.; Boers, M.; Tugwell, P.; Clarke, M.; Williamson, P.R.; Terwee, C.B. How to Select Outcome Measurement Instruments for Outcomes Included in a “Core Outcome Set”—A Practical Guideline. Trials 2016, 17, 449. [Google Scholar] [CrossRef] [Green Version]
- Letellier, M.-E.; Dawes, D.; Mayo, N. Content Verification of the EORTC QLQ-C30/EORTC QLQ-BR23 with the International Classification of Functioning, Disability and Health. Qual. Life Res. 2015, 24, 757–768. [Google Scholar] [CrossRef]
- Cieza, A.; Fayed, N.; Bickenbach, J.; Prodinger, B. Refinements of the ICF Linking Rules to Strengthen Their Potential for Establishing Comparability of Health Information. Disabil. Rehabil. 2019, 41, 574–583. [Google Scholar] [CrossRef]
- Gilchrist, L.S.; Galantino, M.L.; Wampler, M.; Marchese, V.G.; Morris, G.S.; Ness, K.K. A Framework for Assessment in Oncology Rehabilitation. Phys. Ther. 2009, 89, 286–306. [Google Scholar] [CrossRef] [Green Version]
- Mak, K.S.; van Bommel, A.C.M.; Stowell, C.; Abrahm, J.L.; Baker, M.; Baldotto, C.S.; Baldwin, D.R.; Borthwick, D.; Carbone, D.P.; Chen, A.B.; et al. Defining a Standard Set of Patient-Centred Outcomes for Lung Cancer. Eur. Respir. J. 2016, 48, 852–860. [Google Scholar] [CrossRef]
- Martin, N.E.; Massey, L.; Stowell, C.; Bangma, C.; Briganti, A.; Bill-Axelson, A.; Blute, M.; Catto, J.; Chen, R.C.; D’Amico, A.V.; et al. Defining a Standard Set of Patient-Centered Outcomes for Men with Localized Prostate Cancer. Eur. Urol. 2015, 67, 460–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgans, A.K.; van Bommel, A.C.M.; Stowell, C.; Abrahm, J.L.; Basch, E.; Bekelman, J.E.; Berry, D.L.; Bossi, A.; Davis, I.D.; de Reijke, T.M.; et al. Development of a Standardized Set of Patient-Centered Outcomes for Advanced Prostate Cancer: An International Effort for a Unified Approach. Eur. Urol. 2015, 68, 891–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, W.L.; Schouwenburg, M.G.; van Bommel, A.C.M.; Stowell, C.; Allison, K.H.; Benn, K.E.; Browne, J.P.; Cooter, R.D.; Delaney, G.P.; Duhoux, F.P.; et al. A Standard Set of Value-Based Patient-Centered Outcomes for Breast Cancer: The International Consortium for Health Outcomes Measurement (ICHOM) Initiative. JAMA Oncol. 2017, 3, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Zerillo, J.A.; Schouwenburg, M.G.; van Bommel, A.C.M.; Stowell, C.; Lippa, J.; Bauer, D.; Berger, A.M.; Boland, G.; Borras, J.M.; Buss, M.K.; et al. An International Collaborative Standardizing a Comprehensive Patient-Centered Outcomes Measurement Set for Colorectal Cancer. JAMA Oncol. 2017, 3, 686–694. [Google Scholar] [CrossRef]
- Giesinger, J.M.; Efficace, F.; Aaronson, N.; Calvert, M.; Kyte, D.; Cottone, F.; Cella, D.; Gamper, E.-M. Past and Current Practice of Patient-Reported Outcome Measurement in Randomized Cancer Clinical Trials: A Systematic Review. Value Health 2021, 24, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Nolte, S.; Liegl, G.; Petersen, M.A.; Aaronson, N.K.; Costantini, A.; Fayers, P.M.; Groenvold, M.; Holzner, B.; Johnson, C.D.; Kemmler, G.; et al. General Population Normative Data for the EORTC QLQ-C30 Health-Related Quality of Life Questionnaire Based on 15,386 Persons across 13 European Countries, Canada and the Unites States. Eur. J. Cancer 2019, 107, 153–163. [Google Scholar] [CrossRef]
- Nolte, S.; Waldmann, A.; Liegl, G.; Petersen, M.A.; Groenvold, M.; Rose, M. EORTC Quality of Life Group Updated EORTC QLQ-C30 General Population Norm Data for Germany. Eur. J. Cancer 2020, 137, 161–170. [Google Scholar] [CrossRef]
- Lehmann, J.; Giesinger, J.M.; Nolte, S.; Sztankay, M.; Wintner, L.M.; Liegl, G.; Rose, M.; Holzner, B. EORTC Quality of Life Group Normative Data for the EORTC QLQ-C30 from the Austrian General Population. Health Qual. Life Outcomes 2020, 18, 275. [Google Scholar] [CrossRef]
- Basch, E.; Deal, A.M.; Dueck, A.C.; Scher, H.I.; Kris, M.G.; Hudis, C.; Schrag, D. Overall Survival Results of a Trial Assessing Patient-Reported Outcomes for Symptom Monitoring During Routine Cancer Treatment. JAMA 2017, 318, 197–198. [Google Scholar] [CrossRef] [Green Version]
- Barbera, L.; Sutradhar, R.; Seow, H.; Mittmann, N.; Howell, D.; Earle, C.C.; Li, Q.; Thiruchelvam, D. The Impact of Routine Edmonton Symptom Assessment System (ESAS) Use on Overall Survival in Cancer Patients: Results of a Population-Based Retrospective Matched Cohort Analysis. Cancer Med. 2020, 9, 7107–7115. [Google Scholar] [CrossRef] [PubMed]
- Barbera, L.; Sutradhar, R.; Seow, H.; Earle, C.C.; Howell, D.; Mittmann, N.; Li, Q.; Thiruchelvam, D. Impact of Standardized Edmonton Symptom Assessment System Use on Emergency Department Visits and Hospitalization: Results of a Population-Based Retrospective Matched Cohort Analysis. JCO Oncol. Pract. 2020, 16, e958–e965. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Abernethy, A.P. Supporting Clinical Practice Decisions With Real-Time Patient-Reported Outcomes. J. Clin. Oncol. 2011, 29, 954–956. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, E.E.; Keding, A.; Awad, N.; Hofmann, U.; Campbell, L.J.; Selby, P.J.; Brown, J.M.; Velikova, G. Impact of Patient-Reported Outcomes in Oncology: A Longitudinal Analysis of Patient-Physician Communication. J. Clin. Oncol. 2011, 29, 2910–2917. [Google Scholar] [CrossRef]
- Velikova, G.; Booth, L.; Smith, A.B.; Brown, P.M.; Lynch, P.; Brown, J.M.; Selby, P.J. Measuring Quality of Life in Routine Oncology Practice Improves Communication and Patient Well-Being: A Randomized Controlled Trial. J. Clin. Oncol. 2004, 22, 714–724. [Google Scholar] [CrossRef]
- Absolom, K.; Warrington, L.; Hudson, E.; Hewison, J.; Morris, C.; Holch, P.; Carter, R.; Gibson, A.; Holmes, M.; Clayton, B.; et al. Phase III Randomized Controlled Trial of ERAPID: EHealth Intervention During Chemotherapy. J. Clin. Oncol. 2021, 39, 734–747. [Google Scholar] [CrossRef] [PubMed]
- Velikova, G.; Keding, A.; Harley, C.; Cocks, K.; Booth, L.; Smith, A.B.; Wright, P.; Selby, P.J.; Brown, J.M. Patients Report Improvements in Continuity of Care When Quality of Life Assessments Are Used Routinely in Oncology Practice: Secondary Outcomes of a Randomised Controlled Trial. Eur. J. Cancer 2010, 46, 2381–2388. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Ou, L.; Hollis, S.J. A Systematic Review of the Impact of Routine Collection of Patient Reported Outcome Measures on Patients, Providers and Health Organisations in an Oncologic Setting. BMC Health Serv. Res. 2013, 13, 211. [Google Scholar] [CrossRef] [Green Version]
- Nama, V.; Nordin, A.; Bryant, A. Patient-reported Outcome Measures for Follow-up after Gynaecological Cancer Treatment. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Schick-Makaroff, K.; Molzahn, A. Strategies to Use Tablet Computers for Collection of Electronic Patient-Reported Outcomes. Health Qual. Life Outcomes 2015, 13, 2. [Google Scholar] [CrossRef] [Green Version]
- Gwaltney, C.J.; Shields, A.L.; Shiffman, S. Equivalence of Electronic and Paper-and-Pencil Administration of Patient-Reported Outcome Measures: A Meta-Analytic Review. Value Health 2008, 11, 322–333. [Google Scholar] [CrossRef] [Green Version]
- Jensen, R.E.; Snyder, C.F.; Abernethy, A.P.; Basch, E.; Potosky, A.L.; Roberts, A.C.; Loeffler, D.R.; Reeve, B.B. Review of Electronic Patient-Reported Outcomes Systems Used in Cancer Clinical Care. J. Oncol. Pr. 2014, 10, e215–e222. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, L.K.; King, M.; Möller, S.; Jarden, M.; Andersen, C.L.; Frederiksen, H.; Gregersen, H.; Klostergaard, A.; Steffensen, M.S.; Pedersen, P.T.; et al. Strategies to Improve Patient-Reported Outcome Completion Rates in Longitudinal Studies. Qual. Life Res. 2020, 29, 335–346. [Google Scholar] [CrossRef] [Green Version]
- Triplet, J.J.; Momoh, E.; Kurowicki, J.; Villarroel, L.D.; Law, T. yee Law, T.; Levy, J.C. E-Mail Reminders Improve Completion Rates of Patient-Reported Outcome Measures. JSES OA 2017, 1, 25–28. [Google Scholar] [CrossRef] [Green Version]
- Warrington, L.; Absolom, K.; Conner, M.; Kellar, I.; Clayton, B.; Ayres, M.; Velikova, G. Electronic Systems for Patients to Report and Manage Side Effects of Cancer Treatment: Systematic Review. J. Med. Internet Res. 2019, 21, e10875. [Google Scholar] [CrossRef] [Green Version]
- Stover, A.M.; Haverman, L.; van Oers, H.A.; Greenhalgh, J.; Potter, C.M.; Ahmed, S.; Greenhalgh, J.; Gibbons, E.; Haverman, L.; Manalili, K.; et al. Using an Implementation Science Approach to Implement and Evaluate Patient-Reported Outcome Measures (PROM) Initiatives in Routine Care Settings. Qual. Life Res. 2021, 30, 3015–3033. [Google Scholar] [CrossRef]
- Wintner, L.M.; Sztankay, M.; Riedl, D.; Rumpold, G.; Nickels, A.; Licht, T.; Holzner, B. How to Implement Routine Electronic Patient-Reported Outcome Monitoring in Oncology Rehabilitation. Int. J. Clin. Pr. 2021, 75, e13694. [Google Scholar] [CrossRef]
- Wintner, L.M.; Sztankay, M.; Aaronson, N.; Bottomley, A.; Giesinger, J.M.; Groenvold, M.; Petersen, M.A.; van de Poll-Franse, L.; Velikova, G.; Verdonck-de Leeuw, I.; et al. The Use of EORTC Measures in Daily Clinical Practice-A Synopsis of a Newly Developed Manual. Eur. J. Cancer 2016, 68, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinemann, A.W.; Nitsch, K.P.; Gracz, K.; Ehrlich-Jones, L.; Engel, E.; Wilson, M.; Zale, C.; Graham, I.D. Implementing Patient-Reported Outcome Measures in Inpatient Rehabilitation: Challenges and Solutions. Arch. Phys. Med. Rehabil. 2021, S0003-9993(21)00441-X. [Google Scholar] [CrossRef] [PubMed]
- Riedl, D.; Rumpold, G.; Nickels, A.; Licht, T.; Holzner, B. Einsetzbarkeit Eines Computergestützten Home-Monitorings Zur Evaluierung Der Langzeitwirksamkeit Stationärer Onkologischer Rehabilitation. In Proceedings of the 27. Rehabilitationswissenschaftliches Kolloquium der Deutsche Gesellschaft für Rehabilitationswissenschaften (DGRW), München, Germany, 26 February 2018; p. 132. [Google Scholar]
- Hoogland, A.I.; Mansfield, J.; Lafranchise, E.A.; Bulls, H.W.; Johnstone, P.A.; Jim, H.S.L. EHealth Literacy in Older Adults with Cancer. J. Geriatr. Oncol. 2020, 11, 1020–1022. [Google Scholar] [CrossRef] [PubMed]
- Snyder, C.F.; Aaronson, N.K.; Choucair, A.K.; Elliott, T.E.; Greenhalgh, J.; Halyard, M.Y.; Hess, R.; Miller, D.M.; Reeve, B.B.; Santana, M. Implementing Patient-Reported Outcomes Assessment in Clinical Practice: A Review of the Options and Considerations. Qual. Life Res. 2012, 21, 1305–1314. [Google Scholar] [CrossRef]
- Holzner, B.; Giesinger, J.M.; Pinggera, J.; Zugal, S.; Schöpf, F.; Oberguggenberger, A.S.; Gamper, E.M.; Zabernigg, A.; Weber, B.; Rumpold, G. The Computer-Based Health Evaluation Software (CHES): A Software for Electronic Patient-Reported Outcome Monitoring. BMC Med. Inf. Decis. Mak. 2012, 12, 126. [Google Scholar] [CrossRef] [Green Version]
- Macnair, A.; Sharkey, A.; Le Calvez, K.; Walters, R.; Smith, L.; Nelson, A.; Staffurth, J.; Williams, M.; Bloomfield, D.; Maher, J. The Trigger Project: The Challenge of Introducing Electronic Patient-Reported Outcome Measures Into a Radiotherapy Service. Clin. Oncol. 2020, 32, e76–e79. [Google Scholar] [CrossRef] [Green Version]
- Foster, A.; Croot, L.; Brazier, J.; Harris, J.; O’Cathain, A. The Facilitators and Barriers to Implementing Patient Reported Outcome Measures in Organisations Delivering Health Related Services: A Systematic Review of Reviews. J. Patient Rep. Outcomes 2018, 2, 46. [Google Scholar] [CrossRef]
- van Egdom, L.S.E.; Oemrawsingh, A.; Verweij, L.M.; Lingsma, H.F.; Koppert, L.B.; Verhoef, C.; Klazinga, N.S.; Hazelzet, J.A. Implementing Patient-Reported Outcome Measures in Clinical Breast Cancer Care: A Systematic Review. Value Health 2019, 22, 1197–1226. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Traina, S.; Li, T.; Johnson, K.; Ho, K.F.; Molina, A.; Shore, N.D. Relationship between Patient-Reported Outcomes and Clinical Outcomes in Metastatic Castration-Resistant Prostate Cancer: Post Hoc Analysis of COU-AA-301 and COU-AA-302. Ann. Oncol. 2018, 29, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Kane, H.L.; Halpern, M.T.; Squiers, L.B.; Treiman, K.A.; McCormack, L.A. Implementing and Evaluating Shared Decision Making in Oncology Practice. CA Cancer J. Clin. 2014, 64, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.; Ju, A.; King, M.T.; Rutherford, C. Perceived Benefits and Limitations of Using Patient-Reported Outcome Measures in Clinical Practice with Individual Patients: A Systematic Review of Qualitative Studies. Qual. Life Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Nelson, E.C.; Eftimovska, E.; Lind, C.; Hager, A.; Wasson, J.H.; Lindblad, S. Patient Reported Outcome Measures in Practice. BMJ 2015, 350, g7818. [Google Scholar] [CrossRef] [Green Version]
- Rotenstein, L.S.; Huckman, R.S.; Wagle, N.W. Making Patients and Doctors Happier—The Potential of Patient-Reported Outcomes. N. Engl. J. Med. 2017, 377, 1309–1312. [Google Scholar] [CrossRef]
- Austin, E.; LeRouge, C.; Hartzler, A.L.; Chung, A.E.; Segal, C.; Lavallee, D.C. Opportunities and Challenges to Advance the Use of Electronic Patient-Reported Outcomes in Clinical Care: A Report from AMIA Workshop Proceedings. JAMIA Open 2019, 2, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, C.-J.; Dymek, C.; Kim, B.; Russell, B. Advancing the Use of Patient-Reported Outcomes in Practice: Understanding Challenges, Opportunities, and the Potential of Health Information Technology. Qual. Life Res. 2019, 28, 1575–1583. [Google Scholar] [CrossRef] [PubMed]
- van der Hout, A.; van Uden-Kraan, C.F.; Holtmaat, K.; Jansen, F.; Lissenberg-Witte, B.I.; Nieuwenhuijzen, G.A.P.; Hardillo, J.A.; Baatenburg de Jong, R.J.; Tiren-Verbeet, N.L.; Sommeijer, D.W.; et al. Role of EHealth Application Oncokompas in Supporting Self-Management of Symptoms and Health-Related Quality of Life in Cancer Survivors: A Randomised, Controlled Trial. Lancet Oncol. 2020, 21, 80–94. [Google Scholar] [CrossRef]
- Snyder, C.; Smith, K.; Holzner, B.; Rivera, Y.M.; Bantug, E.; Brundage, M. PRO Data Presentation Delphi Panel Making a Picture Worth a Thousand Numbers: Recommendations for Graphically Displaying Patient-Reported Outcomes Data. Qual. Life Res. 2019, 28, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Warrington, L.; Absolom, K.; Velikova, G. Integrated Care Pathways for Cancer Survivors—A Role for Patient-Reported Outcome Measures and Health Informatics. Acta Oncol. 2015, 54, 600–608. [Google Scholar] [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehmann, J.; Rothmund, M.; Riedl, D.; Rumpold, G.; Grote, V.; Fischer, M.J.; Holzner, B. Clinical Outcome Assessment in Cancer Rehabilitation and the Central Role of Patient-Reported Outcomes. Cancers 2022, 14, 84. https://doi.org/10.3390/cancers14010084
Lehmann J, Rothmund M, Riedl D, Rumpold G, Grote V, Fischer MJ, Holzner B. Clinical Outcome Assessment in Cancer Rehabilitation and the Central Role of Patient-Reported Outcomes. Cancers. 2022; 14(1):84. https://doi.org/10.3390/cancers14010084
Chicago/Turabian StyleLehmann, Jens, Maria Rothmund, David Riedl, Gerhard Rumpold, Vincent Grote, Michael J. Fischer, and Bernhard Holzner. 2022. "Clinical Outcome Assessment in Cancer Rehabilitation and the Central Role of Patient-Reported Outcomes" Cancers 14, no. 1: 84. https://doi.org/10.3390/cancers14010084