
Ultrahypofractionated Radiotherapy versus Conventional to Moderate Hypofractionated Radiotherapy for Clinically Localized Prostate Cancer

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment Planning
2.3. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
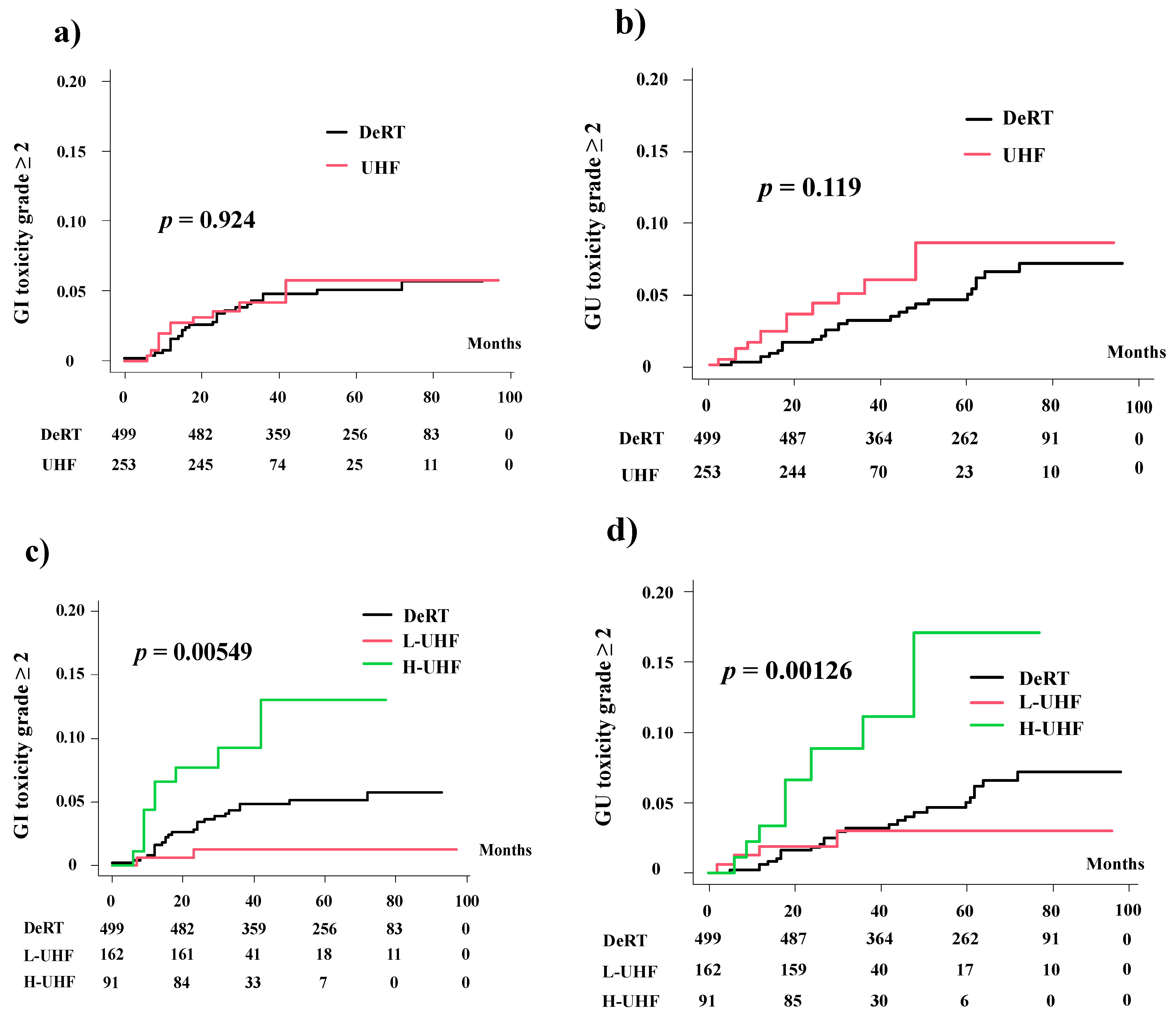
3.2. Late Toxicity
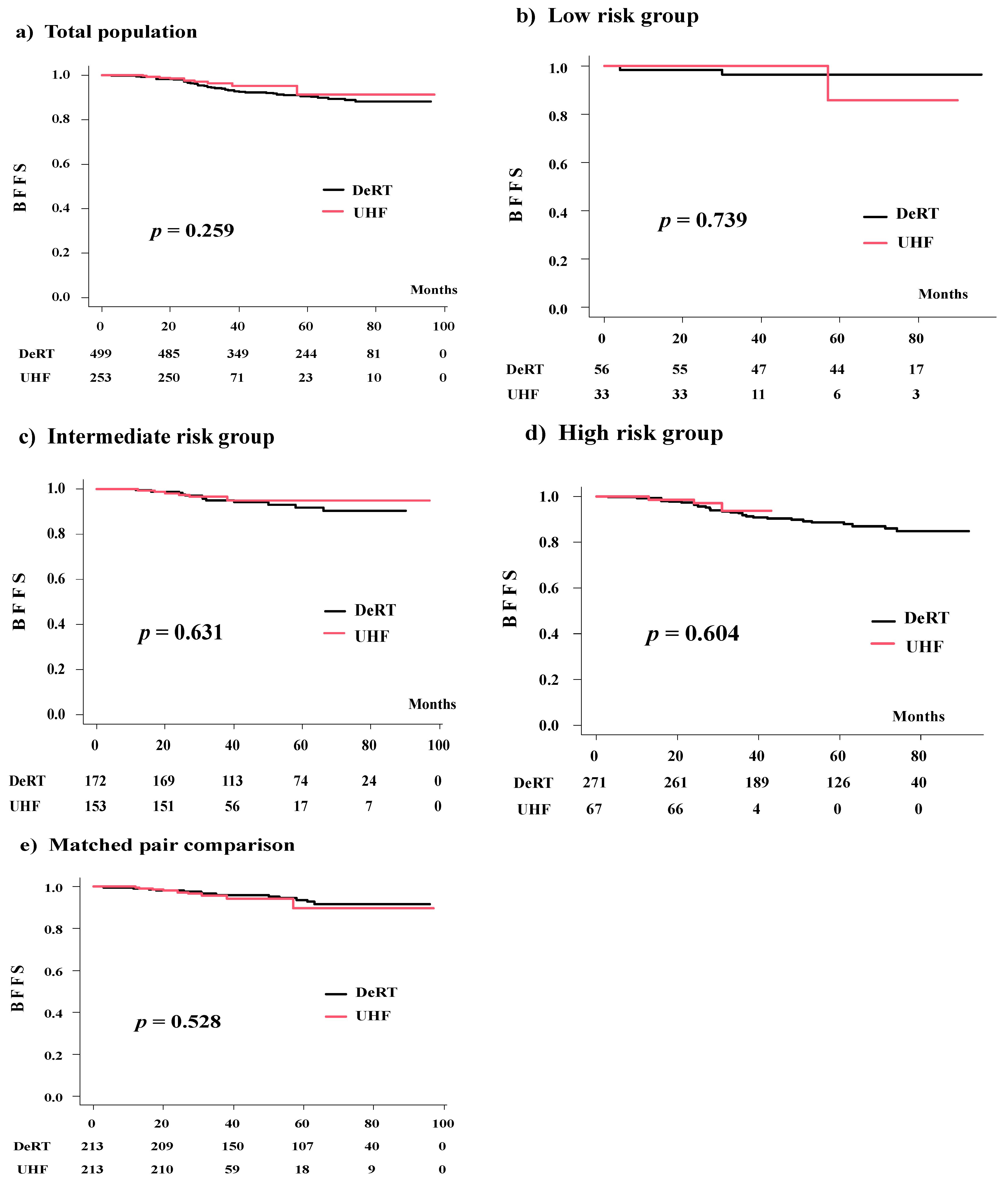
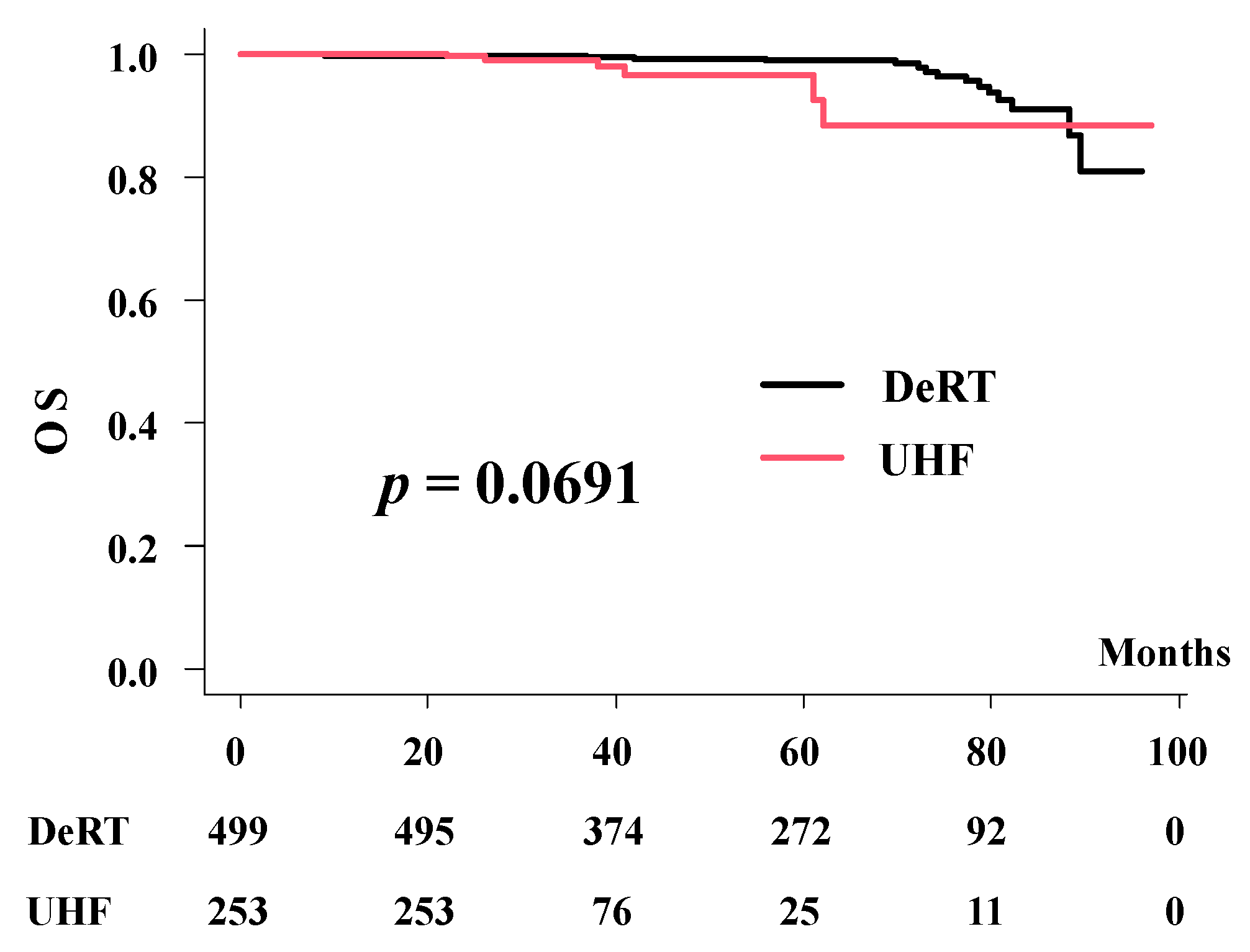
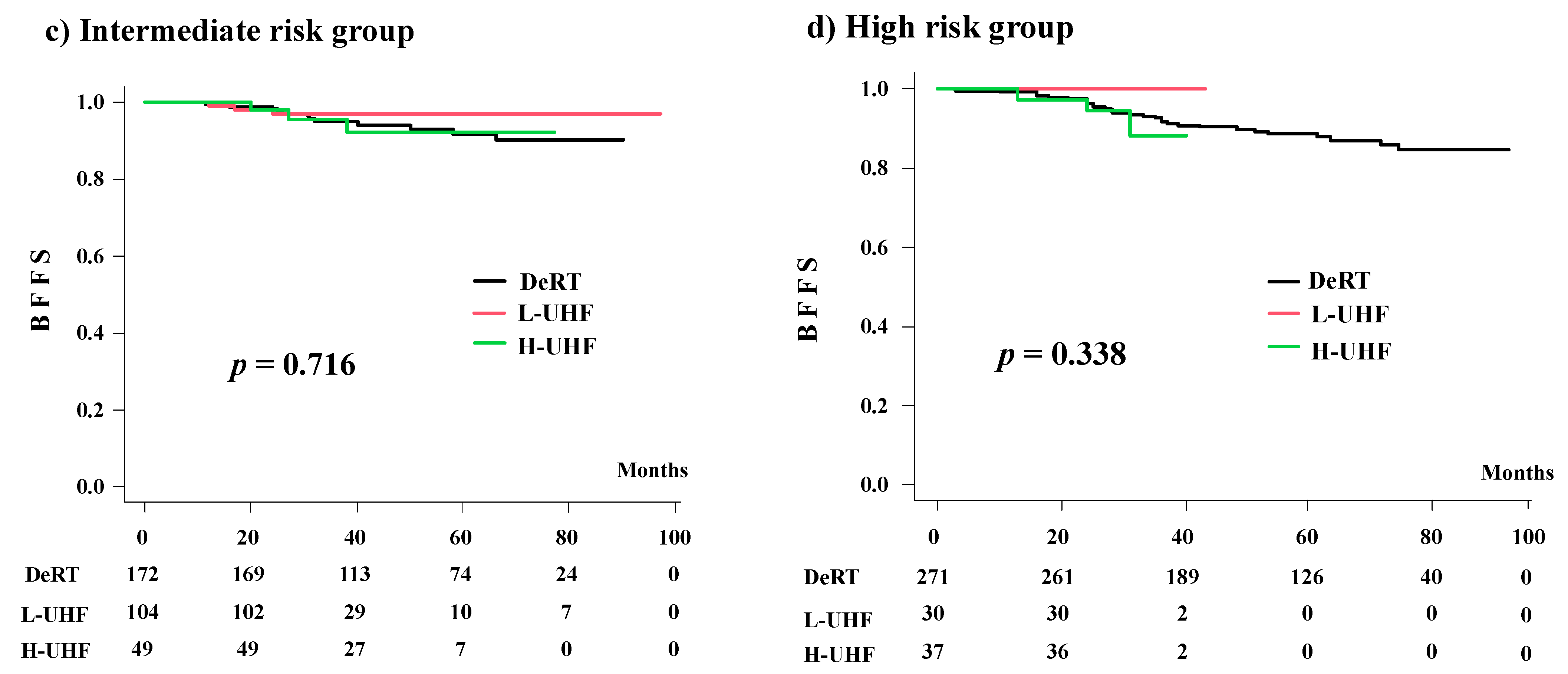
3.3. Biochemical Control, Overall, and Prostate Cancer-Specific Survival
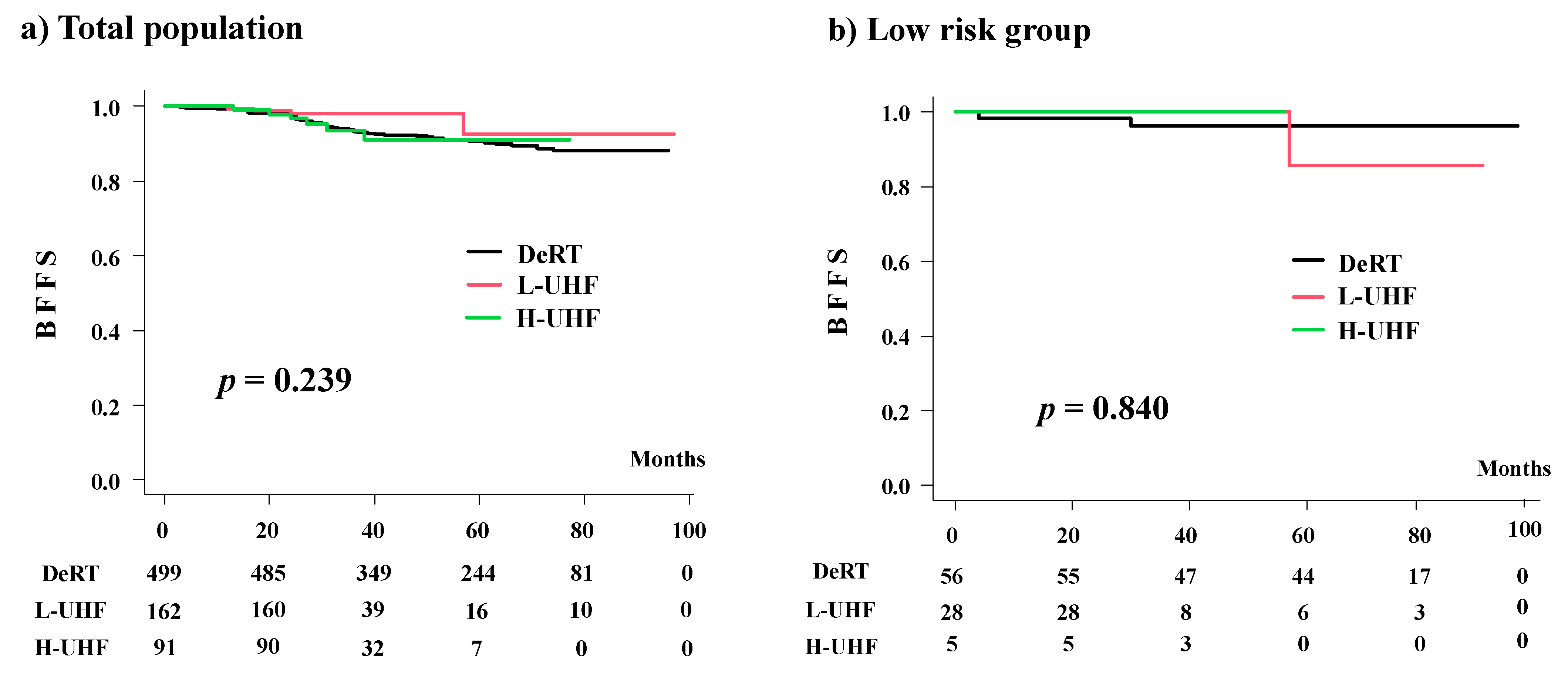
3.4. Comparison among the Three Groups (DeRT vs. L-UHF vs. H-UHF)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Cancer Facts & Figures 2019. Survival Rates for Prostate Cancer. Available online: https://www.cancer.org/cancer/prostate-cancer/detection-diagnosis-staging/survival-rates.html (accessed on 30 January 2021).
- The National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology. Prostate Cancer. 2019. Version 4. Available online: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 10 January 2020).
- Morgan, S.C.; Hoffman, K.; Loblaw, D.A.; Buyyounouski, M.K.; Patton, C.; Barocas, D.; Bentzen, S.; Chang, M.; Efstathiou, J.; Greany, P.; et al. Hypofractionated radiation therapy for localized prostate cancer: An ASTRO, ASCO, and AUA evidence-based guideline. J. Clin. Oncol. 2018, 8, 354–360. [Google Scholar]
- Ishiyama, H.; Tsumura, H.; Nagano, H.; Watanabe, M.; Mizuno, E.; Taka, M.; Kobayashi, H.; Eriguchi, T.; Imada, H.; Inaba, K.; et al. Multi-Institutional retrospective analysis of ultrahypofractionated radiotherapy for Japanese prostate cancer patients. Sci. Rep. 2021, 11, 13194. [Google Scholar] [CrossRef] [PubMed]
- Kainuma, T.; Kawakami, S.; Tsumura, H.; Satoh, T.; Tabata, K.I.; Iwamura, M.; Hayakawa, K.; Ishiyama, H. A phase I dose-escalation trial of stereotactic body radiotherapy using 4 fractions for patients with localized prostate cancer. Radiat. Oncol. 2019, 14, 158. [Google Scholar] [CrossRef] [Green Version]
- An Open Data of Multicenter Data Collection: Outcome of Radiation Therapy for Prostate Cancer (DeRT: B16-143 (UFH:B20-118)). Available online: https://www.khp.kitasato-u.ac.jp/ska/radiotherapy/arcivements/#results (accessed on 30 March 2021).
- Viani, G.A.; Stefano, E.J.; Alfonso, S.L. Higher-than-Conventional radiation doses in localized prostate cancer treatment: A meta-analysis of randomized, controlled trials. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1405–1418. [Google Scholar] [CrossRef]
- Sasaki, N.; Yamazaki, H.; Shimizu, D.; Suzuki, G.; Masui, K.; Nakamura, S.; Okabe, H.; Nishikawa, T.; Yoshida, K. Long-Term outcomes of a dose-reduction trial to decrease late gastrointestinal toxicity in patients with prostate cancer receiving soft tissue-matched image-guided intensity-modulated radiotherapy. Anticancer. Res. 2018, 38, 385–391. [Google Scholar]
- Koontz, B.F.; Bossi, A.; Cozzarini, C.; Wiegel, T.; D’Amico, A. A systematic review of hypofractionation for primary management of prostate cancer. Eur. Urol. 2015, 68, 683–691. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Widmark, A.; Gunnlaugsson, A.; Beckman, L.; Thellenberg-Karlsson, C.; Hoyer, M.; Kindblom, J.; Ginman, C.; Johansson, B.; Björnlinger, K. Ultra-Hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial. Lancet 2019, 394, 385–395. [Google Scholar] [CrossRef]
- Katz, A. Stereotactic body radiotherapy for low-risk prostate cancer: A ten-year analysis. Cureus 2019, 9, e1668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Johnson, J.; Gottschalk, A.R.; Chang, A.J.; Hsu, I.C.; Roach, M., 3rd; Seymour, Z.A. Receiver operating curves and dose-volume analysis of late toxicity with stereotactic body radiation therapy for prostate cancer. Pract. Radiat. Oncol. 2017, 7, e109–e116. [Google Scholar] [CrossRef]
- Macias, V.A.; Blanco, M.L.; Barrera, I.; Garcia, R. A phase II study of stereotactic body radiation therapy for low-intermediate-high-risk prostate cancer using helical Tomotherapy: Dose-Volumetric parameters predicting early toxicity. Front. Oncol. 2014, 4, 336. [Google Scholar] [CrossRef] [Green Version]
- Bernetich, M.; Oliai, C.; Lanciano, R.; Hanlon, A.; Lamond, J.; Arrigo, S.; Yang, J.; Good, M.; Feng, J.; Brown, R. SBRT for the primary treatment of localized prostate cancer: The effect of gleason score, dose and heterogeneity of intermediate risk on outcome utilizing 2.2014 NCCN risk stratification guidelines. Front. Oncol. 2014, 4, 312. [Google Scholar] [CrossRef]
- Chen, L.N.; Suy, S.; Uhm, S.; Oermann, E.K.; Ju, A.W.; Chen, V.; Hanscom, H.N.; Laing, S.; Kim, J.S.; Lei, S.; et al. Stereotactic body radiation therapy (SBRT) for clinically localized prostate cancer: The Georgetown University experience. Radiat. Oncol. 2013, 8, 58. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.W.; Cho, L.C.; Straka, C.; Christie, A.; Lotan, Y.; Pistenmaa, D.; Kavanagh, B.D.; Nanda, A.; Kueplian, P.; Brindle, J.; et al. Predictors of rectal tolerance observed in a dose-escalated phase 1-2 trial of stereotactic body radiation therapy for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 509–517. [Google Scholar] [CrossRef]
- Kishan, A.U.; Dang, A.; Katz, A.J.; Mantz, C.A.; Collins, S.P.; Aghdam, N.; Chu, F.I.; Kaplan, I.D.; Appelbaum, L.; Fuller, D.B.; et al. Long-Term outcomes of stereotactic body radiotherapy for low-risk and intermediate-risk prostate cancer. JAMA Netw. Open 2019, 2, e188006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musunuru, H.B.; Quon, H.; Davidson, M.; Cheung, P.; Zhang, L.; D’Alimonte, L.; Deabreu, A.; Mamedov, A.; Loblaw, A. Dose-Escalation of five-fraction SABR in prostate cancer: Toxicity comparison of two prospective trials. Radiother. Oncol. 2016, 118, 112–117. [Google Scholar] [CrossRef]
- Royce, T.J.; Mavroidis, P.; Wang, K.; Falchook, A.D.; Sheets, N.C.; Fuller, D.B.; Collins, S.P.; Naqa, I.E.l.; Song, D.Y.; Ding, G.X.; et al. Tumor Control probability modeling and systematic review of the literature of stereotactic body radiation therapy for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 227–236. [Google Scholar] [CrossRef]
- Meier, R.M.; Bloch, D.A.; Cotrutz, C.; Beckman, A.C.; Henning, G.T.; Woodhouse, S.A.; Williamson, S.K.; Mohideen, N.; Dombrowski, J.J.; Hong, R.L.; et al. Multicenter trial of stereotactic body radiation therapy for low-and intermediate-risk prostate cancer: Survival and toxicity endpoints. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, A.; Henry, A.; Mitin, T.; Chen, R.; Joseph, N.; Spratt, D.E. Photons, Protons, SBRT, brachytherapy-what is leading the charge for the management of prostate cancer? A perspective from the GU editorial team. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Brand, D.H.; Tree, A.C.; Ostler, P.; van der Voet, H.; Loblaw, A.; Chu, W.; Ford, D.; Tolan, S.; Jain, S.; Martin, A.; et al. PACE Trial Investigators. Intensity-modulated fractionated radiotherapy versus stereotactic body radiotherapy for prostate cancer (PACE-B): Acute toxicity findings from an international, randomised, open-label, phase 3, non-inferiority trial. Lancet Oncol. 2019, 20, 1531–1543. [Google Scholar] [CrossRef]
- Zelefsky, M.J.; Kollmeier, M.; McBride, S.; Varghese, M.; Mychalczak, B.; Gewanter, R.; Garg, M.K.; Happersett, L.; Goldman, D.A.; Pei, I.; et al. Five-Year Outcomes of a phase 1 dose-escalation study using stereotactic body radiosurgery for patients with low-risk and intermediate-risk prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Helou, J.; D’Alimonte, L.; Quon, H.; Deabreu, A.; Commisso, K.; Cheung, P.C.; Chu, W.; Mamedov, A.; Davidson, M.; Ravi, A.; et al. Stereotactic ablative radiotherapy in the treatment of low and intermediate risk prostate cancer: Is there an optimal dose? Radiother. Oncol. 2017, 123, 478–482. [Google Scholar] [CrossRef]
- Zimmermann, M.; Taussky, D.; Menkarios, C.; Vigneault, É.; Beauchemin, M.C.; Bahary, J.P.; Bahary, J.P.; Martin, A.A.; Diaz de Bedoya, L.V.; Lambert, C. Prospective phase II trial of once-weekly Hypofractionated Radiation therapy for low-risk adenocarcinoma of the prostate: Late toxicities and outcomes. Clin. Oncol. (R Coll Radiol.) 2016, 28, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Scobioala, S.; Kittel, C.; Elsayad, K.; Kroeger, K.; Oertel, M.; Samhouri, L.; Haverkamp, U.; Eich, H.T. A treatment planning study comparing IMRT techniques and cyber knife for stereotactic body radiotherapy of low-risk prostate carcinoma. Radiat. Oncol. 2019, 14, 143. [Google Scholar] [CrossRef]
- De Chavez, R.; Grogan, G.; Hug, B.; Howe, K.; Grigg, A.; Waterhouse, D.; Lane, J.; Glyde, A.; Brown, E.; Bydder, S.; et al. Assessment of HDR brachytherapy-replicating prostate radiotherapy planning for tomotherapy, cyberknife and VMAT. Med. Dosim. 2021, S0958-3947, 00078–00079. [Google Scholar] [CrossRef] [PubMed]
- Serra, M.; Ametrano, G.; Borzillo, V.; Quarto, M.; Muto, M.; Di Franco, R.; Federica, S.; Loffredo, F.; Paolo, M. Dosimetric comparison among cyberknife, helical tomotherapy and VMAT for hypofractionated treatment in localized prostate cancer. Medicine 2020, 99, e23574. [Google Scholar] [CrossRef]
- Chen, C.Y.; Lee, L.M.; Yu, H.W.; Lee, S.P.; Lee, H.L.; Lin, Y.W.; Wen, Y.C.; Chen, Y.J.; Chen, C.P.; Tsai, J.T. Dosimetric and radiobiological comparison of Cyberknife and Tomotherapy in stereotactic body radiotherapy for localized prostate cancer. J. Xray Sci. Technol. 2017, 25, 465–477. [Google Scholar] [CrossRef]
- Wang, K.; Mavroidis, P.; Royce, T.J.; Falchook, A.D.; Collins, S.P.; Sapareto, S.; Sheets, N.C.; Fuller, D.B.; El Naqa, I. Prostate stereotactic body radiation therapy: An overview of toxicity and dose response. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 237–248. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Group | DeRT | UHF | p-Value |
|---|---|---|---|---|
| (n = 499) | (n = 253) | |||
| Age | 71.0 [51.0, 86.0] | 72.00 [54.0, 86.0] | 0.069 | |
| iPSA (mg/mL) | 10.21 [3.00, 1454.0] | 8.12 [1.70, 188.0] | <0.001 | |
| T (%) | ≤T2a | 250 (50.2) | 178 (70.4) | <0.001 |
| T2b or c | 121 (24.3) | 50 (19.8) | ||
| T3≤ | 127 (25.5) | 25 (9.9) | ||
| GS (%) | ≤6 | 118 (23.6) | 56 (22.1) | <0.001 |
| 7 | 202 (40.5) | 140 (55.3) | ||
| 8≤ | 178 (35.7) | 57 (22.5) | ||
| NA | 1 (0.2) | 0 (0.0) | ||
| NCCN (%) | High | 271 (54.3) | 67 (26.5) | <0.001 |
| Intermediate | 172 (34.5) | 153 (60.5) | ||
| Low | 56 (11.2) | 33 (13.0) | ||
| EQD2Gy (α/β = 1.5 Gy) | (Gy1.5) | 78.0 [72.0, 91.5] | 90.6 [85.0, 108.0] | <0.001 |
| Follow-up periods | (months) | 61.7 [9.0, 96.0] | 32.0 [22.0, 97.0] | <0.001 |
| Hormonal therapy (%) | Yes | 343 (68.7) | 149 (58.9) | 0.009 |
| No | 156 (31.3) | 104 (41.1) | ||
| Total Hormonal therapy duration | (months) | 8.00 [2.0, 96.0] | 12.0 [2.0, 51.0] | 0.749 |
| Neoadjuvant Hormonal therapy (%) | Yes | 332 (83.8) | 143 (56.5) | <0.001 |
| No | 64 (16.2) | 110 (43.5) | ||
| Neoadjuvant duration | (months) | 6.00 [1.0, 96.0] | 6.00 [1.0, 48.0] | <0.001 |
| Adjuvant Hormonal therapy (%) | Yes | 108 (21.7) | 81 (32.0) | 0.002 |
| No | 390 (78.3) | 172 (68.0) | ||
| Adjuvant duration | (months) | 23.50 [3.0, 8000] | 23.0 [1.0, 33.0] | 0.199 |
| Group | Subgroup | Prescribed Dose/ Fraction No | Treatment | PTNO | EQD2 |
|---|---|---|---|---|---|
| UHF | L-UHF | 35 Gy/5 fr | SBRT | 63 | 85 |
| 32 Gy/4 fr | SBRT | 9 | 87 | ||
| 36.2 5Gy/5 fr | SBRT | 81 | 91 | ||
| 34 Gy/4 fr | SBRT | 9 | 97 | ||
| H-UHF | 36 Gy/4 fr | SBRT | 91 | 108 | |
| DeRT | 62 Gy/20 fr | IMRT | 4 | 82 | |
| 65 Gy/26 fr | IMRT | 3 | 74 | ||
| 67.5 Gy/27 fr | IMRT | 6 | 77 | ||
| 70 Gy/28 fr | IMRT | 83 | 80 | ||
| 72 Gy/36 fr | IMRT | 25 | 72 | ||
| 72. 6 Gy/33 fr | IMRT | 23 | 77 | ||
| 74 Gy/37 fr | IMRT | 125 | 74 | ||
| 74.8 Gy/34 fr | IMRT | 103 | 79 | ||
| 76 Gy/28 fr | IMRT | 1 | 92 | ||
| 78 Gy/39 fr | IMRT | 81 | 78 | ||
| 80 Gy/40 fr | IMRT | 45 | 80 |
| Comparison between UHF and DeRT. | ||||||
| Toxicities | Grade | UHF | DeRT | p-value | ||
| (n = 253) | (n = 499) | |||||
| No. PT | (%) | No. PT | (%) | |||
| Gastrointestinal | 0 | 206 | (81%) | 422 | (85%) | 0.633 |
| 1 | 36 | (14%) | 55 | (11%) | ||
| 2 | 9 | (4%) | 17 | (3%) | ||
| 3 | 2 | (1%) | 5 | (1%) | ||
| Genitourinary | 0 | 170 | (67%) | 405 | (81%) | 0.0001 |
| 1 | 69 | (27%) | 70 | (14%) | ||
| 2 | 13 | (5%) | 22 | (4%) | ||
| 3 | 1 | (0.4%) | 2 | (0%) | ||
| Comparison between H-UHF and L-UHF. | ||||||
| Toxicities | Grade | L-UHF | H-UHF | p-value | ||
| (n = 162) | (n = 91) | |||||
| No. PT | (%) | No. PT | (%) | |||
| Gastrointestinal | 0 | 151 | (93%) | 55 | (60%) | <0.0001 |
| 1 | 9 | (6%) | 27 | (30%) | ||
| 2 | 2 | (1%) | 7 | (8%) | ||
| 3 | 2 | (2%) | ||||
| Genitourinary | 0 | 131 | (81%) | 39 | (43%) | <0.0001 |
| 1 | 27 | (17%) | 42 | (46%) | ||
| 2 | 4 | (2%) | 9 | (10%) | ||
| 3 | 1 | (1%) | ||||
| Variable | Strata | Uni-Variate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | ||
| Age, years | ≤74 | 1 | (referent) | - | 1 | (referent) | - |
| 75≤ | 0.8974 | 0.5015–1.606 | 0.7156 | 0.92 | 0.51–1.67 | 0.79 | |
| T classification | ≤2 | 1 | (referent) | - | 1 | (referent) | - |
| 3≤ | 2.045 | 1.173–3.566 | 0.01164 | 1.84 | 0.94–3.59 | 0.075 | |
| Gleason score | ≤7 | 1 | (referent) | - | 1 | (referent) | - |
| 8≤ | 1.682 | 0.9871–2.867 | 0.05585 | 1.6 | 0.89–2.89 | 0.12 | |
| Pretreatment PSA (ng/mL) | ≤10 | 1 | (referent) | - | 1 | (referent) | - |
| 10< | 2.339 | 1.342–4.078 | 0.002729 | 2.3 | 1.24–4.28 | 0.0084 | |
| NCCN risk classification | Low | 1 | (referent) | - | NA | ||
| Intermediate | 2.03 | 0.597–6.906 | 0.257 | ||||
| High | 3.495 | 1.073–11.386 | 0.0379 | ||||
| Hormonal therapy | No | 1 | (referent) | - | 1 | (referent) | - |
| Yes | 0.9285 | 0.5344–1.613 | 0.7925 | 0.45 | 0.23–0.90 | 0.023 | |
| Treatment modalities | DeRT | 1 | (referent) | - | 1 | (referent) | - |
| UHF | 0.6195 | 0.3079–1.247 | 0.1797 | 0.79 | 0.38–1.63 | 0.52 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamazaki, H.; Suzuki, G.; Aibe, N.; Shimizu, D.; Kimoto, T.; Masui, K.; Yoshida, K.; Nakamura, S.; Hashimoto, Y.; Okabe, H. Ultrahypofractionated Radiotherapy versus Conventional to Moderate Hypofractionated Radiotherapy for Clinically Localized Prostate Cancer. Cancers 2022, 14, 195. https://doi.org/10.3390/cancers14010195
Yamazaki H, Suzuki G, Aibe N, Shimizu D, Kimoto T, Masui K, Yoshida K, Nakamura S, Hashimoto Y, Okabe H. Ultrahypofractionated Radiotherapy versus Conventional to Moderate Hypofractionated Radiotherapy for Clinically Localized Prostate Cancer. Cancers. 2022; 14(1):195. https://doi.org/10.3390/cancers14010195
Chicago/Turabian StyleYamazaki, Hideya, Gen Suzuki, Norihiro Aibe, Daisuke Shimizu, Takuya Kimoto, Koji Masui, Ken Yoshida, Satoaki Nakamura, Yasutoshi Hashimoto, and Haruumi Okabe. 2022. "Ultrahypofractionated Radiotherapy versus Conventional to Moderate Hypofractionated Radiotherapy for Clinically Localized Prostate Cancer" Cancers 14, no. 1: 195. https://doi.org/10.3390/cancers14010195