
Risk Stratification, Measurable Residual Disease, and Outcomes of AML Patients with a Trisomy 8 Undergoing Allogeneic Hematopoietic Stem Cell Transplantation

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Patient Population
2.2. Flow Cytometry, Cytogenetics, and Molecular Markers
2.3. MRD Status at HSCT
2.4. Definition of Clinical Endpoints and Statistical Analyses
3. Results
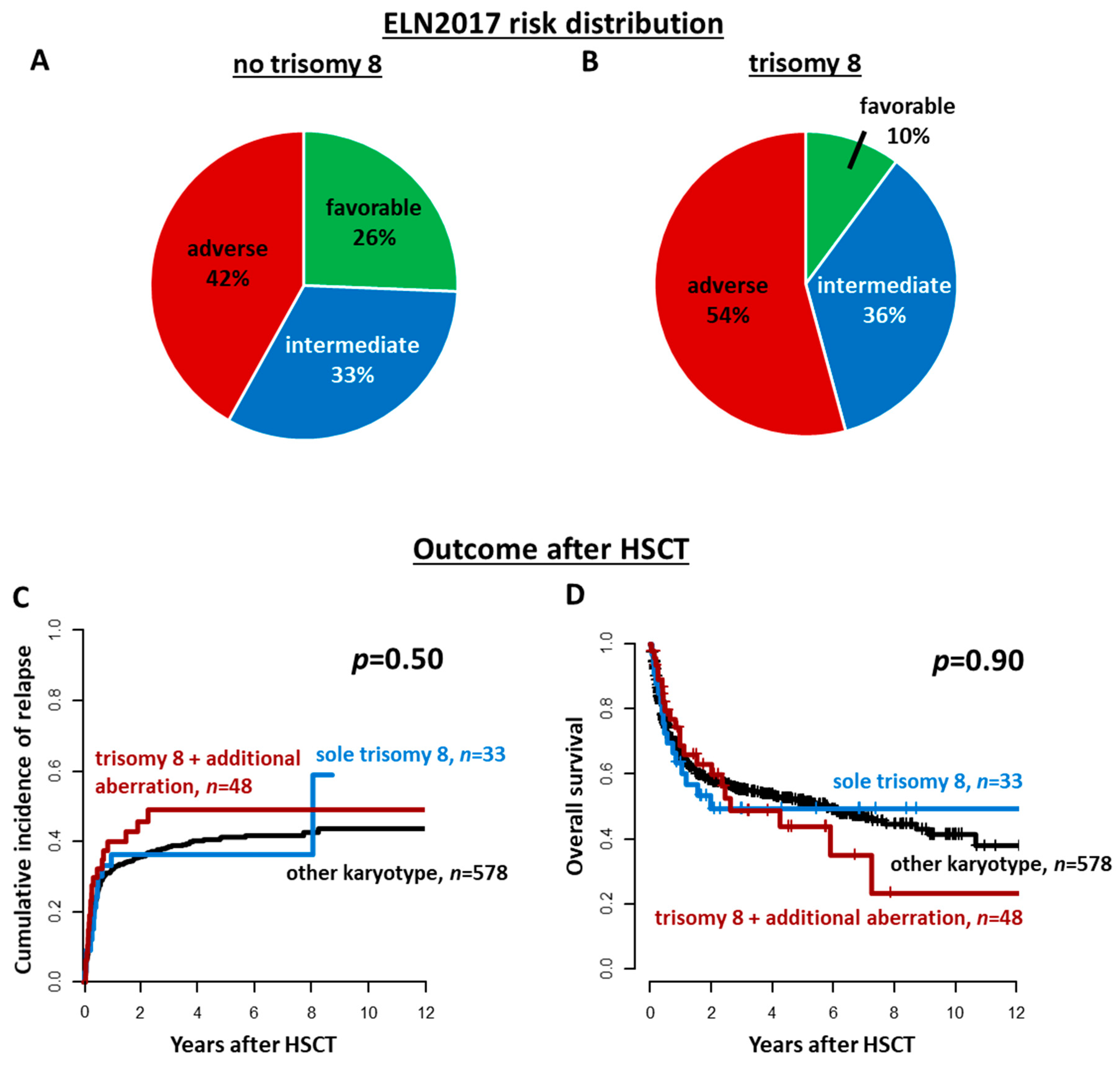
3.1. Incidence of Trisomy 8 in AML Patients Subjected to Allogeneic HSCT
3.2. Characteristics of AML Patients Harboring a Trisomy 8
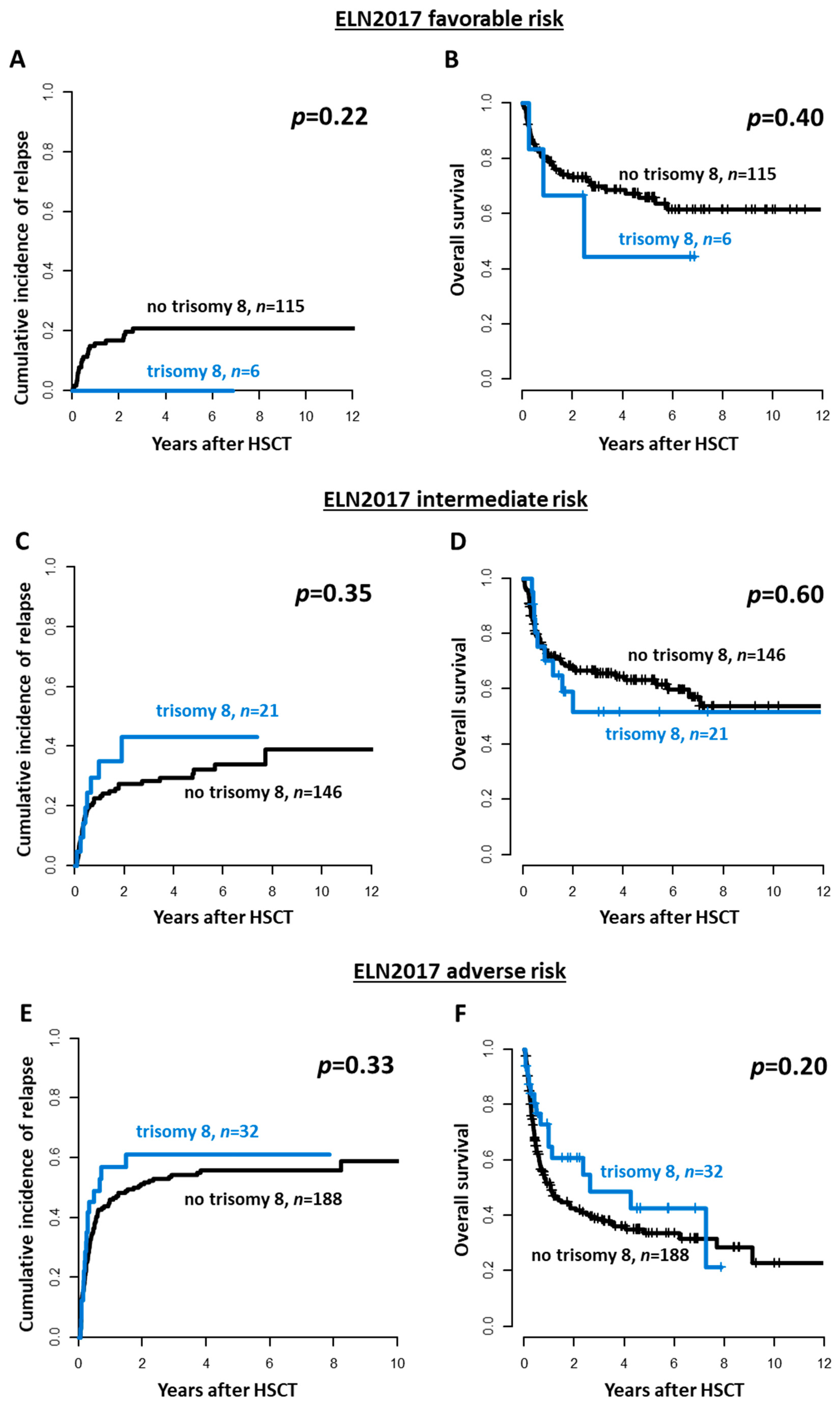
3.3. Outcomes of AML Patients Harboring a Trisomy 8
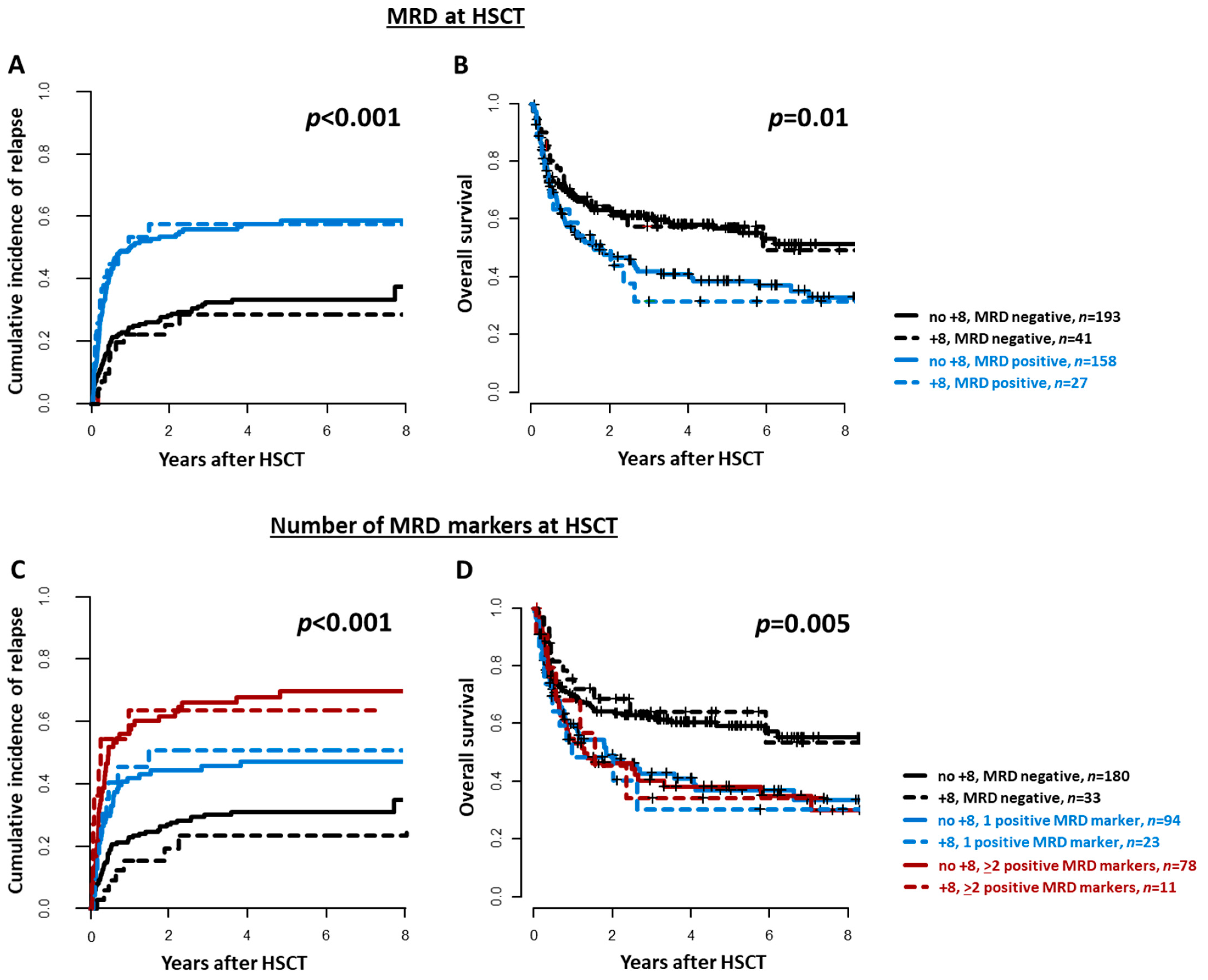
3.4. MRD at HSCT in AML Patients Harboring a Trisomy 8
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grimwade, D.; Hills, R.K.; Moorman, A.V.; Walker, H.; Chatters, S.; Goldstone, A.H.; Wheatley, K.; Harrison, C.J.; Burnett, A.K. Refinement of cytogenetic classification in acute myeloid leukemia: Determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood 2010, 116, 354–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrd, J.; Mrózek, K.; Dodge, R.; Carroll, A. Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: Results from Cancer and Leukemia Group B (CALGB 8461). Blood 2002, 100, 4325–4336. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.H.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Burnett, A.K.; Dombret, H.; Fenaux, P.; Grimwade, D.; Larson, R.A.; et al. Diagnosis and management of acute myeloid leukemia in adults: Recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood 2010, 115, 453–474. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; Levine, R.L.; Lo-coco, F.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [Green Version]
- Grimwade, D.; Walker, H.; Oliver, F.; Wheatley, K.; Harrison, C.; Harrison, G.; Rees, J.; Hann, I.; Stevens, R.; Burnett, A.; et al. The importance of diagnostic cytogenetics on outcome in AML: Analysis of 1612 patients entered into the MRC AML 10 trial. Blood 1998, 92, 2322–2333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alpermann, T.; Haferlach, C.; Eder, C.; Nadarajah, N.; Meggendorfer, M.; Kern, W.; Haferlach, T.; Schnittger, S. AML with gain of chromosome 8 as the sole chromosomal abnormality (+ 8sole) is associated with a specific molecular mutation pattern including ASXL1 mutations in 46.8% of the patients. Leuk. Res. 2015, 39, 265–272. [Google Scholar] [CrossRef]
- Wolman, S.R.; Gundacker, H.; Appelbaum, F.R.; Slovak, M.L. Impact of trisomy 8 (+8) on clinical presentation, treatment response, and survival in acute myeloid leukemia: A Southwest Oncology Group study. Blood 2002, 100, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Schaich, M.; Schlenk, R.F.; Al-Ali, H.K.; Döhner, H.; Ganser, A.; Heil, G.; Illmer, T.; Krahl, R.; Krauter, J.; Sauerland, C.; et al. Prognosis of acute myeloid leukemia patients up to 60 years of age exhibiting trisomy 8 within a non-complex karyotype: Individual patient data-based meta-analysis of the German Acute Myeloid Leukemia Intergroup. Haematologica 2007, 92, 763–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoch, C.; Haase, D.; Fonatsch, C.; Haferlach, T.; Löffler, H.; Schlegelberger, B.; Hossfeld, D.K.; Becher, R.; Sauerland, M.C.; Heinecke, A.; et al. The significance of trisomy 8 in de novo acute myeloid leukaemia: The accompanying chromosome aberrations determine the prognosis. Br. J. Haematol. 1997, 99, 605–611. [Google Scholar] [CrossRef]
- Konuma, T.; Kondo, T.; Yamashita, T.; Uchida, N.; Fukuda, T.; Ozawa, Y.; Ohashi, K.; Ogawa, H.; Kato, C.; Takahashi, S.; et al. Outcome of allogeneic hematopoietic stem cell transplantation in adult patients with acute myeloid leukemia harboring trisomy 8. Ann. Hematol. 2017, 96, 469–478. [Google Scholar] [CrossRef]
- Cornelissen, J.J.; Gratwohl, A.; Schlenk, R.F.; Sierra, J.; Bornhäuser, M.; Juliusson, G.; Råcil, Z.; Rowe, J.M.; Russell, N.; Mohty, M.; et al. The European LeukemiaNet AML Working Party consensus statement on allogeneic HSCT for patients with AML in remission: An integrated-risk adapted approach. Nat. Rev. Clin. Oncol. 2012, 9, 579–590. [Google Scholar] [CrossRef]
- Baron, F.; Labopin, M.; Blaise, D.; Gérard, M.I.; Forcade, E.; Norbert, I.Y.; Gorin, C.; Esteve, J.; Nagler, A.; Mohty, M. Better leukemia-free survival with allogeneic than with autologous HCT in AML patients with isolated trisomy 8: A study from the ALWP of the EBMT. Bone Marrow Transplant. 2021, 56, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Chevallier, P.; Labopin, M.; Nagler, A.; Ljungman, P.; Verdonck, L.F.; Volin, L.; Zander, A.R.; Finke, J.; Socie, G.; Cordonnier, C.; et al. Outcome after allogeneic transplantation for adult acute myeloid leukemia patients exhibiting isolated or associated trisomy 8 chromosomal abnormality: A survey on behalf of the ALWP of the EBMT. Bone Marrow Transplant. 2009, 44, 589–594. [Google Scholar] [CrossRef] [Green Version]
- Thol, F.; Gabdoulline, R.; Liebich, A.; Klement, P.; Schiller, J.; Kandziora, C.; Hambach, L.; Stadler, M.; Koenecke, C.; Flintrop, M.; et al. Measurable residual disease monitoring by ngs before allogeneic hematopoietic cell transplantation in AML. Blood 2018, 132, 1703–1713. [Google Scholar] [CrossRef] [Green Version]
- Krönke, J.; Schlenk, R.F.; Jensen, K.O.; Tschürtz, F.; Corbacioglu, A.; Gaidzik, V.I.; Paschka, P.; Onken, S.; Eiwen, K.; Habdank, M.; et al. Monitoring of minimal residual disease in NPM1-mutated acute myeloid leukemia: A study from the German-Austrian acute myeloid leukemia study group. J. Clin. Oncol. 2011, 29, 2709–2716. [Google Scholar] [CrossRef] [PubMed]
- Ivey, A.; Hills, R.K.; Simpson, M.A.; Jovanovic, J.V.; Gilkes, A.; Grech, A.; Patel, Y.; Bhudia, N.; Farah, H.; Mason, J.; et al. Assessment of minimal residual disease in standard-risk AML. N. Engl. J. Med. 2016, 374, 422–433. [Google Scholar] [CrossRef] [Green Version]
- Jentzsch, M.; Grimm, J.; Bill, M.; Brauer, D.; Backhaus, D.; Schulz, J.; Goldmann, K.; Niederwieser, D.; Platzbecker, U.; Schwind, S. Prognostic relevance of remission and measurable residual disease status in AML patients prior to reduced intensity or non-myeloablative allogeneic stem cell transplantation. Blood Cancer J. 2021, in press. [Google Scholar] [CrossRef]
- Mitelman, F. An International System for Human Cytogenetic Nomenclature: Recommendations of the International Standing Committee on Human Cytogenetic Nomenclature; S. Karger Publishers: Basel, Switzerland, 1995. [Google Scholar]
- Bill, M.; Jentzsch, M.; Grimm, J.; Schubert, K.; Lange, T.; Cross, M.; Behre, G.; Vucinic, V.; Pönisch, W.; Franke, G.N.; et al. Prognostic impact of the European LeukemiaNet standardized reporting system in older AML patients receiving stem cell transplantation after non-myeloablative conditioning. Bone Marrow Transplant. 2017, 52, 932–935. [Google Scholar] [CrossRef] [PubMed]
- Grimm, J.; Jentzsch, M.; Bill, M.; Goldmann, K.; Schulz, J.; Niederwieser, D.; Platzbecker, U. Prognostic impact of the ELN2017 risk classi fi cation in patients with AML receiving allogeneic transplantation. Blood Adv. 2020, 4, 3864–3874. [Google Scholar] [CrossRef]
- Jentzsch, M.; Bill, M.; Grimm, J.; Schulz, J.; Schuhmann, L.; Brauer, D.; Goldmann, K.; Wilke, F.; Franke, G.-N.; Behre, G.; et al. High expression of the stem cell marker GPR56 at diagnosis identifies acute myeloid leukemia patients at higher relapse risk after allogeneic stem cell transplantation in context with the CD34+/CD38- population. Haematologica 2020, 105, e507. [Google Scholar] [CrossRef]
- Grimm, J.; Bill, M.; Jentzsch, M.; Beinicke, S.; Häntschel, J.; Goldmann, K.; Schulz, J.; Cross, M.; Franke, G.-N.; Behre, G.; et al. Clinical impact of clonal hematopoiesis in acute myeloid leukemia patients receiving allogeneic transplantation. Bone Marrow Transplant. 2019, 54, 1189–1197. [Google Scholar] [CrossRef]
- Metzeler, K.H.; Becker, H.; Maharry, K.; Radmacher, M.D.; Kohlschmidt, J.; Mrózek, K.; Nicolet, D.; Whitman, S.P.; Wu, Y.Z.; Schwind, S.; et al. ASXL1 mutations identify a high-risk subgroup of older patients with primary cytogenetically normal AML within the ELN Favorable genetic category. Blood 2011, 118, 6920–6929. [Google Scholar] [CrossRef]
- Bill, M.; Grimm, J.; Jentzsch, M.; Kloss, L.; Goldmann, K.; Schulz, J.; Beinicke, S.; Häntschel, J.; Cross, M.; Vucinic, V.; et al. Digital droplet PCR-based absolute quantification of pre-transplant NPM1 mutation burden predicts relapse in acute myeloid leukemia patients. Ann. Hematol. 2018, 97, 1757–1765. [Google Scholar] [CrossRef]
- Jentzsch, M.; Grimm, J.; Bill, M.; Küpper, J.; Backhaus, D.; Brauer, D.; Schulz, J.; Franke, G.; Vucinic, V.; Niederwieser, D.; et al. Measurable residual disease of canonical versus non-canonical DNMT3A, TET2, or ASXL1 mutations in AML at stem cell transplantation. Bone Marrow Transplant. 2021, 56, 2610–2612. [Google Scholar] [CrossRef]
- Bill, M.; Jentzsch, M.; Grimm, J.; Schmalbrock, L.K.; Küpper, J.; Backhaus, D.; Brauer, D.; Goldmann, K.; Franke, G.-N.; Vucinic, V.; et al. Impact of IDH Mutation Detection at Diagnosis and in Remission in AML Undergoing Allogeneic Transplantation. Under Revision.
- Jentzsch, M.; Bill, M.; Grimm, J.; Schulz, J.; Goldmann, K.; Beinicke, S.; Häntschel, J.; Pönisch, W.; Franke, G.-N.; Vucinic, V.; et al. High BAALC copy numbers in peripheral blood prior to allogeneic transplantation predict early relapse in acute myeloid leukemia patients. Oncotarget 2017, 8, 87944–87954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jentzsch, M.; Bill, M.; Grimm, J.; Schulz, J.; Beinicke, S.; Häntschel, J.; Goldmann, K.; Pönisch, W.; Franke, G.-N.; Vucinic, V.; et al. Prognostic Impact of Blood MN1 Copy Numbers Before Allogeneic Stem Cell Transplantation in Patients With Acute Myeloid Leukemia. HemaSphere 2019, 3, e167. [Google Scholar] [CrossRef] [PubMed]
- Lange, T.; Hubmann, M.; Burkhardt, R.; Franke, G.N.; Cross, M.; Scholz, M.; Leiblein, S.; Al-Ali, H.K.; Edelmann, J.; Thiery, J.; et al. Monitoring of WT1 expression in PB and CD34 donor chimerism of BM predicts early relapse in AML and MDS patients after hematopoietic cell transplantation with reduced-intensity conditioning. Leukemia 2011, 25, 498–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Development Core Team R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2017; Available online: https://www.R-project.org (accessed on 25 August 2021).
- Gray, R.J. A Class of K-Sample Tests for Comparing the Cumulative Incidence of a Competing Risk. Ann. Stat. 1988, 16, 1141–1154. [Google Scholar] [CrossRef]
- Becker, H.; Maharry, K.; Mrozek, K.; Volinia, S.; Eisfeld, A.-K.; Radmacher, M.; Kohlschmidt, J.; Metzeler, K.; Schwind, S.; Whitman, S.; et al. Prognostic gene mutations and distinct gene- and microRNA-expression signatures in acute myeloid leukemia with a sole trisomy 8. Leukemia 2014, 28, 1754–1758. [Google Scholar] [CrossRef] [Green Version]
- Chou, W.C.; Lei, W.C.; Ko, B.S.; Hou, H.A.; Chen, C.Y.; Tang, J.L.; Yao, M.; Tsay, W.; Wu, S.J.; Huang, S.Y.; et al. The prognostic impact and stability of Isocitrate dehydrogenase 2 mutation in adult patients with acute myeloid leukemia. Leukemia 2011, 25, 246–253. [Google Scholar] [CrossRef] [Green Version]
- Döhner, H.; Weisdorf, D.J.; Bloomfield, C.D. Acute myeloid leukemia. N. Engl. J. Med. 2015, 373, 1136–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazarevic, V.; Rosso, A.; Juliusson, G.; Antunovic, P.; Derolf, Å.R.; Deneberg, S.; Möllgård, L.; Uggla, B.; Wennström, L.; Wahlin, A.; et al. Incidence and prognostic significance of isolated trisomies in adult acute myeloid leukemia: A population-based study from the Swedish AML Registry. Eur. J. Haematol. 2017, 98, 493–500. [Google Scholar] [CrossRef]
- Schuurhuis, G.J.; Heuser, M.; Freeman, S.; Béne, M.C.; Buccisano, F.; Cloos, J.; Grimwade, D.; Haferlach, T.; Hills, R.K.; Hourigan, C.S.; et al. Minimal/measurable residual disease in AML: A consensus document from the European LeukemiaNet MRD Working Party. Blood 2018, 131, 1275–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaravaglio, P.; Guglielmelli, T.; Giugliano, E.; Marmont, F.; Audisio, E.; Gallo, E.; Saglio, G.; Rege-cambrin, G. Detection of minimal residual disease in peripheral blood stem cells from two acute myeloid leukemia patients with trisomy 8 predicts early relapse after autologous bone marrow transplantation. Cancer Genet. Cytogenet. 2002, 133, 98–101. [Google Scholar] [CrossRef]
- White, D.L.; Hutchins, C.J.; Turczynowicz, S.; Suttle, J.; Haylock, D.N.; Hughes, T.P.; Juttner, C.A.; To, L.B. Detection of minimal residual disease in an AML patient with trisomy 8 using interphase fish. Pathology 1997, 29, 289–293. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No Trisomy 8 Present (n = 578) | Trisomy 8 Present (n = 81) | p | Sole Trisomy 8
(n = 33) | Trisomy 8 and Additional Aberrations (n = 48) | p | |
|---|---|---|---|---|---|---|
| Clinical Characteristics | ||||||
| Age at diagnosis, years | 0.08 | 0.04 | ||||
| median | 58.7 | 61.9 | 65.4 | 60.4 | ||
| range | 14.3–76.1 | 19.2–76.6 | 20.8–76.5 | 19.2–71.4 | ||
| Sex, n (%) | 0.41 | 0.5 | ||||
| male | 297 (51) | 46 (57) | 17 (52) | 29 (60) | ||
| female | 281 (49) | 35 (43) | 16 (48) | 19 (40) | ||
| Disease origin, n (%) | 0.04 | 0.37 | ||||
| secondary AML | 206 (36) | 39 (48) | 18 (55) | 21 (44) | ||
| de novo AML | 372 (64) | 42 (52) | 15 (45) | 27 (56) | ||
| Hemoglobin at diagnosis, g/L | 0.06 | 0.39 | ||||
| median | 8.7 | 8.9 | 9.5 | 8.8 | ||
| range | 3.2–15.7 | 5.3–15.0 | 6.6–15 | 5.3–14.2 | ||
| Platelet count at diagnosis, × 109/L | 0.37 | 0.84 | ||||
| median | 65 | 58 | 59 | 54 | ||
| range | 1–950 | 2–305 | 8–305 | 2–218 | ||
| WBC count at diagnosis, × 109/L | 0.01 | 0.45 | ||||
| median | 6.5 | 2.5 | 2.4 | 2.5 | ||
| range | 0.1–385 | 0.6–432 | 0.7–432 | 0.6–325 | ||
| Blood blasts at diagnosis, % | 0.48 | 0.13 | ||||
| median | 20 | 22 | 42 | 19 | ||
| range | 0–97 | 0–96 | 0–89 | 0–96 | ||
| BM blasts at diagnosis, % | 0.29 | 0.42 | ||||
| median | 50 | 50 | 55 | 44 | ||
| range | 0–100 | 3–85 | 3–85 | 11–85 | ||
| BM CD34+/CD38− cells at diagnosis, % | 0.05 | 0.8 | ||||
| median | 0.7 | 1.5 | 2.3 | 1.3 | ||
| range | 0–89 | 0–44.5 | 0–28 | 0–44.5 | ||
| Genetic characteristics | ||||||
| ELN2017 genetic group, n (%) | 0.03 | <0.001 | ||||
| favorable | 115 (26) | 6 (10) | 1 (6) | 5 (12) | ||
| Intermediate | 146 (33) | 21 (36) | 13 (76) | 8 (19) | ||
| adverse | 188 (42) | 32 (54) | 3 (18) | 29 (69) | ||
| Complex karyotype, n (%) | 0.03 | <0.001 | ||||
| absent | 480 (86) | 60 (76) | 33 (100) | 27 (59) | ||
| present | 77 (14) | 19 (24) | 0 (0) | 19 (41) | ||
| Core-Binding Factor AML, n (%) | 1 | 0.14 | ||||
| absent | 535 (95) | 77 (95) | 33 (100) | 44 (92) | ||
| present | 29 (5) | 4 (5) | 0 (0) | 4 (8) | ||
| NPM1 at diagnosis, n (%) | 0.002 | 0.63 | ||||
| wild-type | 347 (76) | 54 (93) | 20 (91) | 34 (94) | ||
| mutated | 110 (24) | 4 (7) | 2 (9) | 2 (6) | ||
| FLT3-ITD at diagnosis, n (%) | 0.61 | 0.5 | ||||
| absent | 365 (79) | 48 (83) | 18 (78) | 30 (86) | ||
| present | 98 (21) | 10 (17) | 5 (22) | 5 (14) | ||
| CEBPA at diagnosis, n (%) | 0.47 | 1 | ||||
| wild-type | 341 (90) | 43 (86) | 16 (89) | 27 (84) | ||
| mutated | 40 (10) | 7 (14) | 2 (11) | 5 (16) | ||
| FLT3-TKD at diagnosis, n (%) | 0.82 | 1 | ||||
| wild-type | 387 (90) | 50 (89) | 18 (90) | 32 (89) | ||
| mutated | 43 (10) | 6 (11) | 2 (10) | 4 (11) | ||
| TET2 at diagnosis, n (%) | 1 | 0.06 | ||||
| wild-type | 84 (83) | 16 (84) | 5 (63) | 11 (100) | ||
| mutated | 17 (17) | 3 (16) | 3 (37) | 0 (0) | ||
| ASXL1 at diagnosis, n (%) | 0.29 | 0.62 | ||||
| wild-type | 106 (89) | 17 (81) | 6 (75) | 11 (85) | ||
| mutated | 13 (11) | 4 (19) | 2 (25) | 2 (15) | ||
| BCOR at diagnosis, n (%) | 0.73 | 0.04 | ||||
| wild-type | 85 (86) | 15 (83) | 4 (57) | 11 (100) | ||
| mutated | 14 (14) | 3 (17) | 3 (43) | 0 (0) | ||
| IDH1 or IDH2 at diagnosis, n (%) | 0.05 | 0.71 | ||||
| wild-type | 184 (78) | 19 (61) | 6 (55) | 13 (65) | ||
| mutated | 52 (22) | 12 (39) | 5 (45) | 7 (35) | ||
| JAK2 at diagnosis, n (%) | 0.04 | 0.02 | ||||
| wild-type | 118 (89) | 16 (73) | 4 (44) | 12 (92) | ||
| mutated | 14 (11) | 6 (27) | 5 (56) | 1 (8) | ||
| BAALC copy numbers at diagnosis | 0.08 | 0.26 | ||||
| median | 0.06 | 0.19 | 0.06 | 0.37 | ||
| range | 0.00–56.31 | 0.00–1.42 | 0.02–1.42 | 0.00–0.90 |
| No Trisomy 8 Present (n = 578) | Trisomy 8 Present (n = 81) | p | Sole Trisomy 8
(n = 33) | Trisomy 8 and Additional Aberrations (n = 48) | p | |
|---|---|---|---|---|---|---|
| Disease status at HSCT, n (%) | 0.04 | 0.09 | ||||
| CR/CRi1 | 370 (64) | 56 (69) | 22 (67) | 34 (71) | ||
| CR/CRi 2 or 3 | 102 (18) | 6 (7) | 5 (15) | 1 (2) | ||
| worse | 106 (18) | 19 (23) | 6 (18) | 13 (27) | ||
| Chemotherapy cycles prior to HSCT, n (%) | 0.79 | 0.43 | ||||
| 1 | 177 (31) | 25 (31) | 12 (36) | 13 (27) | ||
| 2 | 295 (51) | 44 (54) | 15 (45) | 29 (60) | ||
| ≥3 | 105 (18) | 12 (15) | 6 (18) | 6 (13) | ||
| Conditioning regimens, n (%) | 0.79 | 0.35 | ||||
| myeloablative | 146 (25) | 44 (54) | 8 (24) | 14 (29) | ||
| reduced-intensity | 96 (17) | 15 (19) | 4 (12) | 11 (23) | ||
| non-myeloablative | 336 (58) | 22 (27) | 21 (64) | 23 (48) | ||
| Donor match, n (%) | 0.73 | 0.33 | ||||
| HLA-matched related | 112 (17) | 14 (17) | 4 (12) | 10 (21) | ||
| HLA-matched unrelated | 350 (52) | 47 (58) | 20 (61) | 27 (56) | ||
| HLA-mismatched | 100 (15) | 18 (22) | 7 (21) | 11 (23) | ||
| haploidentical | 16 (2) | 2 (2) | 2 (6) | 0 (0) | ||
| Donor sex, n (%) | 0.87 | 0.54 | ||||
| all others | 490 (86) | 68 (85) | 27 (82) | 41 (87) | ||
| female to male | 81 (14) | 12 (15) | 6 (18) | 6 (13) | ||
| Acute GvHD ≥ grade 2, n (%) | 0.17 | 0.63 | ||||
| absent | 373 (74) | 49 (65) | 19 (61) | 30 (68) | ||
| present | 133 (26) | 26 (35) | 12 (39) | 14 (32) | ||
| Chronic GvHD, n (%) | 0.07 | 0.88 | ||||
| absent | 173 (45) | 19 (36) | 8 (38) | 11 (34) | ||
| limited | 48 (13) | 14 (36) | 6 (29) | 8 (25) | ||
| extensive | 160 (42) | 19 (38) | 7 (33) | 13 (41) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Backhaus, D.; Jentzsch, M.; Bischof, L.; Brauer, D.; Wilhelm, C.; Schulz, J.; Franke, G.-N.; Pönisch, W.; Vucinic, V.; Platzbecker, U.; et al. Risk Stratification, Measurable Residual Disease, and Outcomes of AML Patients with a Trisomy 8 Undergoing Allogeneic Hematopoietic Stem Cell Transplantation. Cancers 2021, 13, 5679. https://doi.org/10.3390/cancers13225679
Backhaus D, Jentzsch M, Bischof L, Brauer D, Wilhelm C, Schulz J, Franke G-N, Pönisch W, Vucinic V, Platzbecker U, et al. Risk Stratification, Measurable Residual Disease, and Outcomes of AML Patients with a Trisomy 8 Undergoing Allogeneic Hematopoietic Stem Cell Transplantation. Cancers. 2021; 13(22):5679. https://doi.org/10.3390/cancers13225679
Chicago/Turabian StyleBackhaus, Donata, Madlen Jentzsch, Lara Bischof, Dominic Brauer, Christina Wilhelm, Julia Schulz, Georg-Nikolaus Franke, Wolfram Pönisch, Vladan Vucinic, Uwe Platzbecker, and et al. 2021. "Risk Stratification, Measurable Residual Disease, and Outcomes of AML Patients with a Trisomy 8 Undergoing Allogeneic Hematopoietic Stem Cell Transplantation" Cancers 13, no. 22: 5679. https://doi.org/10.3390/cancers13225679