
Use of Azacitidine or Decitabine for the Up-Front Setting in Acute Myeloid Leukaemia: A Systematic Review and Meta-Analysis

 , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Sources and Search Strategies
2.3. Study Selection
2.4. Data Extraction and List of Variables Included
- Study (first author, year)
- Study design: phase I, II or III clinical trial, retrospective, prospective
- Intervention (dose, schedule): azacitidine or decitabine
- Comparison (description): best supportive care, low doses of cytarabine
- Patients (N)
- Age (years): median and range
- Male (%)
- ECOG 0/1, 2, ≥3 (%): Eastern Cooperative Oncology Group (ECOG) scale
- AML type (%): de novo or secondary
- Cytogenetics (%): favourable, intermediate, adverse
- BM blasts (median %): bone marrow blasts
- WBC count (109/L median): white blood cell count
- CR (%): complete remission
- CCR (%): composite complete remission rate (CR + CRi)
- PR (%): partial response
- ORR (%): overall response rate (CR + Cri + PR)
- Median OS (months): overall survival
- Early mortality (first 30 and 60 days since randomisation) (%)
- Mortality (%)
2.5. Definitions
2.6. Methodologic Quality and Risk of Bias
2.7. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
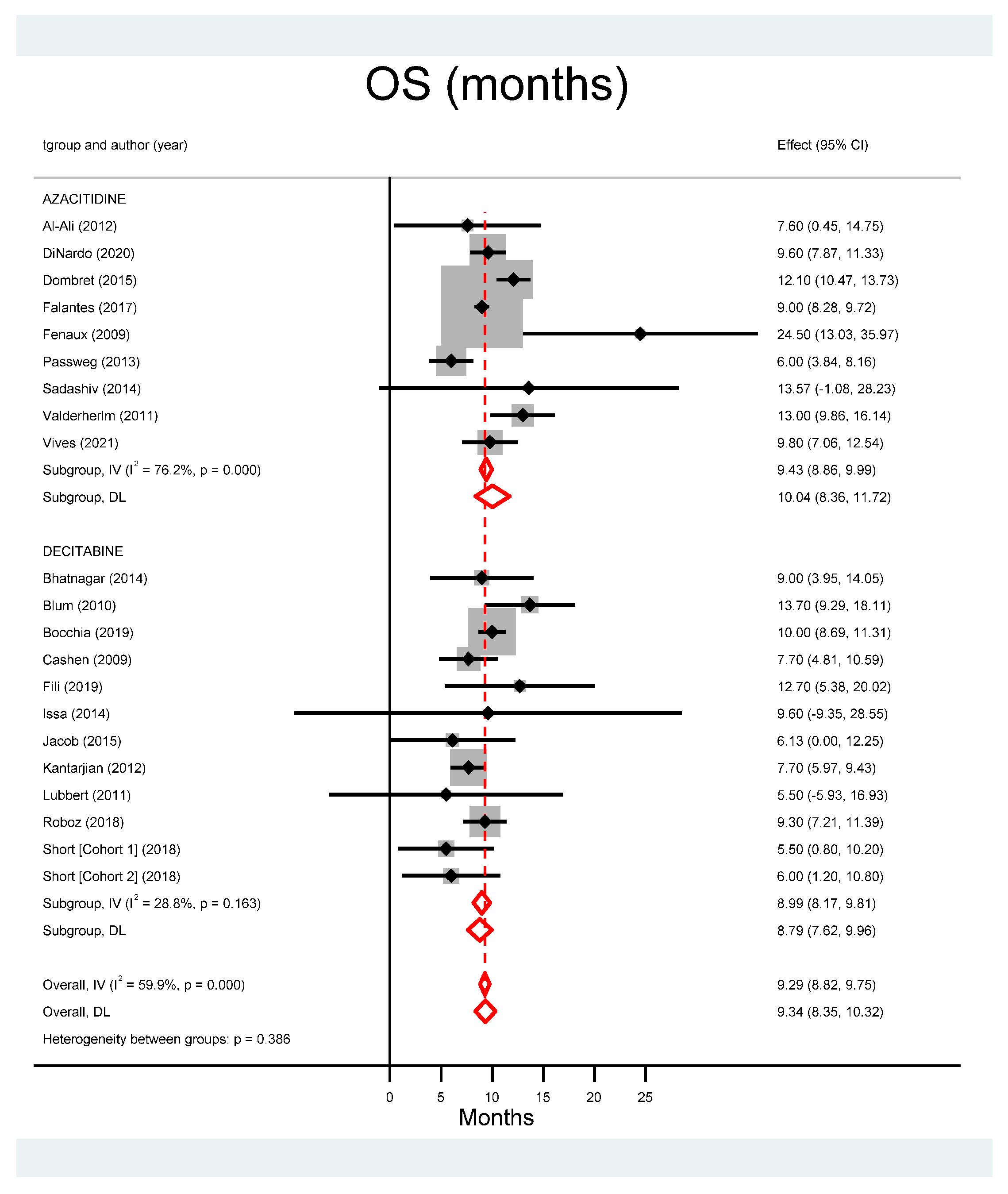
3.3. Outcomes
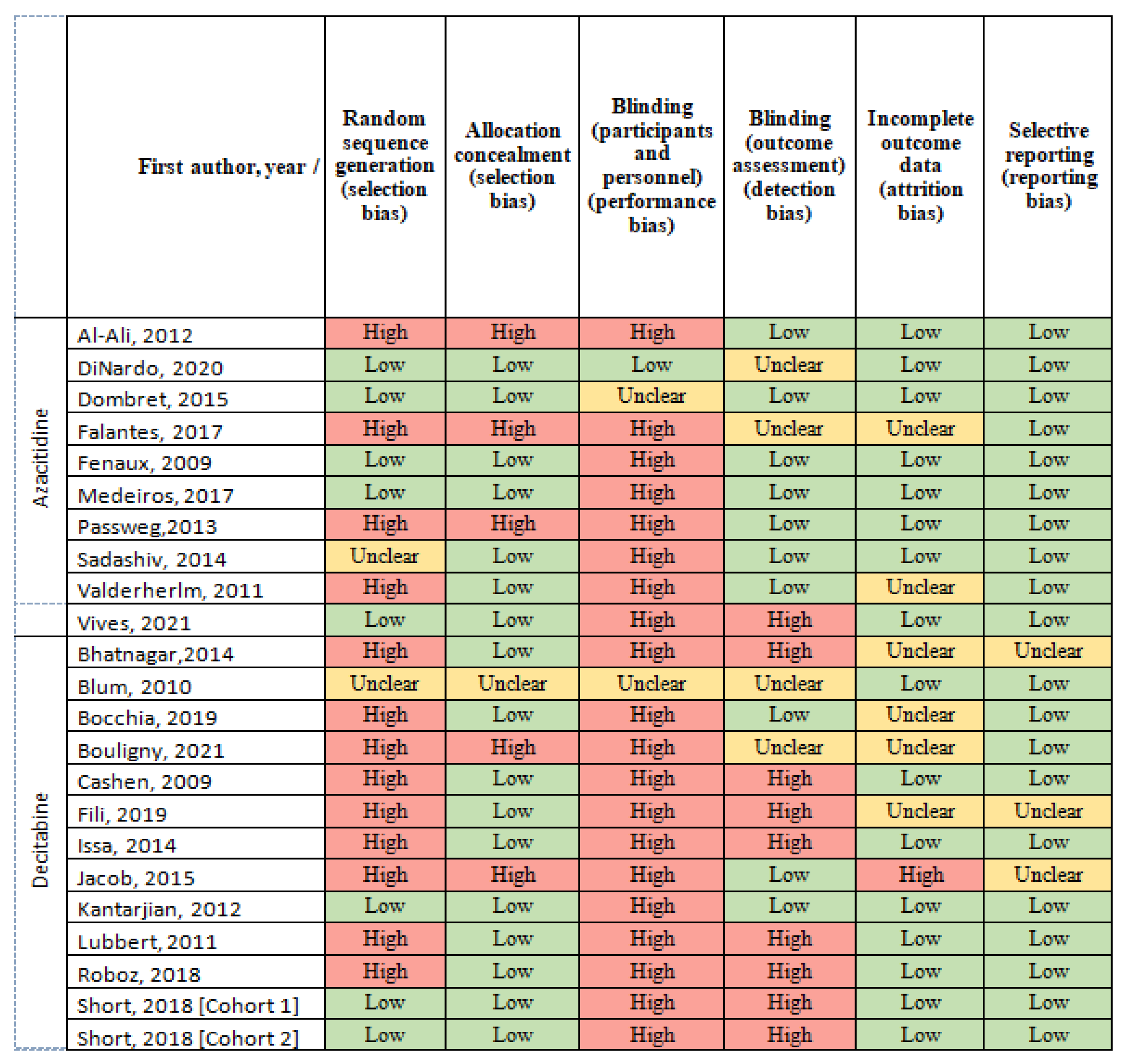
3.4. Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stone, A.; Zukerman, T.; Flaishon, L.; Ben Yakar, R.; Rowe, J.M. Efficacy outcomes in the treatment of older or medically unfit patients with acute myeloid leukaemia: A systematic review and meta-analysis. Leuk. Res. 2019, 82, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Juliusson, G.; Antunovic, P.; Derolf, A.; Lehmann, S.; Möllgård, L.; Stockelberg, D.; Tidefelt, U.; Wahlin, A.; Hoglund, M. Age and acute myeloid leukemia: Real world data on decision to treat and outcomes from the Swedish Acute Leukemia Registry. Blood 2009, 113, 4179–4187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juliusson, G.; Lazarevic, V.; Hörstedt, A.-S.; Hagberg, O.; Hoglund, M. Acute myeloid leukemia in the real world: Why population-based registries are needed. Blood 2012, 119, 3890–3899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visser, O.; Trama, A.; Maynadié, M.; Stiller, C.; Marcos-Gragera, R.; De Angelis, R.; Mallone, S.; Tereanu, C.; Allemani, C.; Ricardi, U.; et al. Incidence, survival and prevalence of myeloid malignancies in Europe. Eur. J. Cancer 2012, 48, 3257–3266. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Andersson, T.M.-L.; Rachet, B.; Björkholm, M.; Lambert, P.C. Survival and cure of acute myeloid leukaemia in England, 1971–2006: A population-based study. Br. J. Haematol. 2013, 162, 509–516. [Google Scholar] [CrossRef]
- Martínez-Cuadrón, D.; Serrano, J.; Gil, C.; Tormo, M.; Martínez-Sánchez, P.; Pérez-Simón, J.A.; García-Boyero, R.; Rodríguez-Medina, C.; López-Pavía, M.; Benavente, C.; et al. Evolving treatment patterns and outcomes in older patients (≥60 years) with AML: Changing everything to change nothing? Leukemia 2021, 35, 1571–1585. [Google Scholar] [CrossRef]
- Meyers, J.; Yu, Y.; Kaye, J.A.; Davis, K.L. Medicare Fee-for-Service Enrollees with Primary Acute Myeloid Leukemia: An Analysis of Treatment Patterns, Survival, and Healthcare Resource Utilization and Costs. Appl. Health Econ. Health Policy 2013, 11, 275–286. [Google Scholar] [CrossRef]
- Erba, H.P. Finding the optimal combination therapy for the treatment of newly diagnosed AML in older patients unfit for intensive therapy. Leuk. Res. 2015, 39, 183–191. [Google Scholar] [CrossRef] [Green Version]
- Buchner, T.; Berdel, W.E.; Haferlach, C.; Haferlach, T.; Schnittger, S.; Müller-Tidow, C.; Braess, J.; Spiekermann, K.; Kienast, J.; Staib, P.; et al. Age-Related Risk Profile and Chemotherapy Dose Response in Acute Myeloid Leukemia: A Study by the German Acute Myeloid Leukemia Cooperative Group. J. Clin. Oncol. 2009, 27, 61–69. [Google Scholar] [CrossRef] [Green Version]
- Jabbour, E.; Kantarjian, H.; O’Brien, S.; Cortes, J.; Giles, F.; Faderl, S.; Garcia-Manero, G.; Wierda, W.; Pierce, S.; Shan, J.; et al. Results of Intensive Chemotherapy in 998 Patients Aged 65 Years or Older with Acute Myeloid Leukemia or High-Risk Myelodysplastic Syndrome—Predictive Prognostic Models for Outcome. Blood 2005, 106, 1846. [Google Scholar] [CrossRef]
- Grimwade, D.; Walker, H.; Harrison, G.; Oliver, F.; Chatters, S.; Harrison, C.; Wheatley, K.; Burnett, A.K.; Goldstone, A.H. The predictive value of hierarchical cytogenetic classification in older adults with acute myeloid leukemia (AML): Analysis of 1065 patients entered into the United Kingdom Medical Research Council AML11 trial. Blood 2001, 98, 1312–1320. [Google Scholar] [CrossRef] [Green Version]
- Farag, S.S.; Archer, K.J.; Mrózek, K.; Ruppert, A.S.; Carroll, A.J.; Vardiman, J.W.; Pettenati, M.J.; Baer, M.R.; Qumsiyeh, M.B.; Koduru, P.R.; et al. Pretreatment cytogenetics add to other prognostic factors predicting complete remission and long-term outcome in patients 60 years of age or older with acute myeloid leukemia: Results from Cancer and Leukemia Group B 8461. Blood 2006, 108, 63–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yun, S.; Vincelette, N.D.; Abraham, I.; Robertson, K.; Fernandez-Zapico, M.E.; Patnaik, M.M. Targeting epigenetic pathways in acute myeloid leukemia and myelodysplastic syndrome: A systematic review of hypomethylating agents trials. Clin. Epigenetics 2016, 8, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyko, F.; Brown, R. DNA Methyltransferase Inhibitors and the Development of Epigenetic Cancer Therapies. J. Natl. Cancer Inst. 2005, 97, 1498–1506. [Google Scholar] [CrossRef] [PubMed]
- Faderl, S.; Kantarjian, H.M. Clinical Manifestations and Treatment of Acute Myeloid Leukemia. Hematology 2018, 924–943. [Google Scholar] [CrossRef]
- Kantarjian, H.M.; Thomas, X.G.; Dmoszynska, A.; Wierzbowska, A.; Mazur, G.; Mayer, J.; Gau, J.-P.; Chou, W.-C.; Buckstein, R.; Cermak, J.; et al. Multicenter, Randomized, Open-Label, Phase III Trial of Decitabine Versus Patient Choice, With Physician Advice, of Either Supportive Care or Low-Dose Cytarabine for the Treatment of Older Patients With Newly Diagnosed Acute Myeloid Leukemia. J. Clin. Oncol. 2012, 30, 2670–2677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dombret, H.; Seymour, J.F.; Butrym, A.; Wierzbowska, A.; Selleslag, D.; Jang, J.H.; Kumar, R.; Cavenagh, J.; Schuh, A.C.; Candoni, A.; et al. International phase 3 study of azacitidine vs conventional care regimens in older patients with newly diagnosed AML with >30% blasts. Blood 2015, 126, 291–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blum, W.; Garzon, R.; Klisovic, R.B.; Schwind, S.; Walker, A.; Geyer, S.; Liu, S.; Havelange, V.; Becker, H.; Schaaf, L.; et al. Clinical response and miR-29b predictive significance in older AML patients treated with a 10-day schedule of decitabine. Proc. Natl. Acad. Sci. USA 2010, 107, 7473–7478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Short, N.J.; Kantarjian, H.M.; Loghavi, S.; Huang, X.; Qiao, W.; Borthakur, G.; Kadia, T.M.; Daver, N.; Ohanian, M.; Dinardo, C.D.; et al. Treatment with a 5-day versus a 10-day schedule of decitabine in older patients with newly diagnosed acute myeloid leukaemia: A randomised phase 2 trial. Lancet Haematol. 2018, 6, e29–e37. [Google Scholar] [CrossRef]
- Al-Ali, H.K.; Jaekel, N.; Junghanss, C.; Maschmeyer, G.; Krahl, R.; Cross, M.; Hoppe, G.; Niederwieser, D. Azacitidine in patients with acute myeloid leukemia medically unfit for or resistant to chemotherapy: A multicenter phase I/II study. Leuk. Lymphoma 2011, 53, 110–117. [Google Scholar] [CrossRef]
- Passweg, J.R.; Pabst, T.; Blum, S.; Bargetzi, M.; Li, Q.; Heim, D.; Stussi, G.; Gregor, M.; Leoncini, L.; Meyer-Monard, S.; et al. Azacytidine for acute myeloid leukemia in elderly or frail patients: A phase II trial (SAKK 30/07). Leuk. Lymphoma 2014, 55, 87–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. The Cochrane Collaboration. 2011. Available online: https://handbook-5-1.cochrane.org/ (accessed on 20 December 2019).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Dinardo, C.D.; Jonas, B.A.; Pullarkat, V.; Thirman, M.J.; Garcia, J.S.; Wei, A.H.; Konopleva, M.; Döhner, H.; Letai, A.; Fenaux, P.; et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N. Engl. J. Med. 2020, 383, 617–629. [Google Scholar] [CrossRef]
- Falantes, J.; Pleyer, L.; Thépot, S.; Almeida, A.M.; Maurillo, L.; Martínez-Robles, V.; Stauder, R.; Itzykson, R.; Pinto, R.; Venditti, A.; et al. Real life experience with frontline azacitidine in a large series of older adults with acute myeloid leukemia stratified by MRC/LRF score: Results from the expanded international E-ALMA series (E-ALMA+). Leuk. Lymphoma 2017, 59, 1113–1120. [Google Scholar] [CrossRef]
- Fenaux, P.; Mufti, G.J.; Hellström-Lindberg, E.; Santini, V.; Gattermann, N.; Germing, U.; Sanz, G.; List, A.F.; Gore, S.; Seymour, J.F.; et al. Azacitidine Prolongs Overall Survival Compared With Conventional Care Regimens in Elderly Patients With Low Bone Marrow Blast Count Acute Myeloid Leukemia. J. Clin. Oncol. 2010, 28, 562–569. [Google Scholar] [CrossRef]
- Medeiros, B.C.; McCaul, K.; Kambhampati, S.; Pollyea, D.A.; Kumar, R.; Silverman, L.R.; Kew, A.; Saini, L.; Beach, C.L.; Vij, R.; et al. Randomized study of continuous high-dose lenalidomide, sequential azacitidine and lenalidomide, or azacitidine in persons 65 years and over with newly-diagnosed acute myeloid leukemia. Haematologica 2017, 103, 101–106. [Google Scholar] [CrossRef] [Green Version]
- Sadashiv, S.K.; Hilton, C.; Khan, C.; Rossetti, J.M.; Benjamin, H.L.; Fazal, S.; Sahovic, E.; Shadduck, R.K.; Lister, J. Efficacy and tolerability of treatment with azacitidine for 5 days in elderly patients with acute myeloid leukemia. Cancer Med. 2014, 3, 1570–1578. [Google Scholar] [CrossRef]
- Van der Helm, L.; Alhan, C.; Wijermans, P.W.; van Marwijk Kooy, M.; Schaafsma, R.; Biemond, B.J.; Beeker, A.; Hoogendoorn, M.; van Rees, B.; de Weerdt, O.; et al. Platelet doubling after the first azacitidine cycle is a promising predictor for response in myelodysplastic syndromes (MDS), chronic myelomonocytic leukaemia (CMML) and acute myeloid leukaemia (AML) patients in the Dutch azacitidine compassionate named p: Azacitidine and Response Predictors in MDS, CMML and AML. Br. J. Haematol. 2011, 155, 599–606. [Google Scholar]
- Vives, S.; Martínez-Cuadrón, D.; Burgues, J.B.; Algarra, L.; Tormo, M.; Martínez-Sánchez, M.P.; Serrano, J.; Herrera, P.; Ramos, F.; Salamero, O.; et al. A phase 3 trial of azacitidine versus a semi-intensive fludarabine and cytarabine schedule in older patients with untreated acute myeloid leukemia. Cancer 2021, 127, 2003–2014. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, B.; Duong, V.H.; Gourdin, T.S.; Tidwell, M.L.; Chen, C.; Ning, Y.; Emadi, A.; Sausville, E.A.; Baer, M.R. Ten-day decitabine as initial therapy for newly diagnosed patients with acute myeloid leukemia unfit for intensive chemotherapy. Leuk. Lymphoma 2014, 55, 1533–1537. [Google Scholar] [CrossRef]
- Bocchia, M.; Candoni, A.; Borlenghi, E.; Defina, M.; Filì, C.; Cattaneo, C.; Sammartano, V.; Fanin, R.; Sciumè, M.; Sicuranza, A.; et al. Real-world experience with decitabine as a first-line treatment in 306 elderly acute myeloid leukaemia patients unfit for intensive chemotherapy. Hematol. Oncol. 2019, 37, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Bouligny, I.M.; Mehta, V.; Isom, S.; Ellis, L.R.; Bhave, R.R.; Howard, D.S.; Lyerly, S.; Manuel, M.; Dralle, S.; Powell, B.L.; et al. Efficacy of 10-day decitabine in acute myeloid leukemia. Leuk. Res. 2021, 103, 106524. [Google Scholar] [CrossRef] [PubMed]
- Cashen, A.F.; Schiller, G.J.; O’Donnell, M.R.; DiPersio, J.F. Multicenter, Phase II Study of Decitabine for the First-Line Treatment of Older Patients With Acute Myeloid Leukemia. J. Clin. Oncol. 2010, 28, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Filì, C.; Candoni, A.; Zannier, M.E.; Olivieri, J.; Imbergamo, S.; Caizzi, M.; Nadali, G.; Di Bona, E.; Ermacora, A.; Gottardi, M.; et al. Efficacy and toxicity of Decitabine in patients with acute myeloid leukemia (AML): A multicenter real-world experience. Leuk. Res. 2019, 76, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Issa, J.-P.J.; Garcia-Manero, G.; Giles, F.J.; Mannari, R.; Thomas, D.; Faderl, S.; Bayar, E.; Lyons, J.; Rosenfeld, C.S.; Cortes, J.; et al. Phase 1 study of low-dose prolonged exposure schedules of the hypomethylating agent 5-aza-2′-deoxycytidine (decitabine) in hematopoietic malignancies. Blood 2004, 103, 1635–1640. [Google Scholar] [CrossRef] [Green Version]
- Jacob, L.A.; Aparna, S.; Lakshmaiah, K.C.; Lokanatha, D.; Babu, G.; Babu, S.; Appachu, S. Decitabine Compared with Low-Dose Cytarabine for the Treatment of Older Patients with Newly Diagnosed Acute Myeloid Leukemia: A Pilot Study of Safety, Efficacy, and Cost-Effectiveness. Adv. Hematol. 2015, 2015, 167029. [Google Scholar] [CrossRef] [Green Version]
- Lübbert, M.; Rüter, B.H.; Claus, R.; Schmoor, C.; Schmid, M.; Germing, U.; Kuendgen, A.; Rethwisch, V.; Ganser, A.; Platzbecker, U.; et al. A multicenter phase II trial of decitabine as first-line treatment for older patients with acute myeloid leukemia judged unfit for induction chemotherapy. Haematologica 2011, 97, 393–401. [Google Scholar] [CrossRef]
- Roboz, G.J.; Mandrekar, S.J.; Desai, P.; Laumann, K.; Walker, A.R.; Wang, E.S.; Kolitz, J.E.; Powell, B.L.; Attar, E.C.; Stock, W.; et al. Randomized trial of 10 days of decitabine ± bortezomib in untreated older patients with AML: CALGB 11002 (Alliance). Blood Adv. 2018, 2, 3608–3617. [Google Scholar] [CrossRef] [Green Version]
- Zeidan, A.M.; Wang, R.; Wang, X.; Shallis, R.M.; Podoltsev, N.A.; Bewersdorf, J.P.; Huntington, S.F.; Neparidze, N.; Giri, S.; Gore, S.D.; et al. Clinical outcomes of older patients with AML receiving hypomethylating agents: A large population-based study in the United States. Blood Adv. 2020, 4, 2192–2201. [Google Scholar] [CrossRef] [PubMed]
- Wen, B.; You, W.; Yang, S.; Du, X. Indirect comparison of azacitidine and decitabine for the therapy of elderly patients with acute myeloid leukemia: A systematic review and network meta-analysis. Exp. Hematol. Oncol. 2020, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, V.; Schnittger, S.; Kohlmann, A.; Eder, C.; Roller, A.; Dicker, F.; Schmid, C.; Wendtner, C.-M.; Staib, P.; Serve, H.; et al. A novel hierarchical prognostic model of AML solely based on molecular mutations. Blood 2012, 120, 2963–2972. [Google Scholar] [CrossRef]
- Rücker, F.G.; Schlenk, R.F.; Bullinger, L.; Kayser, S.; Teleanu, V.; Kett, H.; Habdank, M.; Kugler, C.M.; Holzmann, K.; Gaidzik, V.I.; et al. TP53 alterations in acute myeloid leukemia with complex karyotype correlate with specific copy number alterations, monosomal karyotype, and dismal outcome. Blood 2012, 119, 2114–2121. [Google Scholar] [CrossRef]
- Bories, P.; Prade, N.; Lagarde, S.; Cabarrou, B.; Largeaud, L.; Plenecassagnes, J.; Luquet, I.; De Mas, V.; Filleron, T.; Cassou, M.; et al. Impact of TP53 mutations in acute myeloid leukemia patients treated with azacitidine. PLoS ONE 2020, 15, e0238795. [Google Scholar] [CrossRef]
- Welch, J.S.; Petti, A.A.; Miller, C.; Fronick, C.C.; O’Laughlin, M.; Fulton, R.S.; Wilson, R.K.; Baty, J.D.; Duncavage, E.J.; Tandon, B.; et al. TP53 and Decitabine in Acute Myeloid Leukemia and Myelodysplastic Syndromes. N. Engl. J. Med. 2016, 375, 2023–2036. [Google Scholar] [CrossRef]
- Aldoss, I.; Zhang, J.; Pillai, R.; Shouse, G.; Sanchez, J.F.; Mei, M.; Nakamura, R.; Stein, A.S.; Forman, S.J.; Marcucci, G.; et al. Venetoclax and hypomethylating agents in TP53 -mutated acute myeloid leukaemia. Br. J. Haematol. 2019, 187, e45–e48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinardo, C.D.; Pratz, K.; Pullarkat, V.; Jonas, B.; Arellano, M.; Becker, P.S.; Frankfurt, O.; Konopleva, M.; Wei, A.H.; Kantarjian, H.M.; et al. Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood 2019, 133, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Pollyea, D.A.; Pratz, K.; Letai, A.; Jonas, B.A.; Wei, A.H.; Pullarkat, V.; Konopleva, M.; Thirman, M.J.; Arellano, M.; Becker, P.S.; et al. Venetoclax with azacitidine or decitabine in patients with newly diagnosed acute myeloid leukemia: Long term follow-up from a phase 1b study. Am. J. Hematol. 2020, 96, 208–217. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Study (First Author, Year) | Study Design | Intervention | Comparison | Patients (N) | Age (Years) | Male (%) | ECOG 0/1, 2, ≥3 | AML Type, DN, S (%) | Cytogenetics F, I, A (%) | NPM1 (M, W, NA) (%) | FLT3 (M, W, NA) (%) | BM Blasts (%) | WBC Count (109/L) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Azacitidine | Al-Ali, 2012 [20] | Phase I/II | 75 mg/m2/day SC for 5 days every 4 weeks | NA | 20 | 78 (64–84) | 55 | 40, 60 | 75, 25 | 15, 75, 10 | 15, 75, 10 | 44 (10–90) | 3.4 (0.8–187.3) | |
| DiNardo, 2020 [26] | Phase III | 75 mg/m2/day SC for 7 days every 4 weeks | Aza + Ven | 145 | 76 (60–90) | 60 | 56.44 | 76, 24 | 0, 61, 39 | 12, 47, 41 | 15, 59, 26 | |||
| Dombret, 2015 [17] | Phase III | 75 mg/m2/day SC for 7 days every 4 weeks | Conventional care regimen | 241 | 75 (64–91) | 57.7 | 77.2; 22.8 | 80, 20 | 0, 65, 35 | 70 (2, 100) | 3.1 (0–33) | |||
| Falantes, 2017 [27] | Retrospective | 75 mg/m2/day SC for 7 days every 4 weeks | NA | 710 | 75 (60–93) | 63.1 | 65; 27.7 | 44, 56 | 1.5; 53.1; 31.3 | 38 (1–98) | 2.9 (0.1–190) | |||
| Fenaux, 2009 [28] | Phase III | 75 mg/m2/day SC for 7 days every 4 weeks | Conventional care regimen | 55 | 70 (52–80) | 67.3 | 92.7; 7.3 | 34.5; 69.1; 25.5 | 23 (20–34) | |||||
| Medeiros, 2017 [29] | Phase II | 75 mg/m2/day SC for 7 days every 4 weeks | Lenalidomide | 34 | 75 (66–85) | 55.9 | 79.4; 17.6 | 85.3; 14.7 | 50 | 34 (14–70) | ||||
| Passweg, 2013 [21] | Phase III | 100 mg/m2/day SC for 5 days every 4 weeks | NA | 45 | 74 (55–86) | 60 | ||||||||
| Sadashiv, 2014 [30] | Phase II | 100 mg/m2/day SC for 5 days every 4 weeks | NA | 15 | 74 (64–82) | 60 | 60; 33, 3 | 44 (29–92) | 2.9 (1.2–43.3) | |||||
| van der Herlm, 2011 [31] | Retrospective | 75 mg/m2/day SC for 7 days every 4 weeks | NA | 31 | 71 (40–84) | 74 | 0; 68; 32 | |||||||
| Vives, 2021 [32] | Phase III | 75 mg/m2/day subcutaneously for 7 days every 4 weeks | FLUGA | 142 | 74 (65–90) | 60 | 75.25 | 79; 21 | 52 (10–99) | 4.5 (0.6–235.5) | ||||
| Decitabine | Bhatnagar, 2014 [33] | Retrospective | 20 mg/m2/day IV for 10 days every 4 weeks | NA | 45 | 74 (52–87) | 56 | 58; 42 | 2; 42; 53 | 4; 49; 47 | 13; 62; 24 | 49 (18–96) | 7.7 (0.8–117.2) | |
| Blum, 2010 [18] | Phase II | 20 mg/m2/day IV for 10 days every 4 weeks | NA | 53 | 74 (60–85) | 64 | 52 (20–92) | 2.7 (0.4–150.0) | ||||||
| Bocchia, 2019 [34] | Retrospective | 20 mg/m2/day IV for 5 days every 4 weeks | NA | 306 | 75 (65–90) | 59.5; 40.5 | 3.6; 50.3; 30.4 | 4.5 (1.8–17.1) | ||||||
| Bouligny, 2021 [35] | Prospective | 20 mg/m2/day IV for 10 days every 4 weeks | NA | 72 | 74 (44–88) | 68 | 4.2; 44.4; 51.4 | 3.0 | ||||||
| Cashen, 2009 [36] | Phase II | 20 mg/m2/day IV for 5 days every 4 weeks | NA | 55 | 74 (61–87) | 50 | 82; 18 | 55; 42 | 53; 45 | 50 (0–99) | 2.7 (1–111) | |||
| Fili, 2019 [37] | Retrospective | 20 mg/m2/day IV for 5 days every 4 weeks | NA | 75 | 74 | 53.3 | 88; 12 | 56, 44 | 11.4; 88.6 | 3.4 (0.8–25.5) | ||||
| Issa, 2004 [38] | Phase II | 20 mg/m2/day IV for 5 days every 4 weeks | Decitabine + valproic acid | 62 | 70 (38–83) | |||||||||
| Jacob, 2015 [39] | Prospective | 20 mg/m2/day IV for 5 days every 4 weeks | LDC | 15 | 65 (60–80) | 80 | 53.3; 46.7 | 87, 13 | 40 | |||||
| Kantarjian, 2012 [16] | Phase III | 20 mg/m2/day IV for 5 days every 4 weeks | TC | 242 | 73.0 (64.0–89.0) | 56.6 | 76; 24 | 64; 36 | 63.1; 36.1 | 3.10 (0.3–127.0) | ||||
| Lubbert, 2011 [40] | Phase II | 135 mg/m2 total dose infused IV over 72 h every 6 weeks | NA | 227 | 72 (56–86) | 61.2 | 77; 22.1; 0.9 | 7.3; 92.6; | 7.9; 89 | 56 (10–100) | 4.4 (0.5–241) | |||
| Roboz, 2018 [41] | Phase II | 20 mg/m2/day IV for 10 days every 4 weeks | Decitabine + bortezomib | 82 | 72.4 (60.7–92.3) | 62.2 | 76.8; 19.5; 3.7 | 69.5; 30.5 | 28.2; 26.8; 45.1 | 13.3 (0.4–212.7) | ||||
| Short, 2018 (cohort 1) [19] | Phase II | 20 mg/m2/day IV for 5 days every 4 weeks | NA | 28 | 77 (70–80) | 64; 36 | 54; 46 | 4; 96 | 8; 92 | 40 (29–68) | 2.0 (1.5–3.9) | |||
| Short, 2018 (cohort 2) [19] | Phase II | 20 mg/m2/day IV for 10 days every 4 weeks | NA | 43 | 78 (69–82) | 70; 30 | 58; 42 | 19; 81 | 5; 95 | 46 (25–64) | 3.2 (1.9–10.6) |
| Variable | Study (First Author, Year) | CR (%) | CCR (%) | PR (%) | ORR (%) | Median OS (Months) | 30-Day Mortality (%) | 60-Day Mortality (%) | Mortality (%) |
|---|---|---|---|---|---|---|---|---|---|
| Azacitidine | Al-Ali, 2012 [20] | 10 | 15 | 50 | 7.7 (0.2–14.8) | 61 | |||
| DiNardo, 2020 [26] | 17.9 | 28.3 | 9.6 (7.4–12.7) | 6 | |||||
| Dombret, 2015 [17] | 19.5 | 27.8 | 1,2 | 48.5 | 12,1 (9.2–14.2) | 6.6 | 16.2 | 49.3 | |
| Falantes, 2017 [27] | 35.5 | 9,0 (8.8–11) | 60.8 | ||||||
| Fenaux, 2009 [28] | 18 | 24,5 (14.6–38) | |||||||
| Medeiros, 2017 [29] | 17.6 | 41.2 | 5.9 | 8.8 | 48 | ||||
| Passweg, 2013 [21] | 17.8 | 0 | 17.8 | 6 (3.4–7.8) | 18 | 75.6 | |||
| Sadashiv, 2014 [30] | 20 | 13 | 47 | 11.8 (0.4–30.3) | |||||
| van der Herlm, 2011 [31] | 16 | 23 | 3 | 26 | 13.0 (9.8–16.2) | ||||
| Vives, 2021 [32] | 9 | 13 | 28 | 50 | 9.8 (5.6–14) | 53 | |||
| Decitabine | Bhatnagar, 2014 [33] | 31 | 42 | 9.0 (3.9–14.2) | 4 | 61 | |||
| Blum, 2010 [18] | 47 | 64 | 13.7(9–18) | 15 | |||||
| Bocchia, 2019 [34] | 23.2 | 14.7 | 10.5 | 48.4 | 10.0 (7.9–11.9) | 77.8 | |||
| Bouligny, 2021 [35] | 16.7 | 36.1 | 36.1 | 5.6 | 19.4 | ||||
| Cashen, 2009 [36] | 24 | 26 | 7.7 (5.7–11.6) | 7 | |||||
| Fili, 2019 [37] | 31 | 11 | 42 | 12.7 (0.1–22.5) | 37 | ||||
| Issa, 2004 [38] | 33 | 9.6 (1–59.0) | |||||||
| Jacob, 2015 [39] | 5.5 (0.5–13) | ||||||||
| Kantarjian, 2012 [16] | 15.7 | 25.6 | 2.5 | 43.8 | 7.7 (6.2–9.2) | 9 | 19.7 | ||
| Lubbert, 2011 [40] | 13.21 | 12.77 | 25.98 | 5.5 (1–36.0) | 72 | ||||
| Roboz, 2018 [41] | 39 | 9.3 (5.8–12.2) | |||||||
| Short, 2018 (cohort 1) [19] | 29 | 4 | 0 | 43 | 5.5 (2.1–11.7) | 4 | 21 | ||
| Short, 2018 (cohort 2) [19] | 30 | 5 | 10.5 | 40 | 6.0 (1.9–11.7) | 9 | 25 |
| Drug | CR %, 95% CI | ORR %, 95% CI | 1-Year Mortality %, 95% CI | OS (Months) 95% CI |
|---|---|---|---|---|
| Azacitidine | 16% (12–20) | 41% (32–50) | 54% (47–61) | 10.83 (9.07–12.59) |
| (75 mg/m2, 7d) | I2 = 54.41% | I2 = 85.10% | I2 = 75.71% | |
| Decitabine (20mg/m2, 5d) | 24% (18–30) | 46% (42–50) | 72% (67–76) | 8.46 (7.00–9.93) |
| I2 = 63.54% | I2 = 0% | |||
| p-value | 0.025 | 0.327 | <0.001 | 0.138 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saiz-Rodríguez, M.; Labrador, J.; Cuevas, B.; Martínez-Cuadrón, D.; Campuzano, V.; Alcaraz, R.; Cano, I.; Sanz, M.A.; Montesinos, P. Use of Azacitidine or Decitabine for the Up-Front Setting in Acute Myeloid Leukaemia: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 5677. https://doi.org/10.3390/cancers13225677
Saiz-Rodríguez M, Labrador J, Cuevas B, Martínez-Cuadrón D, Campuzano V, Alcaraz R, Cano I, Sanz MA, Montesinos P. Use of Azacitidine or Decitabine for the Up-Front Setting in Acute Myeloid Leukaemia: A Systematic Review and Meta-Analysis. Cancers. 2021; 13(22):5677. https://doi.org/10.3390/cancers13225677
Chicago/Turabian StyleSaiz-Rodríguez, Miriam, Jorge Labrador, Beatriz Cuevas, David Martínez-Cuadrón, Verónica Campuzano, Raquel Alcaraz, Isabel Cano, Miguel A. Sanz, and Pau Montesinos. 2021. "Use of Azacitidine or Decitabine for the Up-Front Setting in Acute Myeloid Leukaemia: A Systematic Review and Meta-Analysis" Cancers 13, no. 22: 5677. https://doi.org/10.3390/cancers13225677