
Risk, Characteristics and Biomarkers of Cytokine Release Syndrome in Patients with Relapsed/Refractory AML or MDS Treated with CD3xCD123 Bispecific Antibody APVO436

 ,
, 
 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Investigational Medicinal Product
2.2. Study Design and Patients
2.3. Study Conduct
2.4. Ethics Statement and Study Approval
2.5. Grading and Management of Cytokine Release Syndrome (CRS)
2.6. Measurement of Serum Cytokine Levels and Flow Cytometry
2.7. Statistical Analyses
3. Results
3.1. Cytokine Release Syndrome and Its Predictors
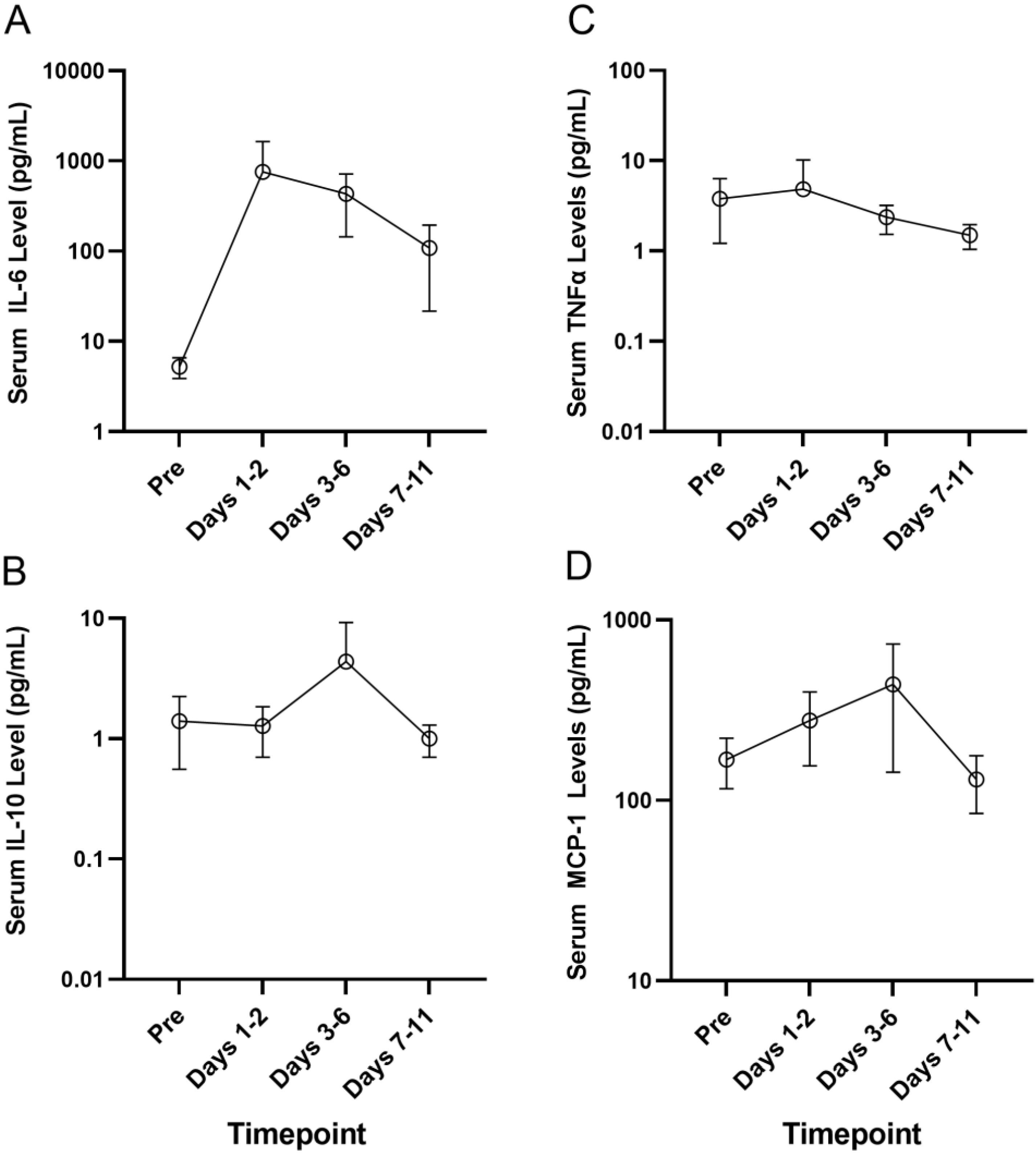
3.2. Serum Cytokine Profiles of Patients Who Developed CRS
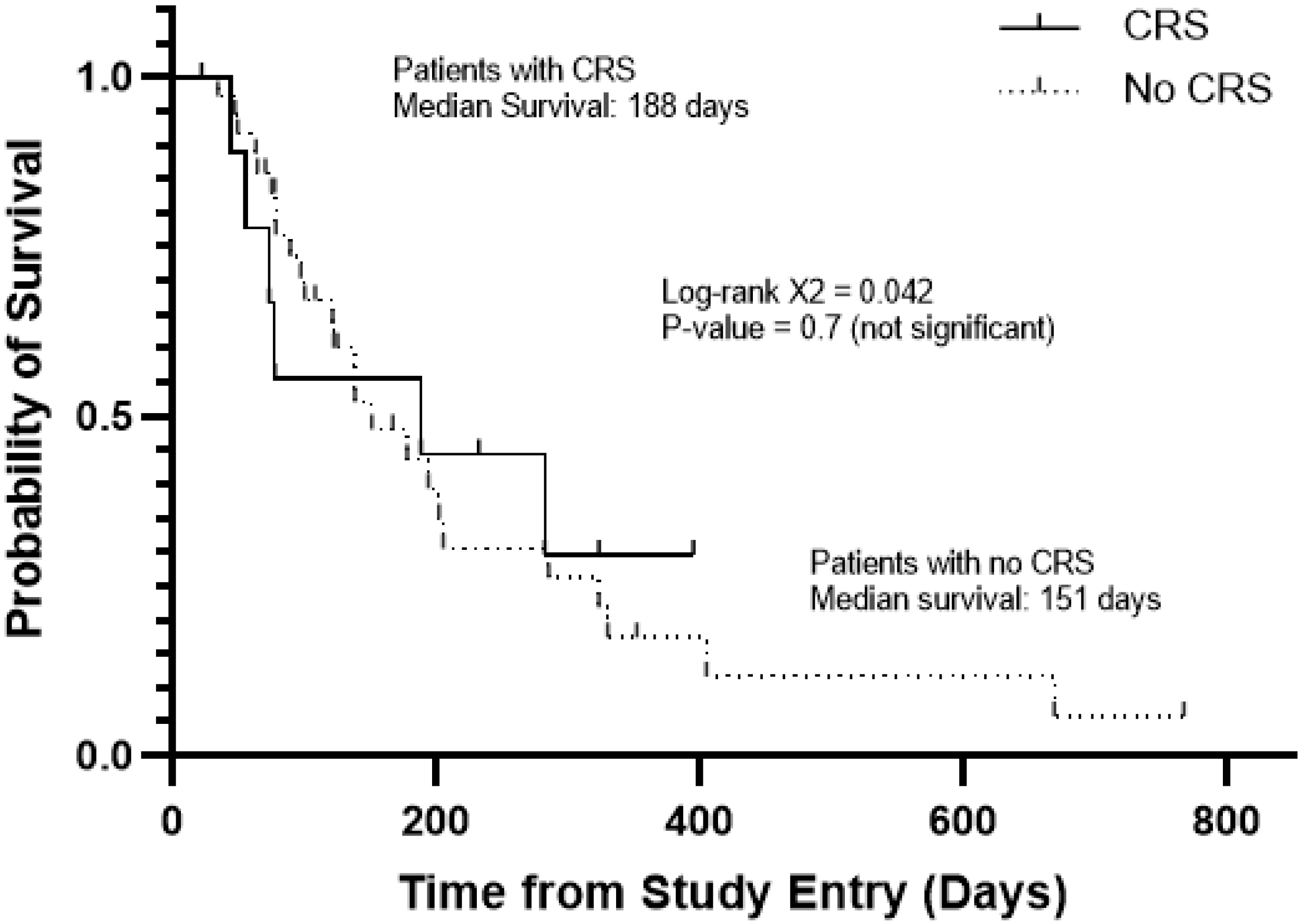
3.3. Clinical Responses to APVO436 in Patients Who Developed CRS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mims, A.S.; Blum, W. Progress in the problem of relapsed or refractory acute myeloid leukemia. Curr. Opin. Hematol. 2019, 26, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Schlenk, R.F.; Muller-Tidow, C.; Benner, A.; Kieser, M. Relapsed/refractory acute myeloid leukemia: Any progress? Curr. Opin. Oncol. 2017, 29, 467–473. [Google Scholar] [CrossRef] [PubMed]
- DiNardo, C.D.; Rausch, C.R.; Benton, C.; Kadia, T.; Jain, N.; Pemmaraju, N.; Daver, N.; Covert, W.; Marx, K.R.; Mace, M.; et al. Clinical experience with the BCL2-inhibitor venetoclax in combination therapy for relapsed and refractory acute myeloid leukemia and related myeloid malignancies. Am. J. Hematol. 2018, 93, 401–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, C.; Doucette, K.; Norsworthy, K. Recent drug approvals for acute myeloid leukemia. J. Hematol. Oncol. 2019, 12, 100. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, F.; Lessi, F.; Vitagliano, O.; Birkenghi, E.; Rossi, G. Current Therapeutic Results and Treatment Options for Older Patients with Relapsed Acute Myeloid Leukemia. Cancers 2019, 11, 224. [Google Scholar] [CrossRef] [Green Version]
- DiNardo, C.D.; Wei, A.H. How I treat acute myeloid leukemia in the era of new drugs. Blood 2020, 135, 85–96. [Google Scholar] [CrossRef]
- Blum, W.G.; Mims, A.S. Treating acute myeloid leukemia in the modern era: A primer. Cancer 2020, 126, 4668–4677. [Google Scholar] [CrossRef]
- Thol, F.; Heuser, M. Treatment for Relapsed/Refractory Acute Myeloid Leukemia. Hemasphere 2021, 5, e572. [Google Scholar] [CrossRef]
- Short, N.J.; Konopleva, M.; Kadia, T.M.; Borthakur, G.; Ravandi, F.; DiNardo, C.D.; Daver, N. Advances in the Treatment of Acute Myeloid Leukemia: New Drugs and New Challenges. Cancer Discov. 2020, 10, 506–525. [Google Scholar] [CrossRef] [Green Version]
- Daver, N.; Wei, A.H.; Pollyea, D.A.; Fathi, A.T.; Vyas, P.; DiNardo, C.D. New Directions for Emerging Therapies in Acute Myeloid Leukemia: The Next Chapter. Blood Cancer J. 2020, 10, 107. [Google Scholar] [CrossRef]
- Uy, G.L.; Aldoss, I.; Foster, M.C.; Sayre, P.H.; Wieduwilt, M.J.; Advani, A.S.; Godwin, J.E.; Arellano, M.L.; Sweet, K.L.; Emadi, A.; et al. Flotetuzumab as salvage immunotherapy for refractory acute myeloid leukemia. Blood 2021, 137, 751–762. [Google Scholar] [CrossRef]
- Daver, N.; Alotaibi, A.S.; Bücklein, V.; Subklewe, M. T-cell-based immunotherapy of acute myeloid leukemia: Current concepts and future developments. Leukemia 2021, 35, 1843–1863. [Google Scholar] [CrossRef] [PubMed]
- Kovtun, Y.; Jones, G.E.; Adams, S.; Harvey, L.; Audette, C.A.; Wilhelm, A.; Bai, C.; Rui, L.; Laleau, R.; Liu, F.; et al. A CD123-targeting antibody-drug conjugate, IMGN632, designed to eradicate AML while sparing normal bone marrow cells. Blood Adv. 2018, 2, 848–858. [Google Scholar] [CrossRef] [Green Version]
- Einsele, H.; Borghaei, H.; Orlowski, R.Z.; Subklewe, M.; Roboz, G.J.; Zugmaier, G.; Kufer, P.; Iskander, K.; Kantarjian, H.M. The BiTE (Bispecific T-cell Engager) Platform: Development and Future Potential of a Targeted Immuno-Oncology Therapy across Tumor Types. Cancer 2020, 126, 3192–3201. [Google Scholar] [CrossRef]
- Isidori, A.; Cerchione, C.; Daver, N.; DiNardo, C.; Garcia-Manero, G.; Konopleva, M.; Jabbour, E.; Ravandi, F.; Kadia, T.; Burguera, A.F.; et al. Immunotherapy in Acute Myeloid Leukemia: Where We Stand. Front. Oncol. 2021, 11, 656218. [Google Scholar] [CrossRef] [PubMed]
- Huehls, A.M.; Coupet, T.A.; Sentman, C.L. Bispecific T-cell Engagers for Cancer Immunotherapy. Immunol. Cell Biol. 2015, 93, 290–296. [Google Scholar] [CrossRef] [Green Version]
- Morris, E.C.; Neelapu, S.S.; Giavridis, T.; Sadelain, M. Cytokine release syndrome and associated neurotoxicity in cancer immunotherapy. Nat. Rev. Immunol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hay, K.A.; Hanafi, L.A.; Li, D.; Gust, J.; Liles, W.C. Kinetics and biomarkers of severe cytokine release syndrome after CD19 chimeric antigen receptor-modified T-cell therapy. Blood 2017, 130, 2295–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aldoss, I.; Khaled, S.K.; Budde, E.; Stein, A.S. Cytokine Release Syndrome with the Novel Treatments of Acute Lymphoblastic Leukemia: Pathophysiology, Prevention, and Treatment. Curr. Oncol. Rep. 2019, 21, 4. [Google Scholar] [CrossRef] [PubMed]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef]
- Lee, D.W.; Gardner, R.; Porter, D.L.; Louis, C.U.; Ahmed, N.; Jensen, M.; Grupp, S.A.; Mackall, C.L. Current concepts in the diagnosis and management of cytokine release syndrome. Blood 2014, 124, 188–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Testa, U.; Riccioni, R.; Coccia, E.; Stellacci, E.; Samoggia, P.; Latagliata, R.; Latagliata, R.; Mariani, G.; Rossini, A.; Battistini, A.; et al. Elevated expression of IL-3Rα in acute myelogenous leukemia is associated with enhanced blast proliferation, increased cellularity and poor prognosis. Blood 2002, 100, 2980–2988. [Google Scholar] [CrossRef]
- Hwang, K.; Park, C.J.; Jang, S.; Chi, H.S.; Kim, D.Y.; Lee, J.H.; Im, H.J.; Seo, J.J. Flow cytometric quantification and immunophenotyping of leukemic stem cells in acute myeloid leukemia. Ann. Hematol. 2012, 91, 1541–1546. [Google Scholar] [CrossRef]
- Jin, L.; Lee, E.M.; Ramshaw, H.S.; Busfiled, S.J.; Peoppl, A.G.; Wilkinson, L.; Wilkinson, L.; Guthridge, M.A.; Thomas, D.; Barry, E.F.; et al. Monoclonal-antibody mediated targeting of CD123, IL-3 receptor alpha chain, eliminates human acute myeloid leukemia stem cells. Cell Stem Cell 2009, 5, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Jordan, C.T.; Upchurch, D.; Szilvassy, S.J.; Guzman, M.L.; Howard, D.S.; Pettigrew, A.L.; Meyerrose, T.; Rossi, R.; Grimes, B.; Rizzieri, D.A.; et al. The interleukin-3 receptor alpha chain is a unique marker for human acute myelogenous leukemia stem cells. Leukemia 2000, 14, 1777–1784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comeau, M.R.; Gottschalk, R.; Daugherty, M.; Sewell, T.; Sewell, T.; Misher, L.; Bannink, J.; Johnson, S.; Parr, L.; Kumer, J.; et al. APVO436, a bispecific anti-CD123 x anti-CD3 ADAPTIR™ molecule for redirected T-cell cytotoxicity with limited cytokine release, is well tolerated in repeat dose toxicology studies in cynomolgus macaques. In Proceedings of the American Association for Cancer Research Annual Meeting 2019, Atlanta, GA, USA, 29 March–3 April 2019; AACR: Philadelphia, PA, USA. Cancer Res. 2019, 79 (Suppl. 13). Abstract nr LB-199. [Google Scholar]
- Comeau, M.R.; Miller, R.E.; Bader, R.; Gottschalk, R.; Daughterty, M.; Sewell, T.; Misher, L.; Parr, L.; DeFrancesco, M.; Bienvenue, D.; et al. APVO436, a bispecific anti-CD123 x anti-CD3 ADAPTIR™ molecule for redirected T-cell cytotoxicity, induces potent T-cell activation, proliferation and cytotoxicity with limited cytokine release. In Proceedings of the American Association for Cancer Research Annual Meeting 2018, Chicago, IL, USA, 14–18 April 2018; AACR: Philadelphia, PA, USA. Cancer Res. 2018, 78 (Suppl. 13). Abstract nr 1786. [Google Scholar]
- Hernandez-Hoyos, G.; Sewell, T.; Bader, R.; Bannink, J.; Chenault, R.A.; Daugherty, M.; Dasovich, M.; Fang, H.; Gottschalk, R.; Kumer, J.; et al. MOR209/ES414, a Novel Bispecific Antibody Targeting PSMA for the Treatment of Metastatic Castration-Resistant Prostate Cancer. Mol. Cancer Ther. 2016, 15, 2155–2165. [Google Scholar] [CrossRef] [Green Version]
- Uckun, F.M.; Lin, T.L.; Mims, A.S.; Patel, P.; Lee, C.; Shahidzadeh, A.; Shami, P.J.; Cull, E.; Cogle, C.R.; Watts, J. A Clinical Phase 1B Study of the CD3xCD123 Bispecific Antibody APVO436 in Patients with Relapsed/Refractory Acute Myeloid Leukemia or Myelodysplastic Syndrome. Cancers 2021, 13, 4113. [Google Scholar] [CrossRef]
- Ravandi, F.; Bashey, A.; Stock, W.; Foran, J.M.; Mawad, R.; Egan, D.; Blum, W.; Yang, A.; Pastore, A.; Johnson, C.; et al. Complete Responses in Relapsed/Refractory Acute Myeloid Leukemia (AML) Patients on a Weekly Dosing Schedule of Vibecotamab (XmAb14045), a CD123 X CD3 T Cell-Engaging Bispecific Antibody; Initial Results of a Phase 1 Study. Blood 2020, 136, 4–5. [Google Scholar] [CrossRef]
- Muller, P.Y.; Milton, M.; Lloyd, P.; Sims, J.; Brennan, F.R. The minimum anticipated biological effect level (MABEL) for selection of first human dose in clinical trials with monoclonal antibodies. Curr. Opin. Biotechnol. 2009, 20, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Santomasso, B.D.; Locke, F.L.; Ghobadi, A.; Turtle, C.J.; Brudno, J.N.; Maus, M.V.; Park, J.H.; Mead, E.; Pavletic, S.; et al. ASTCT Consensus Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated with Immune Effector Cells. Biol. Blood Marrow Transplant. 2019, 25, 625–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breen, E.C.; Reynolds, S.M.; Cox, C.; Jacobson, L.P.; Magpantay, L.; Mulder, C.B.; Dibben, O.; Margolick, J.B.; Bream, J.H.; Sambrano, E.; et al. Multisite comparison of high-sensitivity multiplex cytokine assays. Clin. Vaccine Immunol. 2011, 18, 1229–1242. [Google Scholar] [CrossRef] [Green Version]
- Canter, R.J.; Le, C.T.; Beerthuijzen, J.; Murphy, W.J. Obesity as an immune-modifying factor in cancer immunotherapy. J. Leukoc. Biol. 2018, 104, 487–497. [Google Scholar] [CrossRef]
- Kim, J.; Nam, J.H. Insight into the relationship between obesity-induced low-level chronic inflammation and COVID-19 infection. Int. J. Obes. 2020, 44, 1541–1542. [Google Scholar] [CrossRef]
- Schwartz, R.N.; Stover, L.; Dutcher, J.P. Managing toxicities of high-dose interleukin-2. Oncology 2002, 16 (Suppl. 13), 11–20. [Google Scholar] [PubMed]
- Subklewe, M.; Stein, A.; Walter, R.B.; Bhatia, R.; Wei, A.H.; Ritchie, D.; Bücklein, V.; Vachhani, P.; Dai, T.; Hindoyan, A.; et al. Updated Results from a Phase 1 First-in-Human Dose Escalation Study of AMG 673, a Novel Anti-CD33/CD3 BiTE® (Bispecific T-Cell Engager). In Patients with Relapsed/Refractory Acute Myeloid Leukemia; Abstract: EP548; European Hematology Association: Brussels, Belgium, 2020. [Google Scholar]
- García Roche, A.; Díaz Lagares, C.; Élez, E.; Ferrer Roca, R. Cytokine release syndrome. Reviewing a new entity in the intensive care unit. Med. Intensiva 2019, 43, 480–488. [Google Scholar] [CrossRef]
- Simbaqueba, C.C.; Aponte, M.P.; Kim, P.; Deswal, A.; Palaskas, N.L.; Iliescu, C.; Jahangir, E.; Yang, E.H.; Steiner, R.E.; Lopez-Mattei, J. Cardiovascular complications of chimeric antigen receptor therapy: Cytokine release syndrome and associated arrhytmias. J. Immunother. Precis. Oncol. 2020, 3, 113–120. [Google Scholar] [CrossRef]
- Chen, L.Y.C.; Biggs, C.M.; Jamal, S.; Stukas, S.; Wellington, C.L.; Sekhon, M.S. Soluble Interleukin-6 Receptor in the COVID-19 Cytokine Storm Syndrome. Cell Rep. Med. 2021, 2, 100269. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient No. *** | Steroid Premeds | DL | Start Date | Grade | SAE (Yes/No) | Neuro-Toxicity | Total Duration (Days) | Relatedness with APVO436 | AE Outcome | Changes to Drug Dose or Schedule | Tocilizumab Yes/No |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 214-0002 | No | 1 | C6D1 | 3 | Yes | No | 8 | Related | Resolved | DPD | Yes |
| 203-0003 ** | Yes | 4 | C2D1 | 2 | Yes | Yes | >12 | Related | Fatal (2° ARF, Grade 5) | DPD | Yes |
| 213-0005 | Yes | 4 | C1D3 | 2 | Yes | No | 4 | Related | Resolved | DD | No |
| 217-0002 | Yes | 4 | C1D2 | 4 | Yes | No | 9 | Related | Partially Resolved | DPD | Yes |
| 215-0004 | Yes | 6A | C6D17 | 1 | No | Yes | 2 | Related | Resolved | DR/DD | No |
| 212-0005 | No | 6A | C3D5 | 1 | No | No | 2 | Related | Resolved | DR/DD | No |
| 203-0004 | No | 6A | C1D3 | 3 | Yes | No | 10 | Related | Resolved | DR/DD | Yes |
| 214-0011 | Yes | 7 | C5D1 | 2 | Yes | Yes | 2 | Related | Resolved | TI | Yes |
| 219-0003 | No | 8 | C2D1 | 1 | No | No | 1 | Related | Resolved | None | No |
| 219-0005 * | Yes | A | C1D1 | 3 | Yes | No | 2 | Related | Resolved | TI; pt switched to DL8 | Yes |
| Parameter | CRS | No CRS | p-Value |
|---|---|---|---|
| Age | Mean: 72.9 ± 1.6 95% CI: 69.31, 76.49 Median: 73.50 Range: 66.00–81.00 | Mean: 63.3 ± 2.3 95% CI: 58.8, 68.1 Median: 65.00 Range: 18.00–82.00 | 0.04 |
| Gender | Male: 70% Female: 30% | Male: 47.2% Female: 52.8% | 0.2 |
| Race | C: 70% HL:10% W-HL: 10% A: 10% B: 0% | C: 69.4% HL: 2.8% W-HL: 13.9% A: 2.8% B: 8.3% | 0.6 |
| Dose (µg/kg+) | Mean: 0.28 ± 0.07 95% CI: 0.11, 0.44 Median: 0.19 Range: 0.0040–0.615 | Mean: 0.28 ± 0.04 95% CI: 0.19, 0.37 Median: 0.20 Range: 0.003–0.990 | 1.0 |
| BMI (kg/m2) | Mean: 25.5 ± 1.426 95% CI: 22.3, 28.7 Median: 26.1 Range: 18.3–31.7 (BMI ≥ 30 = 10%; BMI < 30 = 90%) | Mean: 27.5 ± 1.1 95% CI: 25.2, 29.8 Median: 26.5 Range: 16.8–44.4 (BMI ≥ 30 = 34.3%; BMI < 30 = 65.7%) | 0.4 (0.2) |
| Survival Time (ICF–Time of Death or Hospice Transfer) | Mean: 169.1 ± 42.1 95% CI: 73.8, 264.4 Median: 132.5 Range: 22–395 | Mean: 173.9 ± 27.2 95% CI: 118.6, 229.1 Median: 121.5 Range: 34–767 | 0.9 |
| ALC ×103/µL | Mean: 1.3 ± 0.4 95% CI: 0.4, 2.2 Median: 0.9 Range: 0.19–4.36 | Mean: 0.8 ± 0.1 95% CI: 0.6, 1.1 Median: 0.6 Range: 0.01–2.56 | 0.1 |
| % L | Mean: 36.9 ± 6.1 95% CI: 23.2, 50.7 Median: 33.2 Range: 10–72 | Mean: 29.2 ± 3.8 95% CI: 21.5, 36.9 Median: 22 Range: 2–78 | 0.3 |
| WBC ×103/µL | N of Patients = 10 Mean: 4.3 ± 1.495% CI: 1.10, 7.42 Median: 1.8 Range: 0.6–13.5 | N of Patients = 35 Mean: 5.2 ± 1.3 95% CI: 2.5, 7.9 Median: 2.3 Range: 0.3–42.7 | 0.7 |
| % Blasts in Bone Marrow | N of Patients = 10 Mean: 35.1 ± 7.0 95% CI: 19.2, 51.0 Median: 33.5 Range: 5.0–78.0 | N of Patients = 36 Mean: 34.1 ± 4.7 95% CI: 24.6, 43.6 Median: 29.0 Range: 0.0–88.0 | 0.9 |
| % Blasts in Blood | N of Patients = 5 Mean: 10.0 ± 9.5 95% CI: −16.4, 36.4 Median: 0.0 Range: 0.0–48.0 | N of Patients = 19 Mean: 15.9 ± 6.3 95% CI: 2.6, 29.1 Median: 0.0 Range: 0.0–93.0 | 0.1 |
| CD123+CD34+ cellsin blood (% of CD45+) | N of Patients = 7 Mean: 8.24 ± 5.09 95% CI: −4.20, 20.69 Median: 1.48 Range: 0.016–15.39 | N of Patients = 23 Mean: 12.60 ± 4.63 95% CI: 2.99, 22.21 Median: 3.59 Range: 0.005–87.14 | 0.6 |
| T-Cells (% of CD45+) | N of Patients = 7 Mean: 37.93 ± 9.12 95% CI: 15.61, 60.24 Median: 40.81 Range: 6.25–72.40 | N of Patients = 23 Mean: 27.48 ± 5.10 95% CI: 16.90, 38.06 Median: 19.92 Range: 0.32–82.50 | 0.3 |
| Patient ID | Cohort | CRS | Best Overall Response |
|---|---|---|---|
| 214-0002 | 1 | +(Grade 3) | SD |
| 214-0008 | 5 | - | SD |
| 215-0004 | 6A | +(Grade 1) | SD |
| 212-0005 | 6A | +(Grade 1) | PR CR |
| 213-0009 | 6B | - | PR CR |
| 214-0011 | 7 | +(Grade 2) | SD + PBBC-C+ >50%BMB reduction |
| 213-0012 | 10 | - | SD |
| 218-0004 | 10 | - | SD/RES |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uckun, F.M.; Watts, J.; Mims, A.S.; Patel, P.; Wang, E.; Shami, P.J.; Cull, E.; Lee, C.; Cogle, C.R.; Lin, T.L. Risk, Characteristics and Biomarkers of Cytokine Release Syndrome in Patients with Relapsed/Refractory AML or MDS Treated with CD3xCD123 Bispecific Antibody APVO436. Cancers 2021, 13, 5287. https://doi.org/10.3390/cancers13215287
Uckun FM, Watts J, Mims AS, Patel P, Wang E, Shami PJ, Cull E, Lee C, Cogle CR, Lin TL. Risk, Characteristics and Biomarkers of Cytokine Release Syndrome in Patients with Relapsed/Refractory AML or MDS Treated with CD3xCD123 Bispecific Antibody APVO436. Cancers. 2021; 13(21):5287. https://doi.org/10.3390/cancers13215287
Chicago/Turabian StyleUckun, Fatih M., Justin Watts, Alice S. Mims, Prapti Patel, Eunice Wang, Paul J. Shami, Elizabeth Cull, Cynthia Lee, Christopher R. Cogle, and Tara L. Lin. 2021. "Risk, Characteristics and Biomarkers of Cytokine Release Syndrome in Patients with Relapsed/Refractory AML or MDS Treated with CD3xCD123 Bispecific Antibody APVO436" Cancers 13, no. 21: 5287. https://doi.org/10.3390/cancers13215287