
Novel Size-Variable Dedicated Rodent Oxygenator for ECLS Animal Models—Introduction of the “RatOx” Oxygenator and Preliminary In Vitro Results
 , , ,
, , ,  and
and
Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, Year | Animal Model | ECLS Mode | Oxygenator Design and Membrane Type | Oxygenator Priming Volume | Effective Membrane Surface Area | Flow during Experiment | Duration of Experiment | Ref. |
|---|---|---|---|---|---|---|---|---|
| Ali et al. 2014 | SD-rat | ECPR | Undisclosed design/vendor. Images show axial intraluminal flow oxygenator. Silicone membrane. | 8 mL | Undisclosed | 5–6 mL/min. Flow at ECPR-induced arterial pressure of 25–30 mmHg. | 7.3 ± 2.8 min ECPR + 30 min weaning | [33] |
| Fichter et al. 2016 | Fischer-344-rat | Ex vivo organ perfusion | Oxygenator named “Small Animal Micro Oxygenator” (SAMO). Three-layer stacked membrane mats of undisclosed size (5-10 cm edge length, approximated from published image).Polypropylene membranes. | 10 mL for the entire ECC | Undisclosed | 2 mL/min to perfuse isolated free flap | 8 h | [21] |
| Warenits et al. 2016 | SD-rat | ECPR | “SAMO”-oxygenator, see Fichter et al. in this table. Membrane type undisclosed in this publication; group has worked with the same device with polypropylene fibers (see Magnet et al. and Fichter et al. in this table). | Undisclosed | Undisclosed | 100 mL/kg/min | 10 min + 43–83 min weaning | [22] |
| Wiegmann et al. 2016 | In vitro | N/A | In-house design. Single-fiber-mat design. Not for actual ECLS therapy but for experimental endothelialization of hollow-fiber surfaces (oxygenator-like flow chamber). Heparin/albumin-coated polymethylpentene fibers, experimental endothelialization. | 4.275 mL | 18.75 cm2 fiber mat area, i.e., 40 cm2 effective membrane surface area | 15, 30, 60, 90 mL/min | 96 h | [31] |
| Magnet et al. 2017 | SD-rat | ECPR, CBP features | “SAMO”-oxygenator, see Fichter et al. in this table. Polypropylene membrane. | Undisclosed, 15 mL for the entire ECC | Undisclosed | 100 mL/kg/min with rats btw. 460 and 510 g | Max. 10 min + 30 min weaning | [23] |
| Chang et al. 2017 | Wistar–Kyoto rat | ECPR | “Micro-1” rat oxygenator (Dongguan Kewei Medical Instrument Co., Ltd., Guangdong, China). Current commercial availability unknow. Axial flow oxygenator with unknown intra- and extraluminal phases. Membrane type undisclosed in this publication; another group listed below (Cho2021) has likely used the same device from the same manufacturer with polypropylene. | Undisclosed, 19–20 mL for the entire ECC | Undisclosed; Cho et al., also in this table, have likely used the same device by the same vendor (500 cm2) | Undisclosed | 30 min | [26] |
| Madrahimov et al. 2018 | C57BL/6 mouse | VV-ECMO | CPB-oxygenator, in-house design, axial intraluminal flow. Polypropylene membrane. Further information in other publications of Madrahimov et al. [34,35] | Undisclosed,<0.3 mL in referenced [34] | Undisclosed, 50 fibers of 80 mm each of undisclosed outer diameter | 1.5–5 mL/min | 2 h ECC + 5 min weaning | [36] |
| Natanov et al. 2019 | C57BL/6 mouse | VV-ECMO | CPB-oxygenator, in-house design, axial intraluminal flow. Polypropylene membrane. See Madrahimov et al. in this table for further information. | Undisclosed, 500µL for the entire ECC | Undisclosed, 50 fibers of 80 mm each of undisclosed outer diameter | Undisclosed, 3-5 mL/min in [36] | 4 h | [37] |
| Vu et al. 2019 | SD-rat | ECCO2R/Dialysis | “M10” miniaturized dialyzer (Gambro, Lakewood, USA). Only previously described by the group in May et al. [38] and by Goldstein et al. [39]. Axial intraluminal flow oxygenator for neonates. Membrane so-called “AN69” hydrophilic hollow fiber made of s a copolymer of acrylonitrile and sodium methallyl sulfonate. See Thomas et al. [40] for details. | Undisclosed, but the device was designed for infants of 2–15 kg. | 420 cm2 | 1 mL/min | Undisclosed | [30] |
| Wollborn et al. 2019 | SD-rat | VA-ECMO vs. ECPR | “OX “ miniature gas exchange oxygenator, Living Systems Instrumentation, St. Albans City, Vermont, USA. Not further described in the study. The manufacturer’s product description shows an axial extraluminal flow oxygenator and a polypropylene membrane [20]. | Undisclosed, 6 mL for entire ECC. Product sheet by the vendor: 1.6 mL | Undisclosed. Supplier: 115 cm2 [20] | 10–18 mL/min, to reach mean arterial pressure 65 mmHg | 2.5 h + undisclosed weaning | [41] |
| Fujii et al. 2020 | SD-rat | VA-ECMO | “Micro-1” (Senko Medical Instrument Mfg. Co., Ltd., Tokyo, Japan). The picture shows an axial flow oxygenator, apparently with intraluminal flow. The oxygenator appears to be shorter but larger in diameter than other axial flow oxygenators in this table. The oxygenator could not be identified from the manufacturer’s product lists. Membrane type undisclosed. | Undisclosed, 8 mL for entire ECC | Undisclosed | 70 mL/kg/min | 2 h | [28] |
| Edinger et al. 2020 | Lewis rat | VA-ECMO | The “Micro-1” (see Chang et al. in this table) was tested against the “SAMO” (see Fichter et al. in this table) without further device specifications. Both membrane types undisclosed, both polypropylene in other publications with the same devices (Magnet et al. and Cho et al. in this table) | SAMO: 7 mLMicro-1: 3.5 mL | SAMO: 500 cm2; Micro-1: Published with 50 cm2 (Cho et al. published 500 cm2). | 90 mL/kg/min | 2 h | [25] |
| Wilbs et al. 2020 | New Zealand white rabbit | VV-ECMO | In-house design with 40 stacked fiber mat layers. Despite incorporating genuine hollow fibers, the oxygenator was built non-functional regarding gas transfer. It can be considered a simplified mock oxygenator for hemocompatibility testing. Polymethylpentene membrane. This fiber arrangement and fiber bundle design are similar to the RatOx-oxygenator. The stacked fiber mat layers have a cross-sectional flow area that is half that of the RatOx. | Undisclosed | 263 cm2. | 45 mL/min | 4 h | [42] |
| Li et al. 2021 | SD-rat | VV-ECMO | CPB-oxygenator, axial extraluminal flow. Manufactured by Xi’an Xijing Medical Appliance Co. Limited, Xi’An, China. The membrane type is undisclosed in the publication, but based on an inquiry with the supplier, polypropylene fibers are used. | 3 mL | 200 cm2 | 80–90 mL/kg/min | 3.5 h | [43] |
| Cho et al. 2021 | SD-rat | VA- vs. VV-ECMO | “Micro-1”-oxygenator; see Chang et al. in this table. Polypropylene membrane. | 3.5 mL | 500 cm2 | 50 mL/min | 2 h | [27] |
| Fujii et al. 2021 | SD-rat | VV-ECMO | Axial, extraluminal flow oxygenator. Note that the figure in this publication suggests an intraluminal flow, whereas the original publication by Yamada et al. clearly indicates an extraluminal flow. This original publication also includes two other slightly larger oxygenator variations. They also state that polypropylene fibers are used. [17] | Undisclosed, 8 mL for entire ECC. Yamada et al. state a priming volume of 3 mL [17]. | Undisclosed. Yamada et al.: 236 cm2 [17] | 50–60 mL/kg/min | 2 h | [16] |
| Umei et al. 2021 | SD-rat | Mock-ECLS, supported AV-ECMO | A 3D-printed flow cell designed to simulate the local geometry, blood flow patterns and surface area to blood volume ratio of a commercial oxygenator hollow-fiber bundle. Unable to transfer gas. The membrane type is non-functional, clear acrylate resin (PR-48, Colorado Polymer Solutions, Boulder, CO, USA). | 0.3 mL for the oxygenator, 2.5 mL for the entire ECC | 15 cm2 | 1.9 mL/min | 8 h | [13] |
| Edinger et al. 2021 | Lewis rat | VA-ECMO | “SAMO”-oxygenator; see Chang et al. 2017 in this table. Polypropylene membrane. | Undisclosed, 11 mL for the entire ECC | Undisclosed, 500 cm2 in publication of Edinger et al. (2020) in this table | 90 mL/min | 2 h | [24] |
| Govender et al. 2022 | Syrian golden hamster | VA-ECMO | ECC-setup without oxygenator. | Not applicable | Not applicable | 15% of CO | 1.5 h ECC | [44] |
| Greite et al. 2022 | C57BL/6 mouse | VV-ECMO | Redesigned from [35]; CPB-oxygenator, in-house-design, axial intraluminal flow. Polypropylene membrane. | 200 µL | Undisclosed, 50 fibers of 80 mm each of undisclosed outer diameter | Undisclosed, 2.34–6.5 mL/min in [35] | 2 h ECC + 2 h weaning | [45] |
| Huang et al. 2022 | SD-rat | VV-ECMO | See details from Li et al. in this table. | See details from Li et al. in this table. | See details from Li et al. in this table. | See details from Li et al. in this table. | 3 h | [46] |
| Zhang et al. 2022 | SD-rat | VV-ECMO | See details from Li et al. in this table. | See details from Li et al. in this table | See details from Li et al. in this table | 80–90 mL/kg/min | 2 h | [47] |
| Edinger et al. | Lewis rat | VA-ECMO | “Micro-1 “-oxygenator; see Chang et al. 2017 in this table. Polypropylene membrane. | 9 mL | Undisclosed, 500 cm2 in publication by Cho et al. in this table | 90 mL/min | 2 h | [29] |
| Kharnaf et al. 2022 | C57BL/6 mouse | VA-ECMO | “OX” miniature gas exchange oxygenator; see Wollborn et al. in this table. | 1.6 mL oxygenator priming (NaCl, Hetastarch,), 2 mL in remaining ECC (allogeneic blood) | 115 cm2 (supplementary Materials) | 3–5 mL/min | 1 h | [48] |
| Alabdullh et al. 2022 | In vitro | N/A | In-house design. Single-fiber-mat design. Not for actual ECLS therapy but for experimental endothelialization of hollow-fiber surfaces (oxygenator-like flow chamber). The oxygenator design is further development of the device previously published by Wiegmann et al. in this table. Heparin/albumin-coated polymethylpentene fibers with endothelialization. | 4 mL | 19 cm2 | Static | 6 h and 24 h | [32] |
2. Materials and Methods
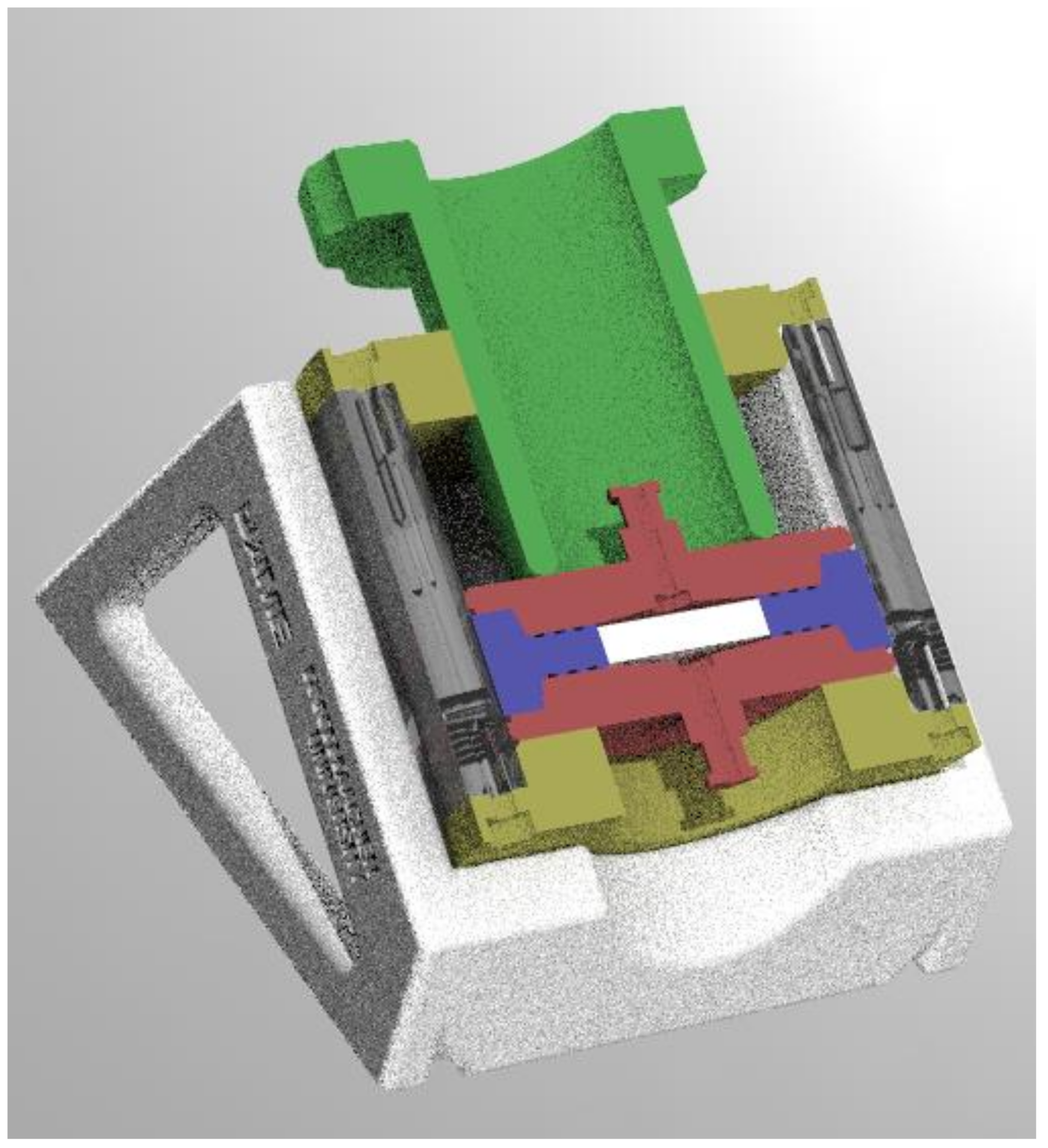
2.1. Oxygenator Design
2.2. In Vitro Proof-of-Concept
3. Results
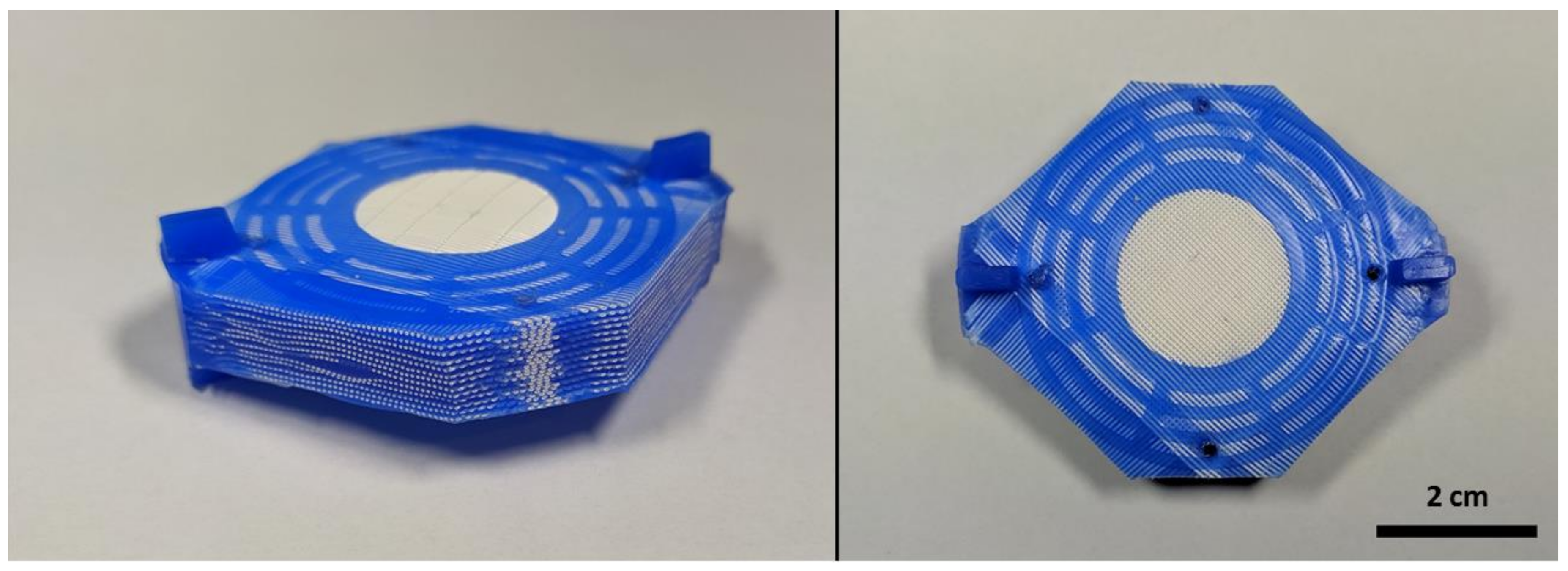
3.1. Oxygenator Design
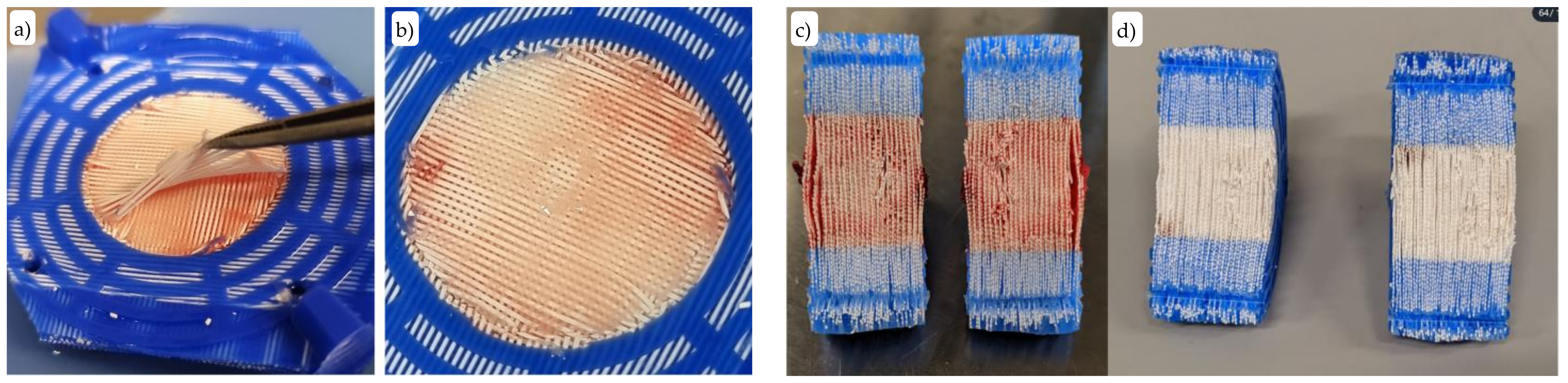
3.2. In Vitro Proof-of-Concept
4. Discussion
5. Conclusions and Outlook
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Tramm, R.; Ilic, D.; Davies, A.R.; Pellegrino, V.A.; Romero, L.; Hodgson, C. Extracorporeal membrane oxygenation for critically ill adults. Cochrane Database Syst. Rev. 2015, 1, CD010381. [Google Scholar] [CrossRef] [PubMed]
- Gannon, W.D.; Trindade, A.J.; Stokes, J.W.; Casey, J.D.; Benson, C.; Patel, Y.J.; Pugh, M.E.; Semler, M.W.; Bacchetta, M.; Rice, T.W. Extracorporeal Membrane Oxygenation Selection by Multidisciplinary Consensus: The ECMO Council. ASAIO J. 2023, 69, 167–173. [Google Scholar] [CrossRef]
- Extracorporeal Life Support Organization. ECLS Registry Report, International Summary 2022. Available online: https://www.elso.org/registry/internationalsummaryandreports/internationalsummary.aspx (accessed on 20 March 2023).
- Bartlett, R.H. ECMO: The next ten years. Egypt. J. Crit. Care Med. 2016, 4, 7–10. [Google Scholar] [CrossRef]
- Lescouflair, T.; Figura, R.; Tran, A.; Kilic, A. Adult veno-arterial extracorporeal life support. J. Thorac. Dis. 2018, 10, S1811–S1818. [Google Scholar] [CrossRef]
- Millar, J.E.; Bartnikowski, N.; Bahr, V.V.; Malfertheiner, M.V.; Obonyo, N.G.; Belliato, M.; Suen, J.Y.; Combes, A.; McAuley, D.F.; Lorusso, R.; et al. Extracorporeal membrane oxygenation (ECMO) and the acute respiratory distress syndrome (ARDS): A systematic review of pre-clinical models. Intensive Care Med. Exp. 2019, 7, 18. [Google Scholar] [CrossRef]
- Yildirim, F.; Amanvermez Senarslan, D.; Yersel, S.; Bayram, B.; Taneli, F.; Tetik, O. Systemic inflammatory response during cardiopulmonary bypass: Axial flow versus radial flow oxygenators. Int. J. Artif. Organs 2022, 45, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Rungatscher, A.; Tessari, M.; Stranieri, C.; Solani, E.; Linardi, D.; Milani, E.; Montresor, A.; Merigo, F.; Salvetti, B.; Menon, T.; et al. Oxygenator is the main responsible for leukocyte activation in experimental model of extracorporeal circulation: A Cautionary tale. Mediat. Inflamm. 2015, 2015, 484979. [Google Scholar] [CrossRef]
- Ballaux, P.K.; Gourlay, T.; Ratnatunga, C.P.; Taylor, K.M. A literature review of cardiopulmonary bypass models for rats. Perfusion 1999, 14, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Berner, M.; Clément, D.; Stadelmann, M.; Kistler, M.; Boone, Y.; Carrel, T.P.; Tevaearai, H.T.; Longnus, S.L. Development of an ultra mini-oxygenator for use in low-volume, buffer-perfused preparations. Int. J. Artif. Organs 2012, 35, 308–315. [Google Scholar] [CrossRef]
- Samarska, I.V.; Henning, R.H.; Buikema, H.; Bouma, H.R.; Houwertjes, M.C.; Mungroop, H.; Struys, M.M.R.F.; Absalom, A.R.; Epema, A.H. Troubleshooting the rat model of cardiopulmonary bypass: Effects of avoiding blood transfusion on long-term survival, inflammation and organ damage. J. Pharmacol. Toxicol. Methods 2013, 67, 82–90. [Google Scholar] [CrossRef]
- Jungwirth, B.; Lange, F.D. Animal models of cardiopulmonary bypass: Development, applications, and impact. Semin. Cardiothorac. Vasc. Anesth. 2010, 14, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Umei, N.; Lai, A.; Miller, J.; Shin, S.; Roberts, K.; Ai Qatarneh, S.; Ichiba, S.; Sakamoto, A.; Cook, K.E. Establishment and evaluation of a rat model of extracorporeal membrane oxygenation (ECMO) thrombosis using a 3D-printed mock-oxygenator. J. Transl. Med. 2021, 19, 179. [Google Scholar] [CrossRef] [PubMed]
- Evseev, A.K.; Zhuravel, S.V.; Alentiev, A.Y.; Goroncharovskaya, I.V.; Petrikov, S.S. Membranes in extracorporeal blood oxygenation technology. Membr. Membr. Technol. 2019, 1, 201–211. [Google Scholar] [CrossRef]
- Olson, S.R.; Murphree, C.R.; Zonies, D.; Meyer, A.D.; Mccarty, O.J.T.; Deloughery, T.G.; Shatzel, J.J. Thrombosis and bleeding in extracorporeal membrane oxygenation (ECMO) without anticoagulation: A systematic review. ASAIO J. 2021, 67, 290–296. [Google Scholar] [CrossRef]
- Fujii, Y.; Sumikura, H.; Nagahama, D. Establishment of a novel miniature veno-venous extracorporeal membrane oxygenation model in the rat. Artif. Organs 2021, 45, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Sumikura, H.; Fujii, Y.; Arafune, T.; Ohgoe, Y.; Yaguchi, T.; Homma, A. Fundamental examination of an extracapillary blood flow type oxygenator for extracorporeal circulation model of a rat. J. Life Support Eng. 2018, 30, 96–104. [Google Scholar] [CrossRef]
- DIN EN ISO 7199:2020-10; Kardiovaskuläre Implantate und künstliche Organe-Blut-Gas-Austauscher (Oxygenatoren), 2020–10. Beuth Verlag GmbH: Berlin, Germany, 2020; 11.040.40. Available online: https://www.beuth.de/de/norm/din-en-iso-7199/317329787 (accessed on 20 February 2023).
- XiJing Medical. Xi’an Xijing Medical Appliance Co., Ltd. of Product Catalogue 2022.10-Membrane Oxygenator for Animal Experiments. Available online: https://www.alibaba.com/product-detail/Membrane-oxygenator-for-animal-experiments_62468042966.html?spm=a2700.shop_index.74.6.3c5e1627VqckuQ (accessed on 29 January 2023).
- Living Systems Instruments. Gas Exchange Oxygenator, Miniature. Available online: https://livingsys.com/product/miniature-gas-exchange-oxygenator/ (accessed on 29 January 2023).
- Fichter, A.M.; Ritschl, L.M.; Borgmann, A.; Humbs, M.; Luppa, P.B.; Wolff, K.-D.; Mücke, T. Development of an extracorporeal perfusion device for small animal free flaps. PLoS ONE 2016, 11, e0147755. [Google Scholar] [CrossRef] [PubMed]
- Warenits, A.-M.; Sterz, F.; Schober, A.; Ettl, F.; Magnet, I.A.M.; Högler, S.; Teubenbacher, U.; Grassmann, D.; Wagner, M.; Janata, A.; et al. Reduction of serious adverse events demanding study exclusion in model development: Extracorporeal life support resuscitation of ventricular fibrillation cardiac arrest in rats. Shock 2016, 46, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Magnet, I.A.M.; Ettl, F.; Schober, A.; Warenits, A.-M.; Grassmann, D.; Wagner, M.; Schriefl, C.; Clodi, C.; Teubenbacher, U.; Högler, S.; et al. Extracorporeal life support increases survival after prolonged ventricular fibrillation cardiac arrest in the rat. Shock 2017, 48, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Edinger, F.; Schmitt, C.; Koch, C.; McIntosh, J.M.; Janciauskiene, S.; Markmann, M.; Sander, M.; Padberg, W.; Grau, V. Application of alpha1-antitrypsin in a rat model of veno-arterial extracorporeal membrane oxygenation. Sci. Rep. 2021, 11, 15849. [Google Scholar] [CrossRef] [PubMed]
- Edinger, F.; Schneck, E.; Schulte, C.; Gehron, J.; Mueller, S.; Sander, M.; Koch, C. Comparison of the effect of membrane sizes and fibre arrangements of two membrane oxygenators on the inflammatory response, oxygenation and decarboxylation in a rat model of extracorporeal membrane oxygenation. BMC Cardiovasc. Disord. 2020, 20, 294. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.-W.; Luo, C.-M.; Yu, H.-Y.; Chen, Y.-S.; Wang, C.-H. Investigation of the pathophysiology of cardiopulmonary bypass using rodent extracorporeal life support model. BMC Cardiovasc. Disord. 2017, 17, 123. [Google Scholar] [CrossRef]
- Cho, H.-J.; Kayumov, M.; Kim, D.; Lee, K.; Onyekachi, F.O.; Jeung, K.-W.; Kim, Y.; Suen, J.Y.; Fraser, J.F.; Jeong, I.-S. Acute immune response in venoarterial and venovenous extracorporeal membrane oxygenation models of rats. ASAIO J. 2021, 67, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Fujii, Y.; Tatsumi, E.; Nakamura, F.; Oite, T. PaO2 greater than 300 mmHg promotes an inflammatory response during extracorporeal circulation in a rat extracorporeal membrane oxygenation model. J. Thorac. Dis. 2020, 12, 749–757. [Google Scholar] [CrossRef]
- Edinger, F.; Schneck, E.; Schulte, C.; Schmidt, G.; Gehron, J.; Sander, M.; Koch, C. Impact of the inspiratory oxygen fraction on the cardiac output during jugulo-femoral venoarterial extracorporeal membrane oxygenation in the rat. BMC Cardiovasc. Disord. 2022, 22, 174. [Google Scholar] [CrossRef]
- Vu, L.H.; Kellum, J.A.; Federspiel, W.J.; Cove, M.E. Carbon dioxide removal using low bicarbonate dialysis in rodents. Perfusion 2019, 34, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Wiegmann, B.; Seggern, H.V.; Höffler, K.; Korossis, S.; Dipresa, D.; Pflaum, M.; Schmeckebier, S.; Seume, J.; Haverich, A. Developing a biohybrid lung-sufficient endothelialization of poly-4-methly-1-pentene gas exchange hollow-fiber membranes. J. Mech. Behav. Biomed. Mater. 2016, 60, 301–311. [Google Scholar] [CrossRef]
- Alabdullh, H.A.; Pflaum, M.; Mälzer, M.; Kipp, M.; Naghilouy-Hidaji, H.; Adam, D.; Kühn, C.; Natanov, R.; Niehaus, A.; Haverich, A.; et al. Biohybrid lung development: Towards complete endothelialization of an assembled extracorporeal membrane oxygenator. Bioengineering 2023, 10, 72. [Google Scholar] [CrossRef]
- Ali, A.A.; Downey, P.; Singh, G.; Qi, W.; George, I.; Takayama, H.; Kirtane, A.; Krishnan, P.; Zalewski, A.; Freed, D.; et al. Rat model of veno-arterial extracorporeal membrane oxygenation. J. Transl. Med. 2014, 12, 37. [Google Scholar] [CrossRef]
- Madrahimov, N.; Natanov, R.; Boyle, E.C.; Goecke, T.; Knöfel, A.-K.; Irkha, V.; Solovieva, A.; Höffler, K.; Maus, U.; Kühn, C.; et al. Cardiopulmonary bypass in a mouse model: A novel approach. J. Vis. Exp. 2017, 127, e56017. [Google Scholar] [CrossRef]
- Madrahimov, N.; Boyle, E.C.; Gueler, F.; Goecke, T.; Knöfel, A.-K.; Irkha, V.; Maegel, L.; Höffler, K.; Natanov, R.; Ismail, I.; et al. Novel mouse model of cardiopulmonary bypass. Eur. J. Cardiothorac. Surg. 2018, 53, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Madrahimov, N.; Khalikov, A.; Boyle, E.C.; Natanov, R.; Knoefel, A.-K.; Siemeni, T.; Hoeffler, K.; Haverich, A.; Maus, U.; Kuehn, C. Veno-venous extracorporeal membrane oxygenation in a mouse. J. Vis. Exp. 2018, 140, e58146. [Google Scholar] [CrossRef]
- Natanov, R.; Khalikov, A.; Gueler, F.; Maus, U.; Boyle, E.C.; Haverich, A.; Kühn, C.; Madrahimov, N. Four hours of veno-venous extracorporeal membrane oxygenation using bi-caval cannulation affects kidney function and induces moderate lung damage in a mouse model. Intensive Care Med. Exp. 2019, 7, 72. [Google Scholar] [CrossRef] [PubMed]
- May, A.G.; Sen, A.; Cove, M.E.; Kellum, J.A.; Federspiel, W.J. Extracorporeal CO2 removal by hemodialysis: In vitro model and feasibility. Intensive Care Med. Exp. 2017, 5, 20. [Google Scholar] [CrossRef]
- Goldstein, S.L.; Hackbarth, R.; Bunchman, T.E.; Blowey, D.; Brophy, P.D. Evaluation of the PRISMA M10® circuit in critically Ill infants with acute kidney injury: A report from the prospective pediatric CRRT registry group. Int. J. Artif. Organs 2006, 29, 1105–1108. [Google Scholar] [CrossRef]
- Thomas, M.; Moriyama, K.; Ledebo, I. AN69: Evolution of the world’s first high permeability membrane. Contrib. Nephrol. 2011, 173, 119–129. [Google Scholar] [CrossRef]
- Wollborn, J.; Siemering, S.; Steiger, C.; Buerkle, H.; Goebel, U.; Schick, M.A. Phosphodiesterase-4 inhibition reduces ECLS-induced vascular permeability and improves microcirculation in a rodent model of extracorporeal resuscitation. Am. J. Physiol. Heart Circ. Physiol. 2019, 316, H751–H761. [Google Scholar] [CrossRef]
- Wilbs, J.; Kong, X.-D.; Middendorp, S.J.; Prince, R.; Cooke, A.; Demarest, C.T.; Abdelhafez, M.M.; Roberts, K.; Umei, N.; Gonschorek, P.; et al. Cyclic peptide FXII inhibitor provides safe anticoagulation in a thrombosis model and in artificial lungs. Nat. Commun. 2020, 11, 3890. [Google Scholar] [CrossRef]
- Li, Y.; Huang, J.; Zhang, R.; Wang, S.; Cheng, X.; Zhang, P.; Zhai, K.; Wang, W.; Liu, D.; Gao, B. Establishment of a venovenous extracorporeal membrane oxygenation in a rat model of acute respiratory distress syndrome. Perfusion 2021, 38, 85–91. [Google Scholar] [CrossRef]
- Govender, K.; Cabrales, P. Extracorporeal circulation impairs microcirculation perfusion and organ function. J. Appl. Physiol. 2022, 132, 794–810. [Google Scholar] [CrossRef]
- Greite, R.; Störmer, J.; Gueler, F.; Khalikov, R.; Haverich, A.; Kühn, C.; Madrahimov, N.; Natanov, R. Different acute kidney injury patterns after renal ischemia reperfusion injury and extracorporeal membrane oxygenation in mice. Int. J. Mol. Sci. 2022, 23, 11000. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Zhang, R.; Zhai, K.; Li, J.; Yao, M.; Wei, S.; Cheng, X.; Yang, J.; Gao, B.; Wu, X.; et al. Venovenous extracorporeal membrane oxygenation promotes alveolar epithelial recovery by activating Hippo/YAP signaling after lung injury. J. Heart Lung Transplant. 2022, 41, 1391–1400. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Zhai, K.; Huang, J.; Wei, S.; Yang, J.; Zhang, Y.; Wu, X.; Li, Y.; Gao, B. Sevoflurane alleviates lung injury and inflammatory response compared with propofol in a rat model of VV ECMO. Perfusion 2022, 2676591221131217. [Google Scholar] [CrossRef]
- Kharnaf, M.; Hogue, S.; Wilkes, Z.; Reagor, J.A.; Leino, D.G.; Gourley, B.; Rosenfeldt, L.; Ma, Q.; Devarajan, P.; Palumbo, J.S.; et al. A murine model of veno-arterial extracorporeal membrane oxygenation. ASAIO J. 2022, 68, e243–e250. [Google Scholar] [CrossRef]
- Bedford, T.G.; Tipton, C.M.; Wilson, N.C.; Oppliger, R.A.; Gisolfi, C.V. Maximum oxygen consumption of rats and its changes with various experimental procedures. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1979, 47, 1278–1283. [Google Scholar] [CrossRef]
- Brands, M.W.; Lee, W.F.; Keen, H.L.; Alonso-Galicia, M.; Zappe, D.H.; Hall, J.E. Cardiac output and renal function during insulin hypertension in Sprague-Dawley rats. Am. J. Physiol. 1996, 271, R276–R281. [Google Scholar] [CrossRef]
- Probst, R.J.; Lim, J.M.; Bird, D.N.; Pole, G.L.; Sato, A.K.; Claybaugh, J.R. Gender differences in the blood volume of conscious sprague-dawley rats. J. Am. Assoc. Lab. Anim. Sci. 2006, 45, 49–52. [Google Scholar]
- Fox, J.G. Laboratory Animal Medicine, 3rd ed.; Elsevier Science & Technology: San Diego, CA, USA, 2015; ISBN 9780124095274. [Google Scholar]
- Suckow, M.A.; Stevens, K.A.; Wilson, R.P. The Laboratory Rabbit, Guinea Pig, Hamster, and Other Rodents, 1st ed.; Elsevier: London, UK, 2012; ISBN 978-0-12-380920-9. [Google Scholar]
- Barbee, R.W.; Perry, B.D.; Re, R.N.; Murgo, J.P. Microsphere and dilution techniques for the determination of blood flows and volumes in conscious mice. Am. J. Physiol. 1992, 263, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Morrison, P.R. Oxygen consumption in several small wild mammals. J. Cell Comp. Physiol. 1948, 31, 69–96. [Google Scholar] [CrossRef] [PubMed]
- Quesenberry, K.E.; Carpenter, J.W. Ferrets, Rabbits, and Rodents; Elsevier (Saunders): Philadelphia, PA, USA, 2012; ISBN 9781416066217. [Google Scholar]
- Cabrales, P.; Acero, C.; Intaglietta, M.; Tsai, A.G. Measurement of the cardiac output in small animals by thermodilution. Microvasc. Res. 2003, 66, 77–82. [Google Scholar] [CrossRef]
- Altman, P.L.; Dittmer, D.S. Biological Handbooks: Respiration and Circulation. Federation of American Societies for Experimental Biology: Rockville, MD, USA, 1971; ISBN 9780913822050. [Google Scholar]
- Ross, B.; McIntosh, M.; Rodaros, D.; Hébert, T.E.; Rohlicek, C.V. Systemic arterial pressure at maturity in rats following chronic hypoxia in early life. Am. J. Hypertens. 2010, 23, 1228–1233. [Google Scholar] [CrossRef]
- Drożdż, D.; Gorecki, A. Oxygen consumption and heat production in Chinchillas. Acta Theriol. 1987, 4, 81–86. [Google Scholar] [CrossRef]
- Hesselmann, F.; Scherenberg, N.; Bongartz, P.; Djeljadini, S.; Wessling, M.; Cornelissen, C.; Schmitz-Rode, T.; Steinseifer, U.; Jansen, S.V.; Arens, J. Structure-dependent gas transfer performance of 3D-membranes for artificial membrane lungs. J. Membr. Sci. 2021, 634, 119371. [Google Scholar] [CrossRef]
- Kaesler, A.; Rosen, M.; Schlanstein, P.C.; Wagner, G.; Groß-Hardt, S.; Schmitz-Rode, T.; Steinseifer, U.; Arens, J. How computational modeling can help to predict gas transfer in artificial lungs early in the design process. ASAIO J. 2020, 66, 683–690. [Google Scholar] [CrossRef]
- Arens, J.; Schraven, L.; Kaesler, A.; Flege, C.; Schmitz-Rode, T.; Rossaint, R.; Steinseifer, U.; Kopp, R. Development and evaluation of a variable, miniaturized oxygenator for various test methods. Artif. Organs 2022, 47, 695–704. [Google Scholar] [CrossRef]
- Hesselmann, F.; Focke, J.M.; Schlanstein, P.C.; Steuer, N.B.; Kaesler, A.; Reinartz, S.D.; Schmitz-Rode, T.; Steinseifer, U.; Jansen, S.V.; Arens, J. Introducing 3D-potting: A novel production process for artificial membrane lungs with superior blood flow design. Bio-Des. Manuf. 2022, 5, 141–152. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Joost, T.; Strassmann, S.; Weber-Carstens, S.; Combes, A.; Windisch, W.; Brodie, D. Safety and efficacy of a novel pneumatically driven extracorporeal membrane oxygenation device. Ann. Thorac. Surg. 2020, 109, 1684–1691. [Google Scholar] [CrossRef] [PubMed]
- He, T.; He, J.; Wang, Z.; Cui, Z. Modification strategies to improve the membrane hemocompatibility in extracorporeal membrane oxygenator (ECMO). Adv. Compos. Hybrid Mater. 2021, 4, 847–864. [Google Scholar] [CrossRef]
- Maul, T.M.; Massicotte, M.P.; Wearden, P.D. ECMO Biocompatibility: Surface Coatings, Anticoagulation, and Coagulation Monitoring. In Extracorporeal Membrane Oxygenation: Advances in Therapy; Firstenberg, M.S., Ed.; InTechIOpen: London, UK, 2016; ISBN 978-953-51-2552-5. [Google Scholar]
- Alentiev, A.Y.; Bogdanova, Y.G.; Dolzhikova, V.D.; Belov, N.A.; Nikiforov, R.Y.; Alentiev, D.A.; Karpov, G.O.; Bermeshev, M.V.; Borovkova, N.V.; Evseev, A.K.; et al. The Evaluation of the hemocompatibility of polymer membrane materials for blood oxygenation. Membr. Membr. Technol. 2020, 2, 368–382. [Google Scholar] [CrossRef]
- Park, A.; Song, Y.; Yi, E.; Duy Nguyen, B.T.; Han, D.; Sohn, E.; Park, Y.; Jung, J.; Lee, Y.M.; Cho, Y.H.; et al. Blood oxygenation using fluoropolymer-based artificial lung membranes. ACS Biomater. Sci. Eng. 2020, 6, 6424–6434. [Google Scholar] [CrossRef] [PubMed]
- Ontaneda, A.; Annich, G.M. Novel surfaces in extracorporeal membrane oxygenation circuits. Front. Med. 2018, 5, 321. [Google Scholar] [CrossRef] [PubMed]
- Gajkowski, E.F.; Herrera, G.; Hatton, L.; Velia Antonini, M.; Vercaemst, L.; Cooley, E. ELSO guidelines for adult and pediatric extracorporeal membrane oxygenation circuits. ASAIO J. 2022, 68, 133–152. [Google Scholar] [CrossRef] [PubMed]






| Requirement | Design Target |
|---|---|
| State of the art design | The oxygenator is built using state-of-the-art design principles. The basic functions are scaled down from commercially available oxygenators. |
| Interchangeable fiber type | All available and similar hollow-fiber membrane types can be used. |
| Effective gas transfer | Based on a rodent body weight of 280 g and a (resting) O2 demand of 0.028 mLO2 per gram body weight per minute (Sprague Dawley rats, both parameters published by Bedfort et al. already in 1979 [49]), the maximum oxygen transfer capacity of the rodent oxygenator should be at least 7.9 mLO2/min. This is valid for blood flow values similar to the physiological cardiac output (121 mL/min, for a 350 g Sprague Dawley rat, published by Brands et al. [50] translates to approximately 100 mL/min for a 280 g rat, assuming the validity of a linear interpolation). |
| Variable gas exchange surface | The design of the oxygenator allows the use of differently sized fiber modules for different animal models and ECLS modalities. The surface area is between 10 cm2 for experimental incubation with scarce endothelial cells (25% of the surface area seeded in a specially designed incubator by Wiegmann et al. [31]) and sufficient gas transfer exchange area toallow the targeted 7.9 mLO2/min of transfer. |
| Low priming volume | The static priming volume is kept as low as possible to minimize hemodilution. The gas exchange area is adjustable to keep the variable priming volume low (see above). The blood volume of a 280 g Sprague Dawley rat can be estimated to be 20.44 mL [51]. Depending on the model, a hemodilution of 20–30% can be tolerated, resulting in a maximum priming volume of approximately 5–9 mL. |
| Low pressure loss | To avoid the need for large pumps and to allow for arteriovenous ECLS cannulation, the pressure drop due to flow resistance across the oxygenator does not exceed 25% of the average mean arterial pressure of the animal, analogous to full-size oxygenators in humans. In the Sprague Dawley rat, this means a tolerable pressure drop of 25 mmHg. |
| Hemocompatibility | Blood-leading components of the oxygenator do not cause avoidable hemocompatibility issues and undesired influences in hemocompatibility testing. Since there are no reference values for oxygenators for hemocompatibility to test this design target, especially not for rodent-sized oxygenators, only state-of-the-art oxygenator designs and materials are used. |
| Transparent housing | The oxygenator is designed to allow for the detection of air bubbles and plasma leakage, using transparent materials where necessary. |
| Reusable housing and removable fiber bundle | To reduce economic burden and to increase availability, the oxygenator design allows for non-destructive disassembly, e.g., without adhesives. All blood-leading materials are made of sterilizable materials. The (disposable) fiber bundle can be explanted and mechanically opened for visual inspection (e.g., immunofluorescence, microscopy). |
| Reproducibility, cross-lab usability and manufacturability | The oxygenator fabrication and assembly process is simple and results in highly reproducible oxygenators. No special equipment is required to fabricate and deploy the oxygenator. The fabrication process uses low-tech equipment so that other laboratories and research groups can fabricate test objects on their own. If other groups do not possess sufficient equipment or resources, the oxygenator can be produced by collaborating institutions. This allows for the reproducibility of results data interpretation across studies, despite the large influence of the oxygenator unit on physiological systems such as hemostasis/thrombosis or inflammatory response [8]. |
| Rodent | Bodyweight (g) | Blood Volume (mL/kg) | Hgb (g/dL) | Hct (%) | Gas Demand O2(l/kg/h) | Heart Rate (min−1) | Mean Art. Pressure (mmHg) | Cardiac Index (mL/min/kg) | References | Comment |
|---|---|---|---|---|---|---|---|---|---|---|
| Mouse (C3H/HeJ, C57BL/6) | 30 ± 5 | 80 ± 4 | 14 ± 2 (a) | 45 ± 7 (a) | 3.5 ± 1.5 (b) | 652 ± 25 | 92 ± 3 | 591 ± 49 | [35,36,37,53,54,55] | (a) Deer mouse (b) Approximation for 6 mouse species based on data from [55]. |
| Gerbil | 89 ± 43 | 73 ± 12 | 14 ± 4 | 44 ± 8 | N/A | 430 ± 170 | 89 ± 11 | N/A | [53,56] | |
| Golden Syrian Hamster | 100 ± 40 | 73 ± 7 (c) | 15 ± 5 (d) | 45 ± 15 (d) | 2.2 ± 0.9 (e) | 390 ± 110 | 113 ± 12 | 197.0 ± 19 | [44,53,57,58] | (c) Listed in [56] without specified hamster strain(d) Listed in [53] without specified hamster strain (e) Gas demand decreasing distinctly with age (11–70 days) |
| Sprague Dawley rat | 410 ± 190 | 58 ± 2 | 15 ± 2 (f) | 50 ± 3 (g) | 1.7 ± 0.1 (h) | 378 ± 64 | 105 ± 20 | 345 ± 20 (i) | [22,43,49,51,53,54,59] | (f) Values for rat strains kangaroo rat and cotton rat, from [53] (g) Values for rat strains kangaroo rat, listed in [53] (h) Calculated from values for animals of 280 g bodyweight (i) Calculated from values for animals of 350 g bodyweight |
| Chinchilla | 500 ± 100 | 57 ± 24 (j) | 12 ± 3 | 43 ± 12 | 0.7 ± 0.1 | 125 ± 25 | N/A | N/A | [53,56,60] | (j) Estimated from absolute values given in [53] |
| Guinea Pig | 950 ± 250 | 80 ± 13 | 14 ± 3 | 40 ± 10 | 0.8 ± 0.04 | 395 ± 75 | 67 ± 3 | 270 ± 30 | [52,53,56] |
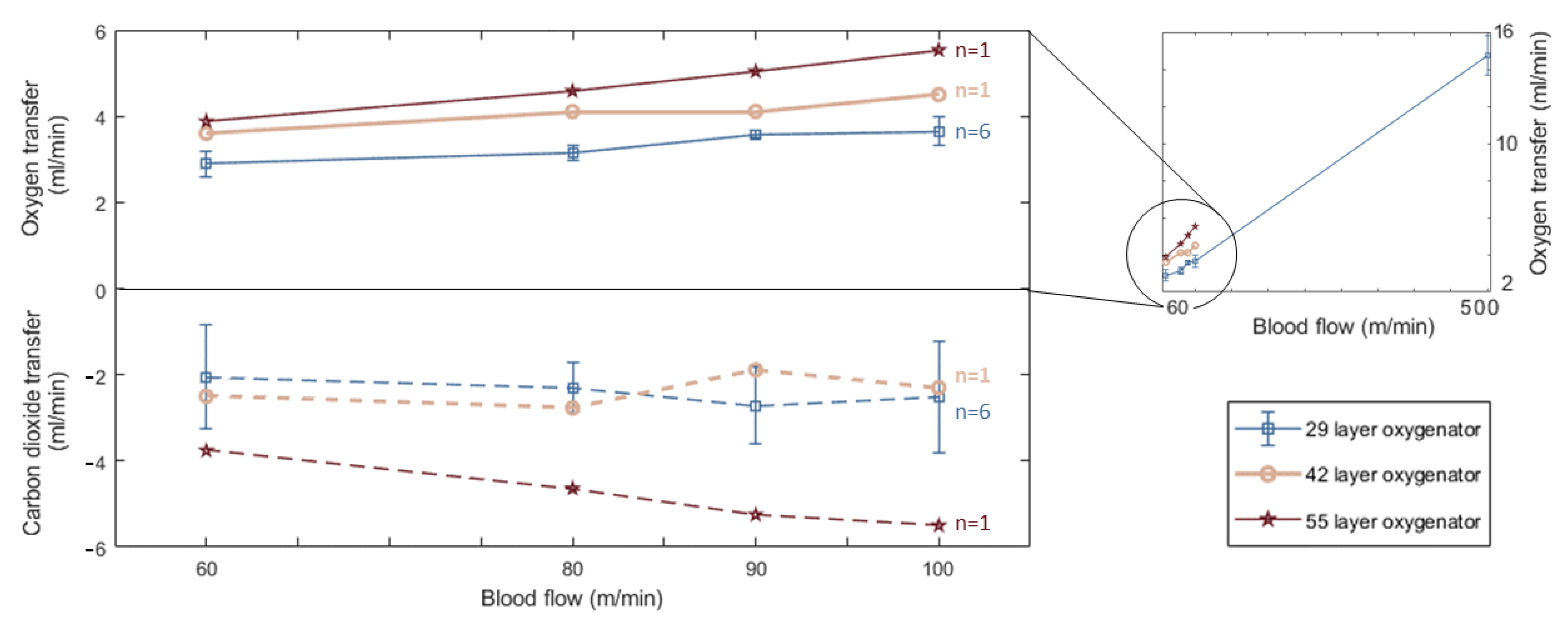
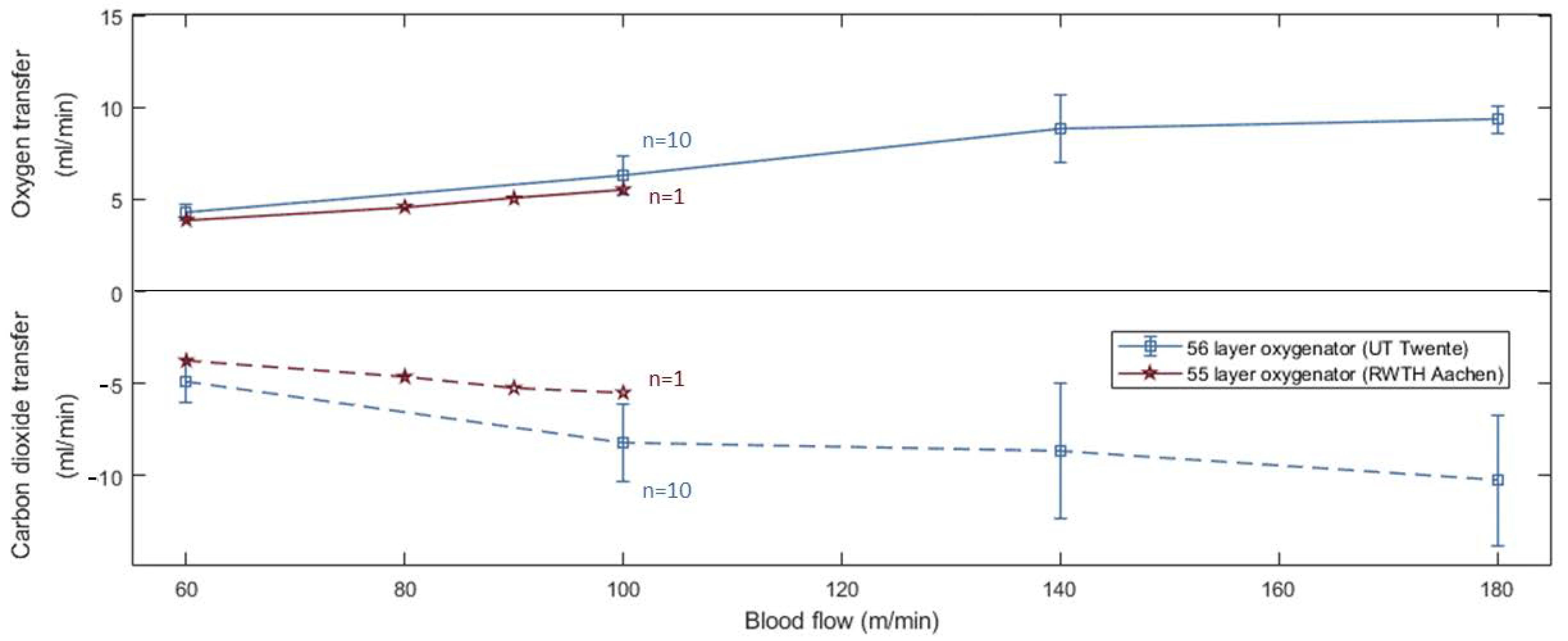
| Blood Flow (mL/min) | Aachen (55 Layers) | Twente (56 Layers) | ||
|---|---|---|---|---|
| Oxygen Transfer (mL/min) | Carbon Dioxide Transfer (mL/min) | Oxygen Transfer (mL/min) | Carbon Dioxide Transfer (mL/min) | |
| 60 | 3.88 | −3.76 | 4.30 ± 0.41 | −4.97 ± 1.10 |
| 80 | 4.59 | −4.64 | N/A | N/A |
| 90 | 5.04 | −5.25 | N/A | N/A |
| 100 | 5.53 | −5.50 | 6.27 ± 0.98 | −8.20 ± 1.97 |
| 140 | N/A | N/A | 8.83 ± 1.77 | −8.64 ± 3.50 |
| 180 | N/A | N/A | 9.33 ± 0.73 | −10.28 ± 3.37 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strudthoff, L.J.; Focke, J.; Hesselmann, F.; Kaesler, A.; Martins Costa, A.; Schlanstein, P.C.; Schmitz-Rode, T.; Steinseifer, U.; Steuer, N.B.; Wiegmann, B.; et al. Novel Size-Variable Dedicated Rodent Oxygenator for ECLS Animal Models—Introduction of the “RatOx” Oxygenator and Preliminary In Vitro Results. Micromachines 2023, 14, 800. https://doi.org/10.3390/mi14040800
Strudthoff LJ, Focke J, Hesselmann F, Kaesler A, Martins Costa A, Schlanstein PC, Schmitz-Rode T, Steinseifer U, Steuer NB, Wiegmann B, et al. Novel Size-Variable Dedicated Rodent Oxygenator for ECLS Animal Models—Introduction of the “RatOx” Oxygenator and Preliminary In Vitro Results. Micromachines. 2023; 14(4):800. https://doi.org/10.3390/mi14040800
Chicago/Turabian StyleStrudthoff, Lasse J., Jannis Focke, Felix Hesselmann, Andreas Kaesler, Ana Martins Costa, Peter C. Schlanstein, Thomas Schmitz-Rode, Ulrich Steinseifer, Niklas B. Steuer, Bettina Wiegmann, and et al. 2023. "Novel Size-Variable Dedicated Rodent Oxygenator for ECLS Animal Models—Introduction of the “RatOx” Oxygenator and Preliminary In Vitro Results" Micromachines 14, no. 4: 800. https://doi.org/10.3390/mi14040800