
Technical and Clinical Progress on Robot-Assisted Endovascular Interventions: A Review
 , , , ,
, , , ,  ,
,
Abstract
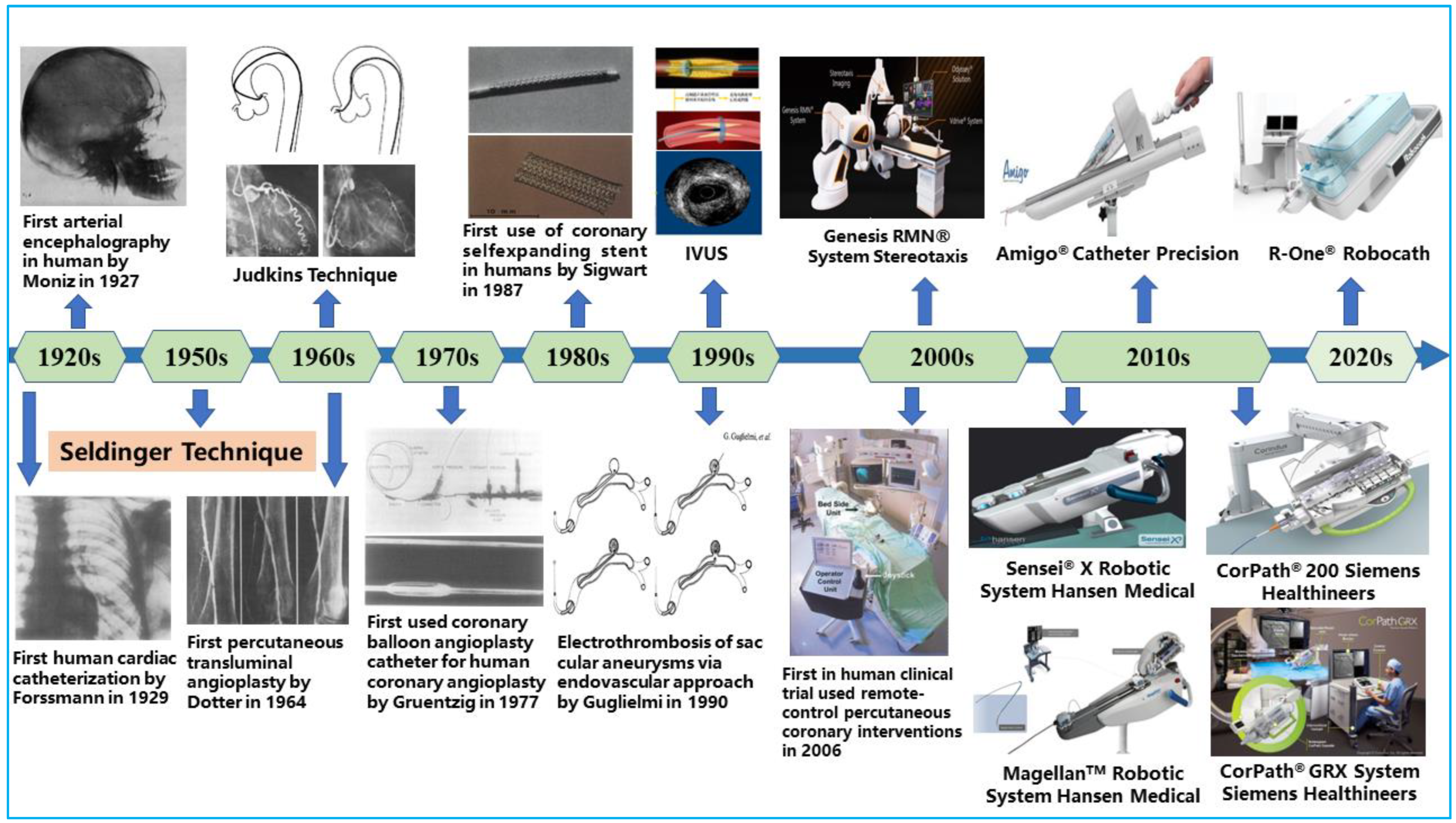
:1. Introduction
2. Key Technologies and Application Areas of Vascular Interventional Robots
2.1. Driving Mechanisms and Teleoperation Setups
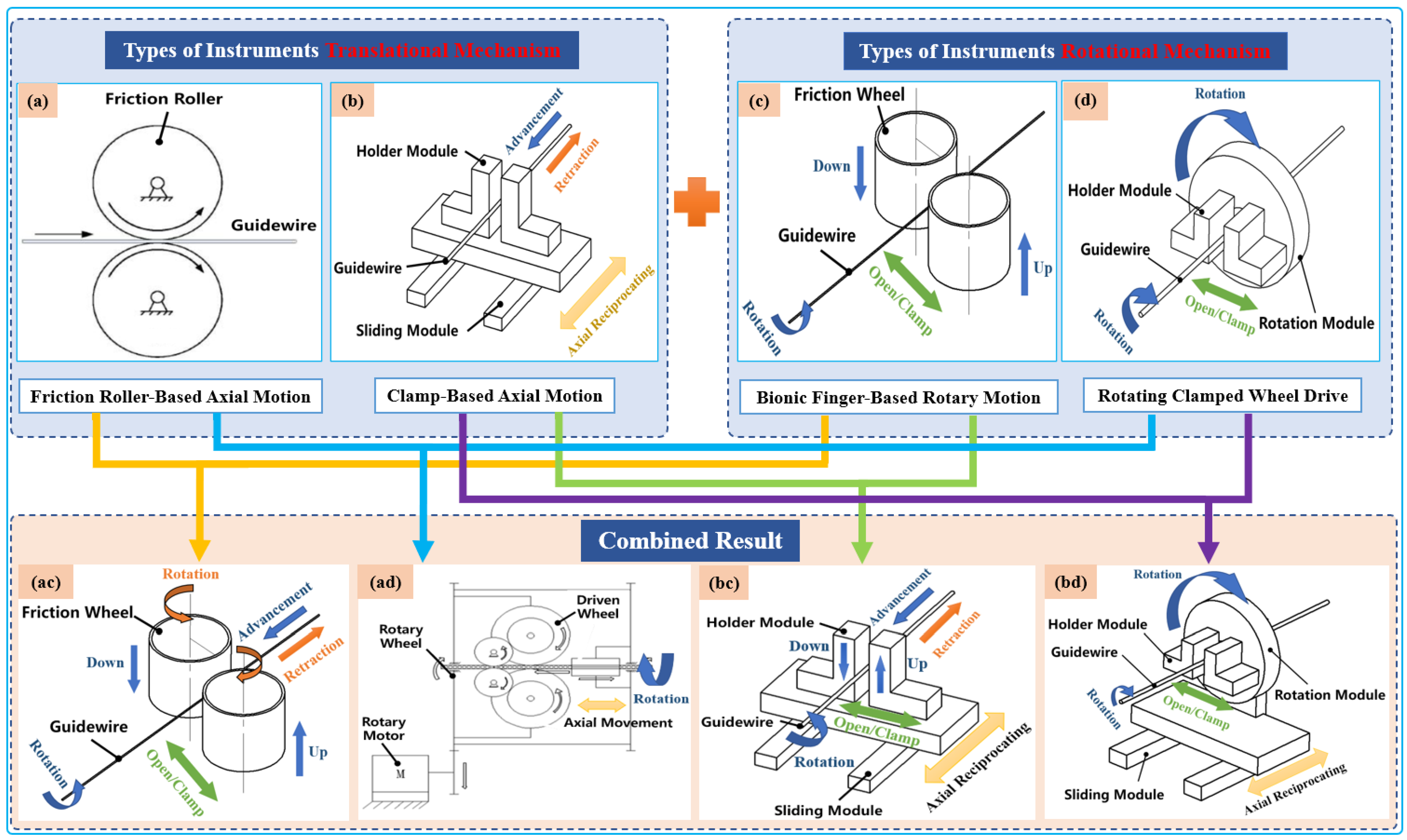
2.1.1. Classification by Driving Mechanisms
- (1)
- Translational Tool Mechanisms
- (2)
- Types of Rotational Instrument Mechanisms
2.1.2. Teleoperation Setup
- (1)
- Isomorphic setup: An isomorphic teleoperation involves using more ergonomic master interfaces that allow surgeons to replicate their natural hand-movement patterns during interventions. In this setup, the master-and-slave systems have similar structural and functional designs. Thus, the actions commands issued on the master side are homogenously replicated in the slave-side device. This makes slave devices exhibit interventionalists’ hand-and-finger dexterity for fine motor-based tool manipulation. Isomorphic setups are new in the endovascular intervention domains. However, recent studies have shown that it can reduce surgeons’ learning curve since they can directly utilize their natural catheterization skills. The isomorphic design by Thakur et al. [25] directly utilizes a real input catheter as the master device and a sensor to record the catheter’s motion while the slave device replicates the master motion to drive a catheter inside the vessel. Similarly, Payne et al. [48] developed a novel master–slave force-feedback system that conforms to a doctor’s natural operating habits and ergonomics. The interface of the same configuration is in line with the intuitive operation of doctors, which is easier to understand and learn. More and more isomorphic platforms have been developed and utilized in recent studies [49,50,51].
- (2)
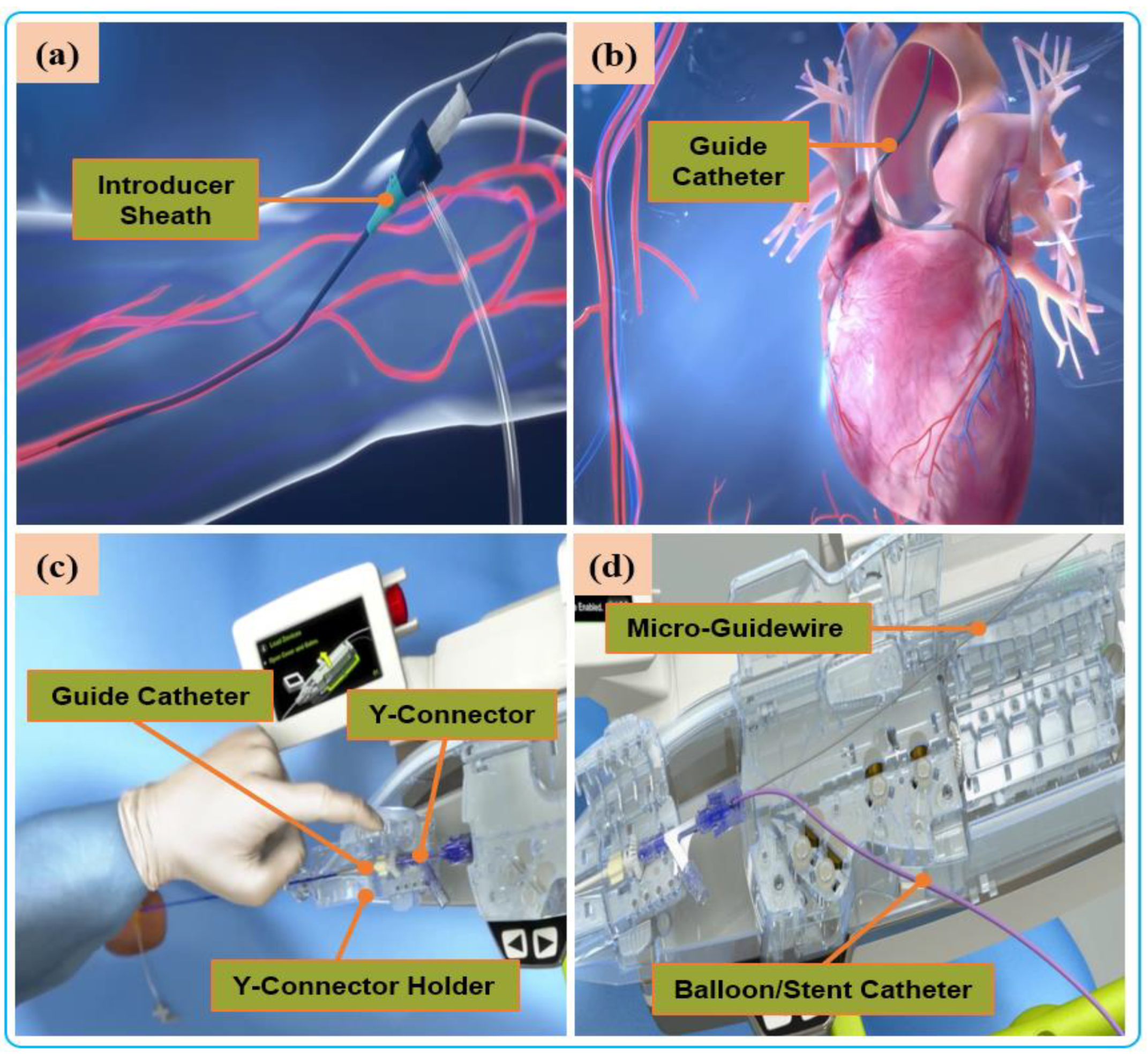
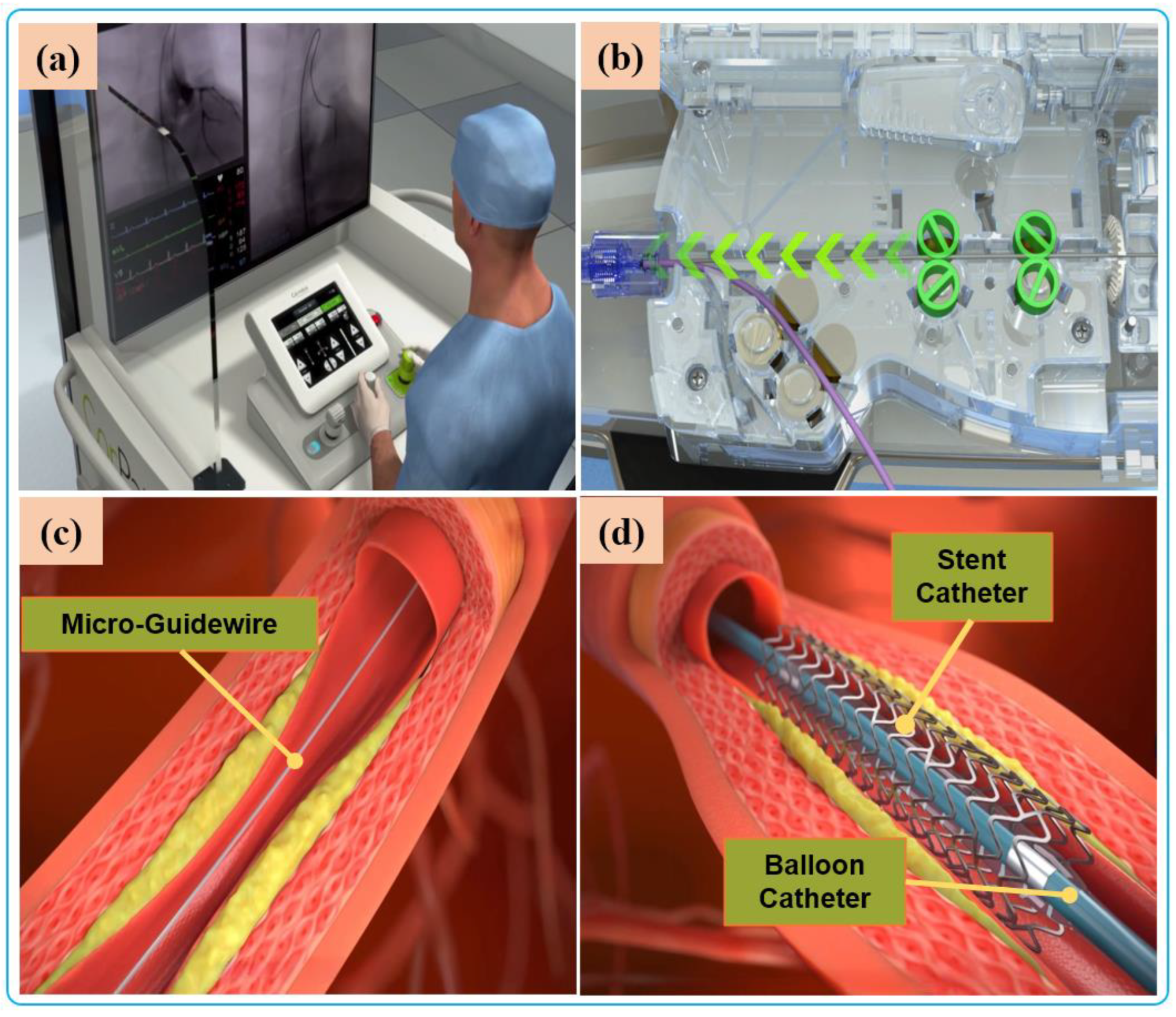
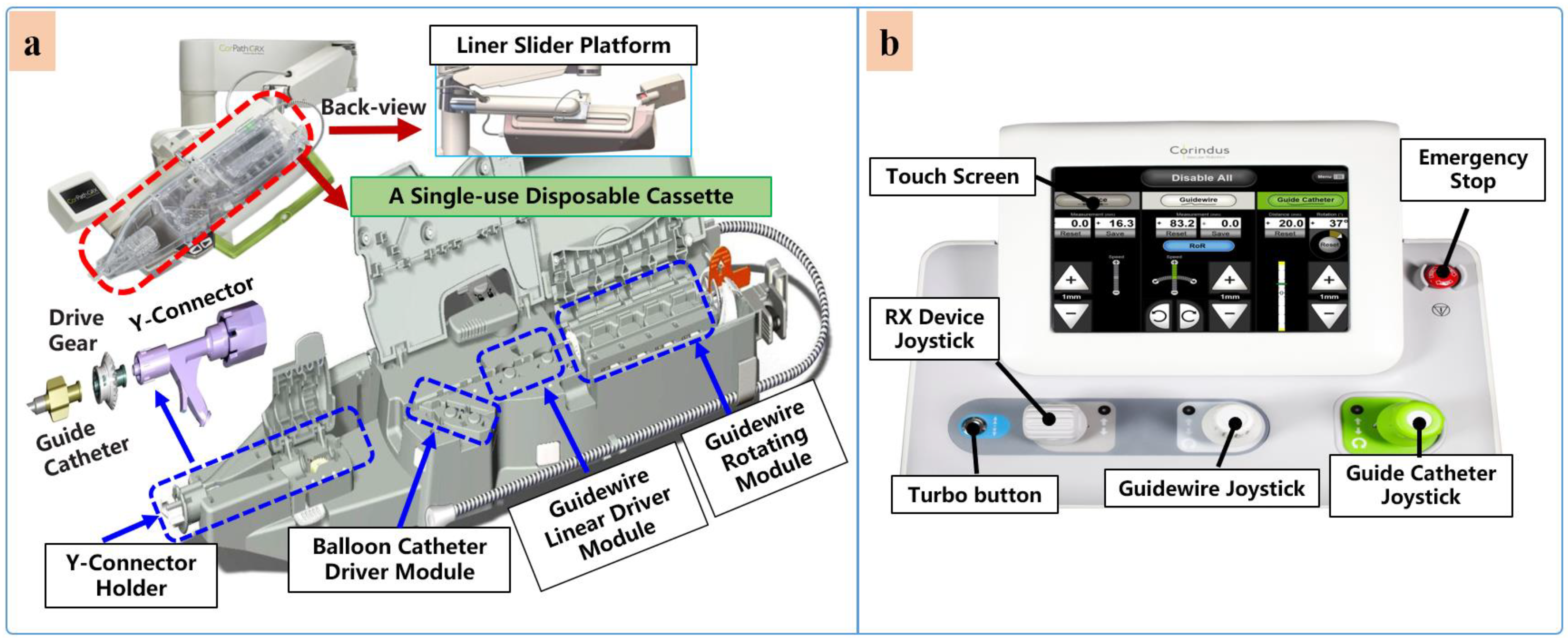
- Non-isomorphic: Non-isomorphic teleoperation design is the earliest and most common approach utilized in robot-assisted minimally invasive interventions. In this mode, a significant difference exists in between the structural design of master-and-slave devices in robotic-platform structural design. Specifically, the robotic setup has master-and-slave control interfaces with a unique design and tool-handling schemes. Currently, most of the commercial robotic systems used for endovascular interventions are generally non-isomorphic. For instance, the control interfaces in CorPath® GRX and CorPath® 200 robotic catheter systems are based on joysticks and touch screens [52]. The typical designs of the CorPath interfaces allows surgeon to manipulate endovascular tools like guidewires with one hand and operate other tools such as the balloon/stent catheter with the other hand. Similarly, in the Amigo® system (Catheter Precision, Inc., Ledgewood, NJ, USA), another major commercial interventional robot used for electrophysiological interventions, the master device is designed as a wireless remote controller for catheter manipulation. The system is able to reproduce linear catheter motions, rotary motion, and tip deflection all issued by the appropriate buttons with one hand on the master device [53]. Although this controller system has an intuitive input method, the design and form are essentially different from the slave robotic platform. Relatedly, some other non-isomorphic setups involve the use of commercial 3-DOF haptic devices as the master-side platform. Typically, Ma et al. [54] and Shen et al. [45] selected Omega (Force Dimension, Nyon, Switzerland), a parallel manipulator capable of producing force feedback to the operator, as the master interface. The commercial controllers are generally adaptable to existing robotic systems. However, customizing them for tool-delivery mechanisms is sometimes difficult.
2.2. Guidance Systems and Robotic Control Scheme
2.2.1. Image-Based Guidance Systems
2.2.2. Robotic-Control Scheme

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Driving Mechanisms (Translation/Rotation) | Teleoperation Setup | Control Scheme | Perception/Feedback | Guidance Systems | Application Areas |
|---|---|---|---|---|---|---|
| CorPath® 200&GRX [73,74,75] | Friction roller-based/Rotating clamped wheel | Non-Isom. | Position and velocity | Obstacle feedback | DSA | PCI PVI NVI |
| MagellanTM [42,76] | Friction roller-based/Friction wheel-based rotation | Non-Isom. | Position and velocity | Haptic | DSA/CT | PVI |
| Guo et al. [26,77] | Clamp-based/Rotating clamped wheel | Non-Isom./Isom. | Position and force | Haptic/Proximal force | DSA | PCI |
| Wang et al. [28,78] | Clamp-based/Rotating clamped wheel | Isom. | Position and force | Haptic/Proximal force | DSA | PCI |
| Wang et al. [40,79] | Friction roller-based/Bionic finger-based rotary | Non-Isom./Isom. | Position and velocity | N/A | DSA | NVI |
| Wang et al. [44,80] | Clamp-based/Rotating clamped wheel | Non-Isom. | Position and velocity | N/A | DSA | PCI PVI |
| Cha et al. [27,81] | Friction roller-based/Rotating clamped wheel | Non-Isom. | Position and force | Haptic/Proximal force | DSA | PCI |
| Choi et al. [82] | Friction roller-based/Bionic finger-based rotary | Non-Isom. | Position and velocity | N/A | DSA | PCI |
| Yang et al. [48,83] | Friction roller-based/Rotating clamped wheel | Isom. | Position and force | Haptic/Distal force | MRI | PCI |
| Tanimoto et al. [84] | Friction roller-based/Rotating clamped wheel | Isom. | Position and force | Haptic/Distal and Proximal force | CT | PCI |
| Omisore et al. [67,85] | Clamp-based/Rotating clamped wheel | Isom. | Position and force | Haptic/Proximal force | DSA | PCI |
| Bian et al. [41,43] | Friction roller-based/Bionic finger-based rotary | Isom. | Position and velocity | N/A | N/A | PCI |
| Zhou et al. [86] | Clamp-based/Rotating clamped wheel | Non-Isom. | Position and force | Proximal force | N/A | PCI |
| Li et al. [87] | Clamp-based/Rotating clamped wheel | N/A | Position and velocity | N/A | IVUS-OCT | PCI |
| Langsch et al. [88] | N/A | N/A | Position and velocity | Proximal force | US | PCI |
2.3. Perception Systiems
2.3.1. Force Feedback
2.3.2. Haptic Perception
2.4. Application Areas of Vascular Interventional Robots
3. Clinical Adoption and Evaluation
4. Discussion and Outlook
- Cooperative Driving Mechanisms of Multiple Instruments
- Perception and Feedback
- Teleoperation Setup and Automation Surgeries
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bentzon, J.F.; Otsuka, F.; Virmani, R.; Falk, E. Mechanisms of Plaque Formation and Rupture. Circ. Res. 2014, 114, 1852–1866. [Google Scholar] [CrossRef]
- Rijanto, E.; Sugiharto, A.; Utomo, S.; Rahmayanti, R.; Afrisal, H.; Nanayakkara, T. Trends in robot assisted endovascular catheterization technology: A review. In Proceedings of the International Conference on Robotics, Biomimetics and Intelligent Computational Systems (Robionetics), Bali, Indonesia, 1 January 2017. [Google Scholar]
- Akinyemi, T.O.; Omisore, O.M.; Lu, G.; Wang, L. Toward a Fiber Bragg Grating-Based Two-Dimensional Force Sensor for Robot-Assisted Cardiac Interventions. IEEE Sens. Lett. 2022, 6, 1–4. [Google Scholar] [CrossRef]
- Kumar, A.; Siddharth, V.; Singh, S.I.; Narang, R. Cost analysis of treating cardiovascular diseases in a super-specialty hospital. PLoS ONE 2022, 17, e262190. [Google Scholar] [CrossRef]
- Akinyemi, T.O.; Omisore, O.M.; Duan, W.; Lu, G.; Al-Handerish, Y.; Han, S.; Wang, L. Fiber Bragg Grating-Based Force Sensing in Robot-Assisted Cardiac Interventions: A Review. IEEE Sens. J. 2021, 21, 10317–10331. [Google Scholar] [CrossRef]
- Artico, M.; Spoletini, M.; Fumagalli, L.; Biagioni, F.; Ryskalin, L.; Fornai, F.; Salvati, M.; Frati, A.; Pastore, F.S.; Taurone, S. Egas Moniz: 90 Years (1927–2017) from Cerebral Angiography. Front. Neuroanat. 2017, 11, 81. [Google Scholar] [CrossRef] [Green Version]
- Omisore, O.M.; Han, S.; Xiong, J.; Li, H.; Li, Z.; Wang, L. A Review on Flexible Robotic Systems for Minimally Invasive Surgery. IEEE Trans. Syst. Man Cybern. Syst. 2022, 52, 631–644. [Google Scholar] [CrossRef]
- Zhao, Y.; Mei, Z.; Luo, X.; Mao, J.; Zhao, Q.; Liu, G.; Wu, D. Remote vascular interventional surgery robotics: A literature review. Quant. Imag. Med. Surg. 2021, 12, 2552–2574. [Google Scholar] [CrossRef]
- Klein, L.W.; Tra, Y.; Garratt, K.N.; Powell, W.; Lopez-Cruz, G.; Chambers, C.; Goldstein, J.A. Occupational health hazards of interventional cardiologists in the current decade: Results of the 2014 SCAI membership survey. Catheter. Cardiovasc. Interv. 2015, 86, 913–924. [Google Scholar] [CrossRef]
- Reeves, R.R.; Ang, L.; Bahadorani, J.; Naghi, J.; Dominguez, A.; Palakodeti, V.; Tsimikas, S.; Patel, M.P.; Mahmud, E. Invasive Cardiologists Are Exposed to Greater Left Sided Cranial Radiation the BRAIN Study (Brain Radiation Exposure and Attenuation during Invasive Cardiology Procedures). JACC Cardiovasc. Interv. 2015, 8, 1197–1206. [Google Scholar] [CrossRef] [Green Version]
- Klein, L.W. Proper Shielding Technique in Protecting Operators and Staff from Radiation Exposure in the Fluoroscopy Environment. J. Invasive Cardiol. 2021, 33, E342–E343. [Google Scholar]
- Andreassi, M.G.; Piccaluga, E.; Guagliumi, G.; Del Greco, M.; Gaita, F.; Picano, E. Occupational Health Risks in Cardiac Catheterization Laboratory Workers. Circ. Cardiovasc. Interv. 2016, 9, e003273. [Google Scholar] [CrossRef]
- Vano, E.; Kleiman, N.J.; Duran, A.; Romano-Miller, M.; Rehani, M.M. Radiation-associated Lens Opacities in Catheterization Personnel: Results of a Survey and Direct Assessments. J. Vasc. Interv. Radiol. 2013, 24, 197–204. [Google Scholar] [CrossRef]
- Campbell, P.T.; Mahmud, E.; Marshall, J.J. Interoperator and intraoperator (in) accuracy of stent selection based on visual estimation. Catheter. Cardiovasc. Interv. 2015, 86, 1177–1183. [Google Scholar] [CrossRef]
- Lo, N.; Gutierrez, J.A.; Swaminathan, R.V. Robotic-Assisted Percutaneous Coronary Intervention. Curr. Treat. Options Cardiovasc. Med. 2018, 20, 14. [Google Scholar] [CrossRef]
- Antoniou, G.A.; Riga, C.V.; Mayer, E.K.; Cheshire, N.J.W.; Bicknell, C.D. Clinical applications of robotic technology in vascular and endovascular surgery. J. Vasc. Surg. 2011, 53, 493–499. [Google Scholar] [CrossRef] [Green Version]
- Bonatti, J.; Vetrovec, G.; Riga, C.; Wazni, O.; Stadler, P. Robotic technology in cardiovascular medicine. Nat. Rev. Cardiol. 2014, 11, 266–275. [Google Scholar] [CrossRef]
- Kazanzides, P.; Fichtinger, G.; Hager, G.D.; Okamura, A.M.; Whitcomb, L.L.; Taylor, R.H. Surgical and Interventional Robotics—Core Concepts, Technology, and Design [Tutorial]. IEEE Robot. Autom. Mag. 2008, 15, 122–130. [Google Scholar] [CrossRef] [Green Version]
- Akinyemi, T.O.; Omisore, O.M.; Chen, X.; Duan, W.; Du, W.; Yi, G.; Wang, L. Adapting Neural-Based Models for Position Error Compensation in Robotic Catheter Systems. Appl. Sci. 2022, 12, 10936. [Google Scholar] [CrossRef]
- Rafii-Tari, H.; Payne, C.J.; Yang, G. Current and Emerging Robot-Assisted Endovascular Catheterization Technologies: A Review. Ann. Biomed. Eng. 2014, 42, 697–715. [Google Scholar] [CrossRef]
- Granada, J.F.; Delgado, J.A.; Uribe, M.P.; Fernandez, A.; Blanco, G.; Leon, M.B.; Weisz, G. First-in-Human Evaluation of a Novel Robotic-Assisted Coronary Angioplasty System. JACC Cardiovasc. Interv. 2011, 4, 460–465. [Google Scholar] [CrossRef] [Green Version]
- Weisz, G.; Metzger, D.C.; Caputo, R.P.; Delgado, J.A.; Marshall, J.J.; Vetrovec, G.W.; Reisman, M.; Waksman, R.; Granada, J.F.; Novack, V.; et al. Safety and Feasibility of Robotic Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2013, 61, 1596–1600. [Google Scholar] [CrossRef]
- Beyar, R.; Gruberg, L.; Deleanu, D.; Roguin, A.; Almagor, Y.; Cohen, S.; Kumar, G.; Wenderow, T. Remote-control percutaneous coronary interventions: Concept, validation, and first-in-humans pilot clinical trial. J. Am. Coll. Cardiol. 2006, 47, 296–300. [Google Scholar] [CrossRef] [Green Version]
- Sankaran, N.K.; Chembrammel, P.; Siddiqui, A.; Snyder, K.; Kesavadas, T. Design and Development of Surgeon Augmented Endovascular Robotic System. IEEE Trans. Biomed. Eng. 2018, 65, 2483–2493. [Google Scholar] [CrossRef]
- Thakur, Y.; Bax, J.S.; Holdsworth, D.W.; Drangova, M. Design and Performance Evaluation of a Remote Catheter Navigation System. IEEE Trans. Biomed. Eng. 2009, 56, 1901–1908. [Google Scholar] [CrossRef]
- Guo, S.; Song, Y.; Yin, X.; Zhang, L.; Tamiya, T.; Hirata, H.; Ishihara, H. A Novel Robot-Assisted Endovascular Catheterization System with Haptic Force Feedback. IEEE Trans. Robot. 2019, 35, 685–696. [Google Scholar] [CrossRef]
- Cha, H.J.; Yi, B.J.; Won, J.Y. An assembly-type master-slave catheter and guidewire driving system for vascular intervention. Proc. Inst. Mech. Eng. Part H 2017, 231, 69–79. [Google Scholar] [CrossRef]
- Wang, H.; Chang, J.; Yu, H.; Liu, H.; Hou, C.; Lu, H. Research on a Novel Vascular Interventional Surgery Robot and Control Method Based on Precise Delivery. IEEE Access 2021, 9, 26568–26582. [Google Scholar] [CrossRef]
- Mahmud, E.; Naghi, J.; Ang, L.; Harrison, J.; Behnamfar, O.; Pourdjabbar, A.; Reeves, R.; Patel, M. Demonstration of the Safety and Feasibility of Robotically Assisted Percutaneous Coronary Intervention in Complex Coronary Lesions Results of the CORA-PCI Study (Complex Robotically Assisted Percutaneous Coronary Intervention). JACC Cardiovasc. Interv. 2017, 10, 1320–1327. [Google Scholar] [CrossRef]
- Mendes Pereira, V.; Cancelliere, N.M.; Nicholson, P.; Radovanovic, I.; Drake, K.E.; Sungur, J.; Krings, T.; Turk, A. First-in-human, robotic-assisted neuroendovascular intervention. J. Neurointerv. Surg. 2020, 12, 338–340. [Google Scholar] [CrossRef] [Green Version]
- Weinberg, J.H.; Sweid, A.; Sajja, K.; Gooch, M.R.; Herial, N.; Tjoumakaris, S.; Rosenwasser, R.H.; Jabbour, P. Comparison of robotic-assisted carotid stenting and manual carotid stenting through the transradial approach. J. Neurosurg. 2020, 135, 21–28. [Google Scholar] [CrossRef]
- Mahmud, E.; Schmid, F.; Kalmar, P.; Deutschmann, H.; Hafner, F.; Rief, P.; Brodmann, M. Feasibility and Safety of Robotic Peripheral Vascular Interventions: Results of the RAPID Trial. JACC Cardiovasc. Interv. 2016, 9, 2058–2064. [Google Scholar] [CrossRef] [PubMed]
- van den Bruck, J.; Sultan, A.; Lüker, J.; Thomas, D.; Willems, S.; Weinmann, K.; Kuniss, M.; Hochadel, M.; Senges, J.; Andresen, D.; et al. Remote vs. conventional navigation for catheter ablation of atrial fibrillation: Insights from prospective registry data. Clin. Res. Cardiol. 2019, 108, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Rufino, M.; Ramos-Arreguín, J.; Rodríguez-Reséndiz, J.; Gorrostieta-Hurtado, E.; Aceves-Fernandez, M. Implementation of ANN-Based Auto-Adjustable for a Pneumatic Servo System Embedded on FPGA. Micromachines 2022, 13, 890. [Google Scholar] [CrossRef] [PubMed]
- García-Martínez, J.R.; Cruz-Miguel, E.E.; Carrillo-Serrano, R.V.; Mendoza-Mondragón, F.; Toledano-Ayala, M.; Rodríguez-Reséndiz, J. A PID-Type Fuzzy Logic Controller-Based Approach for Motion Control Applications. Sensors 2020, 20, 5323. [Google Scholar] [CrossRef] [PubMed]
- Odry, A.; Kecskes, I.; Csik, D.; Rodríguez-Reséndiz, J.; Carbone, G.; Sarcevic, P. Performance Evaluation of Mobile Robot Pose Estimation in MARG-Driven EKF, Cham. In Proceedings of the International Conference of IFToMM ITALY, Napoli, Italy, 7–9 September 2022; Springer: Cham, Switzerland, 2022. [Google Scholar]
- Shi, C.; Song, D.; Lai, D.; Wang, S. Development of a High-Sensitivity Proximal Force/Torque Sensor Based on Optical Sensing for Intravascular Robots. IEEE Trans. Med. Robot. Bionics 2022, 4, 957–966. [Google Scholar] [CrossRef]
- Rafii-Tari, H.; Payne, C.J.; Bicknell, C.; Kwok, K.; Cheshire, N.J.W.; Riga, C.; Yang, G. Objective Assessment of Endovascular Navigation Skills with Force Sensing. Ann. Biomed. Eng. 2017, 45, 1315–1327. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.H. Bian, G.B. Xie, X.L. Hou, Z.G. An Interventionalist-Behavior-Based Data Fusion Framework for Guidewire Tracking in Percutaneous Coronary Intervention. IEEE Trans. Syst. Man Cybern. 2020, 50, 4836–4849. [Google Scholar] [CrossRef]
- Wang, T.; Zhang, D.; Liu, D. Remote-controlled vascular interventional surgery robot. Int. J. Med. Robot. Comp. 2010, 6, 194–201. [Google Scholar] [CrossRef]
- Feng, Z.Q.; Bian, G.B.; Xie, X.L.; Hou, Z.G.; Hao, J.L. Design and evaluation of a bio-inspired robotic hand for percutaneous coronary intervention. In Proceedings of the IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015. [Google Scholar]
- Ghamraoui, A.K.; Ricotta, J.J. Current and Future Perspectives in Robotic Endovascular Surgery. Curr. Surg. Rep. 2018, 6, 21. [Google Scholar] [CrossRef]
- Bian, G.; Xie, X.; Feng, Z.; Hou, Z.; Wei, P.; Cheng, L.; Tan, M. An enhanced dual-finger robotic Hand for Catheter manipulating in vascular intervention: A preliminary study. In Proceedings of the IEEE International Conference on Information and Automation (ICIA), Yinchuan, China, 26–28 August 2013. [Google Scholar]
- Wang, K.; Lu, Q.; Chen, B.; Shen, Y.; Li, H.; Liu, M.; Xu, Z. Endovascular intervention robot with multi-manipulators for surgical procedures: Dexterity, adaptability, and practicability. Robot. Comput.-Integr. Manuf. 2019, 56, 75–84. [Google Scholar] [CrossRef]
- Shen, H.; Wang, C.; Xie, L.; Zhou, S.; Gu, L.; Xie, H. A novel remote-controlled robotic system for cerebrovascular intervention. Int. J. Med. Robot. Comp. 2018, 14, e1943. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Park, S.; Kim, Y.H.; Moon, Y.; Choi, J. A Vascular Intervention Assist Device Using Bi-Motional Roller Cartridge Structure and Clinical Evaluation. Biosensors 2021, 11, 329. [Google Scholar] [CrossRef] [PubMed]
- Kassamali, R.H.; Ladak, B. The role of robotics in interventional radiology: Current status. Quant. Imag. Med. Surg. 2015, 5, 340–343. [Google Scholar]
- Payne, C.J.; Rafii-Tari, H.; Yang, G. A force feedback system for endovascular catheterization. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems, Algarve, Portugal, 7–12 October 2012. [Google Scholar]
- Rafii-Tari, H.; Payne, C.J.; Liu, J.; Riga, C.; Bicknell, C.; Yang, G.Z. Towards automated surgical skill evaluation of endovascular catheterization tasks based on force and motion signatures. In Proceedings of the IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015. [Google Scholar]
- Yu, H.; Wang, H.; Chang, J.; Niu, J.; Wang, F.; Yan, Y.; Tian, H.; Fang, J.; Lu, H. A Novel Vascular Intervention Surgical Robot Based on Force Feedback and Flexible Clamping. Appl. Sci. 2021, 11, 611. [Google Scholar] [CrossRef]
- Omisore, O.M.; Akinyemi, T.O.; Du, W.; Duan, W.; Orji, R.; Do, T.N.; Wang, L. Weighting-Based Deep Ensemble Learning for Recognition of Interventionalists’ Hand Motions During Robot-Assisted Intravascular Catheterization. IEEE Trans. Hum.-Mach. Syst. 2022, 53, 1–13. [Google Scholar] [CrossRef]
- Desai, V.R.; Lee, J.J.; Sample, T.; Kleiman, N.S.; Lumsden, A.; Britz, G.W. First in Man Pilot Feasibility Study in Extracranial Carotid Robotic-Assisted Endovascular Intervention. Neurosurgery 2021, 88, 506–514. [Google Scholar] [CrossRef]
- Khan, E.M.; Frumkin, W.; Ng, G.A.; Neelagaru, S.; Abi-Samra, F.M.; Lee, J.; Giudici, M.; Gohn, D.; Winkle, R.A.; Sussman, J.; et al. First experience with a novel robotic remote catheter system: Amigo™ mapping trial. J. Interv. Card. Electr. 2013, 37, 121–129. [Google Scholar] [CrossRef]
- Ma, Y.; Penney, G.P.; Bos, D.; Frissen, P.; de Fockert, G.; King, A.; Gao, G.; Yao, C.; Totman, J.; Ginks, M.; et al. Evaluation of a robotic arm for echocardiography to X-ray image registration during cardiac catheterization procedures. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009. [Google Scholar]
- Kim, J.; Lee, J.; Chung, J.W.; Shin, Y. Locally adaptive 2D–3D registration using vascular structure model for liver catheterization. Comput. Biol. Med. 2016, 70, 119–130. [Google Scholar] [CrossRef]
- Matl, S.; Brosig, R.; Baust, M.; Navab, N.; Demirci, S. Vascular image registration techniques: A living review. Med. Image Anal. 2017, 35, 1–17. [Google Scholar] [CrossRef]
- Tavallaei, M.A.; Lavdas, M.K.; Gelman, D.; Drangova, M. Magnetic resonance imaging compatible remote catheter navigation system with 3 degrees of freedom. Int. J. Comput. Ass. Rad. 2016, 11, 1537–1545. [Google Scholar] [CrossRef]
- Guo, J.; Shi, C.; Ren, H. Ultrasound-Assisted Guidance with Force Cues for Intravascular Interventions. IEEE Trans. Autom. Sci. Eng. 2019, 16, 253–260. [Google Scholar] [CrossRef]
- Bezerra, H.G.; Attizzani, G.F.; Sirbu, V.; Musumeci, G.; Lortkipanidze, N.; Fujino, Y.; Wang, W.; Nakamura, S.; Erglis, A.; Guagliumi, G.; et al. Optical Coherence Tomography Versus Intravascular Ultrasound to Evaluate Coronary Artery Disease and Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2013, 6, 228–236. [Google Scholar] [CrossRef]
- Rosa, G.M.; Bauckneht, M.; Masoero, G.; Mach, F.; Quercioli, A.; Seitun, S.; Balbi, M.; Brunelli, C.; Parodi, A.; Nencioni, A.; et al. The vulnerable coronary plaque: Update on imaging technologies. Thromb. Haemost. 2013, 110, 706–722. [Google Scholar] [CrossRef] [Green Version]
- Shi, C.; Luo, X.; Guo, J.; Najdovski, Z.; Fukuda, T.; Ren, H. Three-Dimensional Intravascular Reconstruction Techniques Based on Intravascular Ultrasound: A Technical Review. IEEE J. Biomed. Health 2018, 22, 806–817. [Google Scholar] [CrossRef] [PubMed]
- Srimathveeravalli, G.; Kesavadas, T.; Li, X. Design and fabrication of a robotic mechanism for remote steering and positioning of interventional devices. Int. J. Med. Robot. Comp. 2010, 6, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.Q.; Hou, Z.G.; Bian, G.B.; Xie, X.L.; Zhou, X.H. Master-slave Interactive Control and Implementation for Minimally Invasive Vascular Interventional Robots. Acta Autom. Sin. 2016, 42, 696–705. [Google Scholar]
- Song, S.J.; Moon, Y.; Lee, D.H.; Ahn, C.B.; Jo, Y.; Choi, J. Comparative Study of Fuzzy PID Control Algorithms for Enhanced Position Control in Laparoscopic Surgery Robot. J. Med. Biol. Eng. 2015, 35, 34–44. [Google Scholar] [CrossRef]
- Guo, J.; Jin, X.; Guo, S.; Du, W. Study on the tracking performance of the vascular interventional surgical robotic system based on the fuzzy-PID controller. In Proceedings of the IEEE International Conference on Mechatronics and Automation (ICMA), Takamatsu, Japan, 6–9 August 2017. [Google Scholar]
- Omisore, O.M.; Akinyemi, T.O.; Duan, W.; Du, W.; Wang, L. A Novel Sample-efficient Deep Reinforcement Learning with Episodic Policy Transfer for PID-Based Control in Cardiac Catheterization Robots. arXiv 2021, arXiv:211014941. [Google Scholar]
- Omisore, O.M.; Han, S.P.; Ren, L.X.; Wang, G.S.; Ou, F.L.; Li, H.; Wang, L. Towards Characterization and Adaptive Compensation of Backlash in a Novel Robotic Catheter System for Cardiovascular Interventions. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 824–838. [Google Scholar] [CrossRef]
- Zhou, W.; Guo, S.; Guo, J.; Meng, F.; Chen, Z. ADRC-Based Control Method for the Vascular Intervention Master-Slave Surgical Robotic System. Micromachines 2021, 12, 1439. [Google Scholar] [CrossRef]
- Ma, X.; Zhou, J.; Zhang, X.; Qi, Y.; Huang, X. Design of a New Catheter Operating System for the Surgical Robot. Appl. Bionics. Biomech. 2021, 2021, 8898311. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Zhang, Y.; Ourak, M.; Niu, K.; Dankelman, J.; Poorten, E.V. Hysteresis Modeling of Robotic Catheters Based on Long Short-Term Memory Network for Improved Environment Reconstruction. IEEE Robot. Autom. Lett. 2021, 6, 2106–2113. [Google Scholar] [CrossRef]
- Kweon, J.; Kim, K.; Lee, C.; Kwon, H.; Park, J.; Song, K.; Kim, Y.I.; Park, J.; Back, I.; Roh, J.; et al. Deep Reinforcement Learning for Guidewire Navigation in Coronary Artery Phantom. IEEE Access 2021, 9, 166409–166422. [Google Scholar] [CrossRef]
- Karstensen, L.; Ritter, J.; Hatzl, J.; Pätz, T.; Langejürgen, J.; Uhl, C.; Mathis-Ullrich, F. Learning-based autonomous vascular guidewire navigation without human demonstration in the venous system of a porcine liver. Int. J. Comput. Ass. Rad. 2022, 17, 2033–2040. [Google Scholar] [CrossRef] [PubMed]
- Smitson, C.C.; Ang, L.; Pourdjabbar, A.; Reeves, R.; Patel, M.; Mahmud, E. Safety and Feasibility of a Novel, Second-Generation Robotic-Assisted System for Percutaneous Coronary Intervention: First-in-Human Report. J. Invasive Cardiol. 2018, 30, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Legeza, P.; Britz, G.W.; Loh, T.; Lumsden, A. Current utilization and future directions of robotic-assisted endovascular surgery. Expert Rev. Med. Devic. 2020, 17, 919–927. [Google Scholar] [CrossRef]
- Madder, R.D.; VanOosterhout, S.; Parker, J.; Sconzert, K.; Li, Y.; Kottenstette, N.; Madsen, A.; Sungur, J.M.; Bergman, P. Robotic telestenting performance in transcontinental and regional pre-clinical models. Catheter. Cardiovasc. Interv. 2021, 97, E327–E332. [Google Scholar] [CrossRef]
- Bismuth, J.; Kashef, E.; Cheshire, N.; Lumsden, A.B. Feasibility and Safety of Remote Endovascular Catheter Navigation in a Porcine Model. J. Endovasc. Ther. 2011, 18, 243–249. [Google Scholar]
- Bao, X.; Guo, S.; Xiao, N.; Li, Y.; Shi, L. Compensatory force measurement and multimodal force feedback for remote-controlled vascular interventional robot. Biomed. Microdevices 2018, 20, 74. [Google Scholar]
- Yang, X.; Wang, H.; Sun, L.; Yu, H. Operation and Force Analysis of the Guide Wire in a Minimally Invasive Vascular Interventional Surgery Robot System. Chin. J. Mech. Eng. 2015, 28, 249–257. [Google Scholar] [CrossRef]
- Lu, W.S.; Xu, W.Y.; Pan, F.; Liu, D.; Tian, Z.M.; Zeng, Y. Clinical application of a vascular interventional robot in cerebral angiography. Int. J. Med. Robot. Comp. 2016, 12, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Chen, B.; Xu, X. Design and control method of surgical robot for vascular intervention operation. In Proceedings of the IEEE International Conference on Robotics and Biomimetics (ROBIO), Qingdao, China, 3–7 December 2016. [Google Scholar]
- Song, H.; Woo, J.; Won, J.; Yi, B. In Vivo Usability Test of Vascular Intervention Robotic System Controlled by Two Types of Master Devices. Appl. Sci. 2021, 11, 5453. [Google Scholar] [CrossRef]
- Woo, J.; Song, H.; Cha, H.; Yi, B. Advantage of Steerable Catheter and Haptic Feedback for a 5-DOF Vascular Intervention Robot System. Appl. Sci. 2019, 9, 4305. [Google Scholar] [CrossRef] [Green Version]
- Abdelaziz, M.E.; Kundrat, D.; Pupillo, M.; Dagnino, G.; Kwok, T.M.; Chi, W.; Yang, G.Z. Toward a versatile robotic platform for fluoroscopy and mri-guided endovascular interventions: A pre-clinical study. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Macau, China, 3–8 November 2019. [Google Scholar]
- Tanimoto, M.; Arai, F.; Fukuda, T.; Itoigawa, K.; Hashimoto, M.; Takahashi, I.; Negoro, M. Telesurgery system for intravascular neurosurgery. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Pittsburgh, PA, USA, 11–14 October 2000; Springer: Berlin/Heidelberg, Germany, 2000. [Google Scholar]
- Omisore, O.M.; Duan, W.; Du, W.; Zheng, Y.; Akinyemi, T.; Al-Handerish, Y.; Li, W.; Liu, Y.; Xiong, J.; Wang, L. Automatic tool segmentation and tracking during robotic intravascular catheterization for cardiac interventions. Quant. Imag. Med. Surg. 2021, 11, 2688–2710. [Google Scholar] [CrossRef]
- Zhou, J.; Mei, Z.; Miao, J.; Mao, J.; Wang, L.; Wu, D.; Sun, D.; Zhao, Y. A Remote-Controlled Robotic System with Safety Protection Strategy Based on Force-Sensing and Bending Feedback for Transcatheter Arterial Chemoembolization. Micromachines 2020, 11, 805. [Google Scholar] [CrossRef]
- Li, X.; Li, J.; Jing, J.; Ma, T.; Liang, S.; Zhang, J.; Mohar, D.; Raney, A.; Mahon, S.; Brenner, M.; et al. Integrated IVUS-OCT Imaging for Atherosclerotic Plaque Characterization. IEEE J. Sel. Top. Quantum Electron. 2014, 20, 196–203. [Google Scholar]
- Langsch, F.; Virga, S.; Esteban, J.; Gobl, R.; Navab, N. Robotic Ultrasound for Catheter Navigation in Endovascular Procedures. In Proceedings of the IEEE/RSJ International Conference On Intelligent Robots And Systems (IROS), Macau, China, 4–8 November 2019. [Google Scholar]
- Hasan, F.; Bonatti, J. Robotically assisted percutaneous coronary intervention: Benefits to the patient and the cardiologist. Expert Rev. Cardiovas. 2015, 13, 1165–1168. [Google Scholar] [CrossRef]
- Akinyemi, T.O.; Omisore, O.M.; Duan, W.; Lu, G.; Du, W.; Alhanderish, Y.; Li, Y.; Wang, L. Development of a Millinewton FBG-Based Distal Force Sensor for Intravascular Interventions. In Proceedings of the International Conference on Control Automation Robotics and Vision (ICARCV 2020), Shenzhen, China, 13–15 December 2020. [Google Scholar]
- Reddy, V.Y.; Shah, D.; Kautzner, J.; Schmidt, B.; Saoudi, N.; Herrera, C.; Jaïs, P.; Hindricks, G.; Peichl, P.; Yulzari, A.; et al. The relationship between contact force and clinical outcome during radiofrequency catheter ablation of atrial fibrillation in the TOCCATA study. Heart Rhythm 2012, 9, 1789–1795. [Google Scholar] [CrossRef]
- Guo, J.; Guo, S.; Yu, Y. Design and characteristics evaluation of a novel teleoperated robotic catheterization system with force feedback for vascular interventional surgery. Biomed. Microdevices 2016, 18, 76. [Google Scholar] [CrossRef]
- Wei, W.; Yang, D.; Li, L.; Xia, Y. An Intravascular Catheter Bending Recognition Method for Interventional Surgical Robots. Machines 2022, 10, 42. [Google Scholar] [CrossRef]
- Bandari, N.M.; Ahmadi, R.; Hooshiar, A.; Dargahi, J.; Packirisamy, M. Hybrid piezoresistive-optical tactile sensor for simultaneous measurement of tissue stiffness and detection of tissue discontinuity in robot-assisted minimally invasive surgery. J. Biomed. Opt. 2017, 22, 77002. [Google Scholar] [CrossRef] [PubMed]
- Gan, L.; Duan, W.; Akinyemi, T.O.; Du, W.; Omisore, O.M.; Wang, L. Development of a Fiber Bragg Grating-based Force Sensor for Minimally Invasive Surgery—Case Study of Ex-vivo Tissue Palpation. IEEE Trans. Instrum. Meas. 2021, 1. [Google Scholar] [CrossRef]
- He, C.; Wang, S.; Zuo, S. A linear stepping endovascular intervention robot with variable stiffness and force sensing. Int. J. Comput. Ass. Rad. 2018, 13, 671–682. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Wang, H.; Yu, H.; Wang, F.; Fang, J.; Niu, J.; Guo, S. Machine Learning-based Surgical State Perception and Collaborative Control for a Vascular Interventional Robot. IEEE Sens. J. 2022, 22, 7106–7118. [Google Scholar] [CrossRef]
- Bao, X.; Guo, S.; Guo, Y.; Yang, C.; Shi, L.; Li, Y.; Jiang, Y. Multilevel Operation Strategy of a Vascular Interventional Robot System for Surgical Safety in Teleoperation. IEEE Trans. Robot. 2022, 38, 2238–2250. [Google Scholar] [CrossRef]
- Westebring-Van Der Putten, E.P.; Goossens, R.H.M.; Jakimowicz, J.J.; Dankelman, J. Haptics in minimally invasive surgery—A review. Minim. Invasive Ther. Allied Technol. 2008, 17, 3–16. [Google Scholar] [CrossRef]
- Hooshiar, A.; Najarian, S.; Dargahi, J. Haptic Telerobotic Cardiovascular Intervention: A Review of Approaches, Methods, and Future Perspectives. IEEE Rev. Biomed. Eng. 2020, 13, 32–50. [Google Scholar] [CrossRef]
- Hu, Z.; Zhang, J.; Xie, L.; Cui, G. A generalized predictive control for remote cardiovascular surgical systems. ISA Trans. 2020, 104, 336–344. [Google Scholar] [CrossRef]
- Hasanzadeh, S.; Janabi-Sharifi, F. Model-based Force Estimation for Intracardiac Catheters. IEEE/ASME Trans. Mechatron. 2016, 21, 154–162. [Google Scholar]
- Amir, H.; Javad, A.; Naghmeh, B. Image-based Estimation of Contact Forces on Catheters for Robot-assisted Cardiovascular Intervention. In Proceedings of the Hamlyn Symposium on Medical Robotics, London, UK, 24–27 June 2018. [Google Scholar]
- Dagnino, G.; Liu, J.; Abdelaziz, M.E.; Chi, W.; Riga, C.; Yang, G.Z. Haptic feedback and dynamic active constraints for robot-assisted endovascular catheterization. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Madrid, Spain, 1–5 October 2018. [Google Scholar]
- Guo, S.; Yamaji, H.; Kita, Y.; Izuishi, K.; Tamiya, T. A novel active catheter system for Ileus treatment. In Proceedings of the International Conference on Automation and Logistics, Qingdao, China, 1–3 September 2008. [Google Scholar]
- Shen, H.; Wang, C.; Xie, L.; Zhou, S.; Gu, L.; Xie, H. A novel robotic system for vascular intervention: Principles, performances, and applications. Int. J. Comput. Ass. Rad. 2019, 14, 671–683. [Google Scholar] [CrossRef]
- Li, X.; Guo, S.; Shi, P.; Jin, X.; Kawanishi, M. An Endovascular Catheterization Robotic System Using Collaborative Operation with Magnetically Controlled Haptic Force Feedback. Micromachines 2022, 13, 505. [Google Scholar] [CrossRef] [PubMed]
- Saliba, W.; Cummings, J.E.; Oh, S.; Zhang, Y.; Mazgalev, T.N.; Schweikert, R.A.; Burkhardt, J.D.; Natale, A. Novel robotic catheter remote control system: Feasibility and safety of transseptal puncture and endocardial catheter navigation. J. Cardiovasc. Electr. 2006, 17, 1102–1105. [Google Scholar] [CrossRef]
- Kanagaratnam, P.; Koa-Wing, M.; Wallace, D.T.; Goldenberg, A.S.; Peters, N.S.; Davies, D.W. Experience of robotic catheter ablation in humans using a novel remotely steerable catheter sheath. J. Interv. Card. Electr. 2008, 21, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krause, K.; Adamu, U.; Weber, M.; Hertting, K.; Hamm, C.; Kuck, K.; Hoffmann, R.; Kelm, M.; Blindt, R. German stereotaxis-guided percutaneous coronary intervention study group: First multicenter real world experience. Clin. Res. Cardiol. 2009, 98, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Bai, R.; Di Biase, L.; Valderrabano, M.; Lorgat, F.; Mlcochova, H.; Tilz, R.; Meyerfeldt, U.; Hranitzky, P.M.; Wazni, O.; Kanagaratnam, P.; et al. Worldwide Experience with the Robotic Navigation System in Catheter Ablation of Atrial Fibrillation: Methodology, Efficacy and Safety. J. Cardiovasc. Electr. 2012, 23, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Wellens, H. Catheter ablation for cardiac arrhythmias. N. Engl. J. Med. 2004, 351, 1172–1174. [Google Scholar] [CrossRef] [Green Version]
- Beaman, C.B.; Kaneko, N.; Meyers, P.M.; Tateshima, S. A Review of Robotic Interventional Neuroradiology. Am. J. Neuroradiol. 2021, 42, 808–814. [Google Scholar] [CrossRef]
- Walters, D.; Omran, J.; Patel, M.; Reeves, R.; Ang, L.; Mahmud, E. Robotic-Assisted Percutaneous Coronary Intervention. Interv. Cardiol. Clin. 2019, 8, 149–159. [Google Scholar] [CrossRef]
- Sajja, K.C.; Sweid, A.; Al, S.F.; Chalouhi, N.; Avery, M.B.; Schmidt, R.F.; Tjoumakaris, S.I.; Gooch, M.R.; Herial, N.; Abbas, R.; et al. Endovascular robotic: Feasibility and proof of principle for diagnostic cerebral angiography and carotid artery stenting. J. Neurointerv. Surg. 2020, 12, 345–349. [Google Scholar] [CrossRef]
- Panesar, S.S.; Britz, G.W. Endovascular Robotics: The Future of Cerebrovascular Surgery. World Neurosurg. 2019, 129, 327–329. [Google Scholar] [CrossRef]
- Mahmud, E.; Pourdjabbar, A.; Ang, L.; Behnamfar, O.; Patel, M.P.; Reeves, R.R. Robotic technology in interventional cardiology: Current status and future perspectives. Catheter. Cardiovasc. Interv. 2017, 90, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Pourdjabbar, A.; Ang, L.; Reeves, R.R.; Patel, M.P.; Mahmud, E. The Development of Robotic Technology in Cardiac and Vascular Interventions. Rambam Maimonides Med. 2017, 8, e30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolls, A.; Riga, C. Endovascular robotics the current state and the future direction. Ann. R. Coll. Surg. 2018, 1007, 14. [Google Scholar] [CrossRef] [PubMed]
- Riga, C.V.; Bicknell, C.D.; Rolls, A.; Cheshire, N.J.; Hamady, M.S. Robot-assisted Fenestrated Endovascular Aneurysm Repair (FEVAR) Using the Magellan System. J. Vasc. Interv. Radiol. 2013, 24, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.Y.; Wang, H.B.; Zhang, W.; Liu, H.Y.; Chang, J.Y.; Huang, D. Master-slave system research of a vascular interventional surgical robot. In Proceedings of the IEEE International Conference on Real-time Computing and Robotics (RCAR), Kandima, Maldives, 1–5 August 2018. [Google Scholar]
- Wang, H.; Tian, H.; Guo, H.; Yang, X.; Tian, Y.; Hu, X.; Chen, J. Design of propulsion mechanism for vascular interventional operation robot. In Proceedings of the International Conference on Advanced Mechatronic Systems (ICAMechS), Zhengzhou, China, 30 August–2 September 2018. [Google Scholar]
- Perera, A.H.; Riga, C.V.; Monzon, L.; Gibbs, R.G.; Bicknell, C.D.; Hamady, M. Robotic Arch Catheter Placement Reduces Cerebral Embolization During Thoracic Endovascular Aortic Repair (TEVAR). Eur. J. Vasc. Endovasc. 2017, 53, 362–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dello Russo, A.; Fassini, G.; Conti, S.; Casella, M.; Di Monaco, A.; Russo, E.; Riva, S.; Moltrasio, M.; Tundo, F.; De Martino, G.; et al. Analysis of catheter contact force during atrial fibrillation ablation using the robotic navigation system: Results from a randomized study. J. Interv. Card. Electr. 2016, 46, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Gil, M.; Salgado, R.; Merino, J.L.; Datino, T.; Figueroa, J.; Arenal, A.; Mejia, E.; Salguero, R.; Fontenla, A.; Arribas, F. Cavo-tricuspid isthmus radiofrequency ablation using a novel remote navigation catheter system in patients with typical atrial flutter. Europace 2014, 16, 558–562. [Google Scholar] [CrossRef] [Green Version]
- Maor, E.; Eleid, M.F.; Gulati, R.; Lerman, A.; Sandhu, G.S. Current and Future Use of Robotic Devices to Perform Percutaneous Coronary Interventions: A Review. J. Am. Heart Assoc. 2017, 6, e006239. [Google Scholar] [CrossRef]
- Patel, T.M.; Shah, S.C.; Pancholy, S.B. Long Distance Tele-Robotic-Assisted Percutaneous Coronary Intervention: A Report of First-in-Human Experience. Eclinicalmedicine 2019, 14, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Guo, S.X. Current Systems and Research Directions for Robot-based Endovascular Intervention. Life Sci. Instrum. 2013, 11, 3–12. [Google Scholar]
- Simaan, N.; Yasin, R.M.; Wang, L. Medical Technologies and Challenges of Robot-Assisted Minimally Invasive Intervention and Diagnostics. Annu. Rev. Contr. Robot. 2018, 1, 465–490. [Google Scholar] [CrossRef] [Green Version]
- Yang, G.Z.; Cambias, J.; Cleary, K.; Daimler, E.; Drake, J.; Dupont, P.E.; Hata, N.; Kazanzides, P.; Martel, S.; Patel, R.V.; et al. Medical Robotics-Regulatory, ethical, and legal considerations for increasing levels of autonomy. Sci. Robot. 2017, 2, eaam8638. [Google Scholar] [CrossRef] [PubMed]






| Paper | Device | Year | Intervention | Treated Lesions | Technical Accuracy (%) | Clinical Accuracy (%) |
|---|---|---|---|---|---|---|
| Mahmud et al. RAPID [32] | CorPath® 200 | 2016 | R-PVI | 20 | 100 | 100 |
| Mahmud et al. CORA-PCI [29] | CorPath® 200 | 2017 | R-PCI | 157 | 91.7 | 99.1 |
| Perera et al. [123] | MagellanTM | 2017 | R-TEVAR | 11 | N/A | 100 |
| Smitson et al. [73] | CorPath® GRX | 2018 | R-PCI | 40 | 90 | 97.5 |
| Patel et al. REMOTE-PCI [127] | CorPath® GRX | 2019 | Tele-PCI | 5 | 100 | 100 |
| Weinberg et al. [31] | CorPath® GRX | 2020 | RA-NVI | 13 | 100 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duan, W.; Akinyemi, T.; Du, W.; Ma, J.; Chen, X.; Wang, F.; Omisore, O.; Luo, J.; Wang, H.; Wang, L. Technical and Clinical Progress on Robot-Assisted Endovascular Interventions: A Review. Micromachines 2023, 14, 197. https://doi.org/10.3390/mi14010197
Duan W, Akinyemi T, Du W, Ma J, Chen X, Wang F, Omisore O, Luo J, Wang H, Wang L. Technical and Clinical Progress on Robot-Assisted Endovascular Interventions: A Review. Micromachines. 2023; 14(1):197. https://doi.org/10.3390/mi14010197
Chicago/Turabian StyleDuan, Wenke, Toluwanimi Akinyemi, Wenjing Du, Jun Ma, Xingyu Chen, Fuhao Wang, Olatunji Omisore, Jingjing Luo, Hongbo Wang, and Lei Wang. 2023. "Technical and Clinical Progress on Robot-Assisted Endovascular Interventions: A Review" Micromachines 14, no. 1: 197. https://doi.org/10.3390/mi14010197