1. Introduction
RBPs acting as left ventricular assist devices (LVADs) always operate in a constant-speed mode in clinics, providing sufficient output for serious heart failure patients. Although this control method possesses the merits of simplicity, reliability, stability, and durability, it reduces pulsatility, which may lead to a variety of complications [
1,
2]. Moreover, this control mode cannot adapt to a patient’s complex and variable physiological environment. Owing to the lower preload sensitivity of RBPs in the conventional constant speed controller (CSC) [
3], various physiological control techniques have been developed to match the pump output to physiological perfusion requirements [
4].
To meet the perfusion prerequisites for different physiological states of the patient, a variable speed physiological control system is needed for adjusting the motor speed. The Frank–Starling mechanism that mimics the natural heart has been used widely in the development of variable speed physiological control systems [
5,
6,
7,
8,
9]. Stevens MC et al. proposed a control strategy mimicking the Frank–Starling mechanism by directly measuring LAP with a pressure sensor and mounting a flow sensor at the pump outlet catheter used to measure pump flow [
5]. The control system adjusts the pump speed according to the measured pump flow rate, and the Frank–Starling mechanism enables the adjusted pump flow rate to correspond to the venous return volume. However, this control strategy relies on pressure and flow sensors. Petrou et al. proposed a physiological controller based on left ventricular systolic pressure [
6]. Cordeiroa put forward a synchronous physiological control system of a pulsatile pediatric pump to adjust the pump ejection pressure at each cardiac cycle to keep the mean arterial pressure at a specified reference value [
7]. Fetanat developed a novel adaptive physiological control system for an implantable heart pump to respond to interpatient and intra-patient variations to maintain the left ventricular end-diastolic pressure in the normal range to prevent ventricle suction and pulmonary congestion. This study shows that the control performance can be guaranteed across different patients and conditions when using the adaptive physiological control system [
8]. Magkoutas presented a physiological data-driven iterative-learning controller (PDD-ILC) that accurately tracked predefined pump flow trajectories, and achieved physiological, pulsatile, and treatment-driven responses of cfVADs [
9].
Most physiological control systems use sensors to measure hemodynamic parameters, such as pressure and flow in real time for feedback to the controller. However, there are no commercially available implantable sensors, which are stable over time, and the use of these sensors may increase the risk of postoperative complications, such as thrombosis, or require extensive regulatory inquisition [
10]. Therefore, a non-invasive physiological control system using the estimator may solve this problem. Wang Y et al. proposed a sensorless suction prevention and physiologic control (SPPC) algorithm for axial and centrifugal pumps that required only the inherent parameters of the left ventricular assist (pump speed and power) and used a proportional-integral (PI) controller to keep the differential motor speed (△RPM) above a defined threshold [
11]. This controller can effectively maintain the mean reference pressure difference between the left ventricle and the aorta to achieve physiological perfusion, but the performance of the algorithm is affected by problems, such as pump thrombosis. Fu and Xu [
12] proposed a sensorless fuzzy logic control system that uses motor speed and current as inputs to the system without making invasive measurements. However, the assumption that pump flow is proportional to heart rate ignores the influence of cardiac contractile and peripheral circulation on the required flow. Bakouri [
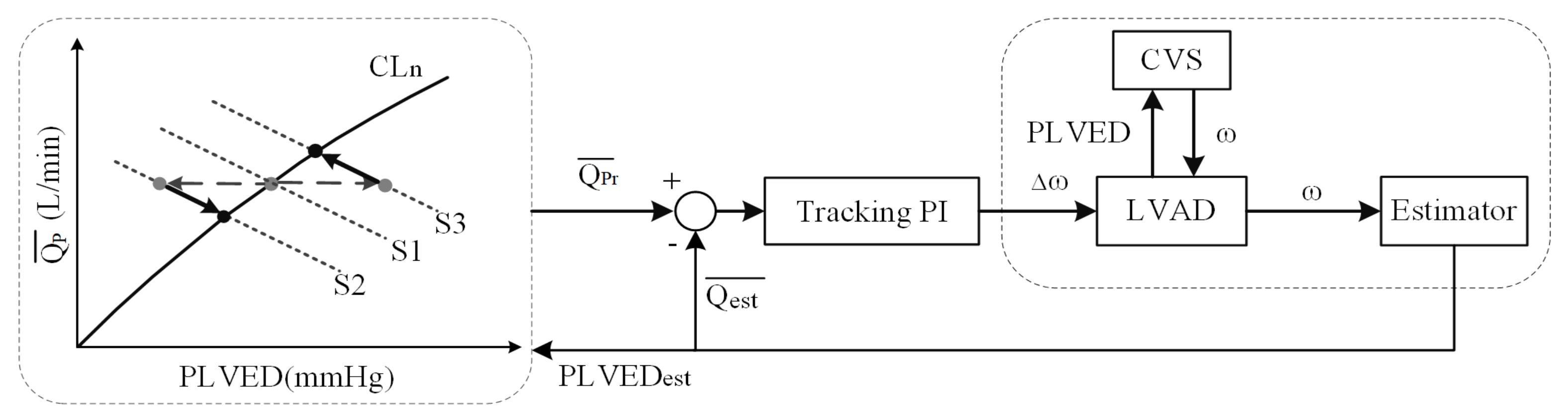
13] used the sliding mode non-invasive control algorithm to take pump speed as the input and pump flow as the estimated output. However, this control algorithm has a corresponding drawback. When left ventricular failure occurs, as is the case in all patients implanted with left ventricular assist devices, the systolic capacity of the left ventricle is severely reduced. Therefore, the dynamic range of the pulsation index is very small, so its ability as a control input is limited. In this paper, a non-invasive adaptive physiological control system based on the Frank–Starling-like mechanism (NAC-FSL) is proposed to solve these problems. The system is also designed to enhance the adaptability to cardiac demand and clinical conditions of the heart that have plagued traditional control strategies. It linked the preload and reference average pump flow and imitated the preload sensitivity of the native heart. This non-linear relationship between the pump flow and ventricular preload enabled the controller to deliver a low preload sensitivity at a high preload, thereby avoiding the ventricle suction and reducing the pump power at a high preload to avoid over-pumping [
14,
15].
In the preload-based control systems using the Frank–Starling mechanism or Frank–Starling-like mechanism, there are no non-invasive instantaneous preload measurement methods available. Although the preload sensitivity (K) of the left ventricle was primarily defined in a third-order polynomial function by Guyton [
16], the determination of the K value, which might affect the robustness of the control system is still unknown. Consequently, this paper will put forward a non-invasive instantaneous preload measurement method and explore the effect of the K value range on the NAC-FSL system under various degrees of heart failure.
3. Results
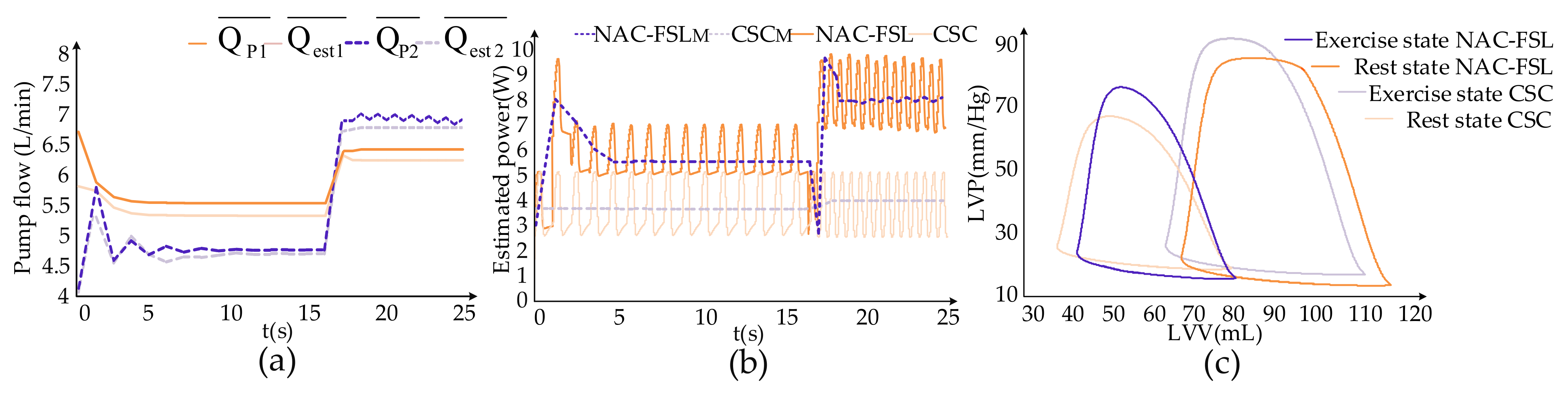
Figure 4 showed the effects of the control systems on hemodynamic parameters from the resting to exercise state. Rotational speed and pump flow are periodic parameters. Therefore, the mean rotational speed means the average value of rotational speed over its period and the mean pump flow refers to the average value over its period in this paper. From the resting to exercise state, the mean motor speed during a cycle of the CSC system remained constant at 2600 r/min. In contrast, the mean motor speed of the NAC-FSL system fluctuated at first and then remained at 2859 r/min at the resting state for the Frank–Starling mechanism. When changing to the exercise state, the mean rotational speed increased to 2945 r/min. As demonstrated in
Figure 4a,
in the CSC system rose from 5.28 L/min to 6.33 L/min, with an increase of 1.05 L/min. The average error in the CSC system between
and
reached R = 0.991 by the algorithm.
in the NAC-FSL system increased from 4.6 L/min to 6.85 L/min, rising by 2.25 L/min from rest to exercise state, and the average error between
and
achieved R = 0.9552. The error between
and
in the NAC-FSL system was smaller than that of the CSC system. When the control system changed from the resting to exercise state, the increase of average pump flow in the NAC-FSL system was higher than that in the CSC system. The higher pump flow helped the NAC-FSL system adapt to the blood flow required for state changes.
In this paper, the pump power (Pe) from a resting state to an exercise state is estimated under the control of two systems, according to the motor speed (ω). Equation (4) depicted the specific calculation for both the systems and the trend of Pe was indicated in
Figure 4b. In the CSC system, Pe was between 2.94 and 5.01 W during both states. However, in the NAC-FSL system, Pe changed from 5.0 to 6.73 W during the resting state and 6.79 to 9.32 W during the exercise state. It means that in the NAC-FSL system, more power from the pump motor is needed to provide higher hydraulic performance, thus unloading the left ventricle more.
The ability to unload the left ventricle is an important indicator for evaluating the physiological control system. The P-V loop (the relationship between LAP and LVV) is always used to evaluate the ability to unload the control systems. In
Figure 4c, the solid lines represent the P-V loop under the resting state, while the broken lines represent an exercise state. Comparing the P-V loops under both control systems, in the rest state, the P-V loop under the NAC-FSL shifts to the left distinctly against the CSC, with a stroke volume (SV) of 40.87 mL and ejection fraction (EF) of 52.19%. While in the exercise activity level, the scores of NAC-FSL and CSC system reach 47.75 mL vs. 41.53 mL and 42.39% vs. 37.49%, respectively. In general, the NAC-FSL control system unloads the left ventricle more than the CSC control system, with a higher EF close to normal levels.
The K value mentioned earlier was added to the controller to provide a means of altering preload sensitivity. The selection of an optimal scale factor (K) for patients with different levels of heart failure was explained in this paper in order to provide the appropriate pump flow. As suggested in
Table 3, this paper approximately graded the degree of heart failure into severe heart failure (Emax = 0.5), moderate heart failure (Emax = 1.0), and mild heart failure (Emax = 1.5) [
18].
Figure 5 depicts the differences in hemodynamic parameters due to the changes in the value of K, thereby figuring out a more appropriate value of K for different degrees of heart failure.
Figure 5a–c represent severe, moderate, and mild heart failures, respectively, and highlight the changes in aortic flow (AOF), aortic pressure (AOP), and
for different K values. For a patient undergoing severe heart failure (Emax = 0.5), when K is less than or equal to 1.0, the control system will work out of the normal states and the data were over-adjusted. When 1.0 < K < 1.5, AOP, AOF, and
tended to stabilize, but as the K value increased, the Frank–Starling-like control baseline CL
n tended to be flatter concerning smaller preload, resulting in a decrease in average pump flow. When K ≥ 1.7, severe oscillations were observed in
. Thus, when the patient undergoes severe heart failure, this paper recommends the K value to be about 1.3. When the patient experiences moderate heart failure, as indicated in
Figure 5b, K ≤ 0.5, and the data are over-adjusted. For 0.5 < K < 1.3, AOP, AOF, and
tend to stabilize. Similarly,
gradually decreases with the increase in the K value. For K ≥ 1.3, the system data oscillates. When the patient experiences moderate heart failure, the K value of around 1.0 is recommended in this article. When the patient undergoes mild heart failure, in
Figure 5c, and 0.8 < K < 1.5, AOP, AOF, and
are relatively stable.
For K ≥ 1.5, the system would shock. In the case of mild heart failure, this paper suggests that the optimal K value was around 0.8.
4. Discussion
The NAC-FSL controller not only solves the postoperative complications in the traditional control system, which uses invasive sensors but also helps to prevent suction by the control curve construction of Frank–Starling. Since the NAC-FSL controller includes a flat slope at high preload, over-pumping at the high preload can be prevented.
Compared to CSC, the NAC-FSL evaluated in this study is able to synchronize the systemic and pulmonary flow irrespective of variations in the venous return by emulating the Starling mechanism of the native’s heart. When changing from a resting state to an exercise state, the increase of the average pump flow in NAC-FSL reached 2.25 L/min, which is higher than CSC. For the closed state of the aortic valve, the cardiac output was found to be equal to the pump flow. Therefore, it was concluded that the system under NAC-FSL could provide more cardiac output and meet the perfusion requirements under various physiological states. When changing from the resting to exercise state, the P-V loops under NAC-FSL shift to the left with a reduction in the area, and shift to the right with an increase in area under CSC. This means that the NAC-FSL system could unload the left ventricle effectively, so the left ventricle does less work. However, the CSC system under the exercise state could not help the effective unloading of the left ventricular. For matching the perfusion requirement in exercise, the left ventricle has to do more work, leading to the enlargement of the P-V loops.
Gaddum et al. (2014) utilized pulsatility-based controllers to imitate the native Starling flow sensitivity and proved that each hemodynamic parameter was superior to CSC [
21]. In the controller system, pump pulsatility is a consequence of LV contraction, which is dependent on the LV preload. When severe heart failure occurs, the contraction of the left ventricle is not sufficient to provide a suitable pulsatility index for this control system. When the speed of the motor increases with the patient’s perfusion requirement, the unloading effect of the left ventricle becomes more obvious, and the contractility decreases accordingly.
To determine the patient’s working point OP
t in one cycle, the NAC-FSL control system proposed in this paper measured instantaneous preload instead of average preload. As a result, the system responded to the changes in the physiological state of the patient in time. Mahdi Mansouri et al. proposed a preload-based Frank–Starling system where they measured average preload to determine the patient’s working point and cost for at least two cycles and could not successfully respond to changes in the physiological state of the patient in time [
18].
The NAC-FSL control system still had some problems that needed to be addressed. When setting the reference CVS to obtain a patient’s pathological preload, it is mandatory to obtain a large amount of information from the patient to fit into the patient’s cardiovascular model. Moreover, when the control system changes from resting to exercise state, the NAC-FSL has higher fluctuation than CSC. One reason may be the non-real-time control method. This issue needs to be solved in a future study.
In this study, the effect of K on control robustness and hemodynamics was investigated and appropriate K values were determined in the NAC-FSL control system. K value is always used to indicate preload sensitivity. The K value might be determined by the physiological states, the level of heart failure, and various other parameters. However, the appropriate way of selecting the K value remains uncertain. When designing and utilizing physiological control systems based on the Frank–Starling mechanism, the determination of the K value is crucial and needs to be solved. At each level of heart failure (mild, moderate, and severe), if the K is too small, the control system overshoots, and the motor speed goes out of control. As the K value increases, the waveform of parameters gradually becomes stable, but the error between and becomes larger, thereby compromising the accuracy of the controller. When K exceeds a predefined limit, the hemodynamic system parameters severely oscillate, and the unstable system is unable to adjust the LVAD motor speed to meet the perfusion requirement. By considering the stability, error, and overshoot of the control system, the optimal range of the K value under different degrees of heart failure was suggested in this paper. The K values in three grades of heart failure (mild, moderate, and severe) were recommended to be around 1.3, 1.0, and 0.8, respectively. In this study, overshoot and oscillation were observed for inappropriate K values. These phenomena must be avoided to prevent accidents while using a preload physiological control system based on the Frank–Starling-like mechanism. Further work will focus on the validation of the K value in in vitro and in vivo experiments.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}