
Structural Design of Vascular Stents: A Review


Abstract
:1. Introduction
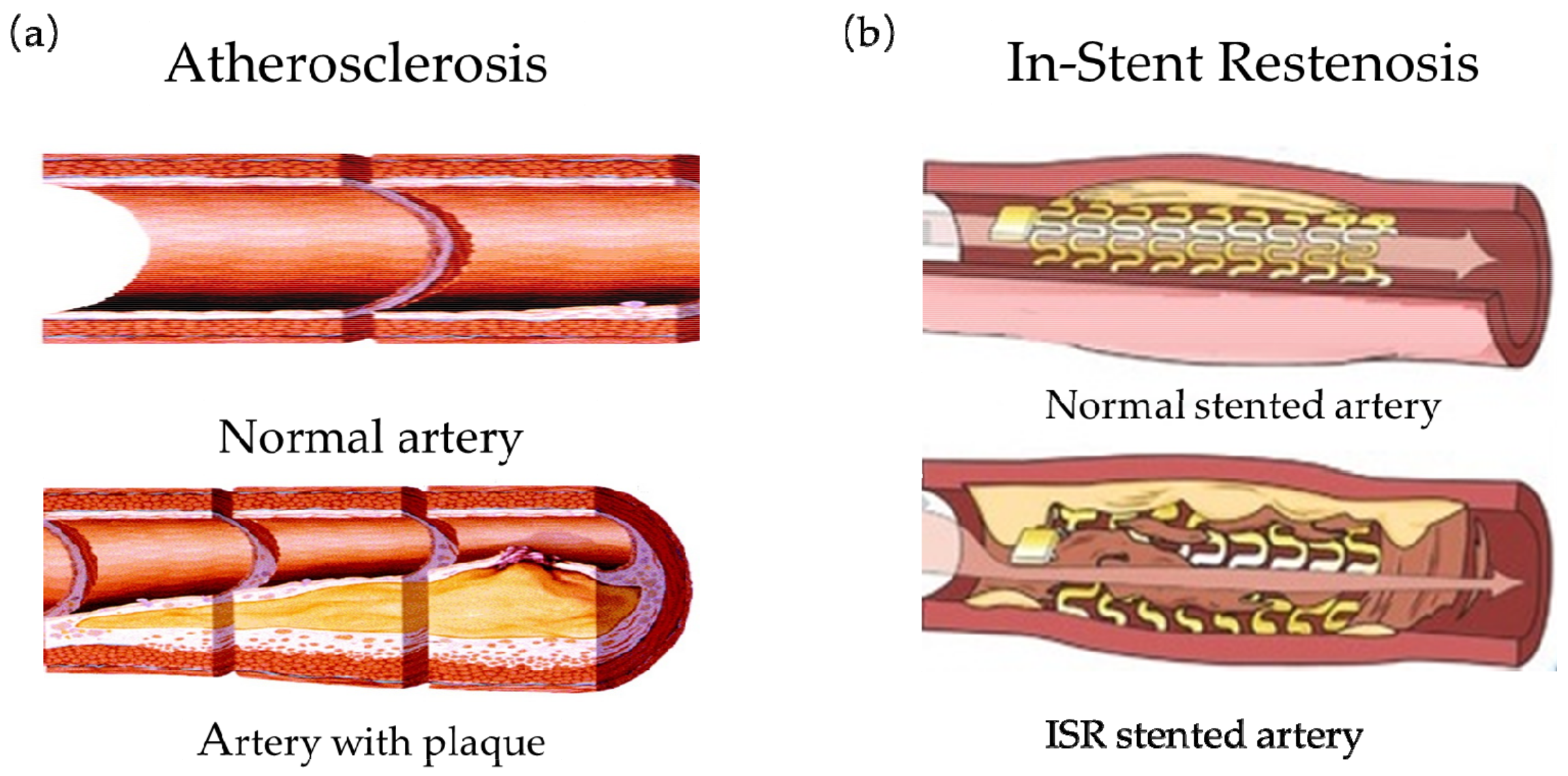
2. Introduction to the Vascular Stents
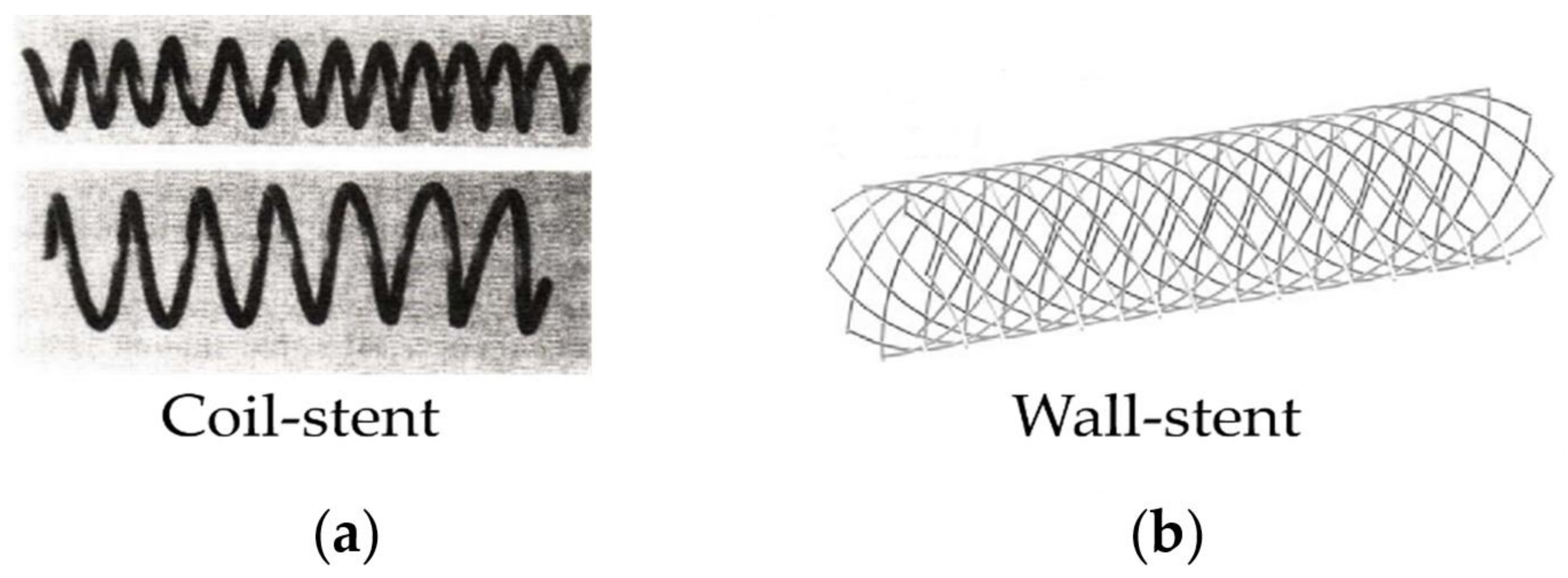
2.1. The First Generation of Vascular Stents: Bare Metal Stents (BMS)
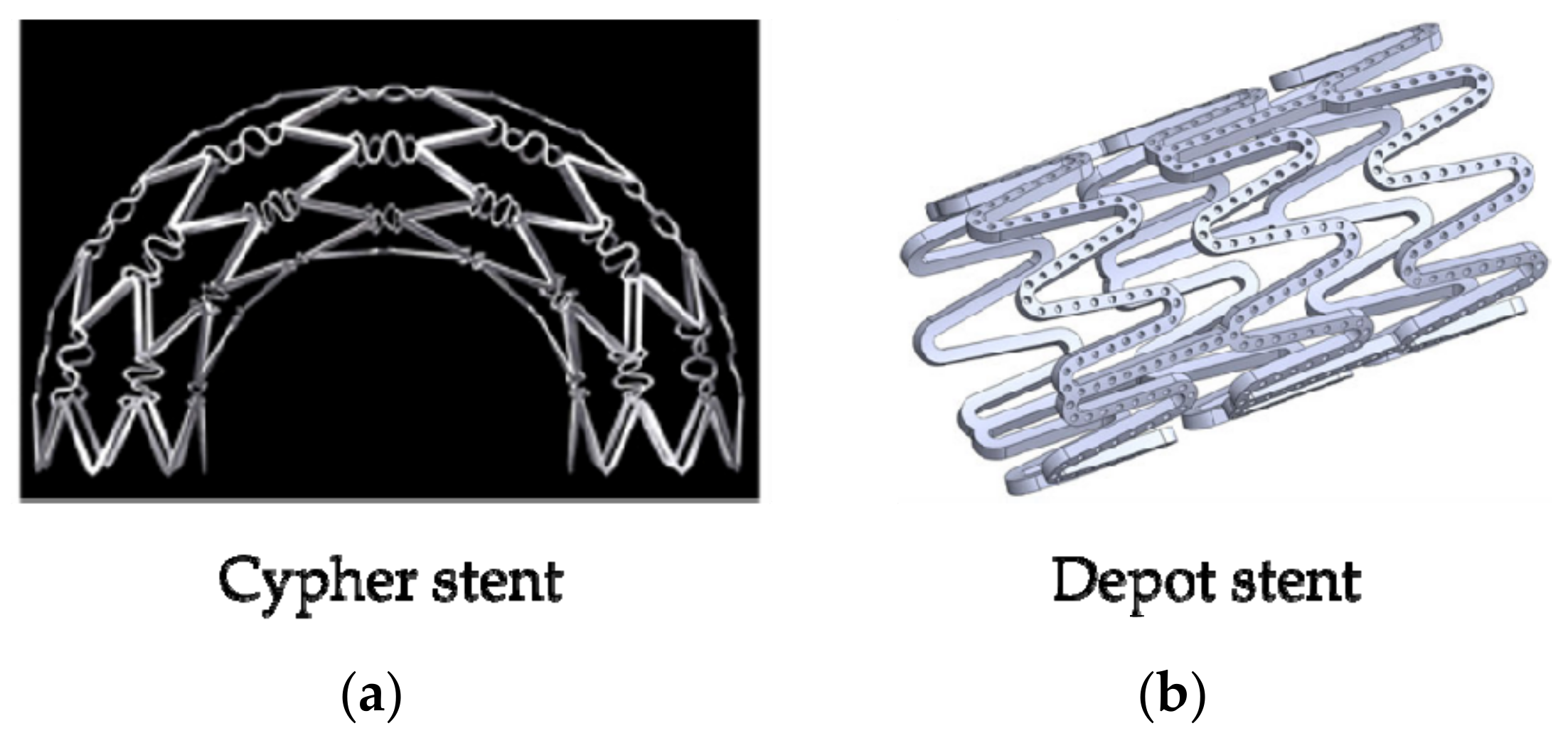
2.2. The Second Generation of Vascular Stent: Drug Eluting Stent (DES)
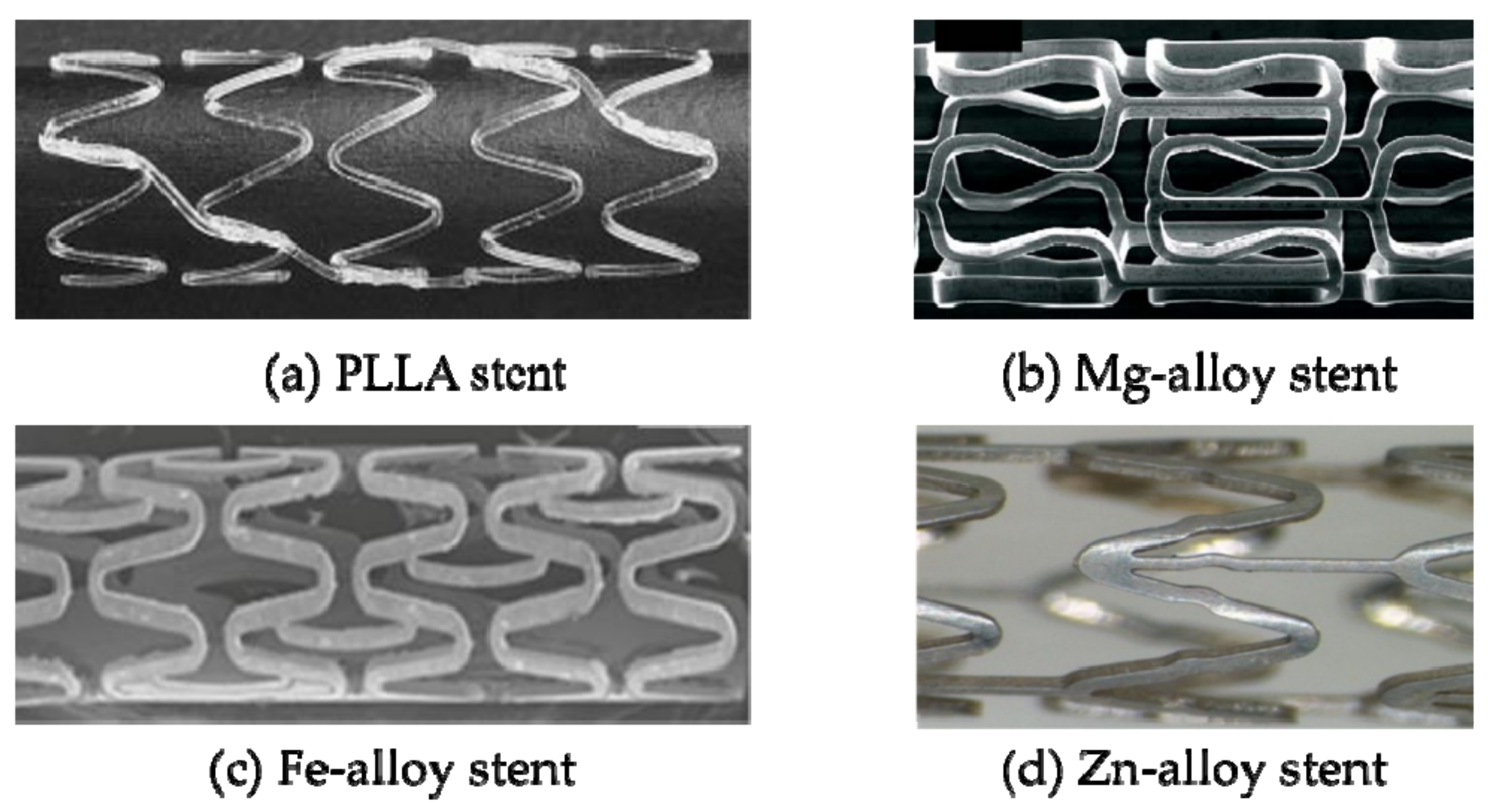
2.3. The Third Generation of Vascular Stent: Biodegradable Stent (BDS)
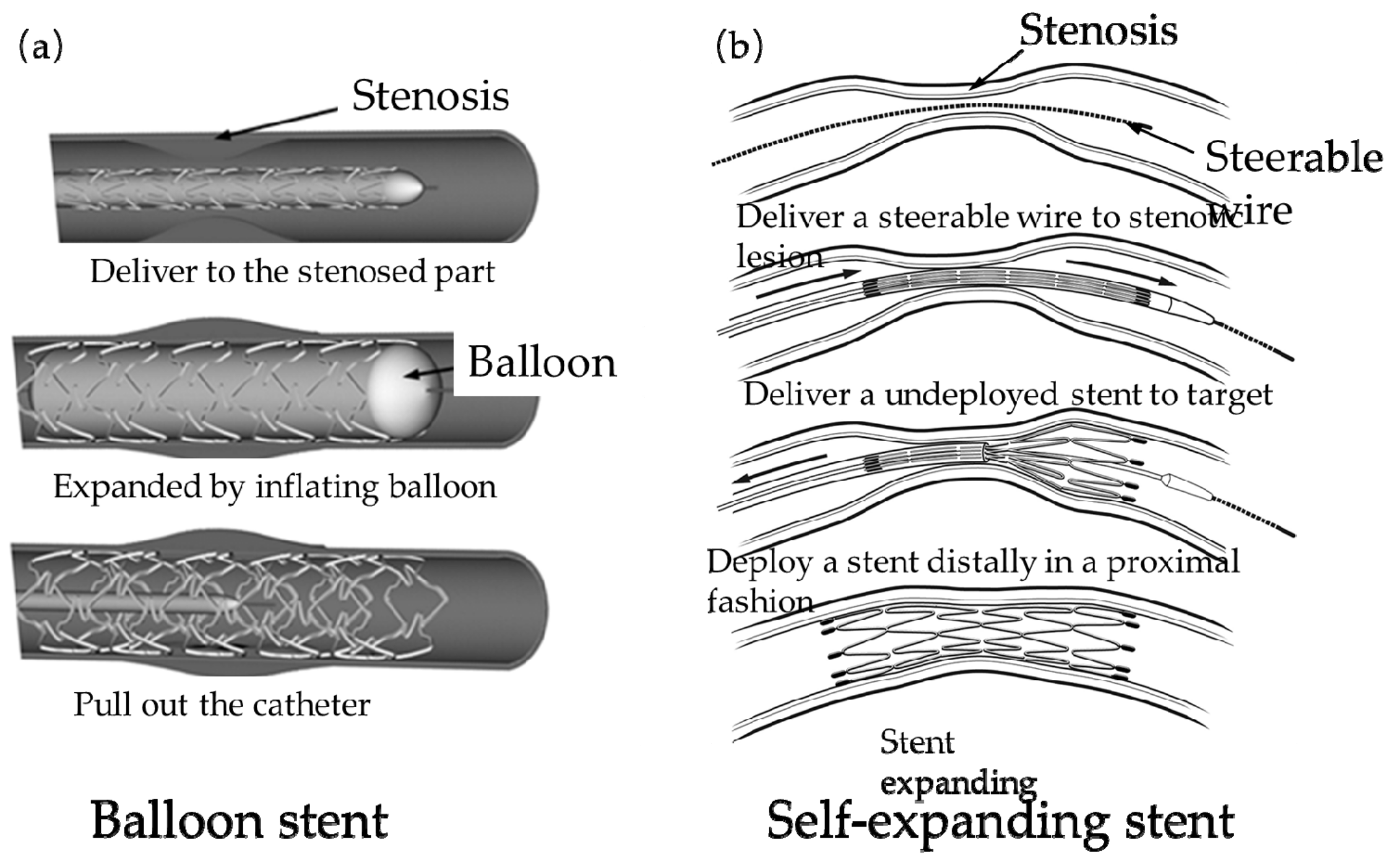
2.4. The Delivery Devices and Methods of Stents
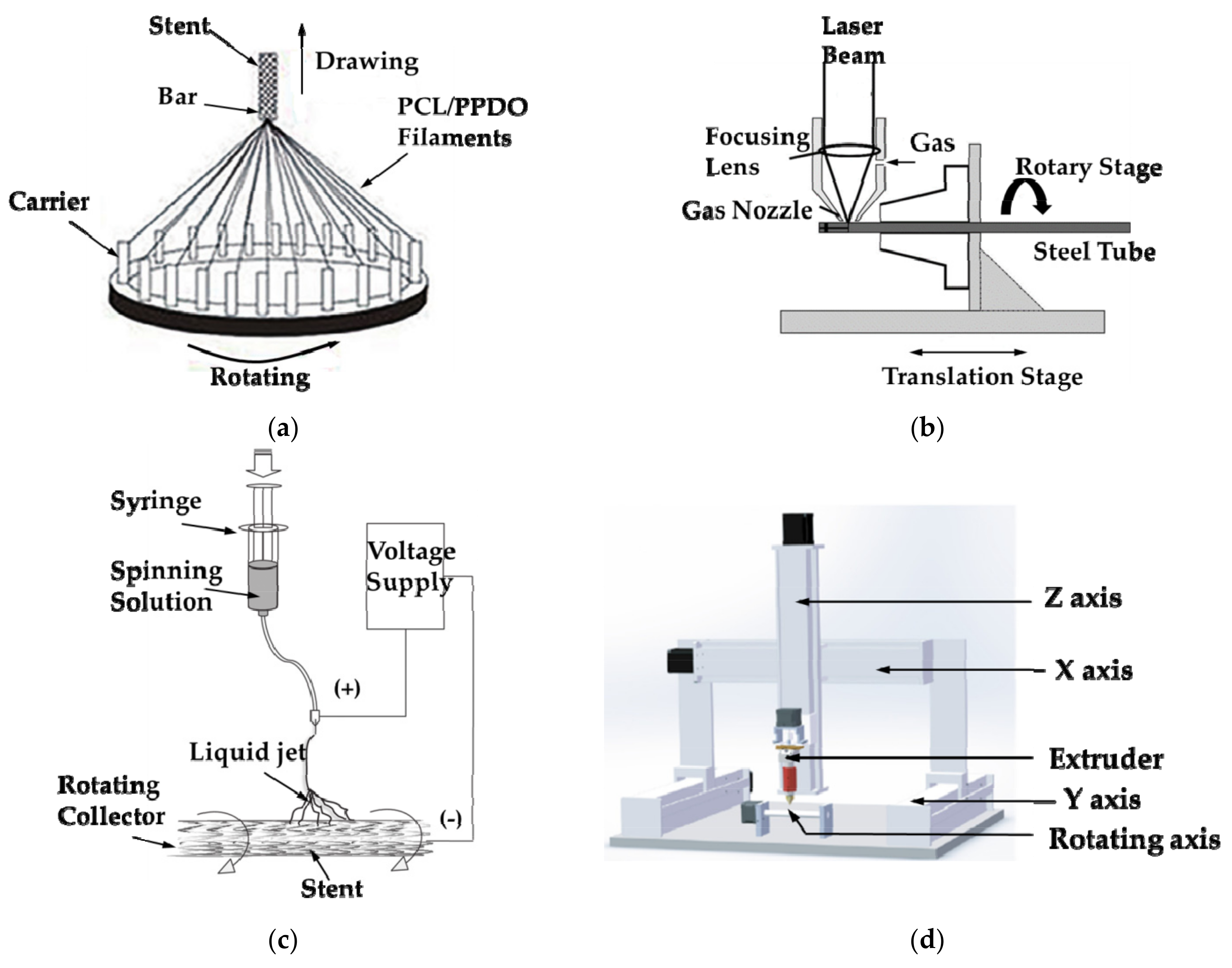
2.5. Introduction to the Manufacturing Method of Vascular Stents
3. Structure Design of Vascular Stents
3.1. Evaluation Standards of Mechanical Properties
3.1.1. Radial Stiffness or Radial Elastic-Recoil
3.1.2. Foreshortening
3.1.3. “Dogbone”
3.1.4. Axial Flexibility
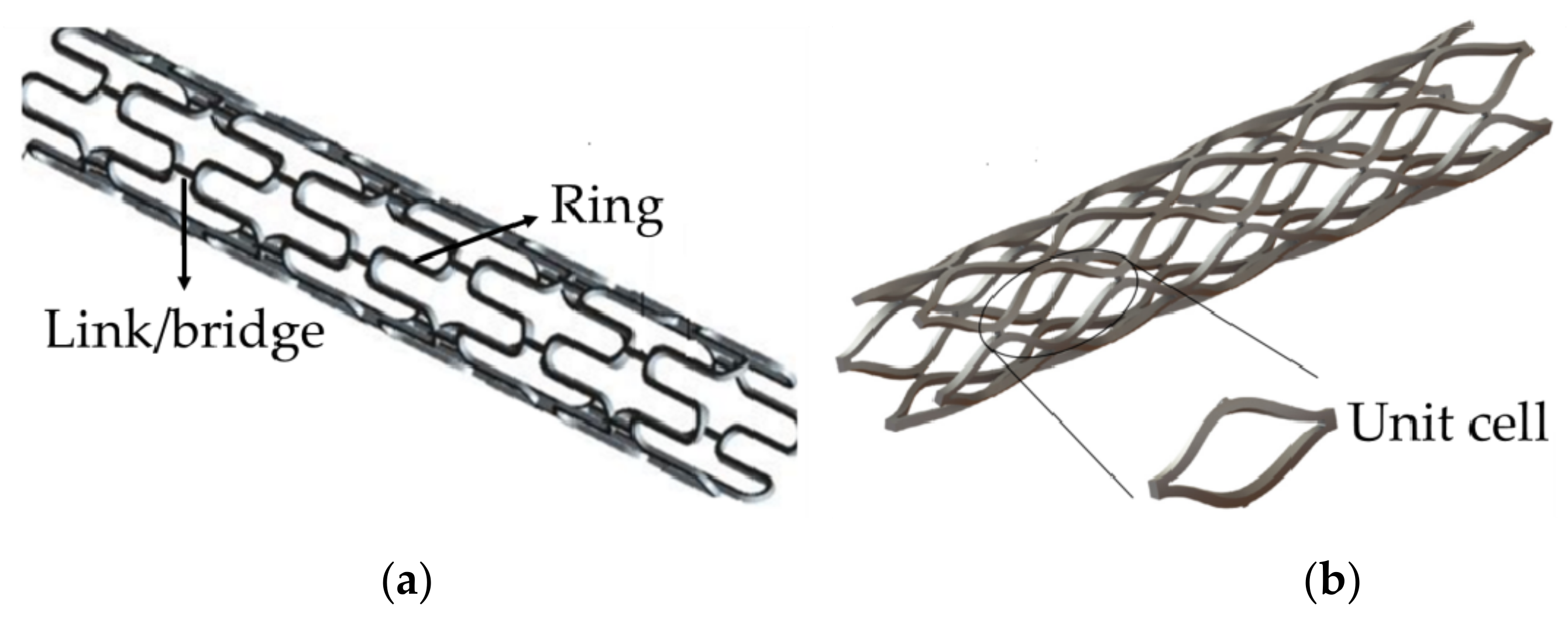
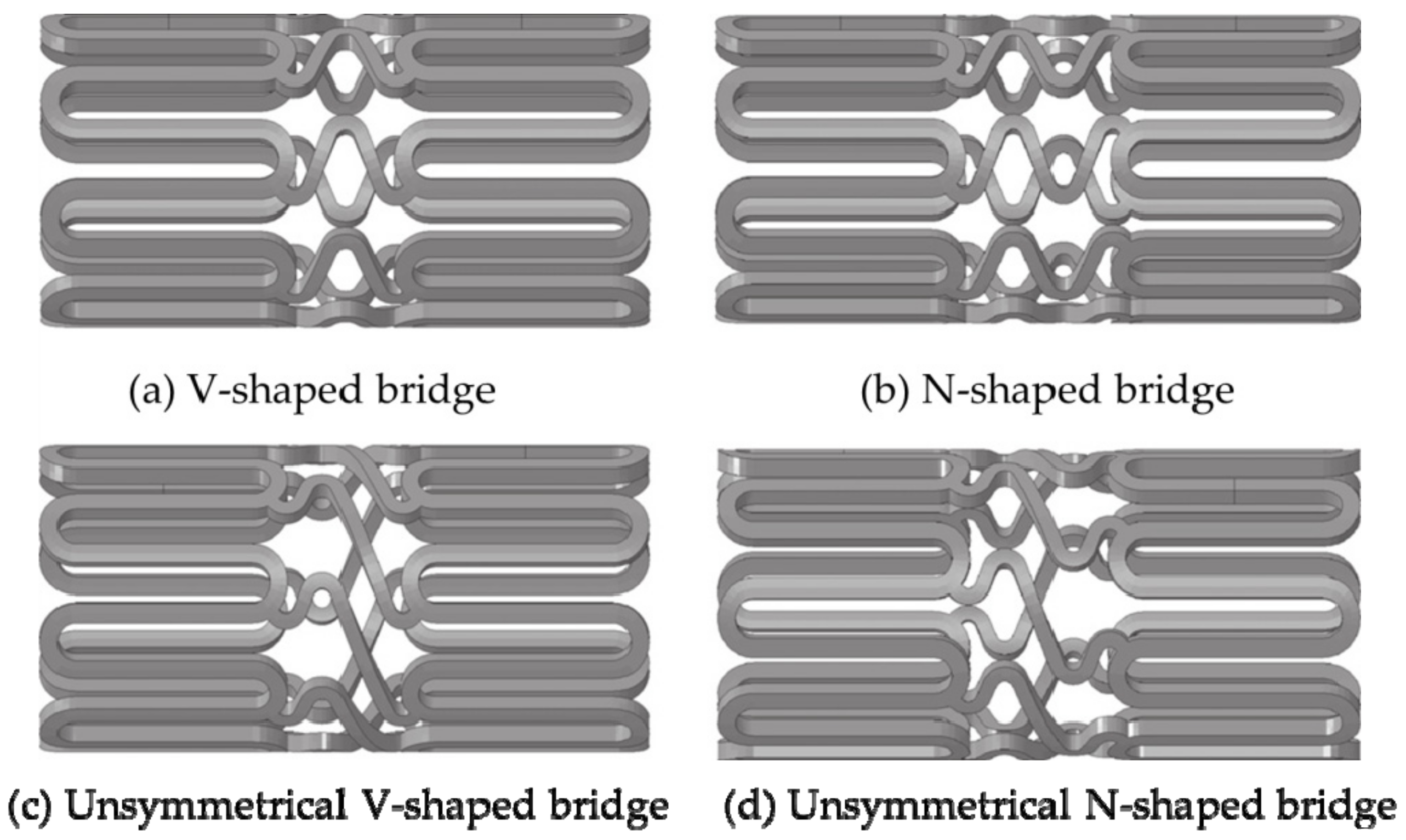
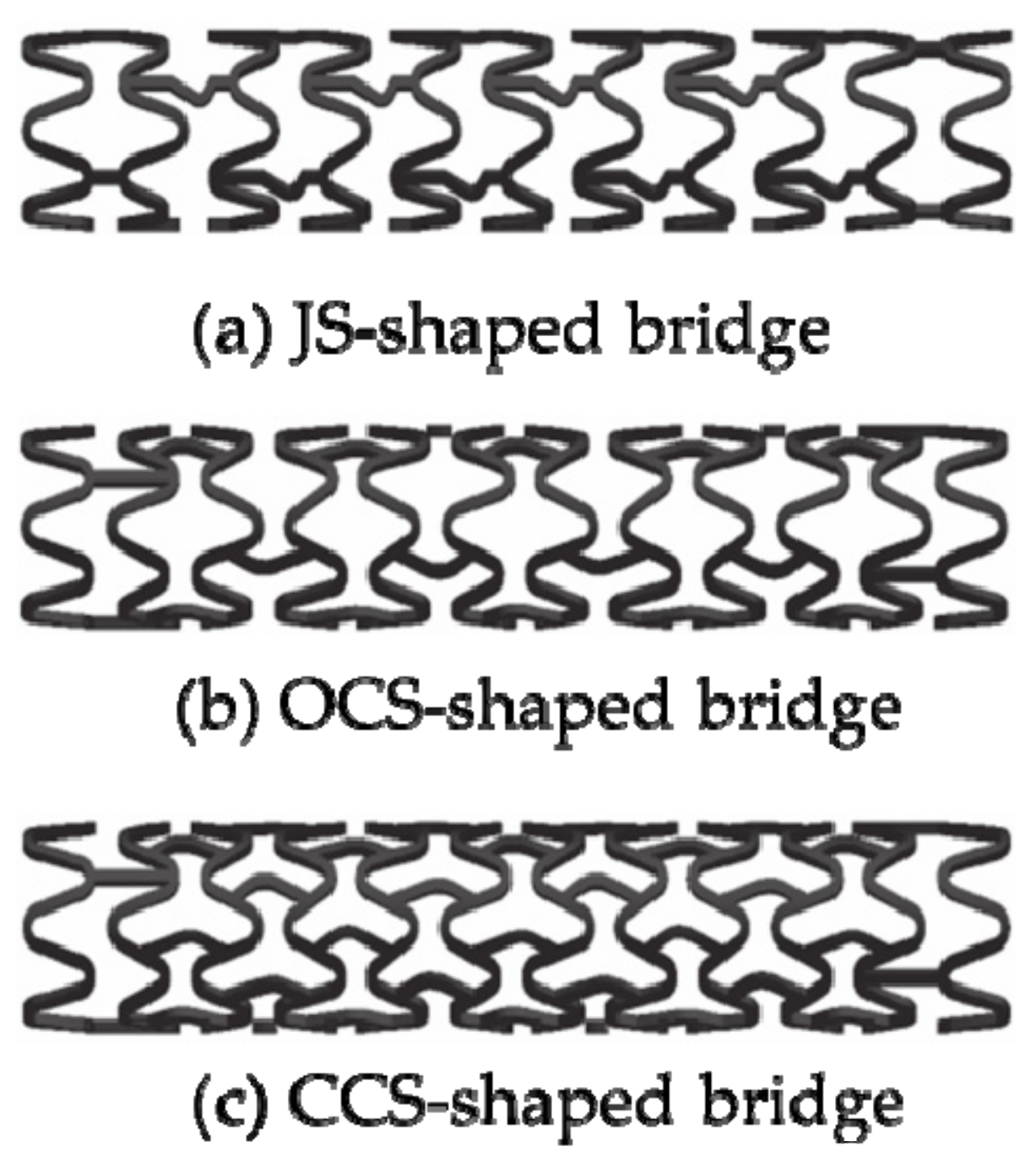
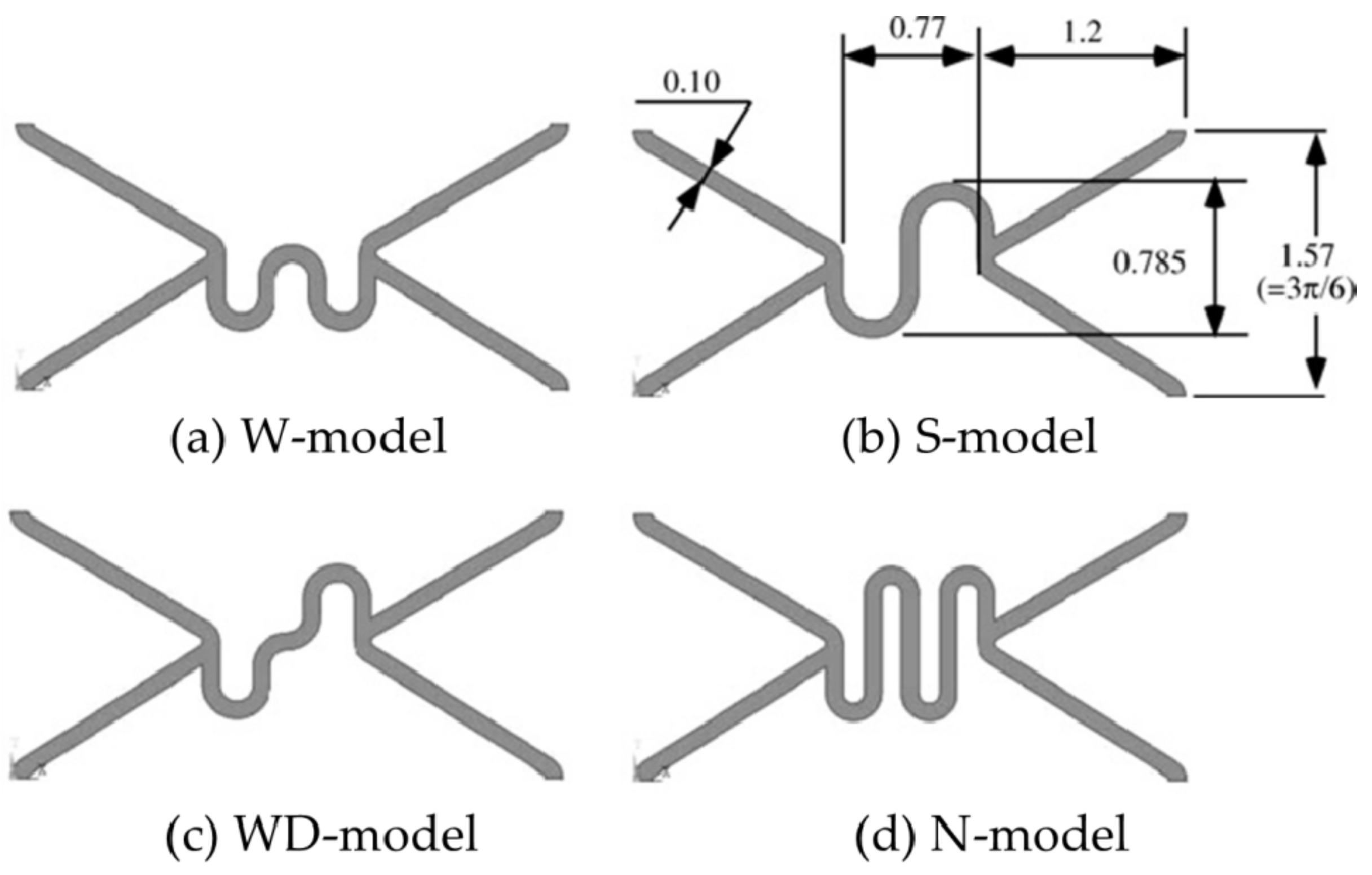
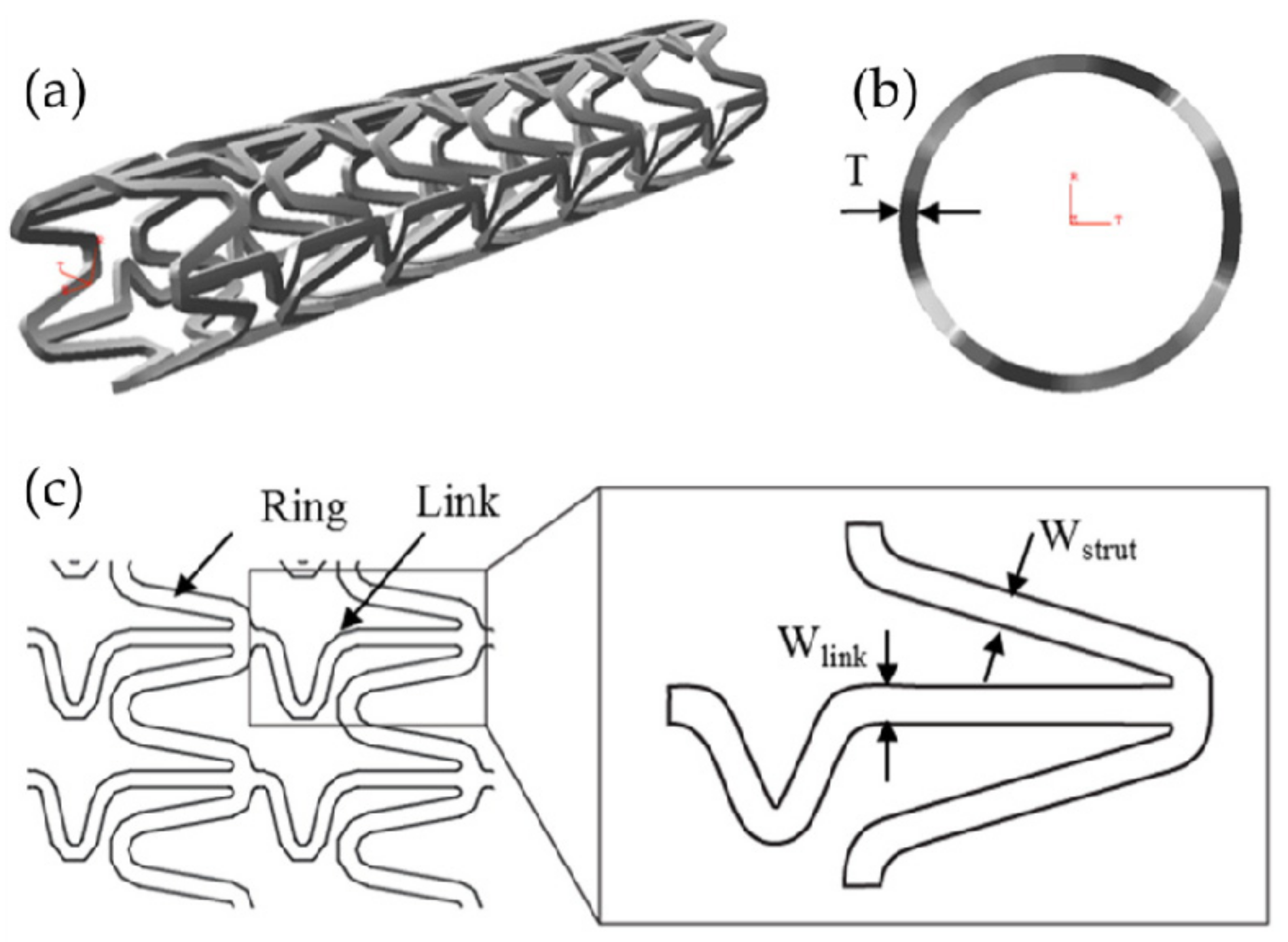
3.2. Design of “Bridge/Link” Stents
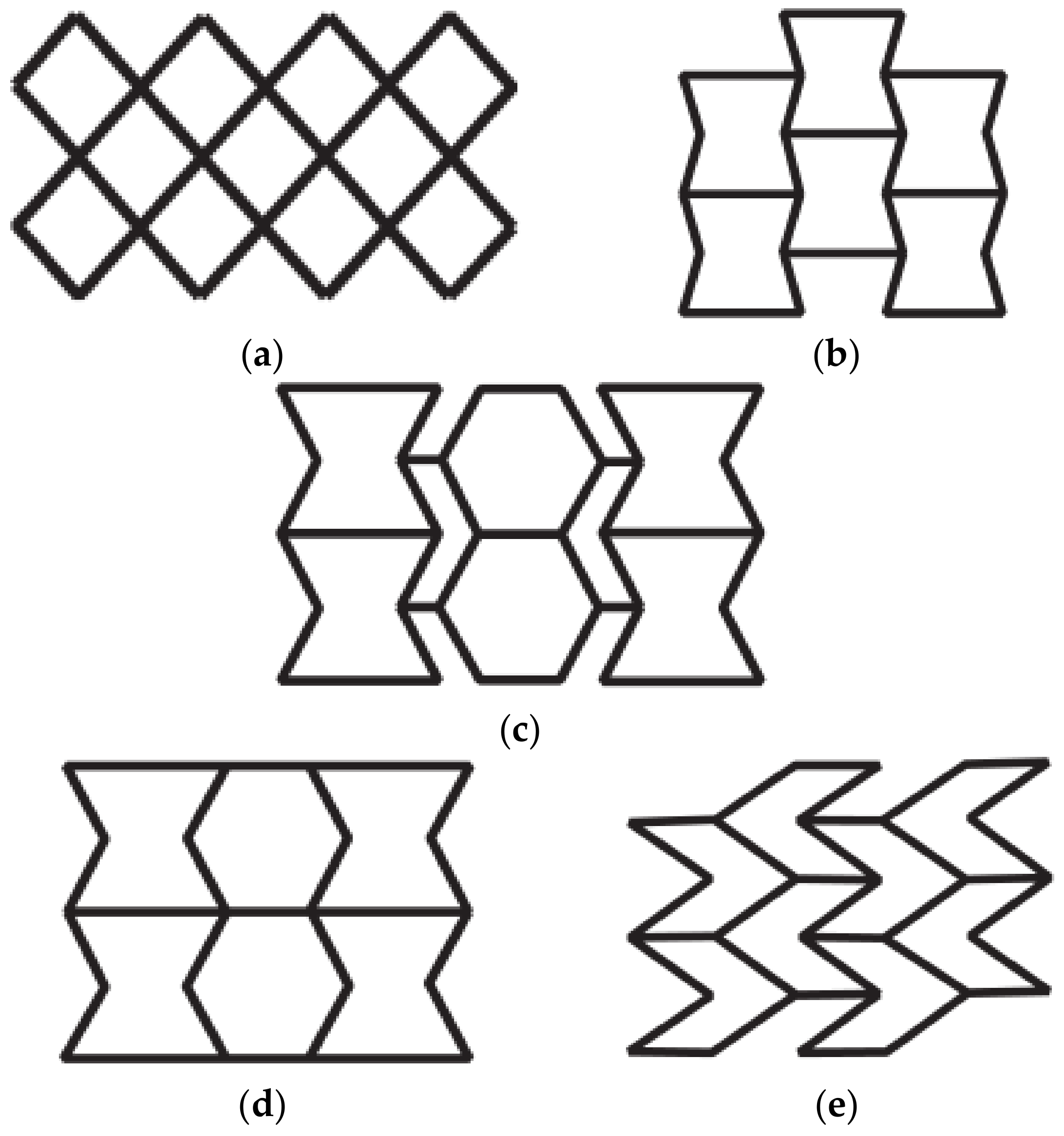
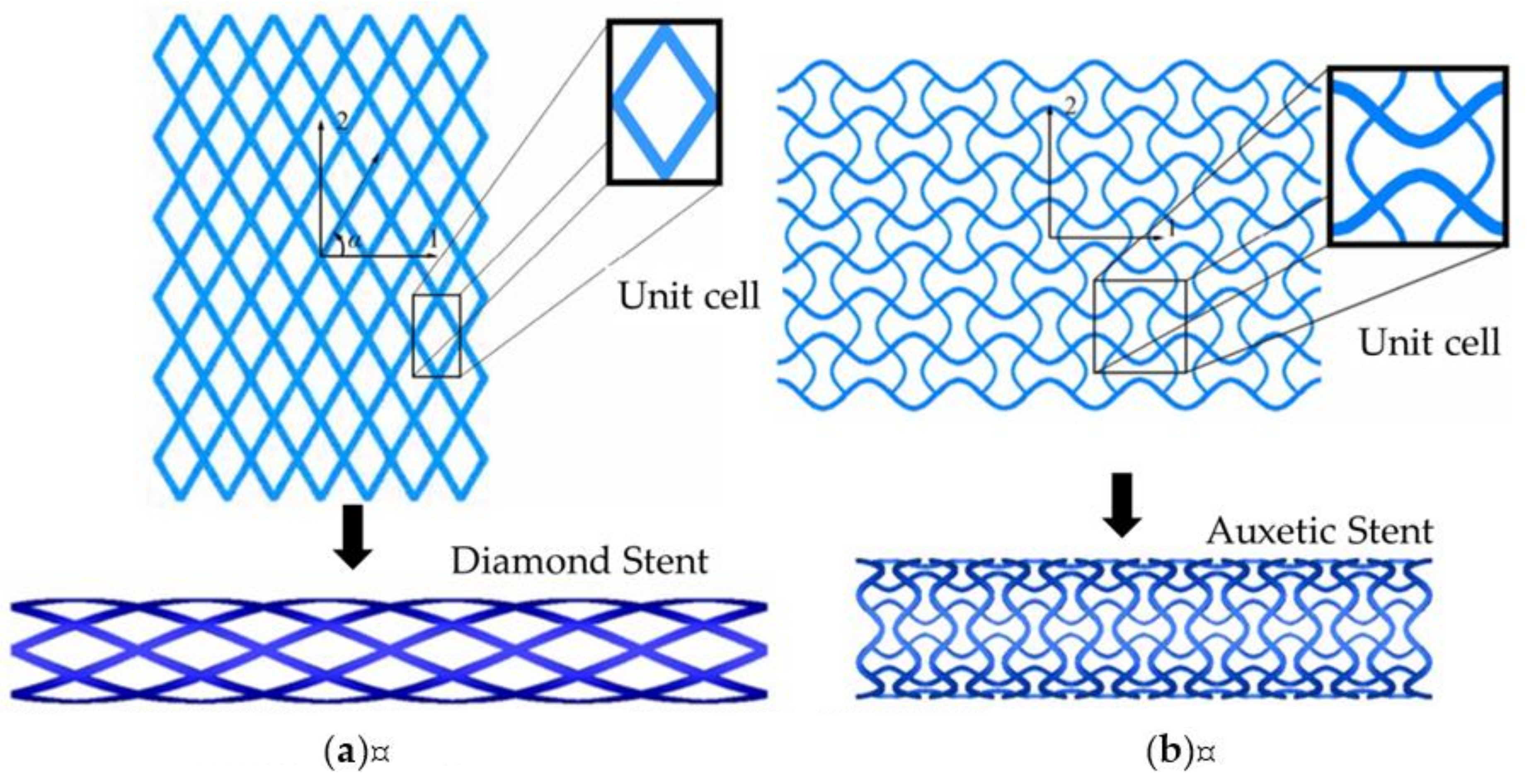
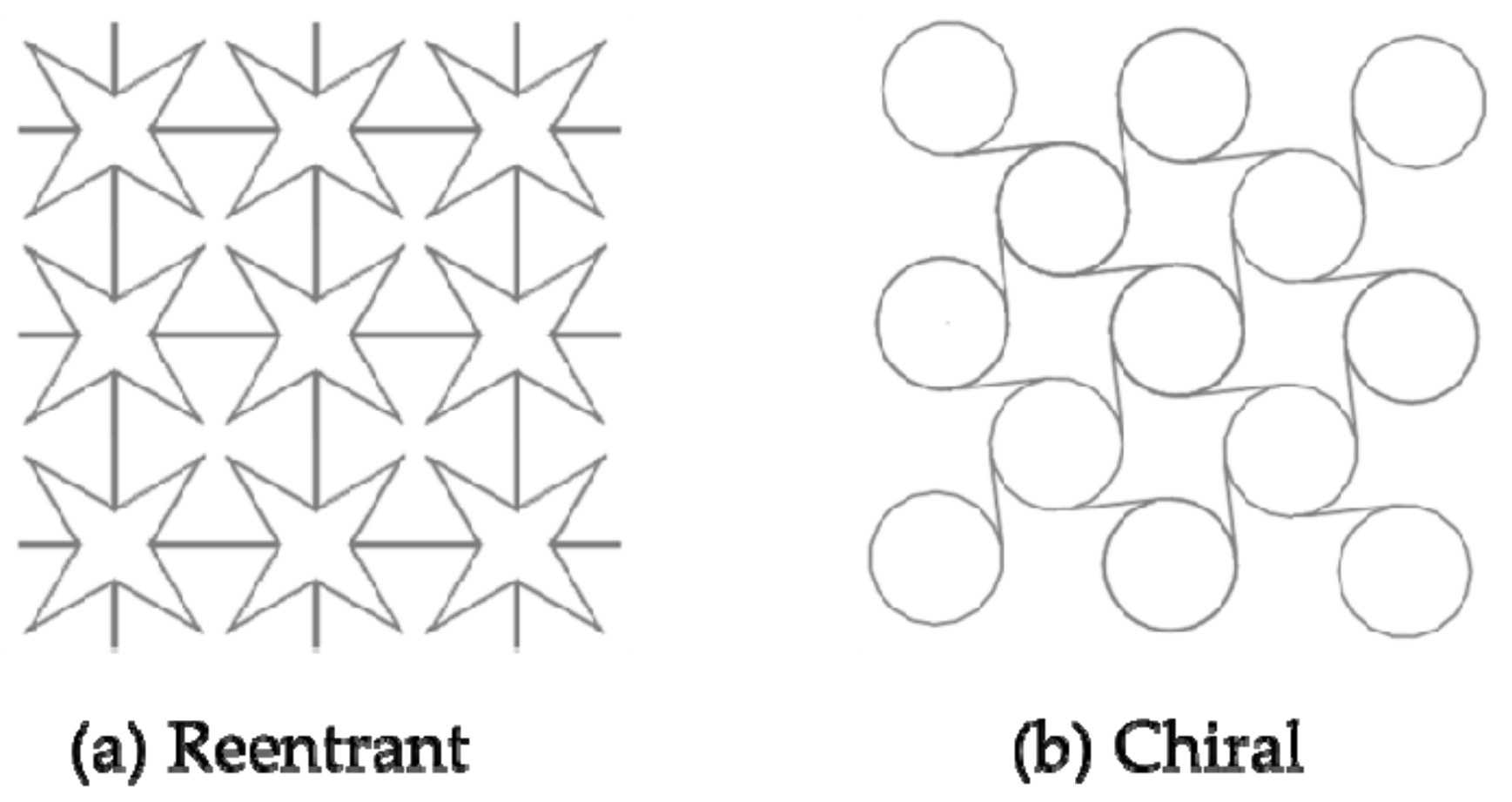
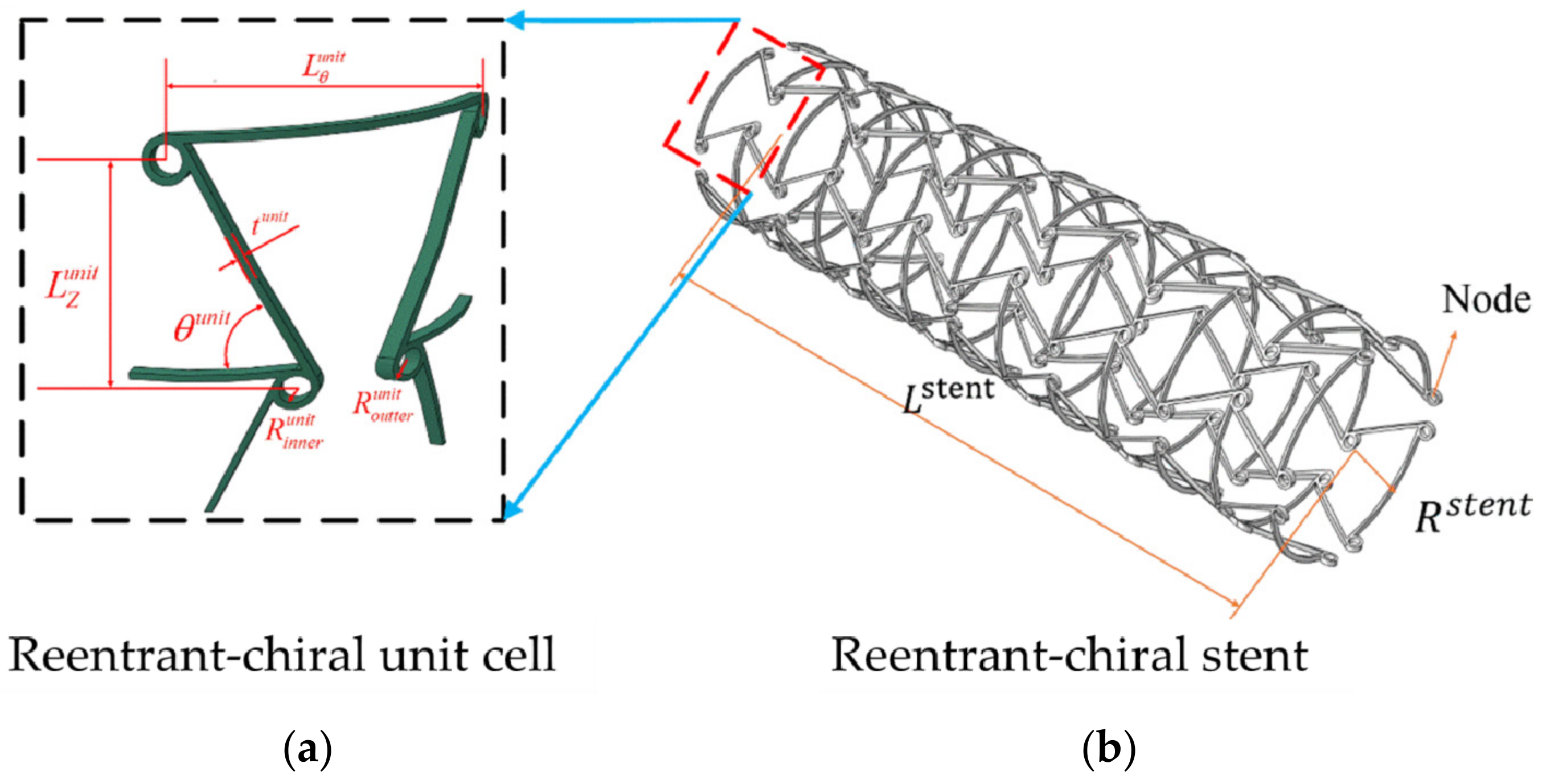
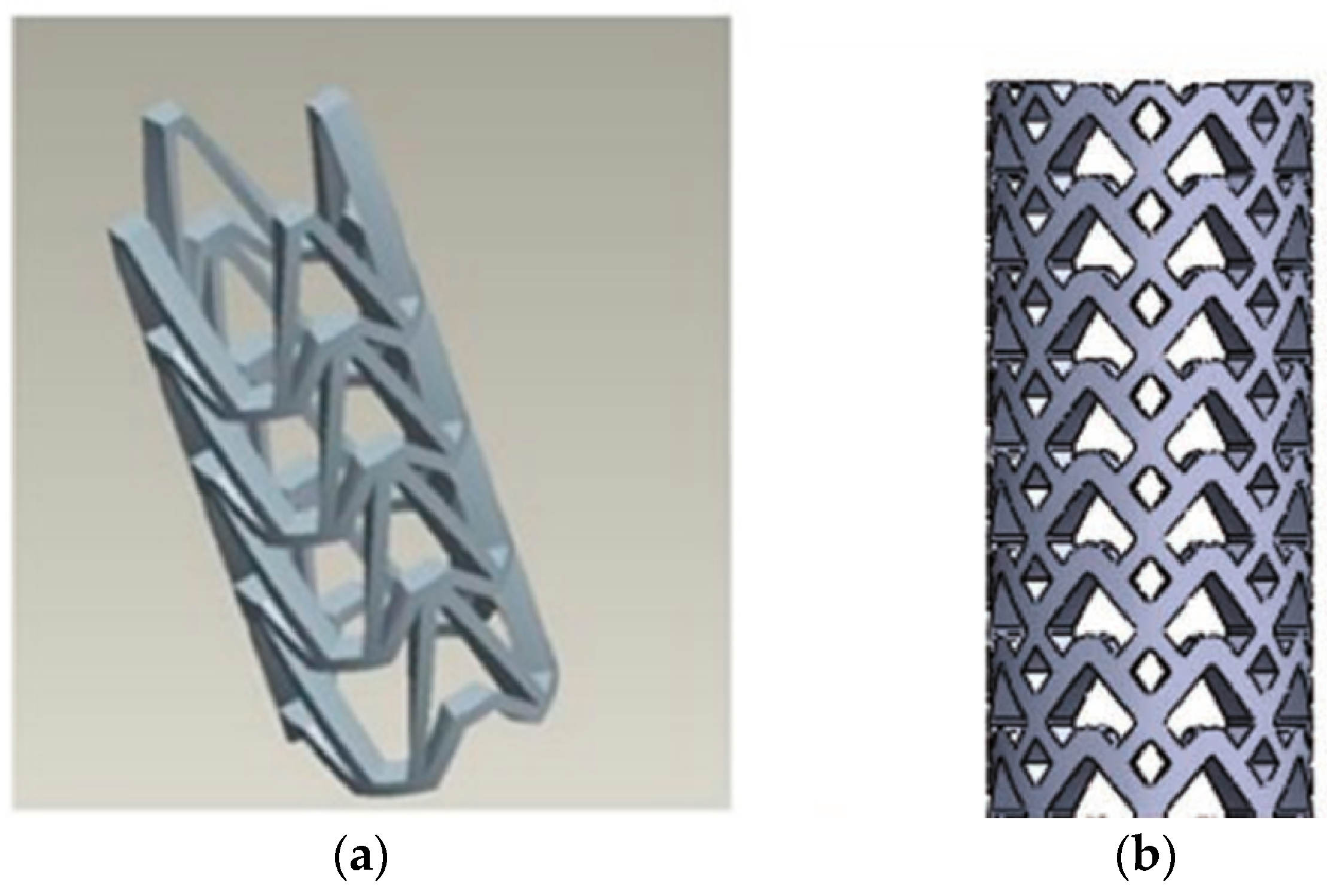
3.3. Design of RUC/RVE Stents
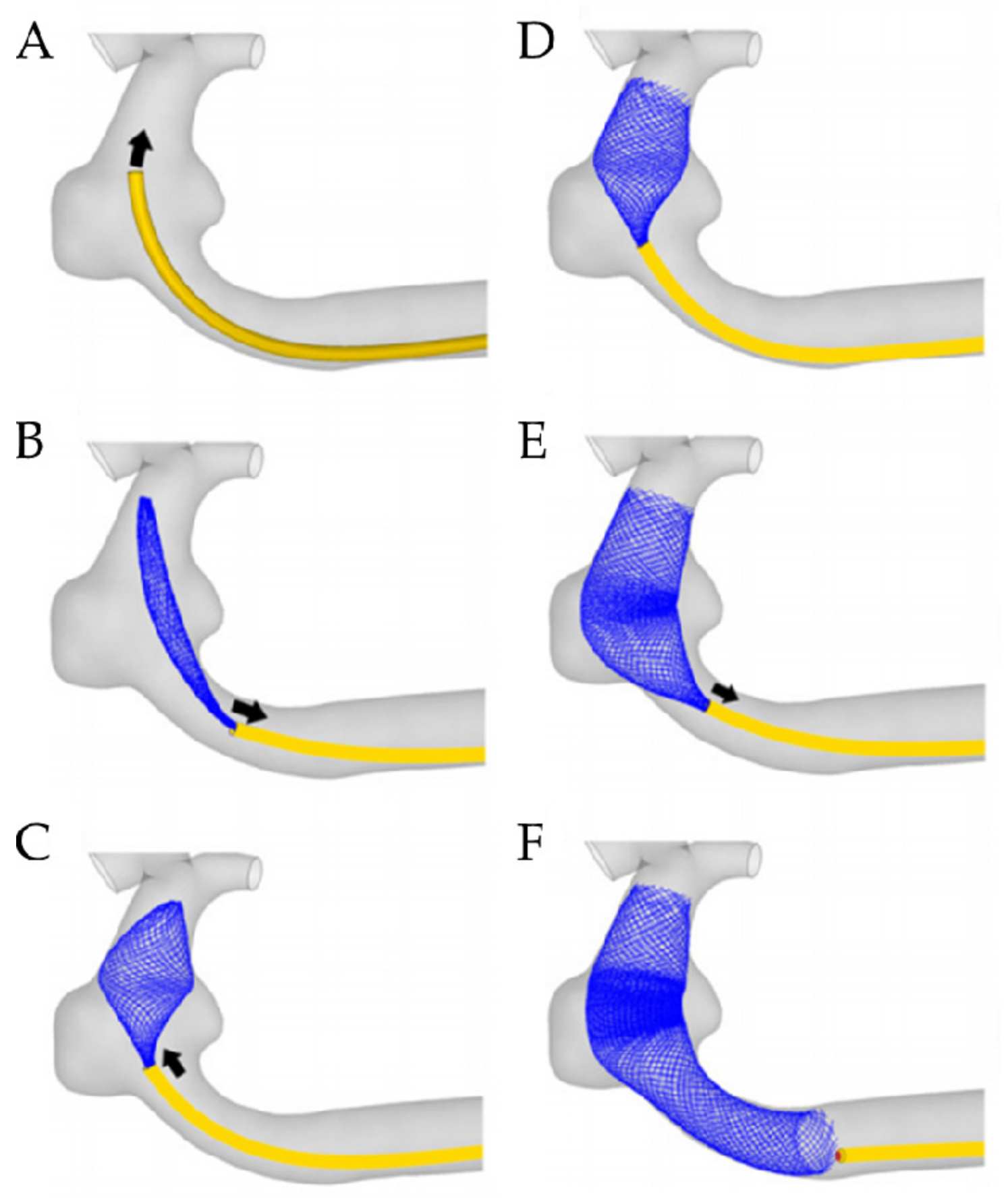
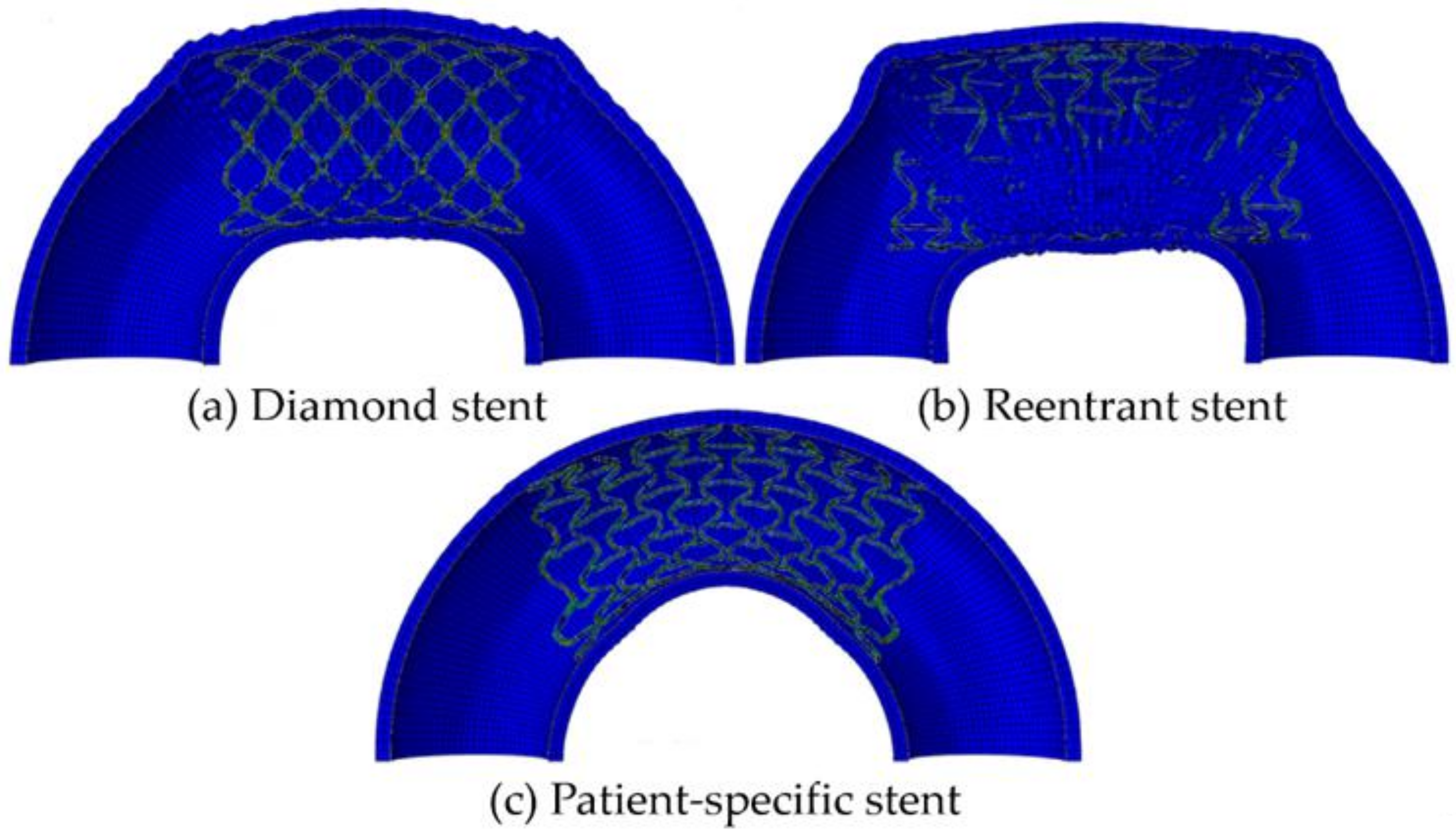
3.4. Design of Patient-Specific Stents
4. Perspectives on the Future and Challenges of Designing and Fabricating Stents
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

| Types of Stent | Advantages | Disadvantages |
|---|---|---|
| L-shaped bridge | Axial stiffness and flexibility [99] | |
| N-shaped bridge | Axial flexibility [92] | |
| Un/symmetrical N-shaped bridge | Axial flexibility [92] | |
| S-shaped bridge | Axial flexibility [101] | |
| symmetrical V-shaped bridge stent | Torsional performance [92] | |
| unsymmetrical V-shaped bridge | Axial flexibility [92] | |
| W-shaped bridge | Bending stiffness [104] | |
| WD-shaped bridge | Axial flexibility [104] | |
| JS-shaped bridge | Bending stiffness No axial foreshortening [102,103] | Radial strength [102,103] |
| CCS-shaped bridge | Radial strength No axial foreshortening [102,103] | |
| OCS-shaped bridge | Radial strength Bending stiffness No axial foreshortening [102,103] | |
| Diamond | Axial flexibility Axial foreshortening Radial recoil Radial stiffness [96,110,124] | |
| Auxetic | Radial stiffness Elastic recoil No axial foreshortening [110,111,115] | |
| Hybrid A | Radial stiffness Elastic recoil No axial foreshortening [96] | |
| Hybrid B | Elastic recoil No axial foreshortening [96] | Radial stiffness [96] |
| Chevron | Elastic recoil No axial foreshortening [96] | Radial stiffness [96] |
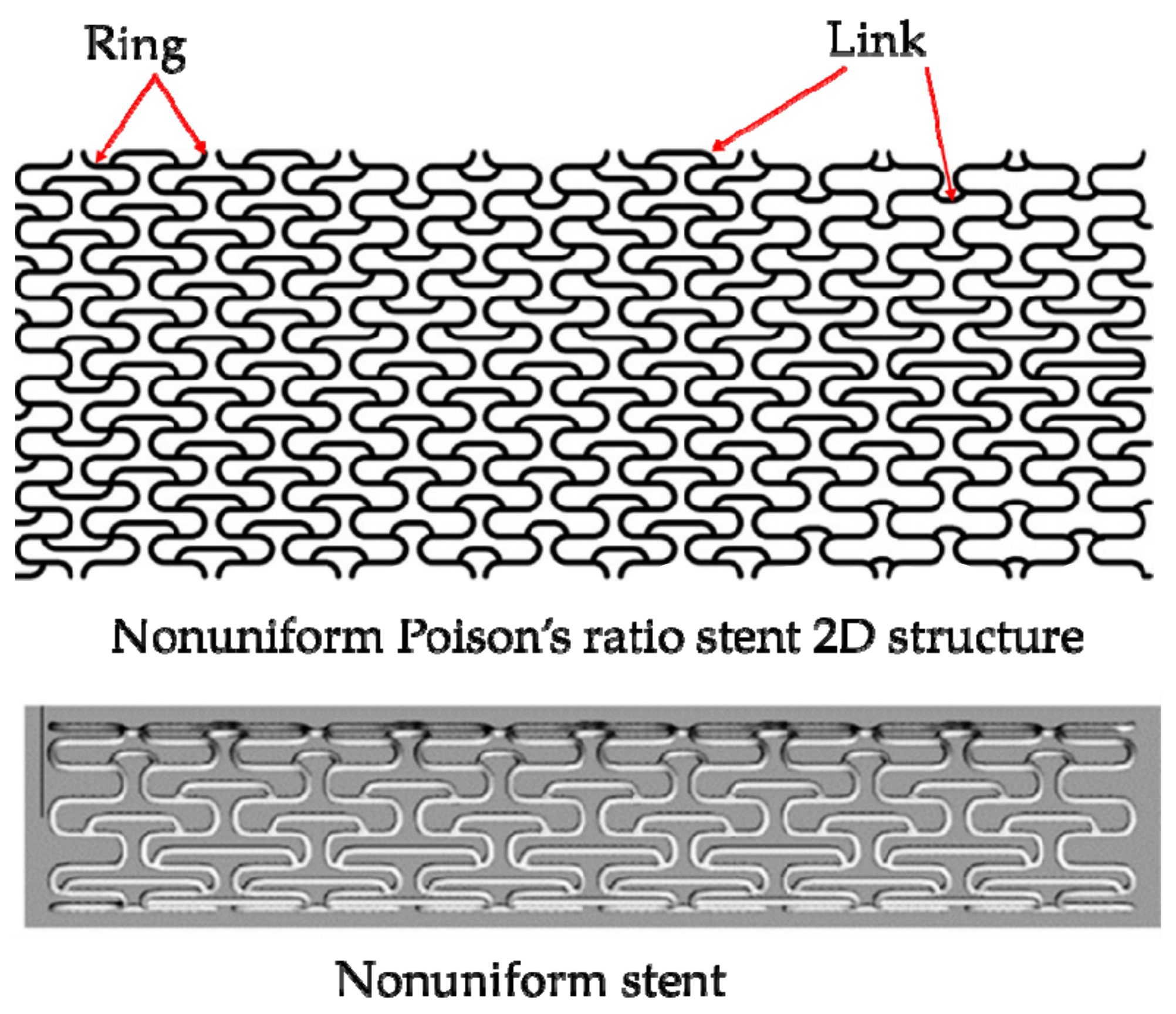
| Non-uniform Poisson’s ratio stent | Axial flexibility Radial stiffness Elastic recoil [124] No axial foreshortening |
References
- Sal, H.; Kara, B.; Krali, M.K. Focus on Coronary Atherosclerosis. In Atherosclerosis-Yesterday, Today and Tomorrow; Gianturco, L., Ed.; IntechOpen: Rijeka, Croatia, 2018; p. 7. [Google Scholar]
- Block, P.C. Percutaneous transluminal coronary angioplasty. Am. J. Roentgenol. 1980, 135, 955–959. [Google Scholar] [CrossRef] [PubMed]
- Landau, C.; Lange, R.A.; Hillis, L.D. Percutaneous Transluminal Coronary Angioplasty. N. Engl. J. Med. 1994, 330, 981–993. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.W.; Morice, M.C.; Kappetein, A.P.; Colombo, A.; Holmes, D.R.; Mack, M.J.; Ståhle, E.; Feldman, T.E.; Marcel, V.D.B.; Bass, E.J. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N. Engl. J. Med. 2009, 3, 961–972. [Google Scholar] [CrossRef] [PubMed]
- Migliavacca, F.; Petrini, L.; Colombo, M.; Auricchio, F.; Pietrabissa, R. Mechanical behavior of coronary stents investigated through the finite element method. J. Biomech. 2002, 35, 803–811. [Google Scholar] [CrossRef]
- Kumar, G.P.; Jafary-Zadeh, M.; Tavakoli, R.; Cui, F. Feasibility of using bulk metallic glass for self-expandable stent applications. J. Biomed. Mater. Res. Part B 2017, 105, 1874–1882. [Google Scholar] [CrossRef]
- Liu, Y.; Jie, Y.; Zhou, Y.; Jia, H. Structure Design of Vascular Stents. In Multiscale Simulations and Mechanics of Biological Materials, 1st ed.; Li, S.F., Qian, D., Eds.; Wiley: Hoboken, NJ, USA, 2013; pp. 310–317. [Google Scholar]
- Chen, X.; Assadsangabi, B.; Hsiang, Y.; Takahata, K. Enabling Angioplasty-Ready "Smart" Stents to Detect In-Stent Restenosis and Occlusion. Adv. Sci. 2018, 5, 1700560. [Google Scholar] [CrossRef]
- Schillinger, M.; Sabeti, S.; Dick, P. Sustained Benefit at 2 Years of Primary Femoropopliteal Stenting Compared with Balloon Angioplasty with Optional Stenting. Circulation 2007, 115, 2745–2749. [Google Scholar] [CrossRef]
- Schofer, J.; Schlüter, M.; Gershlick, A.H.; Wijns, W.; Garcia, E.; Schampaert, E.; Breithardt, G. Sirolimus-eluting stents for treatment of patients with long atherosclerotic lesions in small coronary arteries: Double-blind, randomised controlled trial (E-SIRIUS). Lancet 2003, 362, 1093–1099. [Google Scholar] [CrossRef]
- Moses, J.W.; Leon, M.B.; Popma, J.J.; Fitzgerald, P.G.; Kuntz, R.E. Sirolimus-Eluting Stents versus Standard Stents in Patients with Stenosis in a Native Coronary Artery. N. Engl. J. Med. 2003, 349, 1315–1323. [Google Scholar] [CrossRef] [Green Version]
- LaDisa, J.F.; Olson, L.E.; Molthen, R.C.; Hettrick, D.A.; Pratt, P.F.; Hardel, M.D.; Kersten, J.R.; Warltier, D.C.; Pagel, P.S. Alterations in wall shear stress predict sites of neointimal hyperplasia after stent implantation in rabbit iliac arteries. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, H2465. [Google Scholar] [CrossRef] [Green Version]
- Papafaklis, M.I.; Bourantas, C.V.; Theodorakis, P.E.; Katsouras, C.S.; Fotiadis, D.I.; Michalis, L.K. Relationship of shear stress with in-stent restenosis: Bare metal stenting and the effect of brachytherapy. Int. J. Cardiol. 2009, 134, 25–32. [Google Scholar] [CrossRef]
- Sanmartín, M.; Goicolea, J.; García, C.; García, J.; Crespo, A.; Rodríguez, J.; Goicolea, J.M. Influence of Shear Stress on In-Stent Restenosis: In Vivo Study Using 3D Reconstruction and Computational Fluid Dynamics. Rev. Española Cardiol. 2006, 59, 20–27. [Google Scholar] [CrossRef]
- Colombo, M.; He, Y.; Corti, A.; Gallo, G.; Ninno, F.; Casarin, S.; Rozowsky, J.M.; Migliavacca, F.; Berceli, S.; Chiastra, C. In-Stent Restenosis Progression in Human Superficial Femoral Arteries: Dynamics of Lumen Remodeling and Impact of Local Hemodynamics. Ann. Biomed. Eng. 2021, 1–16. [Google Scholar] [CrossRef]
- Kim, B.J.; Yoon, Y.; Lee, D.H.; Kang, D.W.; Kwon, S.U.; Kim, J.S. The shape of middle cerebral artery and plaque location: High-resolution MRI finding. Int. J. Stroke 2015, 10, 856–860. [Google Scholar] [CrossRef]
- Benndorf, G.; Claus, B.; Strother, C.M.; Chang, L.; Klucznik, R.P. Increased cell opening and prolapse of struts of a neuroform stent in curved vasculature: Value of angiographic computed tomography: Technical case report. Neurosurgery 2006, 58, Ons-E380. [Google Scholar]
- Dong, R.Q.; Jiang, W.T.; Zheng, T.H.; Yan, F.; Fan, Y.B. Numerical analysis on drug deposition from drug-eluting stents in curved artery. J. Med. Biomech. 2011, 26, 13–17. [Google Scholar]
- Gyöngyösi, M.; Yang, P.; Khorsand, A.; Glogar, D. Longitudinal straightening effect of stents is an additional predictor for major adverse cardiac events. Austrian Wiktor Stent Study Group and European Paragon Stent Investigators. J. Am. Coll. Cardiol. 2000, 35, 1580–1589. [Google Scholar] [CrossRef] [Green Version]
- Fam, J.M.; Ishibashi, Y.; Felix, C.; Zhang, B.C.; Diletti, R.; Mieghem, N.; Regar, E.; Domburg, R.; Onuma, Y.; Geuns, R.J. Conformability in everolimus-eluting bioresorbable scaffolds compared with metal platform coronary stents in long lesions. Int. J. Cardiovasc. Imaging 2017, 33, 1863–1871. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.; Wang, W.Q.; Yang, D.Z.; Qi, M. Stent expansion in curved vessel and their interactions: A finte element analysis. J. Biomech. 2007, 40, 2580–2585. [Google Scholar] [CrossRef]
- Kasiri, S.; Kelly, D.J. An Argument for the Use of Multiple Segment Stents in Curved Arteries. J. Biomech. Eng. 2011, 133, 084501. [Google Scholar] [CrossRef] [Green Version]
- Ichiro, S.; Akira, W.; Makoto, S. A Study on Designing Balloon Expandable Magnesium Alloy Stent for Optimization of Mechanical Characteristics. Proceedings 2018, 2, 523. [Google Scholar]
- Fiorella, D.; Levy, E.I.; Turk, A.S.; Albuquerque, F.C.; McDougall, C.G. US multicenter experience with the wingspan stent system for the treatment of intracranial atheromatous disease: Periprocedural results. Stroke 2007, 38, 881–887. [Google Scholar] [CrossRef] [Green Version]
- Stoeckel, D.; Bonsignore, C.; Duda, S. A survey of stent designs. Minim. Invasive Ther. Allied Technol. 2002, 11, 137–147. [Google Scholar] [CrossRef]
- Dotter, C.T.; Judkins, M.P. Percutaneous Transluminal Treatment of Arteriosclerotic Obstruction. Radiology 1965, 84, 631–643. [Google Scholar] [CrossRef]
- Dotter, C.T. Transluminally-placed coilspring endarterial tube grafts. Long-term patency in canine popliteal artery. Investig. Radiol. 1969, 4, 329–332. [Google Scholar] [CrossRef]
- Dotter, C.T.; Buschmann, R.W.; McKinney, M.K.; Rösch, J. Transluminal expandable nitinol coil stent grafting: Preliminary report. Radiology 1983, 147, 259–260. [Google Scholar] [CrossRef]
- Colombo, A.; Tobis, J. Techniques in Coronary Artery Stenting. Circulation 2000, 104, e68. [Google Scholar]
- Sigwart, U.; Puel, J.; Mirkovitch, V.; Joffre, F.; Kappenberger, L. Intravascular Stents to Prevent Occlusion and Re-Stenosis after Transluminal Angioplasty. N. Engl. J. Med. 1987, 316, 701–706. [Google Scholar] [CrossRef]
- Palmaz, J.C.; Richter, G.M.; Noeldge, G.; Schatz, R.A.; Robison, P.D.; Gardiner, G.A.; Becker, G.J.; Mclean, G.K.; Denny, D.F.; Lammer, J. Intraluminal stents in atherosclerotic iliac artery stenosis: Preliminary report of a multicenter study. Radiology 1988, 168, 727–731. [Google Scholar] [CrossRef]
- Günther, R.W.; Vorwerk, D.; Bohndorf, K.; Klose, K.C.; Kistler, D.; Mann, H.; Sieberth, H.G.; El-Din, A. Venous stenoses in dialysis shunts: Treatment with self-expanding metallic stents. Radiology 1989, 170, 401–405. [Google Scholar] [CrossRef]
- Kim, M.; Taulbee, D.; Tremmel, M.; Meng, H. Comparison of Two Stents in Modifying Cerebral Aneurysm Hemodynamics. Ann. Biomed. Eng. 2008, 36, 726–741. [Google Scholar] [CrossRef] [PubMed]
- Palmerini, T.; Biondi-Zoccai, G.; Riva, D.D.; Stettler, C.; Sangiorgi, D.; D’Ascenzo, F.; Kimura, P.T.; Briguotri, C.; Sabatè, M.; Kim, H.S.; et al. Stent thrombosis with drug-eluting and bare-metal stents: Evidence from a comprehensive network meta-analysis. Lancet 2012, 379, 1393–1402. [Google Scholar] [CrossRef]
- Kirtane, A.J.; Gupta, A.; Iyengar, S.; Moses, J.W.; Leon, M.B.; Applegate, R.; Brodie, B.; Hannan, E.; Harjai, K.; Jensen, L.O.; et al. Safety and efficacy of drug eluting and bare metal stents: Comprehensive meta-analysis of randomized trials and observational studies. Circulation 2009, 119, 3198–3206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douglas, J.S. Role of adjunct pharmacologic therapy in the era of drug-eluting stents. Atheroscler. Suppl. 2005, 6, 47–52. [Google Scholar] [CrossRef]
- Virmani, R. Localized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: Should we be cautious. Circulation 2004, 110, 701–705. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.N.; Zuo, M.C.; Zhang, S.X.; Wu, H.L.; Wang, W.H.; Chen, W.Z.; Ni, J.H. Advances in Clinical Research of Biodegradable Stents. Acta Metall. Sin. 2017, 53, 1215–1226. [Google Scholar]
- Yuan, F.; Pei, J.; Yuan, G.Y. A review on current clinical applications of biodegradable/bioresorbable drug-eluting scaffolds. J. Funct. Mater. 2018, 5, 05028–05034. [Google Scholar]
- Karjalainen, P.P.; Nammas, W.; Airaksinen, J.K.E. Optimal stent design: Past, present and future. J. Interv. Cardiol. 2014, 6, 29–44. [Google Scholar] [CrossRef]
- Lemos, P.A. Unrestricted Utilization of Sirolimus-Eluting Stents Compared With Conventional Bare Stent Implantation in the “Real World”: The Rapamycin-Eluting Stent Evaluated At Rotterdam Cardiology Hospital (RESEARCH) Registry. Circulation 2004, 109, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Serruys, P.W.; Onuma, Y.; Garg, S.; Vranckx, P.; Bruyne, B.D.; Morice, M.C.; Colombo, A.; Macaya, C.; Richardt, G.; Fajadet, J. 5-year clinical outcomes of the ARTS II (Arterial Revascularization Therapies Study II) of the sirolimus-eluting stent in the treatment of patients with multivessel de novo coronary artery lesions. J. Am. Coll. Cardiol. 2010, 55, 1093–1101. [Google Scholar] [CrossRef] [Green Version]
- Li, B. Development of imported drug eluting stent. Chin. J. Cardiovasc. Med. 2009, 14, 263–265. [Google Scholar]
- Hsiao, H.M.; Chiu, Y.H. Assessment of mechanical integrity for drug-eluting renal stent with micro-sized drug reservoirs. Comput. Methods Biomech. Biomed. Eng. 2012, 16, 1307–1318. [Google Scholar] [CrossRef]
- Ielasi, A.; Al-Lamee, R.; Colombo, A. Stent Thrombosis and Duration of Dual Antiplatelet Therapy. Curr. Pharm. Des. 2010, 16, 4052–4063. [Google Scholar] [CrossRef]
- Bourantas, C.V.; Onuma, Y.; Farooq, V.; Zhang, Y.; Serruys, P.W. Bioresorbable scaffolds: Current knowledge, potentialities and limitations experienced during their first clinical applications. Int. J. Cardiol. 2013, 167, 11–21. [Google Scholar] [CrossRef]
- Samochowiec, L.; Wójcicki, J.; Gregorczyk, K.; Szmatloch, E. Current status of bioresorbable scaffolds in the treatment of coronary artery disease. J. Am. Coll. Cardiol. 2014, 64, 2541–2551. [Google Scholar]
- Stack, R.S. New interventional technology. Am. J. Cardiol. 1988, 62, F12–F24. [Google Scholar]
- Chapman, G.D.; Gammon, R.S.; Bauman, R.P.; Stack, R.S. Intravascular stents. Trends Cardiovasc. Med. 1991, 1, 127–131. [Google Scholar] [CrossRef]
- Murphy, J.G.; Schwartz, R.S.; Huber, K.C.; Holmes, D.R. Polymeric stents: Modern alchemy or the future. J. Invasive Cardiol. 1991, 3, 144–148. [Google Scholar]
- Zheng, Y.F.; Yamg, H.T. Research Progress in Biodegradable Metals for Stent Application. Acta Metall. Sin. 2017, 53, 1227–1237. [Google Scholar]
- Yamawaki, T.; Shimokawa, H.; Kozai, T.; Miyata, K.; Higo, T.; Tanaka, E.; Egashira, K.; Shiraishi, T.; Tamai, H.; Igaki, K. Intramural delivery of a specific tyrosine kinase inhibitor with biodegradable stent suppresses the restenotic changes of the coronary artery in pigs in vivo. J. Am. Coll. Cardiol. 1998, 32, 780–786. [Google Scholar] [CrossRef] [Green Version]
- Tamai, K.; Igaki, E.; Kyo, K.; Kosuga, A.; Kawashima, S.; Matsui, H.; Komori, T.; Tsuji, S.; Motohara, S.; Uehata, H. Initial and 6-month results of biodegradable poly-l-lactic acid coronary stents in humans. Circulation 2000, 102, 399–404. [Google Scholar] [CrossRef] [Green Version]
- Erbel, R.; Mario, C.D.; Bartunek, J.; Bonnier, J.; Bruyne, B.D.; Eberli, F.R.; Erne, P.; Haude, M.; Heublein, B.; Horrigan, M. Temporary scaffolding of coronary arteries with bioabsorbable magnesium stents: A prospective, non-randomised multicentre trial. Lancet 2007, 369, 1869. [Google Scholar] [CrossRef]
- Moravej, M.; Mantovani, D. Biodegradable Metals for Cardiovascular Stent Application: Interests and New Opportunities. Int. J. Mol. Sci. 2011, 12, 4250–4270. [Google Scholar] [CrossRef] [Green Version]
- Hehrlein, C.; Björn, S.; Kress, N.; Arab, A.; Mühlen, C.; Bode, C.; Epting, T.; Haberstroh, J.; Mey, L.; Schwarzbach, H. Zn-alloy provides a novel platform for mechanically stable bioresorbable vascular stents. PLoS ONE 2019, 14, e0209111. [Google Scholar] [CrossRef]
- Abizaid, A.; Schofer, J.; Maeng, M.; Witzenbichler, B.; Botelho, R.; Ormiston, J.A.; Costa, R.A.; Costa, J.; Chamié, D.; Abizaid, A.; et al. TCT-610 Prospective, Multi-Center Evaluation of the DESolve Novolimus-Eluting Bioresorbable Coronary Scaffold: Imaging Outcomes and 2-Year Clinical Results. J. Am. Coll. Cardiol. 2014, 64, 610–637. [Google Scholar] [CrossRef] [Green Version]
- Ormiston, J.A.; Serruys, P.W.; Evelyn, R.; Dariusz, D.; Leif, T.; Webster, M.W.I.; Yoshinobu, O.; Garcia-Garcia, H.M.; Robert, M.G.; Susan, V. A bioabsorbable everolimus-eluting coronary stent system for patients with single de-novo coronary artery lesions (ABSORB): A prospective open-label trial. Lancet 2008, 371, 899–907. [Google Scholar] [CrossRef]
- Lin, W.; Qin, L.; Qi, H.; Zhang, D.; Zhang, G.; Gao, R.; Qiu, H.; Xia, Y.; Cao, P.; Wang, X. Long-term in vivo corrosion behavior, biocompatibility and bioresorption mechanism of a bioresorbable nitrided iron scaffold. Acta Biomater. 2017, 54, 454–468. [Google Scholar] [CrossRef]
- Lin, W.J.; Zhang, D.Y.; Zhang, G.; Sun, H.T.; Qi, H.P.; Chen, L.P.; Liu, Z.Q.; Gao, R.L.; Zheng, W. Design and characterization of a novel biocorrodible iron-based drug-eluting coronary scaffold-ScienceDirect. Mater. Des. 2016, 91, 72–79. [Google Scholar] [CrossRef]
- Peng, K.; Qiao, A. Structural design and mechanical analysis of a novel biodegradable zinc alloy stent. Comput. Model. Eng. Sci. 2018, 117, 17–28. [Google Scholar]
- Peng, K.; Li, J.; Wang, S.R.; Xia, J.; Qiao, A. Research Progress on the Structure Design and Optimization of Biodegradable Stents. Chin. J. Biomed. Eng. 2019, 38, 367–374. [Google Scholar]
- LaDisa, J.F. Stent design properties and deployment ratio influence indexes of wall shear stress: A three-dimensional computational fluid dynamics investigation within a normal artery. J. Appl. Physiol. 2004, 97, 424–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Gu, J.; Wang, M.; Zhao, D.; Bao, Z. Multi-objective optimization of coronary stent using Kriging surrogate model. Biomed. Eng. OnLine 2016, 15, 275–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, N.; Zhang, H.W. Optimization model of longitudinal flexibility of a coronary stent. Chin. J. Comput. Mech. 2011, 28, 315–319. [Google Scholar]
- Damiano, R.J.; Tutino, V.M.; Lamooki, S.R.; Paliwal, N.; Dargush, G.F.; Davies, J.M.; Siddiqui, A.H.; Meng, H. Improving accuracy for finite element modeling of endovascular coiling of intracranial aneurysm. PLoS ONE 2019, 14, e0226421. [Google Scholar] [CrossRef]
- Damiano, R.J.; Ma, D.; Xiang, J.; Siddiqui, A.H.; Snyder, K.V.; Meng, H. Finite element modeling of endovascular coiling and flow diversion enables hemodynamic prediction of complex treatment strategies for intracranial aneurysm. J. Biomech. 2015, 48, 3332–3340. [Google Scholar] [CrossRef] [Green Version]
- Damiano, R.J.; Tutino, V.M.; Paliwal, N.; Ma, D.; Davies, J.M.; Siddiqui, A.H.; Meng, H. Compacting a Single Flow Diverter versus Overlapping Flow Diverters for Intracranial Aneurysms: A Computational Study. Am. J. Neuroradiol. 2017, 38, 603–610. [Google Scholar] [CrossRef] [Green Version]
- Ma, D.; Dargush, G.F.; Natarajan, S.K.; Levy, E.I.; Siddiqui, A.H.; Meng, H. Computer modeling of deployment and mechanical expansion of neurovascular flow diverter in patient-specific intracranial aneurysms. J. Biomech. 2012, 45, 2256–2263. [Google Scholar] [CrossRef]
- Babiker, M.H.; Chong, B.; Gonzalez, L.F.; Cheema, S.; Frakes, D.H. Finite element modeling of embolic coil deployment: Multifactor characterization of treatment effects on cerebral aneurysm hemodynamics. J. Biomech. 2013, 46, 2809–2816. [Google Scholar] [CrossRef]
- Cai, Y.H.; Meng, Z.Y.; Jiang, Y.Q.; Zhang, X.L.; Yang, X.J.; Wang, S.Z. Finite Element Modeling and Simulation of the Implantation of Braided Stent to Treat Cerebral Aneurysm. Med. Nov. Technol. Devices 2020, 5, 100031. [Google Scholar] [CrossRef]
- Leng, X.C.; Yang, W.; Xu, J.; Jiang, Y.Q.; Zhang, X.L.; Xiang, J.P. Numerical simulation of patient-specific endovascular stenting and coiling for intracranial aneurysm surgical planning. J. Transl. Med. 2018, 16, 208. [Google Scholar] [CrossRef] [Green Version]
- Bock, S.D.; Iannaccone, F.; Santis, G.D.; Beule, M.D.; Van Loo, D.; Devos, D.; Vermassen, F.; Segers, P.; Verhegghe, B. Virtual evaluation of stent graft deployment: A validated modeling and simulation study. J. Mech. Behav. Biomed. 2012, 13, 129–139. [Google Scholar] [CrossRef]
- Gijsen, F.J.; Migliavacca, F.; Schievano, S.; Socci, L.; Petrini, L.; Thury, A.; Steen, A.F.C.D.; Serruys, P.W.; Dubini, G. Simulation of stent deployment in a realistic human coronary artery. Biomed. Eng. Online 2008, 7, 23. [Google Scholar] [CrossRef] [Green Version]
- Zhao, F.; Xue, W.; Wang, F.; Yu, C.; Xu, H.; Hao, Y.; Wang, L. A new approach to improve the local compressive properties of PPDO self-expandable stent. J. Mech. Behav. Biomed. 2017, 68, 318–326. [Google Scholar] [CrossRef]
- Nuutinen, J.P.; Clerc, C.; Reinikainen, R.; Törmälä, P. Mechanical properties and in vitro degradation of bioabsorbable self-expanding braided stents. J. Biomater. Sci. Polym. Ed. 2003, 14, 255–266. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.; Sun, K.; Bai, K.; Chen, S.; Wang, F.J.; Zhao, F.; Hong, N.C.; Hu, H.B. A novel braided biodegradable stent for use in congenital heart disease: Short-term results in porcine iliac artery. J. Biomed. Mater. Res. Part A 2019, 107, 1667–1677. [Google Scholar] [CrossRef]
- Ueng, K.C.; Wen, S.P.; Lou, C.W.; Lin, J.H. Stainless steel/nitinol braid coronary stents: Braiding structure stability and cut section treatment evaluation. J. Ind. Text. 2014, 45, 965–977. [Google Scholar] [CrossRef]
- Stępak, B.; Antończak, A.J.; Bartkowiak-Jowsa, M.; Filipiak, J.; Pezowicz, C.; Abramski, K.M. Fabrication of a polymer-based biodegradable stent using a CO2 laser. Arch. Civ. Mech. Eng. 2014, 14, 317–326. [Google Scholar] [CrossRef]
- Momma, C.; Knoop, U.; Nolte, S. Laser cutting of slotted tube coronary stents, State of the art and future developments. Prog. Biomed. Res. 1999, 4, 39–44. [Google Scholar]
- Kathuria, Y.P. Laser microprocessing of metallic stent for medical therapy. J. Mater. Process. Technol. 2005, 170, 545–550. [Google Scholar] [CrossRef]
- Meng, H.; Liao, J.; Zhou, Y.; Zhang, Q. Laser micro-processing of cardiovascular stent with fiber laser cutting system. Opt. Laser Technol. 2009, 41, 300–302. [Google Scholar] [CrossRef]
- Guerra, A.J.; Tejeda-Alejandre, R.; Rodríguez, C.A.; Ciurana, G. Electrospun Tubular Scaffold for Stenting Application: A Proof of Concept. Procedia Manuf. 2019, 41, 312–319. [Google Scholar] [CrossRef]
- Jungst, T.; Pennings, I.; Schmitz, M.; Rosenberg, A.J.W.P.; Groll, J.; Gawlitta, D. Heterotypic Scaffold Design Orchestrates Primary Cell Organization and Phenotypes in Cocultured Small Diameter Vascular Grafts. Adv. Funct. Mater. 2019, 29, 1905987. [Google Scholar] [CrossRef] [Green Version]
- Arafat, M.; Fouladian, P.; Blencowe, A.; Albrecht, H.; Garg, S. Drug-eluting non-vascular stents for localised drug targeting in obstructive gastrointestinal cancers. J. Control. Release 2019, 308, 209–231. [Google Scholar] [CrossRef]
- Heo, D.N.; Lee, J.B.; Bae, M.S.; Hwang, Y.S.; Kwon, K.H.; Kwon, K. Development of nanofiber coated indomethacin-eluting stent for tracheal regeneration. J. Nanosci. Nanotechnol. 2011, 11, 5711. [Google Scholar] [CrossRef]
- Guerra, A.J.; Cano, P.; Rabionet, M.; Puig, T.; Ciurana, J. 3D-Printed PCL/PLA Composite Stents: Towards a New Solution to Cardiovascular Problems. Materials 2018, 11, 1679. [Google Scholar] [CrossRef] [Green Version]
- Park, S.A.; Lee, S.J.; Lim, K.S.; Bae, I.H.; Lee, J.H.; Wan, D.K.; Jeong, M.H.; Park, J.K. In vivo evaluation and characterization of a bio-absorbable drug-coated stent fabricated using a 3D-printing system. Mater. Lett. 2015, 141, 355–358. [Google Scholar] [CrossRef]
- Zhao, D.; Zhou, R.; Sun, J.; Li, H.; Jin, Y. Experimental Study of Polymeric Stent Fabrication Using Homemade 3D Printing System. Polym. Eng. Sci. 2019, 59, 1122–1131. [Google Scholar] [CrossRef]
- Demir, A.G.; Previtali, B. Additive manufacturing of cardiovascular CoCr stents by selective laser melting. Mater. Des. 2017, 119, 338–350. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Zhang, L.; Fang, Y.; Sun, W. Design, Characterization, and 3D Printing of Cardiovascular Stents with Zero Poisson’s Ratio in Longitudinal Deformation. Engineering 2020. [Google Scholar] [CrossRef]
- Azaouzi, M.; Makradi, A.; Belouettar, S. Numerical investigations of the structural behavior of a balloon expandable stent design using finite element method. Comput. Mater. Sci. 2013, 72, 54–61. [Google Scholar] [CrossRef]
- Khosravi, A.; Akbari, A.; Bahreinizad, H.; Salimi Bani, M.; Karimi, A. Optimizing through computational modeling to reduce dogboning of functionally graded coronary stent material. J. Mater. Sci. Mater. Med. 2017, 28, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Bedoya, J.; Meyer, C.A.; Timmins, L.H.; Moreno, M.R.; Moore, J.E. Effects of Stent Design Parameters on Normal Artery Wall Mechanics. J. Biomech. Eng. 2006, 128, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Petrini, L.; Migliavacca, F.; Auricchio, F.; Dubini, G. Numerical investigation of the intravascular coronary stent flexibility. J. Biomech. 2004, 37, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Prithipaul, P.K.M.; Kokkolaras, M.; Pasini, D. Assessment of structural and hemodynamic performance of vascular stents modelled as periodic lattices. Med. Eng. Phys. 2018, 57, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, H.M.; Lin, C.H.; Liao, Y.C.; Chen, H.Y.; Wang, T.W. Hemodynamic Behavior of Coronary Stents in Straight and Curved Arteries. Curr. Nanosci. 2014, 10, 205–211. [Google Scholar] [CrossRef]
- Rieu, R.; Barragan, P.; Garitey, V.; Roquebert, P.O.; Fuseri, J.; Commeau, P.; Sainsous, J. Assessment of the trackability, flexibility, and conformability of coronary stents: A comparative analysis. Catheter. Cardiovasc. Interv. 2003, 59, 496–503. [Google Scholar] [CrossRef]
- Behrend, D.; Behrens, P.; Schmidt, W. Comparative Studies of Different Stent Designs. Prog. Biomed. Res. 1999, 4, 52–58. [Google Scholar]
- Ormiston, J.A.; Dixon, S.R.; Webster, M.W.I.; Ruygrok, P.N.; Stewart, J.T.; Minchington, I.; West, T. Stent longitudinal flexibility: A comparison of 13 stent designs before and after balloon expansion. Catheter. Cardiovasc. Interv. 2000, 50, 120–124. [Google Scholar] [CrossRef]
- Wei, L.; Chen, Q.; Li, Z. Study on the Impact of Straight Stents on with Different Curvatures. J. Mech. Med. Biol. 2016, 16, 1650093. [Google Scholar] [CrossRef]
- Wei, Y.B.; Wang, M.J.; Zhao, D.Y.; Li, H.X. In vitro experimental study on the mechanical properties of biodegradable polymer stents. J. Biomed. Eng. 2019, 36, 604–612. [Google Scholar]
- Wei, Y.B.; Zhao, D.Y.; Wang, M.J.; Li, H.X. Design and Mechanics Analysis of Biodegradable Polymer Vascular Stents with High Radial Supporting Property. Chin. J. Mech. Eng. 2020, 31, 1098–1107. [Google Scholar]
- Mori, K.; Saito, T. Effects of Stent Structure on Stent Flexibility Measurements. Ann. Biomed. Eng. 2005, 33, 733–742. [Google Scholar] [CrossRef]
- Tammareddi, S.; Sun, G.; Li, Q. Multiobjective robust optimization of coronary stents. Mater. Des. 2016, 90, 682–692. [Google Scholar] [CrossRef]
- Wang, W.Q.; Liang, D.K.; Yang, D.Z.; Qin, M. Analysis of the transient expansion behavior and design optimization of coronary stents by finite element method. J. Biomech. 2006, 39, 21–32. [Google Scholar] [CrossRef]
- Xia, Z.; Ju, F.; Sasaki, K. A general finite element analysis method for balloon expandable stents based on repeated unit cell (RUC) model. Finite Elem. Anal. Des. 2007, 43, 649–658. [Google Scholar] [CrossRef]
- Abad, E.M.K.; Pasini, D.; Cecere, R. Shape optimization of stress concentration-free lattice for self-expandable Nitinol stent-grafts. J. Biomech. 2012, 45, 1028–1035. [Google Scholar] [CrossRef] [Green Version]
- Douglas, G.R.; Phani, A.S.; Gagnon, J. Analyses and design of expansion mechanisms of balloon expandable vascular stents. J. Biomech. 2014, 47, 1438–1446. [Google Scholar] [CrossRef]
- Dolla, W.J.S.; Fricke, B.A.; Becker, B.R. Structural and Drug Diffusion Models of Conventional and Auxetic Drug-Eluting Stents. J. Med. Devices 2007, 1, 47. [Google Scholar] [CrossRef]
- Tan, T.W.; Douglas, G.R.; Bond, T.; Phani, A.S. Compliance and Longitudinal Strain of Cardiovascular Stents: Influence of Cell Geometry. J. Med. Devices 2011, 5, 041002. [Google Scholar] [CrossRef]
- Baughman, R.H. Auxetic materials: Avoiding the shrink. Nature 2003, 425, 667. [Google Scholar] [CrossRef]
- Carneiro, V.H.; Meireles, J.; Puga, H. Auxetic materials-A review. Mater. Sci. Pol. 2013, 31, 561–571. [Google Scholar] [CrossRef]
- Ali, M.N.; Busfield, J.J.C.; Rehman, I.U. Auxetic oesophageal stents: Structure and mechanical properties. J. Mater. Sci. Mater. Med. 2014, 25, 527–553. [Google Scholar] [CrossRef]
- Carneiro, V.H.; Puga, H. Modeling and elastic simulation of auxetic magnesium stents. In Proceedings of the 2015 IEEE 4th Portuguese Meeting on Bioengineering (ENBENG), Porto, Portugal, 26–28 February 2015; pp. 1–4. [Google Scholar]
- Liu, R.; Xu, S.; Luo, X.; Liu, Z.S. Theoretical and Numerical Analysis of Mechanical Behaviors of a Metamaterial-Based Shape Memory Polymer Stent. Polymers 2020, 12, 1784. [Google Scholar] [CrossRef]
- Ruan, X.L.; Li, J.J.; Song, X.K.; Zhou, H.J.; Yuan, W.; Wu, W.W.; Xia, R. Mechanical Design of Antichiral-Reentrant Hybrid Intravascular Stent. Int. J. Appl. Mech. 2019, 10, 1850105. [Google Scholar] [CrossRef]
- Geng, L.C.; Ruan, X.L.; Wu, W.W.; Xia, R.; Fang, D.N. Mechanical Properties of Selective Laser Sintering (SLS) Additive Manufactured Chiral Auxetic Cylindrical Stent. Exp. Mech. 2019, 59, 913–925. [Google Scholar] [CrossRef]
- Wu, Z.; Zhao, J.; Wu, W.; Wang, P.P.; Wang, B.F.; Li, G.W.; Zhang, S. Radial Compressive Property and the Proof-of-Concept Study for Realizing Self-expansion of 3D Printing Polylactic Acid Vascular Stents with Negative Poisson’s Ratio Structure. Materials 2018, 11, 1357. [Google Scholar] [CrossRef] [Green Version]
- Lith, R.V.; Baker, E.; Ware, H.; Jian, Y.; Farsheed, A.C.; Sun, C.; Ameer, G. 3D-Printing Strong High-Resolution Antioxidant Bioresorbable Vascular Stents. Adv. Mater. Technol. 2016, 1, 1600138. [Google Scholar] [CrossRef]
- Ware, H.O.T.; Farsheed, A.C.; Akar, B.; Duan, C.; Chen, X.F.; Ameer, G.; Sun, C. High-speed on-demand 3D printed bioresorbable vascular scaffolds. Mater. Today Chem. 2018, 7, 25–34. [Google Scholar] [CrossRef]
- Ware, H.O.T.; Farsheed, A.C.; Baker, E.; Ameer, G.; Sun, C. Fabrication Speed Optimization for High-resolution 3D-printing of Bioresorbable Vascular Scaffolds. Procedia CIRP 2017, 65, 131–138. [Google Scholar] [CrossRef]
- Torki, M.M.; Hassanajili, S.; Jalisi, M.M. Design optimizations of PLA stent structure by FEM and investigating its function in a simulated plaque artery. Math. Comput. Simul. 2020, 169, 103–116. [Google Scholar] [CrossRef]
- Han, Y.F.; Lu, W.F. Optimizing the deformation behavior of stent with nonuniform Poisson’s ratio distribution for curved artery. J. Mech. Behav. Biomed. 2018, 88, 442–452. [Google Scholar] [CrossRef] [PubMed]
- Auricchio, F.; Conti, M.; Beule, M.D.; Santis, G.D.; Verhegghe, B. Carotid artery stenting simulation: From patient-specific images to finite element analysis. Med. Eng. Phys. 2011, 33, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Morlacchi, S.; Colleoni, S.G.; Cárdenes, R.; Chiastra, C.; Diez, J.L.; Larrabide, I.; Migliavacca, F. Patient-specific simulations of stenting procedures in coronary bifurcations: Two clinical cases. Med. Eng. Phys. 2013, 35, 1272–1281. [Google Scholar] [CrossRef]
- Ragkousis, G.E.; Curzen, N.; Bressloff, N.W. Simulation of longitudinal stent deformation in a patient-specific coronary artery. Med. Eng. Phys. 2014, 36, 467–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




| Therapeutic Techniques | Bare Metal Stent (BMS) | Drug Elution Stent (DES) | Biodegradable Stent (BDS) |
|---|---|---|---|
| Main materials | Stainless steel; NiTi alloy. | Coated: sirolimus; paclitaxel; everolimus. The main substrates: stainless steel; cobalt-chromium alloy; NiTi shape memory alloy. | Polylactic acid; poly-L-lactic acid; polycaprolactone; Racemic polylactic acid; Mg alloy; Fe alloy; Zn alloy. |
| Material strength | High | High | Moderate/low |
| Biocompatability | No | No/coating material Yes | Yes |
| Biodegradability | No | No/coating material Yes | Yes |
| Post-implantation Drug administration | No | Always | Always |
| Vascular function interruption | Yes | Yes | Yes |
| Incidence complicaions | High | Moderate | Low (but may be higher than DESs) |
| Manufacturing method | Laser cutting; Traditional cutting. | 3D printing; electrospinning technology. | 3D printing; electrospinning technology; laser cutting. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, C.; Han, Y.; Lu, J. Structural Design of Vascular Stents: A Review. Micromachines 2021, 12, 770. https://doi.org/10.3390/mi12070770
Pan C, Han Y, Lu J. Structural Design of Vascular Stents: A Review. Micromachines. 2021; 12(7):770. https://doi.org/10.3390/mi12070770
Chicago/Turabian StylePan, Chen, Yafeng Han, and Jiping Lu. 2021. "Structural Design of Vascular Stents: A Review" Micromachines 12, no. 7: 770. https://doi.org/10.3390/mi12070770