Botulinum Toxin Therapy for Psychiatric Disorders in Clinical Practice: A Retrospective Case Study


Abstract
:1. Introduction
2. Results
2.1. Participants
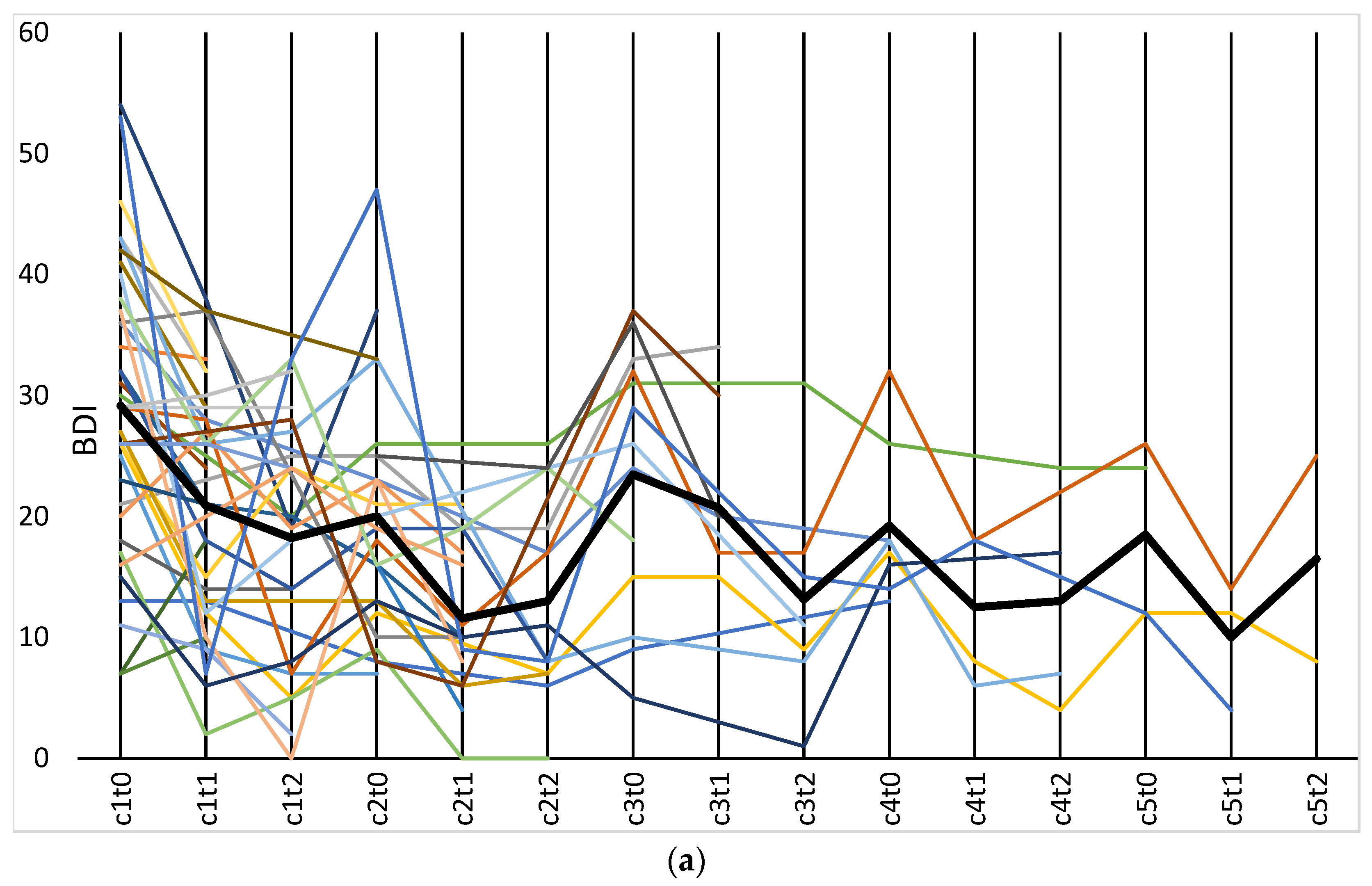
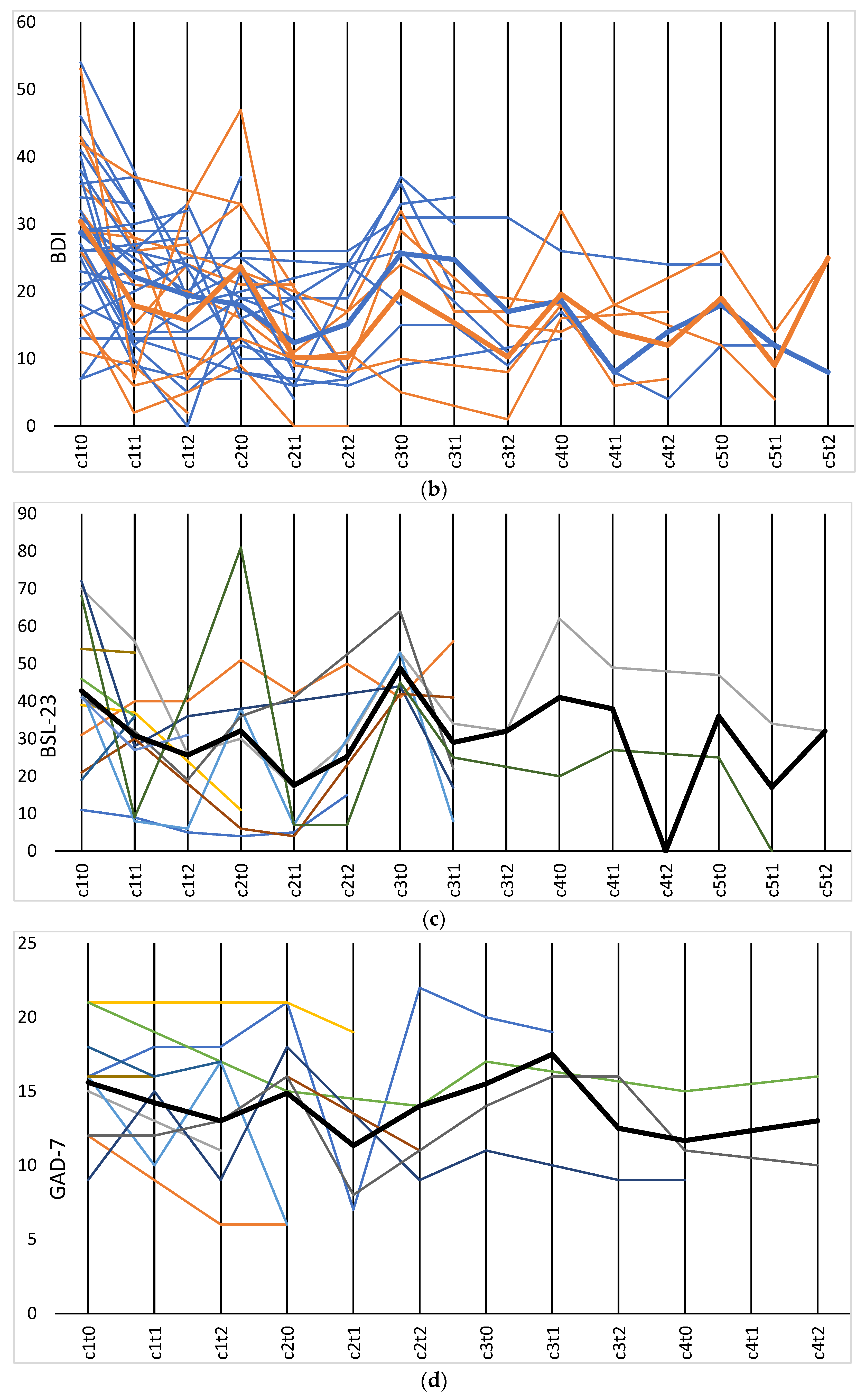
2.2. BDI
2.3. BSL-23
2.4. GAD-7
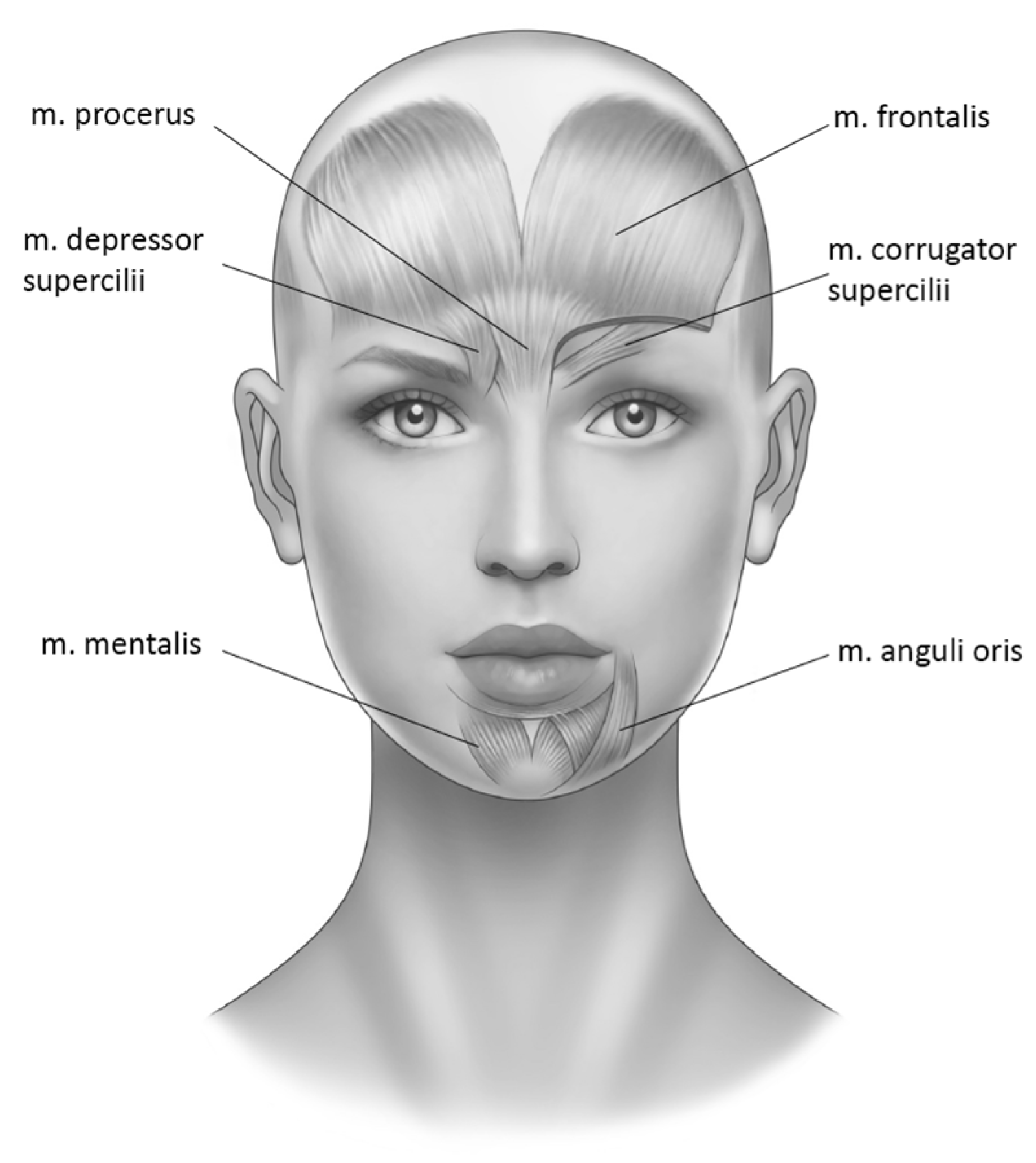
2.5. Comparison of Treatment Locations
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Procedure
5.2. Data Collection
5.3. Data Preparation
5.4. Data Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finzi, E.; Wasserman, E. Treatment of Depression with Botulinum Toxin A: A Case Series. Dermatol. Surg. 2006, 32, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Brin, M.F.; Durgam, S.; Lum, A.; James, L.; Liu, J.; Thase, M.E.; Szegedi, A. OnabotulinumtoxinA for the treatment of major depressive disorder: A phase 2 randomized, double-blind, placebo-controlled trial in adult females. Int. Clin. Psychopharmacol. 2020, 35, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finzi, E.; Rosenthal, N.E. Treatment of depression with onabotulinumtoxinA: A randomized, double-blind, placebo controlled trial. J. Psychiatr. Res. 2014, 52, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Magid, M.; Reichenberg, J.S.; Poth, P.E.; Robertson, H.T.; LaViolette, A.K.; Kruger, T.H.C.; Wollmer, M.A. Treatment of major depressive disorder using botulinum toxin A: A 24-week randomized, double-blind, placebo-controlled study. J. Clin. Psychiatry 2014, 75, 837–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wollmer, M.A.; de Boer, C.; Kalak, N.; Beck, J.; Gotz, T.; Schmidt, T.; Hodzic, M.; Bayer, U.; Kollmann, T.; Kollewe, K.; et al. Facing depression with botulinum toxin: A randomized controlled trial. J. Psychiatr. Res. 2012, 46, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Zamanian, A.; Ghanbari Jolfaei, A.; Mehran, G.; Azizian, Z. Efficacy of Botox versus Placebo for Treatment of Patients with Major Depression. Iran J. Public Health 2017, 46, 982–984. [Google Scholar]
- Li, Y.; Zhu, T.; Shen, T.; Wu, W.; Cao, J.; Sun, J.; Liu, J.; Zhou, X.; Jiang, C.; Tang, Z.; et al. Botulinum toxin A (BoNT/A) for the treatment of depression: A randomized, double-blind, placebo, controlled trial in China. J. Affect. Disord. 2022, 318, 48–53. [Google Scholar] [CrossRef]
- Arnone, D.; Galadari, H.; Rodgers, C.J.; Ostlundh, L.; Aziz, K.A.; Stip, E.; Young, A.H. Efficacy of onabotulinumtoxinA in the treatment of unipolar major depression: Systematic review, meta-analysis and meta-regression analyses of double-blind randomised controlled trials. J. Psychopharmacol. 2021, 35, 910–918. [Google Scholar] [CrossRef]
- Crowley, J.S.; Silverstein, M.L.; Reghunathan, M.; Gosman, A.A. Glabellar Botulinum Toxin Injection Improves Depression Scores: A Systematic Review and Meta-Analysis. Plast. Reconstr. Surg. 2022, 150, 211e–220e. [Google Scholar] [CrossRef]
- Cohen, I.V.; Makunts, T.; Atayee, R.; Abagyan, R. Population scale data reveals the antidepressant effects of ketamine and other therapeutics approved for non-psychiatric indications. Sci. Rep. 2017, 7, 1450. [Google Scholar] [CrossRef] [Green Version]
- Coles, N.A.; Larsen, J.T.; Lench, H.C. A meta-analysis of the facial feedback literature: Effects of facial feedback on emotional experience are small and variable. Psychol. Bull. 2019, 145, 610–651. [Google Scholar] [CrossRef] [PubMed]
- Darwin, C. The Expression of the Emotions in Man and Animals; John Murray: London, UK, 1872; Volume 1, p. 374. [Google Scholar]
- Wollmer, M.A.; Neumann, I.; Jung, S.; Bechinie, A.; Herrmann, J.; Muller, A.; Wohlmuth, P.; Fournier-Kaiser, L.; Sperling, C.; Peters, L.; et al. Clinical effects of glabellar botulinum toxin injections on borderline personality disorder: A randomized controlled trial. J. Psychopharmacol. 2022, 36, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Larsen, R.J.; Kasimatis, M.; Frey, K. Facilitating the Furrowed Brow: An Unobtrusive Test of the Facial Feedback Hypothesis Applied to Unpleasant Affect. Cogn. Emot. 1992, 6, 321–338. [Google Scholar] [CrossRef] [PubMed]
- Marzoli, D.; Custodero, M.; Pagliara, A.; Tommasi, L. Sun-induced frowning fosters aggressive feelings. Cogn. Emot. 2013, 27, 1513–1521. [Google Scholar] [CrossRef]
- Mori, K.; Mori, H. Examination of the Passive Facial Feedback Hypothesis Using an Implicit Measure: With a Furrowed Brow, Neutral Objects with Pleasant Primes Look Less Appealing. Percept. Motor Skills 2010, 111, 785–789. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, G.E.; Fair, P.L.; Salt, P.; Mandel, M.R.; Klerman, G.L. Facial muscle patterning to affective imagery in depressed and nondepressed subjects. Science 1976, 192, 489–491. [Google Scholar] [CrossRef]
- Whatmore, G.B.; Ellis, R.M. Some neurophysiologic aspects of depressed states: An electromyographic study. AMA Arch. Gen. Psychiatry 1959, 1, 70–80. [Google Scholar] [CrossRef]
- Whatmore, G.B.; Ellis, R.M., Jr. Further Neurophysiologic Aspects of Depressed States: An Electromyographic Study. Arch. Gen. Psychiatry 1962, 6, 243–253. [Google Scholar] [CrossRef]
- Carney, R.M.; Hong, B.A.; O’Connell, M.F.; Amado, H. Facial electromyography as a predictor of treatment outcome in depression. Br. J. Psychiatry 1981, 138, 485–489. [Google Scholar] [CrossRef]
- Schwartz, G.E.; Fair, P.L.; Mandel, M.R.; Salt, P.; Mieske, M.; Klerman, G.L. Facial electromyography in the assessment of improvement in depression. Psychosom. Med. 1978, 40, 355–360. [Google Scholar] [CrossRef]
- Greden, J.F.; Price, H.L.; Genero, N.; Feinberg, M.; Levine, S. Facial EMG activity levels predict treatment outcome in depression. Psychiatry Res. 1984, 13, 345–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, J.T.; Norris, C.J.; Cacioppo, J.T. Effects of positive and negative affect on electromyographic activity over zygomaticus major and corrugator supercilii. Psychophysiology 2003, 40, 776–785. [Google Scholar] [CrossRef]
- Keltner, D.; Sauter, D.; Tracy, J.; Cowen, A. Emotional Expression: Advances in Basic Emotion Theory. J. Nonverbal. Behav. 2019, 43, 133–160. [Google Scholar] [CrossRef] [PubMed]
- Magid, M.; Reichenberg, J. Botulinum toxin for depression? An idea that’s raising some eyebrows. Curr. Psychiatry 2015, 14, 43–56. [Google Scholar]
- Antonucci, F.; Rossi, C.; Gianfranceschi, L.; Rossetto, O.; Caleo, M. Long-distance retrograde effects of botulinum neurotoxin A. J. Neurosci. 2008, 28, 3689–3696. [Google Scholar] [CrossRef] [PubMed]
- Hennenlotter, A.; Dresel, C.; Castrop, F.; Ceballos-Baumann, A.O.; Wohlschlager, A.M.; Haslinger, B. The link between facial feedback and neural activity within central circuitries of emotion--new insights from botulinum toxin-induced denervation of frown muscles. Cereb Cortex. 2009, 19, 537–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W. Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. J. Pers Assess 1996, 67, 588–597. [Google Scholar] [CrossRef]
- Bohus, M.; Limberger, M.F.; Frank, U.; Sender, I.; Gratwohl, T.; Stieglitz, R.D. Development of the Borderline Symptom List. Psychother. Psychosom. Med. Psychol. 2001, 51, 201–211. [Google Scholar] [CrossRef]
- Lowe, B.; Decker, O.; Muller, S.; Brahler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | N | % | Range | M | SD |
|---|---|---|---|---|---|
| Gender | |||||
| Female | 31 | 72.09 | |||
| Male | 12 | 27.91 | |||
| Age (years) | 43 | 100 | 29–80 | 51.28 | 12.76 |
| Estimated time since initial diagnosis (years) | 29 | 67.44 | 2–75 | 21.92 | 16.95 |
| Duration of current depressive episode (months) | 11 | 26.19 | 3–72 | 36.82 | 24.82 |
| Primary diagnosis: Generalized Anxiety Disorder | 1 | 2.33 | |||
| Primary diagnosis: Borderline Personality Disorder | 5 | 11.63 | |||
| Primary diagnosis: Depression | 37 | 86.05 | |||
| F31.3 Mild or Moderate Bipolar Depression | 2 | 4.65 | |||
| F31.4 Severe Bipolar Depression | 1 | 2.33 | |||
| F32.1 Moderate Depressive Episode | 9 | 20.93 | |||
| F32.2 Severe Depressive Episode | 9 | 20.93 | |||
| F33.1 Recurrent Depressive Disorder, Moderate | 8 | 18.60 | |||
| F33.2 Recurrent Depressive Disorder, Severe | 8 | 18.60 | |||
| Comorbid psychiatric diagnoses | 24 | 55.81 | |||
| F11.2 Opioid Addiction | 1 | 2.33 | |||
| F41.0 Panic Disorder | 1 | 2.34 | |||
| F41.1 Generalized Anxiety Disorder | 6 | 13.95 | |||
| F42.2 Obsessive–Compulsive Disorder | 2 | 4.65 | |||
| F43.1 Post-Traumatic Stress Disorder | 5 | 11.63 | |||
| F45.0 Somatization Disorder | 1 | 2.33 | |||
| F50.2 Bulimia Nervosa | 1 | 2.34 | |||
| F60.31 Borderline Personality Disorder | 7 | 16.28 | |||
| Antidepressant medication | 18 | 41.86 | |||
| Tricyclic | 2 | 4.65 | |||
| SNRIs | 5 | 11.63 | |||
| SSRIs | 5 | 11.63 | |||
| MAOI | 1 | 2.33. | |||
| Others | 5 | 11.63 | |||
| Other psychopharmaceuticals | 29 | 67.44 | |||
| Antipsychotics | 11 | 25.58 | |||
| Sedatives | 4 | 9.33 | |||
| Lithium | 4 | 9.33 | |||
| Others | 10 | 23.26 | |||
| BDI | 39 | 90.70 | 7–54 | 29.16 | |
| BSL-23 | 13 | 30.23 | 11–27 | 40.77 | |
| GAD-7 | 11 | 25.58 | 9–21 | 15.60 |
| t0 | t1 | t2 | t0 | t1 | t2 | t0 | t1 | t2 | t0 | t1 | t2 | t0 | t1 | t2 | |
| BDI | |||||||||||||||
| N | 36 | 34 | 24 | 21 | 14 | 15 | 13 | 7 | 7 | 8 | 4 | 4 | 4 | 3 | 2 |
| Mean | 29.6 | 21.3 | 18.2 | 19.1 | 10.5 | 13.5 | 25.4 | 20.8 | 13.1 | 20.5 | 12.5 | 13.0 | 16.7 | 10.0 | 16.5 |
| SD | 11.7 | 9.9 | 10.2 | 9.2 | 5.9 | 8.1 | 11.3 | 9.5 | 9.4 | 7.0 | 6.4 | 9.2 | 8.1 | 5.3 | 12.0 |
| F(2,49) = 16.5, p < 0.001, ηp2 = 0.452; N = 21 | F(1.2,8.5) = 2.95, p = 0.118, ηp2 = 0.297; N = 8 | ||||||||||||||
| BSL-23 | |||||||||||||||
| N | 13 | 13 | 8 | 8 | 7 | 4 | 7 | 7 | 1 | 2 | 2 | 0 | 2 | 2 | 1 |
| Mean | 42.8 | 30.9 | 25.6 | 32.1 | 17.6 | 25.3 | 48.9 | 29.0 | 32.0 | 41.0 | 38.0 | 0 | 36 | 17 | 32 |
| SD | 19.5 | 15.3 | 14.5 | 26.0 | 16.9 | 18.9 | 8.3 | 16.1 | 0 | 29.7 | 15.6 | 0 | 15.6 | 24 | 0 |
| F(2,14) = 6.16, p = 0.012, ηp2 = 0.468; N = 8 | |||||||||||||||
| GAD-7 | |||||||||||||||
| N | 9 | 9 | 7 | 6 | 3 | 4 | 3 | 2 | 2 | 2 | 0 | 2 | |||
| Mean | 15 | 14.2 | 13 | 17.8 | 11.3 | 14 | 15 | 18 | 13 | 13 | 0 | 13 | |||
| SD | 3.6 | 3.5 | 4.6 | 2.7 | 6.7 | 5.7 | 4.6 | 2.1 | 5 | 2.8 | 0 | 4.3 | |||
| Cycle 1 | Cycle 2 | Cycle 3 | Cycle 4 | Cycle 5 | |||||||||||
| t0 | t1 | t2 | t0 | t1 | t2 | t0 | t1 | t2 | t0 | t1 | t2 | t0 | t1 | t2 | |
| BDI | |||||||||||||||
| N | 36 | 34 | 24 | 21 | 14 | 15 | 13 | 7 | 7 | 8 | 4 | 4 | 4 | 3 | 2 |
| Mean | 29.6 | 21.3 | 18.2 | 19.1 | 10.5 | 13.5 | 25.4 | 20.8 | 13.1 | 20.5 | 12.5 | 13.0 | 16.7 | 10.0 | 16.5 |
| SD | 11.7 | 9.9 | 10.2 | 9.2 | 5.9 | 8.1 | 11.3 | 9.5 | 9.4 | 7.0 | 6.4 | 9.2 | 8.1 | 5.3 | 12.0 |
| F(2,49) = 16.5, p < 0.001, ηp2 = 0.452; N = 21 | F(1.2,8.5) = 2.95, p = 0.118, ηp2 = 0.297; N = 8 | ||||||||||||||
| BSL-23 | |||||||||||||||
| N | 13 | 13 | 8 | 8 | 7 | 4 | 7 | 7 | 1 | 2 | 2 | 0 | 2 | 2 | 1 |
| Mean | 42.8 | 30.9 | 25.6 | 32.1 | 17.6 | 25.3 | 48.9 | 29.0 | 32.0 | 41.0 | 38.0 | 0 | 36 | 17 | 32 |
| SD | 19.5 | 15.3 | 14.5 | 26.0 | 16.9 | 18.9 | 8.3 | 16.1 | 0 | 29.7 | 15.6 | 0 | 15.6 | 24 | 0 |
| F(2,14) = 6.16, p = 0.012, ηp2 = 0.468; N = 8 | |||||||||||||||
| GAD-7 | |||||||||||||||
| N | 9 | 9 | 7 | 6 | 3 | 4 | 3 | 2 | 2 | 2 | 0 | 2 | |||
| Mean | 15 | 14.2 | 13 | 17.8 | 11.3 | 14 | 15 | 18 | 13 | 13 | 0 | 13 | |||
| SD | 3.6 | 3.5 | 4.6 | 2.7 | 6.7 | 5.7 | 4.6 | 2.1 | 5 | 2.8 | 0 | 4.3 | |||
| t0c1 | t1c1 | t2c1 | t0 | t1 | t2 | t0 | t1 | t2 | t0 | t1 | t2 | t0 | t1 | t2 | |
| BDI-UF | |||||||||||||||
| N | 26 | 24 | 16 | 13 | 9 | 8 | 6 | 4 | 3 | 2 | 1 | 2 | 1 | 1 | 1 |
| Mean | 29.3 | 22.7 | 19.4 | 16.9 | 11.9 | 15.1 | 29.7 | 24.8 | 17 | 21.5 | 8 | 14 | 12 | 12 | 8 |
| SD | 11.1 | 8.9 | 9.6 | 6.5 | 6.3 | 8.9 | 8.2 | 8.7 | 12.2 | 6.4 | 14.1 | / | / | / | |
| F(1.4,16.7) = 9,79, p = 0.003, ηp2 = 0.449; N = 13 | |||||||||||||||
| t0c1 | t1c1 | t2c1 | t0 | t1 | t2 | t0 | t1 | t2 | t0 | t1 | t2 | t0 | t1 | t2 | |
| BDI-ULF | |||||||||||||||
| N | 10 | 10 | 8 | 8 | 5 | 7 | 4 | 2 | 4 | 4 | 3 | 2 | 2 | 2 | 1 |
| Mean | 30.4 | 17.9 | 15.8 | 22.5 | 8 | 11.7 | 19 | 13 | 10.3 | 20 | 14 | 12 | 19 | 9 | 25 |
| SD | 13.6 | 11.8 | 11.7 | 12 | 6.7 | 6.4 | 11.9 | 5.7 | 7.3 | 7.1 | 6.9 | 7.1 | 9.9 | 7.1 | / |
| F(2,14) = 6,74, p = 0.009, ηp2 = 0.490; N = 8 | |||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehnert, F.; Neumann, I.; Krüger, T.H.C.; Wollmer, M.A. Botulinum Toxin Therapy for Psychiatric Disorders in Clinical Practice: A Retrospective Case Study. Toxins 2023, 15, 385. https://doi.org/10.3390/toxins15060385
Lehnert F, Neumann I, Krüger THC, Wollmer MA. Botulinum Toxin Therapy for Psychiatric Disorders in Clinical Practice: A Retrospective Case Study. Toxins. 2023; 15(6):385. https://doi.org/10.3390/toxins15060385
Chicago/Turabian StyleLehnert, Franziska, Insa Neumann, Tillmann H. C. Krüger, and Marc A. Wollmer. 2023. "Botulinum Toxin Therapy for Psychiatric Disorders in Clinical Practice: A Retrospective Case Study" Toxins 15, no. 6: 385. https://doi.org/10.3390/toxins15060385