Effects of Probiotics, Prebiotics, and Synbiotics on Human Health

Abstract
:1. Introduction
2. Probiotics
2.1. Selection Criteria and Requirements for Probiotic Strains
2.2. Probiotic Microorganisms
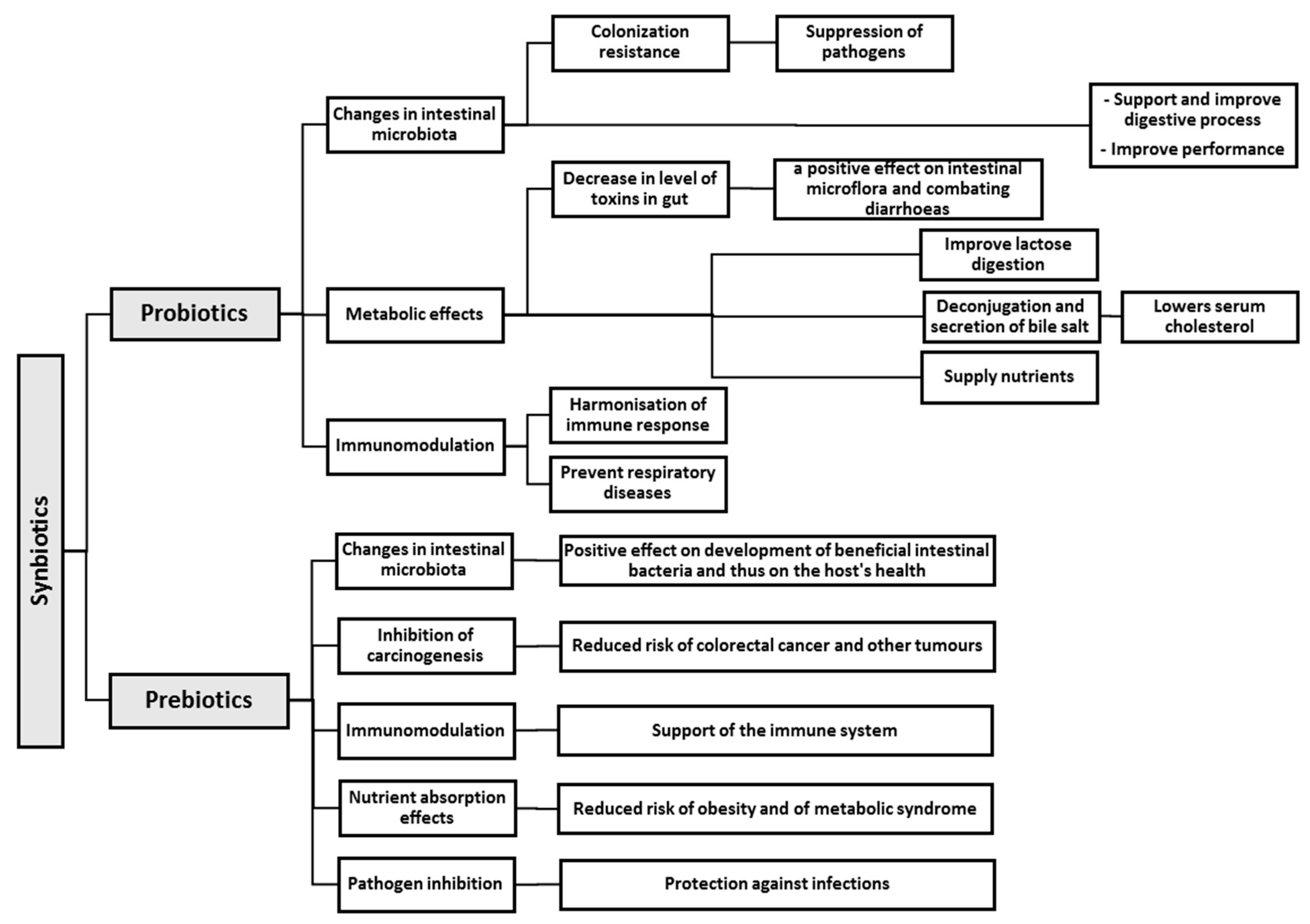
2.3. Mechanism of Action of Probiotics
- (1)
- Induction and maintenance of the state of immunological tolerance to environmental antigens (nutritional and inhalatory);
- (2)
- Induction and control of immunological reactions against pathogens of bacterial and viral origin;
- (3)
- Inhibition of auto-aggressive and allergic reactions.
2.4. Probiotics for Humans
3. Prebiotics
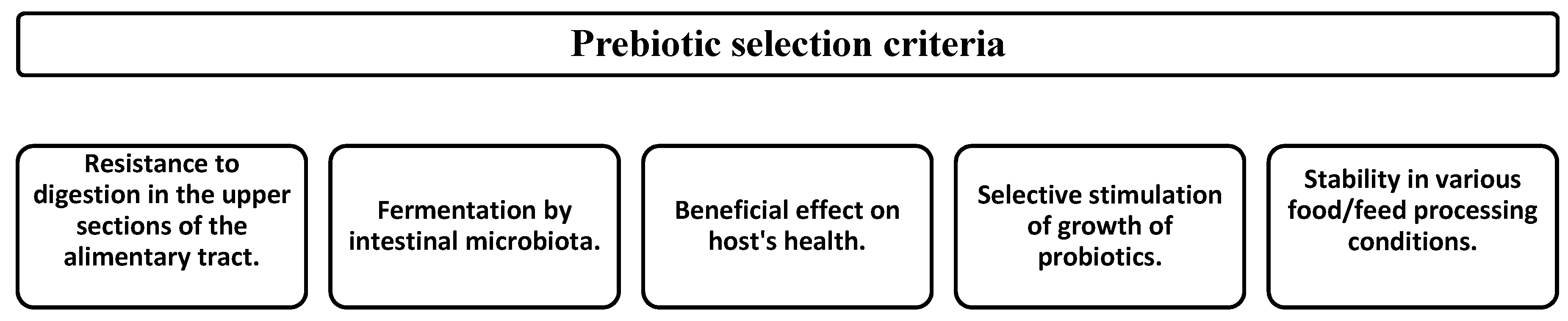
3.1. Prebiotic Selection Criteria
3.2. Prebiotic Substances
- not digested (or only partially digested);
- not absorbed in the small intestine;
- poorly fermented by bacteria in the oral cavity;
- well fermented by seemingly beneficial intestinal bacteria;
- poorly fermented by potential pathogens in the bowel.
3.3. Mechanism of Action of Prebiotics
- (1)
- Prebiotics are able to regulate the action of hepatic lipogenic enzymes by influencing the increased production of short-chain fatty acids (SCFAs), such as propionic acid.
- (2)
- The production of SCFAs (especially of butyric acid) as a result of fermentation was identified as a modulator of histone acetylation, thus increasing the availability of numerous genes for transcription factors.
- (3)
- The modulation of mucin production.
- (4)
- It was demonstrated that FOS and several other prebiotics cause an increased count of lymphocytes and/or leukocytes in gut-associated lymphoid tissues (GALTs) and in peripheral blood.
- (5)
- The increased secretion of IgA by GALTs may stimulate the phagocytic function of intra-inflammatory macrophages.
3.4. Prebiotics for Humans
4. Synbiotics
4.1. Synbiotic Selection Criteria
4.2. Synbiotics in Use
4.3. Mechanism of Action of Synbiotics
- (1)
- Action through the improved viability of probiotic microorganisms;
- (2)
- Action through the provision of specific health effects.
4.4. Synbiotics for Humans
- (1)
- Increased Lactobacillus and Bifidobacterium genus count and maintenance of balance of the intestinal microbiota;
- (2)
- Improved hepatic function in patients suffering from cirrhosis;
- (3)
- Improved immunomodulative abilities;
- (4)
- Prevention of bacterial translocation and reduced incidence of nosocomial infections in patients’ post-surgical procedures and similar interventions.
5. Summary
Acknowledgments
Conflicts of Interest
References
- Vergin, F. Anti-und Probiotica. Hipokrates 1954, 25, 116–119. [Google Scholar]
- Lilly, D.M.; Stillwell, R.H. Probiotics: Growth promoting factors produced by microorganisms. Science 1965, 147, 747–748. [Google Scholar] [CrossRef] [PubMed]
- Fuller, R. Probiotics in man and animals. J. Appl. Microbiol. 1989, 66, 365–378. [Google Scholar]
- Guarner, F.; Schaafsma, G.J. Probiotics. Int. J. Food Microbiol. 1998, 39, 237–238. [Google Scholar] [CrossRef]
- Food and Agriculture Organization (FAO). Guidelines for the Evaluation of Probiotics in Food; Report of a Joint FAO/WHO Working Group on Drafting Guidelines for the Evaluation of Probiotics in Food; FAO: London, ON, Canada, 30 April–1 May 2002.
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.G.; Roberfroid, M.B. Dietary modulation of the human colonic microbiota: Introducing the concept of prebiotics. J. Nutr. 1995, 125, 1401–1412. [Google Scholar] [PubMed]
- Gibson, G.R.; Probert, H.M.; van Loo, J.; Rastall, R.A.; Roberfroid, M. Dietary modulation of the human colonic microbiota: Updating the concept of the prebiotics. Nutr. Res. Rev. 2004, 17, 259–275. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization. FAO Technical Meeting on Prebiotics: Food Quality and Standards Service (AGNS), Food and Agriculture Organization of the United Nations (FAO); FAO Technical Meeting Report; FAO: Rome, Italy, 15–16 September 2007. [Google Scholar]
- Skalkam, M.L.; Wiese, M.; Nielsen, D.S.; van Zanten, G. In Vitro Screening and Evaluation of Synbiotics; University of Copenhagen: Copenhagen, Denmark, 2016; Chapter 33; pp. 477–486. [Google Scholar]
- Cencic, A.; Chingwaru, W. The role of functional foods, nutraceuticals, and food supplements in intestinal health. Nutrients 2010, 2, 611–625. [Google Scholar] [CrossRef] [PubMed]
- Rioux, K.P.; Madsen, K.L.; Fedorak, R.N. The role of enteric microflora in inflammatory bowel disease: Human and animal studies with probiotics and prebiotics. Gastroenterol. Clin. N. Am. 2005, 34, 465–482. [Google Scholar] [CrossRef] [PubMed]
- Bengmark, S. Bioecological control of the gastrointestinal tract: The role of flora and supplemented probiotics and synbiotics. Gastroenterol. Clin. N. Am. 2005, 34, 413–436. [Google Scholar] [CrossRef] [PubMed]
- Panesar, P.S.; Kaur, G.; Panesar, R.; Bera, M.B. Synbiotics: Potential Dietary Supplements in Functional Foods; IFIS: Berkshire, UK, 2009. [Google Scholar] [CrossRef]
- Hosono, A. Fermented milk in the orient. In Functions of Fermented Milk: Challengers for the Health Sciences; Nakazawa, Y., Hosono, A., Eds.; Elsevier Science Publishers Ltd.: Barking, UK, 1992; pp. 61–78. [Google Scholar]
- Miecznikow, E. O naturze ludzkiej—Zarys Filozofii Optymistycznej; Translation F. Wermiński; Wydawnictwo Biblioteka Naukowa: Warszawa, Poland, 1907. [Google Scholar]
- Lee, Y.K. Selection and maintenance of probiotic microorganisms. In Handbook of Probiotics and Prebiotics; Lee, Y.K., Salminen, S., Eds.; Wiley-VCH: Weinheim, Germany, 2009; pp. 177–187. [Google Scholar] [CrossRef]
- Sanders, M.E.; Gibson, G.; Harsharnjit, S.G.; Guarner, F. Probiotics: Their Potential to Impact Human Health; CAST Issue Paper; CAST: Ames, IA, USA, 2007; Volume 36, pp. 1–20. [Google Scholar]
- Sanders, M.E.; Lenoir-Wijnkoop, I.; Salminen, S.; Merenstein, D.J.; Gibson, G.R.; Petschow, B.W.; Nieuwdorp, M.; Tancredi, D.J.; Cifelli, C.J.; Jacques, P.; et al. Probiotics and prebiotics: Prospects for public health and nutritional recommendations. Ann. N. Y. Acad. Sci. 2014, 1309, 19–29. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Opinion of the Scientific Committee on a request from EFSA related to a generic approach to the safety assessment by EFSA of microorganisms used in food/feed and the production of food/feed additives. EFSA J. 2005, 226, 1–12. [Google Scholar]
- Simon, O. Micro-organisms as feed additives—Probiotics. Adv. Pork Prod. 2005, 16, 161–167. [Google Scholar]
- Anadón, A.; Martínez-Larrańaga, M.R.; Martínez, M.A. Probiotics for animal nutrition in the European Union. Regulation and safety assessment. Regul. Toxicol. Pharmacol. 2006, 45, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Gaggia, F.; Mattarelli, P.; Biavati, B. Probiotics and prebiotics in animal feeding for safe food production. Int. J. Food Microbiol. 2010, 141, S15–S28. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). The European Union Summary report on trends and sources of zoonoses, zoonotic agents and food-borne outbreaks in 2011. EFSA J. 2013, 3129, 1–250. [Google Scholar]
- European Food Safety Authority (EFSA). Scientific opinion on the maintenance of the list of QPS biological agents intentionally added to food and feed (2013 update). EFSA J. 2013, 15, 1–108. [Google Scholar]
- European Food Safety Authority (EFSA). Scientific Opinion on the update of the list of QPS-recommended biological agents intentionally added to food or feed as notified to EFSA (2017 update). EFSA J. 2017, 15, 1–177. [Google Scholar]
- Schachtsiek, M.; Hammes, W.P.; Hertel, C. Characterization of Lactobacillus coryniformis DSM 20001T surface protein CPF mediating coaggregation with and aggregation among pathogens. Appl. Environ. Microbiol. 2004, 70, 7078–7085. [Google Scholar] [CrossRef] [PubMed]
- Oelschlaeger, T.A. Mechanisms of probiotic actions—A review. Int. J. Med. Microbiol. 2010, 300, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Cremonini, F.; di Caro, S.; Nista, E.C.; Bartolozzi, F.; Capelli, G.; Gasbarrini, G.; Gasbarrini, A. Meta-analysis: The eqect of probiotic administration on antibiotic associateddiarrhoea. Aliment. Pharmacol. Ther. 2002, 16, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Johnston, B.C.; Supina, A.L.; Vohra, S. Probiotics for pediatric antibiotic-associated diarrhea: A meta-analysis of randomized placebo-controlled trials. Can. Med. Assoc. J. 2006, 175, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Schoster, A.; Kokotovic, B.; Permin, A.; Pedersen, P.D.; Dal Bello, F.; Guardabassi, L. In Vitro inhibition of Clostridium difficile and Clostridium perfringens by commercial probiotic strains. Anaerobe 2013, 20, 36–41. [Google Scholar] [CrossRef] [PubMed]
- JimmySaint-Cyr, M.; Haddad, N.; Taminiau, B.; Poezevara, T.; Quesne, S.; Amelot, M.; Daube, G.; Chemaly, M.; Dousset, X.; Guyard-Nicodème, M. Use of the potential probiotic strain Lactobacillus salivarius SMXD51 to control Campylobacter jejuni in broilers. Int. J. Food Microbiol. 2017, 247, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.; Adams, M.; La Ragione, R.M.; WoodWard, M.J. Colonisation of poultry by Salmonella Enteritidis S1400 is reduced by combined administration of Lactobacillus salivarius 59 and Enterococcus faecium PXN-33. Vet. Microbiol. 2017, 199, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Chingwaru, W.; Vidmar, J. Potential of Zimbabwean commercial probiotic products and strains of Lactobacillus plantarum as prophylaxis and therapy against diarrhoea caused by Escherichia coli in children. Asian Pac. J. Trop. Med. 2017, 10, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.A.; Patil, G.R.; Reddi, S.; Yadav, V.; Pothuraju, R.; Singh, R.R.B.; Kapila, S. Aloe vera (Aloe barbadensis Miller) supplemented probiotic lassi prevents Shigella infiltration from epithelial barrier into systemic blood flow in mice model. Microb. Pathog. 2017, 102, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Sikorska, H.; Smoragiewicz, W. Role of probiotics in the prevention and treatment of ethicillin-resistant Staphylococcus aureus infections. Int. J. Antimicrob. Agents 2013, 42, 475–481. [Google Scholar] [CrossRef] [PubMed]
- De Montijo-Prieto, S.; Moreno, E.; Bergillos-Meca, T.; Lasserrot, A.; Ruiz-López, M.; Ruiz-Bravo, A.; Jimenez-Valera, M. A Lactobacillus plantarum strain isolated from kefir protects against intestinal infection with Yersinia enterocolitica O9 and modulates immunity in mice. Res. Microbiol. 2015, 166, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.W.; Greer, F. Probiotics and prebiotics in pediatrics. Pediatrics 2010, 126, 1217–1231. [Google Scholar] [CrossRef] [PubMed]
- Heczko, P.; Strus, M.; Jawień, M.; Szymański, H. Medyczne zastosowanie probiotyków. Wiad. Lek. 2005, 58, 640–646. [Google Scholar] [PubMed]
- Kumar, S.; Bansal, A.; Chakrabarti, A.; Singhi, S. Evaluation of efficacy of probiotics in prevention of Candida colonization in a PICU—A randomized controlled trial. Crit. Care Med. 2013, 41, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Nase, L.; Hatakka, K.; Savilahti, E. Eqect of long-term consumption of Lactobacillus GG in milk on dental caries and caries risk in children. Caries Res. 2001, 35, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Gu, Q. Complete genome sequence of Lactobacillus plantarum LZ95, a potential probiotic strain producing bacteriocins and B-group vitamin riboflavin. J. Biotechnol. 2016, 229, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Zhang, C.; Song, D.; Li, P.; Zhu, X. Enhancing vitamin B12 content in soy-yogurt by Lactobacillus reuteri. Int. J. Food Microbiol. 2015, 206, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Pompei, A.; Cordisco, L.; Amaretti, A.; Zanoni, S.; Matteuzzi, D.; Rossi, M. Folate production by bifidobacteria as a potential probiotic property. Appl. Environ. Microbiol. 2007, 73, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Nova, E.; Warnberg, J.; Gomez-Martinez, S.; Diaz, L.E.; Romeo, J.; Marcos, A. Immunodulatory effects of probiotics in different stages of life. Br. J. Nutr. 2007, 98, S90–S95. [Google Scholar] [CrossRef] [PubMed]
- Mishra, C.; Lambert, J. Production of anti-microbial substances by probiotics. Asia Pac. J. Clin. Nutr. 1996, 5, 20–24. [Google Scholar] [PubMed]
- Ouwehand, A.C.; Kirjavainen, P.V.; Shortt, C.; Salminen, S. Probiotics: Mechanisms and established effects. Int. Dairy J. 1999, 9, 43–52. [Google Scholar] [CrossRef]
- Reid, G.; McGroarty, J.A.; Angotti, R.; Cook, R.L. Lactobacillus inhibitor production against Escherichia coli and coaggregation ability with uropathogens. Can. J. Microbiol. 1988, 34, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Schellenberg, J.; Smoragiewicz, W.; Karska-Wysocki, B. A rapid method combining immunofluorescence and flow cytometry for improved understanding of competitive interactions between lactic acid bacteria (LAB) and methicillin-resistant S. aureus (MRSA) in mixed culture. J. Microbiol. Methods 2006, 65, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Akedo, I.; Otani, T.; Suzuki, T.; Nakamura, T.; Takeyama, I.; Ishiguro, S.; Miyaoka, E.; Sobue, T.; Kakizoe, T. Randomized trial of dietary fiber and Lactobacillus casei administration for prevention of colorectal tumors. Int. J. Cancer 2005, 116, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Vandenbergh, P.A. Lactic acid bacteria, their metabolic products and interference with microbial growth. FEMS Microbiol. Rev. 1993, 12, 221–238. [Google Scholar] [CrossRef]
- Guillot, J.F. Probiotic feed additives. J. Vet. Pharmacol. Ther. 2003, 26, 52–55. [Google Scholar]
- Isolauri, E.; Sutas, Y.; Kankaanpaa, P.; Arvilommi, H.; Salminen, S. Probiotics: Effects on immunity. Am. J. Clin. Nutr. 2001, 73, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Brandao, R.L.; Castro, I.M.; Bambirra, E.A.; Amaral, S.C.; Fietto, L.G.; Tropia, M.J.M. Intracellular signal triggered by cholera toxin in Saccharomyces boulardii and Saccharomyces cerevisiae. Applied Environ. Microbiol. 1998, 64, 564–568. [Google Scholar] [PubMed]
- Collado, M.C.; Meriluoto, J.; Salminen, S. Interactions between pathogens and lactic acid bacteria: Aggregation and coaggregation abilities. Eur. J. Food Res. Technol. 2007, 226, 1065–1073. [Google Scholar] [CrossRef]
- Begley, M.; Hill, C.; Gahan, C.G.M. Bile salt hydrolase activity in probiotics. Appl. Environ. Microbiol. 2006, 72, 1729–1738. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, E.D. The Lactobacillus anomaly: Total iron abstinence. Perspect. Biol. Med. 1997, 40, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Elli, M.; Zink, R.; Rytz, A.; Reniero, R.; Morelli, L. Iron requirement of Lactobacillus spp. in completely chemically defined growth media. J. Appl. Microbiol. 2000, 88, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Borchers, A.T.; Selmi, C.; Meyers, F.J.; Keen, C.L.; Gershwin, M.E. Probiotics and immunity. J. Gastroenterol. 2009, 44, 26–46. [Google Scholar] [CrossRef] [PubMed]
- Gill, H.S.; Cross, M.L. Probiotics and immune function. In Nutrition and Immune Function; Calder, P.C., Field, C.J., Gill, H.S., Eds.; CABI Publishing: Wallingford, UK, 2002; pp. 251–272. [Google Scholar]
- Marteau, P.; Shanahan, F. Basic aspects and pharmacology of probiotics: An overview of pharmacokinetics, mechanisms of action and side-effects. Best Pract. Res. Clin. Gastroenterol. 2003, 17, 725–740. [Google Scholar] [CrossRef]
- Schatzmayr, G.; Zehner, F.; Taubel, M.; Schatzmayr, D.; Klimitsch, A.; Loibner, A.P.; Binder, E.M. Microbiologicals for deactivating mycotoxins. Mol. Nutr. Food Res. 2006, 50, 543–551. [Google Scholar] [CrossRef] [PubMed]
- McCormick, S.P. Microbial detoxification of mycotoxins. J. Chem. Ecol. 2013, 39, 907–918. [Google Scholar] [CrossRef] [PubMed]
- Nikbakht Nasrabadi, E.; Jamaluddin, R.; Abdul Mutalib, M.S.; Khaza’ai, H.; Khalesi, S.; Mohd Redzwan, S. Reduction of aflatoxin level in aflatoxin-induced rats by the activity of probiotic Lactobacillus casei strain Shirota. J. Appl. Microbiol. 2013, 114, 1507–1515. [Google Scholar] [CrossRef] [PubMed]
- Upadrasta, A.; Madempudi, R.S. Probiotics and blood pressure: Current insights. Integr. Blood Press. Control 2016, 9, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Khalesi, S.; Sun, J.; Buys, N.; Jayasinghe, R. Effect of probiotics on blood pressure. A Systematic review and meta-analysis of randomized, controlled trials. Hypertension 2014, 70, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Y.; Sun, J.; He, J.; Chen, F.; Chen, R.; Chen, H. Effect of probiotics on glycemic control: A systematic review and meta-analysis of randomized, controlled trials. PLoS ONE 2015, 10, e0132121. [Google Scholar] [CrossRef] [PubMed]
- Lima-Filho, J.V.M.; Vieira, E.C.; Nicoli, J.R. Saccharomyces boulardii and Escherichia coli combinations against experimential infections with Shigella flexneri and Salmonella enteritidis subsp. Typhimurium. J. Appl. Microbiol. 2000, 88, 365–370. [Google Scholar] [CrossRef]
- Bengmark, S. Bioecological control of inflammatory bowel disease. Clin. Nutr. 2007, 26, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Geier, M.S.; Butler, R.N.; Howarth, G.S. Inflammatory bowel disease: Current insights into pathogenesis and new therapeutic options; probiotics, prebiotics and synbiotics. Int. J. Food Microbiol. 2007, 115, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Montalto, M.; Curigliano, V.; Santoro, L.; Vastola, M.; Cammarota, G.; Manna, R.; Gasbarrini, A.; Gasbarrini, G. Management and treatment of lactose malabsorption. World J. Gastroenterol. 2006, 12, 187. [Google Scholar] [CrossRef] [PubMed]
- Levri, K.M.; Ketvertis, K.; Deramo, M.; Merenstein, J.H.; D’Amico, F. Do probiotics reduce adult lactose intolerance? J. Family Pract. 2005, 54, 613–620. [Google Scholar]
- Geier, M.S.; Butler, R.N.; Howarth, G.S. Probiotics, prebiotics and synbiotics: A role in chemoprevention for colorectal cancer? Cancer Biol. Ther. 2006, 5, 1265–1269. [Google Scholar] [CrossRef] [PubMed]
- Lesbros-Pantoflickova, D.; Corthesy-Theulaz, I.; Blum, A.L. Helicobacter pylori and probiotics. J. Nutr. 2007, 137, 812S–818S. [Google Scholar] [PubMed]
- Guarner, F.; Khan, A.G.; Garisch, J.; Eliakim, R.; Gangl, A.; Thomson, A.; Krabshuis, J.; Lemair, T. Probiotics and Prebiotics; World Gastroenterology Organisation Global Guidelines; World Gastroenterology Organisation: Milwaukee, WI, USA, 2011; Volume 46, pp. 468–481. [Google Scholar]
- Falagas, M.E.; Betsi, G.I.; Tokas, T.; Athanasiou, S. Probiotics for prevention of recurrent urinary tract infections in women: A review of the evidence from microbiological and clinical studies. Drugs 2006, 66, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Anukam, K.C.; Osazuwa, E.; Osemene, G.I.; Ehigiagbe, F.; Bruce, A.W.; Reid, G. Clinical study comparing probiotic Lactobacillus GR-1 and RC-14 with metronidazole vaginal gel to treat symptomatic bacterial vaginosis. Microbes Infect. 2006, 8, 2772–2776. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.; Bruce, A.W. Probiotics to prevent urinary tract infections: The rationale and evidence. World J. Urol. 2005, 24, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Kukkonen, K.; Savilahti, E.; Haahtela, T.; Juntunen-Backman, K.; Korpela, R.; Poussa, T.; Tuure, T.; Kuitunen, M. Probiotics and prebiotic galacto-oligosaccharides in the prevention of allergic diseases: A randomized, double-blind, placebo-controlled trial. J. Allergy Clin. Immunol. 2007, 119, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Simons, L.A.; Amansec, S.G.; Conway, P. Effect of Lactobacillus fermentum on serum lipids in subjects with elevated serum cholesterol. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Lieske, J.C.; Goldfarb, D.S.; de Simone, C.; Regnier, C. Use of a probiotic to decrease enteric hyperoxaluria. Kidney Int. 2005, 68, 1244–1249. [Google Scholar] [CrossRef] [PubMed]
- Rousseaux, C.; Thuru, X.; Gelot, A.; Barnich, N.; Neut, C.; Dubuquoy, L.; Dubuquoy, C.; Merour, E.; Geboes, K.; Chamaillard, M.; et al. Lactobacillus acidophilus modulates intestinal pain and induces opioid and cannabinoid receptors. Nat. Med. 2006, 13, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Billoo, A.G.; Memon, M.A.; Khaskheli, S.A.; Murtaza, G.; Iqbal, K.; Saeed Shekhani, M.; Siddiqi, A.Q. Role of a probiotic (Saccharomyces boulardii) in management and prevention of diarrhoea. World J. Gastroenterol. 2006, 12, 4557–4560. [Google Scholar] [CrossRef] [PubMed]
- Parvez, S.; Malik, K.A.; Ah Kang, S.; Kim, H.Y. Probiotics and their fermented food products are beneficial for health. J. Appl. Microbiol. 2006, 100, 1171–1185. [Google Scholar] [CrossRef] [PubMed]
- McFarland, L.V. Meta-Analysis of probiotics for the prevention of antibiotic associated diarrhea and the treatment of Clostridium difficile disease. Am. J. Gastroenterol. 2006, 101, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Hatakka, K.; Savilahti, E.; Pönkä, A.; Meurman, J.H.; Poussa, T.; Näse, L.; Saxelin, M.; Ko, R. Effect of long term consumption of probiotic milk on infections in children attending day care centres: Double blind, randomised trial. Br. Med. J. 2001, 322, 1327. [Google Scholar] [CrossRef]
- Olivares, M.; Diaz-Ropero, M.; Gomez, N.; Sierra, S.; Lara-Villoslada, F.; Martin, R.; Miguel Rodriguez, J.; Xaus, J. Dietary deprivation of fermented foods causes a fall in innate immune response. Lactic acid bacteria can counteract the immunological effect of this deprivation. J. Dairy Res. 2006, 73, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Olivares, M.; Diaz-Ropero, M.A.; Gomez, N.; Lara-Villoslada, F.; Sierra, S.; Maldonado, J.A.; Martin, R.; Lopez-Huertas, E.; Rodriguez, J.M.; Xaus, J. Oral administration of two probiotic strains, Lactobacillus gasseri CECT5714 and Lactobacillus coryniformis CECT5711, enhances the intestinal function of healthy adults. Int. J. Food Microbiol. 2006, 107, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Alvaro, E.; Andrieux, C.; Rochet, V.; Rigottier-Gois, L.; Leprcq, P.; Sutren, M.; Galan, P.; Duval, Y.; Juste, C.; Dore, J. Composition and metabolism of the intestinal microbiota in consumers and non-consumers of yogurt. Br. J. Nutr. 2007, 97, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Larsen, N.; Vogensen, F.K.; Gøbel, R.J.; Michaelsen, K.F.; Forssten, S.D.; Lahtinen, S.J.; Jakobsen, M. Effect of Lactobacillus salivarius Ls-33 on fecal microbiota in obese adolescents. Clin. Nutr. 2013, 32, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Gøbel, R.J.; Larsen, N.; Jakobsen, M.; Mølgaard, C.; Michaelsen, K.F. Probiotics to adolescents with obesity: Effects on inflammation and metabolic syndrome. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Kadooka, Y.; Sato, M.; Imaizumi, K.; Ogawa, A.; Ikuyama, K.; Akai, Y.; Okano, M.; Kagoshima, M.; Tsuchida, T. Regulation of abdominal adiposity by probiotics (Lactobacillus gasseri SBT2055) in adults with obese tendencies in a randomized controlled trial. Eur. J. Clin. Nutr. 2010, 64, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Kadooka, Y.; Sato, M.; Ogawa, A.; Miyoshi, M.; Uenishi, H.; Ogawa, H.; Ikuyama, K.; Kagoshima, M.; Tsuchida, T. Effect of Lactobacillus gasseri SBT2055 in fermented milk on abdominal adiposity in adults in a randomised controlled trial. Br. J. Nutr. 2013, 110, 1696–1703. [Google Scholar] [CrossRef] [PubMed]
- Sharafedtinov, K.K.; Plotnikova, O.A.; Alexeeva, R.I.; Sentsova, T.B.; Songisepp, E.; Stsepetova, J.; Smidt, I.; Mikelsaar, M. Hypocaloric diet supplemented with probiotic cheese improves body mass index and blood pressure indices of obese hypertensive patients—A randomized double-blind placebo-controlled pilot study. Nutr. J. 2013, 12, 138. [Google Scholar] [CrossRef] [PubMed]
- Zarrati, M.; Salehi, E.; Mofid, V.; Hossein Zadeh-Attar, M.J.; Nourijelyani, K.; Bidad, K.; Shidfar, F. Relationship between probiotic consumption and IL-10 and IL-17 secreted by PBMCs in overweight and obese people. Iran. J. Allergy Asthma Immunol. 2013, 12, 404–406. [Google Scholar] [PubMed]
- Zarrati, M.; Salehi, E.; Nourijelyani, K.; Mofid, V.; Zadeh, M.J.; Najafi, F.; Ghaflati, Z.; Bidad, K.; Chamari, M.; Karimi, M.; et al. Effects of probiotic yogurt on fat distribution and gene expression of proinflammatory factors in peripheral blood mononuclear cells in overweight and obese people with or without weight-loss diet. J. Am. Coll. Nutr. 2014, 33, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Zarrati, M.; Shidfar, F.; Nourijelyani, K.; Mofid, V.; Hossein zadeh-Attar, M.J.; Bidad, K.; Najafi, F.; Gheflati, Z.; Chamari, M.; Salehi, E. Lactobacillus acidophilus La5, Bifidobacterium BB12, and Lactobacillus casei DN001 modulate gene expression of subset specific transcription factors and cytokines in peripheral blood mononuclear cells of obese and overweight people. Biofactors 2013, 39, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Agerholm-Larsen, L.; Raben, A.; Haulrik, N.; Hansen, A.S.; Manders, M.; Astrup, A. Effect of 8 week intake of probiotic milk products on risk factors for cardiovascular diseases. Eur. J. Clin. Nutr. 2000, 54, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, H.; Mahmood, N.; Kumar, M.; Varikuti, S.R.; Challa, H.R.; Myakala, S.P. Effect of probiotic (VSL#3) and W-3 on lipid profile, insulin sensitivity, inflammatory markers, and gut colonization in overweight adults: A randomized, controlled trial. Mediat. Inflamm. 2014, 2014, 1–8. [Google Scholar]
- Brahe, L.K.; Le Chatelier, E.; Prifti, E.; Pons, N.; Kennedy, S.; Blædel, T.; Håkansson, J.; Dalsgaard, T.K.; Hansen, T.; Pedersen, O. Dietary modulation of the gut microbiota—A randomised controlled trial in obese postmenopausal women. Br. J. Nutr. 2015, 114, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Ivey, K.L.; Hodgson, J.M.; Kerr, D.A.; Thompson, P.L.; Stojceski, B.; Prince, R.L. The effect of yoghurt and its probiotics on blood pressure and serum lipid profile; a randomised controlled trial. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Leber, B.; Tripolt, N.J.; Blattl, D.; Eder, M.; Wascher, T.C.; Pieber, T.R.; Stauber, R.; Sourij, H.; Oettl, K.; Stadlbauer, V. The influence of probiotic supplementation on gut permeability in patients with metabolic syndrome: An open label, randomized pilot study. Eur. J. Clin. Nutr. 2012, 66, 1110–1115. [Google Scholar] [CrossRef] [PubMed]
- Tripolt, N.J.; Leber, B.; Blattl, D.; Eder, M.; Wonisch, W.; Scharnagl, H.; Stojakovic, T.; Obermayer-Pietsch, B.; Wascher, T.C.; Pieber, T.R.; et al. Effect of supplementation with Lactobacillus casei Shirota on insulin sensitivity, β-cell function, and markers of endothelial function and inflammation in subjects with metabolic syndrome—A pilot study. J. Dairy Sci. 2013, 96, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Barreto, F.M.; Colado Simão, A.N.; Morimoto, H.K.; Batisti Lozovoy, M.A.; Dichi, I.; da Silva Miglioranza, H.L. Beneficial effects of Lactobacillus plantarum on glycemia and homocysteine levels in postmenopausal women with metabolic syndrome. Nutrition 2014, 30, 939–942. [Google Scholar] [CrossRef] [PubMed]
- Hariri, M.; Salehi, R.; Feizi, A.; Mirlohi, M.; Ghiasvand, R.; Habibi, N. A randomized, double-blind, placebo-controlled, clinical trial on probiotic soy milk and soy milk: Effects on epigenetics and oxidative stress in patients with type II diabetes. Genes Nutr. 2015, 10, 52. [Google Scholar] [CrossRef] [PubMed]
- Tonucci, L.B.; Olbrich Dos Santos, K.M.; Licursi de Oliveira, L.; Rocha Ribeiro, S.M.; Duarte Martino, H.S. Clinical application of probiotics in type 2 diabetes mellitus: A randomized, double-blind, placebo-controlled study. Clin. Nutr. 2015, 36, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Mohamadshahi, M.; Veissi, M.; Haidari, F.; Javid, A.Z.; Mohammadi, F.; Shirbeigi, E. Effects of probiotic yogurt consumption on lipid profile in type 2 diabetic patients: A randomized controlled clinical trial. J. Res. Med. Sci. 2014, 19, 531–536. [Google Scholar] [PubMed]
- Ejtahed, H.S.; Mohtadi-Nia, J.; Homayouni-Rad, A.; Niafar, M.; Asghari-Jafarabadi, M.; Mofid, V. Probiotic yogurt improves antioxidant status in type 2 diabetic patients. Nutrition 2012, 28, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Ejtahed, H.S.; Mohtadi-Nia, J.; Homayouni-Rad, A.; Niafar, M.; Asghari-Jafarabadi, M.; Mofid, V.; Akbarian-Moghari, A. Effect of probiotic yogurt containing Lactobacillus acidophilus and Bifidobacterium lactis on lipid profile in individuals with type 2 diabetes mellitus. J. Dairy Sci. 2011, 94, 3288–3294. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, A.S.; Larsen, N.; Pedersen-Skovsgaard, T.; Berg, R.M.; Møller, K.; Svendsen, K.D.; Jakobsen, M.; Pedersen, B.K. Effects of Lactobacillus acidophilus NCFM on insulin sensitivity and the systemic inflammatory response in human subjects. Br. J. Nutr. 2010, 104, 1831–1838. [Google Scholar] [CrossRef] [PubMed]
- Vajro, P.; Mandato, C.; Licenziati, M.R.; Franzese, A.; Vitale, D.F.; Lenta, S.; Caropreso, M.; Vallone, G.; Meli, R. Effects of Lactobacillus rhamnosus strain GG in pediatric obesity-related liver disease. J. Gastroenterol. Nutr. 2011, 52, 740–743. [Google Scholar] [CrossRef] [PubMed]
- Aller, R.; de Luis, D.A.; Izaola, O.; Conde, R.; Gonzalez Sagrado, M.; Primo, D.; de la Fuente, B.; Gonzalez, J. Effect of a probiotic on liver aminotransferases in nonalcoholic fatty liver disease patients: A double blind randomized clinical trial. Eur. Rev. Med. Pharmacol. Sci. 2011, 15, 1090–1095. [Google Scholar] [PubMed]
- Nabavi, S.; Rafraf, M.; Somi, M.H.; Homayouni-Rad, A.; Asghari-Jafarabadi, M. Effects of probiotic yogurt consumption on metabolic factors in individuals with nonalcoholic fatty liver disease. J. Dairy Sci. 2014, 97, 7386–7393. [Google Scholar] [CrossRef] [PubMed]
- Alisi, A.; Bedogni, G.; Baviera, G.; Giorgio, V.; Porro, E.; Paris, C.; Giammaria, P.; Reali, L.; Anania, F.; Nobili, V. Randomised clinical trial: The beneficial effects of VLS_3 in obese children with non-alcoholic steatohepatitis. Aliment. Pharmacol. Ther. 2014, 39, 1276–1285. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.Y.; Li, S.N.; Liu, C.S.; Perng, D.S.; Su, Y.C.; Wu, D.C.; Jan, C.M.; Lai, C.H.; Wang, T.N.; Wang, W.M. Effects of ingesting Lactobacillus- and Bifidobacterium-containing yogurt in subjects with colonized Helicobacter pylori. Am. J. Clin. Nutr. 2005, 81, 939–940. [Google Scholar]
- Cats, A.; Kuipers, E.J.; Bosschaert, M.A.; Pot, R.G.; Vandenbroucke-Grauls, C.M.; Kusters, J.G. Effect of frequent consumption of Lactobacillus casei—Containing milk drink in Helicobacter pylori-colonized subjects. Aliment. Pharmacol. Ther. 2003, 17, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Kotowska, M.; Albrecht, P.; Szajewska, H. Saccharomyces boulardii in the prevention of antibiotic-associated diarrhoea in children: A randomized double-blind placebo-controlled trial. Aliment. Pharmacol. Ther. 2005, 21, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Sood, A.; Midha, V.; Makharia, G.K.; Ahuja, V.; Singal, D.; Goswami, P.; Tandon, R.K. The probiotic preparation, VSL#3 induces remission in patients with mild-to-moderately active ulcerative colitis. Clin. Gastroenterol. Hepatol. 2009, 7, 1202–1209. [Google Scholar] [CrossRef] [PubMed]
- Niv, E.; Naftali, T.; Hallak, R.; Vaisman, N. The efficacy of Lactobacillus reuteri ATCC 55730 in the treatment of patients with irritable bowel syndrome–A double blind, placebo-controlled, randomized study. Clin. Nutr. 2005, 24, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Wickens, K.; Black, P.N.; Stanley, T.V.; Mitchell, E.; Fitzharris, P.; Tannock, G.W.; Purdie, G.; Crane, J. A differential effect of 2 probiotics in the prevention of eczema and atopy: A double-blind, randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2008, 122, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Weston, S.; Halbert, A.; Richmond, P.; Prescott, S.L. Effects of probiotics on atopic dermatitis: A randomised controlled trial. Arch. Dis. Child. 2005, 90, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Niers, L.; Martı́n, R.; Rijkers, G.; Sengers, F.; Timmerman, H.; van Uden, N.; Smidt, H.; Kimpen, J.; Hoekstra, M. The effects of selected probiotic strains on the development of eczema (the PandA study). Allergy 2009, 64, 1349–1358. [Google Scholar] [CrossRef] [PubMed]
- Gøbel, R.J.; Larsen, N.; Mølgaard, C.; Jakobsen, M.; Michaelsen, K.F. Probiotics to young children with atopic dermatitis: A randomized placebo-controlled trial. Int. J. Probiotics Prebiotics 2010, 5, 53–60. [Google Scholar]
- Hertzler, S.R.; Clancy, S.M. Kefir improves lactose digestion and tolerance in adults with lactose maldigestion. J. Am. Dietetic Assoc. 2003, 103, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Roškar, I.; Švigelj, K.; Štempelj, M.; Volfand, J.; Štabuc, B.; Malovrh, Š.; Rogelj, I. Effects of a probiotic product containing Bifidobacterium animalis subsp. animalis IM386 and Lactobacillus plantarum MP2026 in lactose intolerant individuals: Randomized, placebo-controlled clinical trial. J. Funct. Foods 2017, 35, 1–8. [Google Scholar] [CrossRef]
- Liu, Z.; Qin, H.; Yang, Z.; Xia, Y.; Liu, W.; Yang, J.; Jiang, Y.; Zhang, H.; Wang, Y.; Zheng, Q. Randomized clinical trial: The effects of perioperative probiotic treatment on barrier function and post-operative infectious complications in colorectal cancer surgery—A double-blind study. Aliment. Pharmacol. Ther. 2011, 33, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Chitapanarux, I.; Chitapanarux, T.; Traisathit, P.; Kudumpee, S.; Tharavichitkul, E.; Lorvidhaya, V. Randomized controlled trial of live Lactobacillus acidophilus plus Bifidobacterium bifidum in prophylaxis of diarrhea during radiotherapy in cervical cancer patients. Radiat. Oncol. 2010, 5, 31. [Google Scholar] [CrossRef] [PubMed]
- Österlund, P.; Ruotsalainen, T.; Korpela, R.; Saxelin, M.; Ollus, A.; Valta, P.; Kouri, M.; Elomaa, I.; Joensuu, H. Lactobacillus supplementation for diarrhoea related to chemotherapy of colorectal cancer: A randomised study. Br. J. Cancer 2007, 97, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.S.F.; Walker, A.W.; Louis, P.; Parkhill, J.; Vermeiren, J.; Bosscher, D.; Duncan, S.H.; Flint, H.J. Modulation of the human gut microbiota by dietary fibres occurs at the species level. BMC Biol. 2016, 14, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Crittenden, R.; Playne, M.J. Nutrition News. Facts and functions of prebiotics, probiotics and synbiotics. In Handbook of Probiotics and Prebiotics; Lee, Y.K., Salminen, S., Eds.; Wiley-Interscience, Kansas State University: Hoboken, NJ, USA; Manhattan, KS, USA, 2008; pp. 535–582. [Google Scholar]
- Jakubczyk, E.; Kosikowska, M. Nowa generacja mlecznych produktów fermentowanych z udziałem probiotyków i prebiotyków, produkty synbiotyczne. Prz. Mlecz. 2000, 12, 397–400. [Google Scholar]
- Wang, Y. Prebiotics: Present and future in food science and technology. Food Res. Int. 2009, 42, 8–12. [Google Scholar] [CrossRef]
- Maccfarlane, G.T.; Steed, H.; Maccfarlane, S. Bacterial metabolism and health-related effects of galacto-oligosaccharides and other prebiotics. J. Appl. Microbiol. 2008, 104, 305–344. [Google Scholar] [CrossRef] [PubMed]
- Crittenden, R.; Playne, M.J. Prebiotics. In Handbook of Probiotics and Prebiotics; Lee, Y.K., Salminen, S., Eds.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2009; pp. 535–561. [Google Scholar]
- Huebner, J.; Wehling, R.L.; Parkhurst, A.; Hutkins, R.W. Effect of processing conditions on the prebiotic activity of commercial prebiotics. Int. Dairy J. 2008, 18, 287–293. [Google Scholar] [CrossRef]
- Ze, X.; Duncan, S.H.; Louis, P.; Flint, H.J. Ruminococcus bromii is a keystone species for the degradation of resistant starch in the human colon. ISME J. 2012, 6, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Angelakis, E. Weight gain by gut microbiota manipulation in productive animals. Microb. Pathog. 2017, 106, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Śliżewska, K.; Nowak, A.; Barczyńska, R.; Libudzisz, Z. Prebiotyki—Definicja, właściwości i zastosowanie w przemyśle. Żywność Nauka Technologia Jakość 2013, 1, 5–20. [Google Scholar]
- Sivieri, K.; Morales, M.L.V.; Saad, S.M.I.; Adorno, M.A.T.; Sakamoto, I.K.; Rossi, E.A. Prebiotic effect of fructooligosaccharide in the simulator of the human intestinal microbial ecosystem (SHIME (R) Model). J. Med. Food 2014, 17, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Van Den Abbeele, P.; Venema, K.; van de Wiele, T.; Verstraete, W.; Possemiers, S. Different human gut models reveal the distinct fermentation patterns of arabinoxylan versus inulin. J. Agric. Food Chem. 2013, 61, 9819–9827. [Google Scholar] [CrossRef] [PubMed]
- Ouwehand, A.; Derrien, M.; de Vos, W.; Tiihonen, K.; Rautonen, N. Prebiotics and other microbial substrates for gut functionality. Curr. Biol. 2005, 16, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.A.; Burkholder, K.M. Application of prebiotics and probiotics in poultry production. Poult. Sci. 2003, 82, 627–631. [Google Scholar] [CrossRef] [PubMed]
- Annison, G.; Illman, R.; Topping, D. Acetylated, propionylated or butyrylated starches raise large bowel short-chain fatty acids preferentially when fed to rats. J. Nutr. 2003, 133, 3523–3528. [Google Scholar] [PubMed]
- Baurhoo, B.; Letellier, A.; Zhao, X.; Ruiz-Feria, C.A. Cecal populations of Lactobacilli and Bifidobacteria and Escherichia coli after In Vivo Escherichia coli challenge in birds fed diets with purified lignin or mannanoligo-saccharides. Poult. Sci. 2007, 86, 2509–2516. [Google Scholar] [CrossRef] [PubMed]
- Olveira, G.; González-Molero, I. An update on probiotics, prebiotics and symbiotics in clinical nutrition. Endocrinol. Nutr. 2016, 63, 482–494. [Google Scholar] [CrossRef] [PubMed]
- Sáez-Lara, M.J.; Robles-Sanchez, C.; Ruiz-Ojeda, F.J.; Plaza-Diaz, J.; Gil, A. Effects of probiotics and synbiotics on obesity, insulin resistance syndrome, type 2 diabetes and non-alcoholic fatty liver disease: A review of human clinical trails. Int. J. Mol. Sci. 2016, 17, 928. [Google Scholar] [CrossRef] [PubMed]
- Van Loo, J.; Clune, Y.; Bennett, M.; Collins, J.K. The SYNCAN project: Goals, set-up, first results and settings of the human intervention study. Br. J. Nutr. 2005, 93, S91–S98. [Google Scholar] [PubMed]
- Schiffrin, E.J.; Kumar, V.B.; Brown, C.; Hager, C.; Van’t Hof, M.A.; Morley, J.E.; Guigoz, Y. Systemic inflammatory markers in older persons: The effect of oral nutritional supplementation with prebiotics. J. Nutr. Health Aging 2007, 11, 475–479. [Google Scholar] [PubMed]
- Vulevic, J.; Drakoularakou, A.; Yaqoob, P.; Tzortzis, G.; Gibson, G.R. Modulation of the fecal microflora profile and immune function by a novel transgalactooligosaccharide mixture (B-GOS) in healthy elderly volunteers. Am. J. Clin. Nutr. 2008, 88, 1438–1446. [Google Scholar] [PubMed]
- Schley, P.D.; Field, C.J. The immune-enhancing effects of dietary fibres and prebiotics. Br. J. Nutr. 2002, 87, S221–S230. [Google Scholar] [CrossRef] [PubMed]
- Grajek, W.; Olejnik, A.; Sip, A. Probiotics, prebiotics and antioxidants as functional foods. Acta Biochim. Pol. 2005, 52, 665–671. [Google Scholar] [PubMed]
- Gibson, G.R.; Wang, X. Regulatory effects of bifidobacteria on the growth of other colonic bacteria. J. Appl. Microbiol. 1994, 77, 412–420. [Google Scholar] [CrossRef]
- Bovee-Oudenhoven, I.M.J.; Termont, D.S.; Heidt, P.J.; van der Meer, R. Increasing the intestinal resistance of rats to the invasive pathogen Salmonella enteritidis: Additive effects of dietary lactulose and calcium. Gut 1997, 40, 497–504. [Google Scholar] [CrossRef] [PubMed]
- De Preter, V.; Hamer, H.M.; Windey, K.; Verbeke, K. The impact of pre- and/or probiotics on human colonic metabolism: Does it affect human health? Mol. Nutr. Food Res. 2011, 55, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Demigné, C.; Jacobs, H.; Moundras, C.; Davicco, M.J.; Horcajada, M.N.; Bernalier, A.; Coxam, V. Comparison of native or reformulated chicory fructans, or non-purified chicory, on rat cecal fermentation and mineral metabolism. Eur. J. Nutr. 2008, 47, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Mojka, K. Probiotyki, prebiotyki i synbiotyki—Charakterystyka i funkcje. Probl. Hig. Epidemiol. 2014, 95, 541–549. [Google Scholar]
- Socha, P.; Stolarczyk, M.; Socha, J. Wpływ probiotyków i prebiotyków na gospodarkę lipidową. Pediatr. Współcz. Gastroenterol. Hepatol. Żyw. Dziecka 2002, 4, 85–88. [Google Scholar]
- Asahara, T.; Nomoto, K.; Shimizu, K.; Watanuki, M.; Tanaka, R. Increased resistance of mice to Salmonella enteritica serovar Typhymurium infection by synbiotic administration of bifidobacteria and transgalactosylated-oligosaccharides. J. Appl. Microbiol. 2001, 91, 985–996. [Google Scholar] [CrossRef] [PubMed]
- Buddington, K.K.; Danohoo, J.B.; Buddington, R.K. Dietary oligofructose and inulin protect mice from enteric and systemic pathogens and tumour inducers. J. Nutr. 2002, 132, 472–477. [Google Scholar] [PubMed]
- Cummings, J.H.; Macfarlane, G.T. Gastrointestinal effects of prebiotics. Br. J. Nutr. 2002, 87, 145–151. [Google Scholar] [CrossRef]
- Scheppach, W.; Weiler, F. The butyrate story: Old wine in new bottles? Butyrate appears to be essential for a wide range of intestinal mucosal health benefits; however, the mechanisms behind this remain to be determined. Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Tsa, O.D.; Morita, A.; Bella, A. Effect of sodium butyrate and three human colorectal adenocarcinoma cell lines in culture. Falk Symp. 1982, 31, 317–323. [Google Scholar]
- Munjal, U.; Glei, M.; Pool-Zobel, B.L.; Scharlau, D. Fermentation products of inulin-type fructans reduce proliferation and induce apoptosis in human colon tumour cells of different stages of carcinogenesis. Br. J. Nutr. 2009, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Verghese, M.; Rao, D.R.; Chawan, C.B.; Williams, L.L.; Shackelford, L. Dietary inulin suppresses azoxymethane-induced aberrant crypt foci and colon tumors at the promotion stage in young Fisher 344 rats. J. Nutr. 2002, 132, 2809–2813. [Google Scholar] [PubMed]
- Taper, H.S.; Roberfroid, M.B. Inulin/Oligofructose and anticancer therapy. Br. J. Nutr. 2002, 87, 283–286. [Google Scholar] [CrossRef]
- Parnell, J.A.; Reimer, R.A. Weight loss during oligofructose supplementation is associated with decreased ghrelin and increased peptide YY in overweight and obese adults. Am. J. Clin. Nutr. 2009, 89, 1751–1759. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; van Yperselle, M.; Rizkalla, S.W.; Rossi, F.; Bornet, F.R.; Slama, G. Chronic consumption of short-chain fructooligosaccharides does not affect basal hepatic glucose production or insulin resistance in type 2 diabetics. J. Nutr. 2000, 130, 1572–1577. [Google Scholar] [PubMed]
- Lu, Z.X.; Walker, K.Z.; Muir, J.G.; O’Dea, K. Arabinoxylan fibre improves metabolic control in people with type II diabetes. Eur. J. Clin. Nutr. 2004, 58, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.L.; Otto, B.; Reich, S.C. Arabinoxylan consumption decreases postprandial serum glucose, serum insulin and plasma total ghrelin response in subjects with impaired glucose tolerance. Eur. J. Clin. Nutr. 2007, 61, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Daubioul, C.A.; Horsmans, Y.; Lambert, P.; Danse, E.; Delzenne, N.M. Effects of oligofructose on glucose and lipid metabolism in patients with nonalcoholic steatohepatitis: Results of a pilot study. Eur. J. Clin. Nutr. 2005, 59, 723–726. [Google Scholar] [CrossRef] [PubMed]
- Bruzzese, E.; Volpicelli, M.; Salvini, F.; Bisceglia, M.; Lionetti, P.; Cinquetti, M.; Iacono, G.; Guarino, A. Early administration of GOS/FOS prevents intestinal and respiratory infections in infants. J. Pediatr. Gastroenterol. Nutr. 2006, 42, E95. [Google Scholar]
- Costalos, C.; Kapiki, A.; Apostolou, M.; Papathoma, E. The effect of a prebiotic supplemented formula on growth and stool microbiology of term infants. Early Hum. Dev. 2008, 84, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Scholtens, P.A.; Alliet, P.; Raes, M.; Alles, M.S.; Kroes, H.; Boehm, G.; Knippels, L.M.; Knol, J.; Vandenplas, Y. Fecal secretory immunoglobulin A is increased in healthy infants who receive a formula with short-chain galacto-oligosaccharides and long-chain fructo-oligosaccharides. J. Nutr. 2008, 138, 1141–1147. [Google Scholar] [PubMed]
- Welters, C.F.; Heineman, E.; Thunnissen, F.B.; van den Bogaard, A.E.; Soeters, P.B.; Baeten, C.G. Effect of dietary inulin supplementation on inflammation of pouch mucosa in patients with an ileal pouch-anal anastomosis. Dis. Colon Rectum 2002, 45, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, J.O.; Whelan, K.; Stagg, A.J.; Gobin, P.; Al-Hassi, H.O.; Rayment, N.; Forbes, A. Clinical, microbiological, and immunological effects of fructo-oligosaccharide in patients with Crohn’s disease. Gut 2006, 55, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Moro, G.; Arslanoglu, S.; Stahl, B.; Jelinek, J.; Wahn, U.; Boehm, G. A mixture of prebiotic oligosaccharides reduces the incidence of atopic dermatitis during the first six months of age. Arch. Dis. Child. 2006, 91, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Arslanoglu, S.; Moro, G.E.; Boehm, G. Early supplementation of prebiotic oligosaccharides protects formula-fed infants against infections during the first 6 months of life. J. Nutr. 2007, 137, 2420–2424. [Google Scholar] [PubMed]
- Azcarate-Peril, M.A.; Ritter, A.J.; Savaiano, D.; Monteagudo-Mera, A.; Anderson, C.; Magness, S.T.; Klaenhammer, T.R. Impact of short-chain galactooligosaccharides on the gut microbiome of lactose-intolerant individuals. Proc. Natl. Acad. Sci. USA 2017, 114, E367–E375. [Google Scholar] [CrossRef] [PubMed]
- Gourbeyre, P.; Denery, S.; Bodinier, M. Probiotics, prebiotics, and synbiotics: Impact on the gut immune system and allergic reactions. J. Leukoc. Biol. 2011, 89, 685–695. [Google Scholar] [CrossRef] [PubMed]
- De Vrese, M.; Schrezenmeir, J. Probiotics, prebiotics and synbiotics. In Food Biotechnology, Advances in Biochemical Engineering/Biotechnology; Stahl, U., Donalies, U.E.B., Nevoigt, E., Eds.; Springer: Berlin, Germany, 2008; pp. 1–66. [Google Scholar] [CrossRef]
- Scavuzzi, B.M.; Henrique, F.C.; Miglioranza, L.H.S.; Simão, A.N.C.; Dichi, I. Impact of prebiotics, probiotics and synbiotics on components of the metabolic syndrome. Ann. Nutr. Disord. Ther. 2014, 1, 1009. [Google Scholar]
- Hamasalim, H.J. Synbiotic as feed additives relating to animal health and performance. Adv. Microbiol. 2016, 6, 288–302. [Google Scholar] [CrossRef]
- Sekhon, B.S.; Jairath, S. Prebiotics, probiotics and synbiotics: An overview. J. Pharm. Educ. Res. 2010, 1, 13–36. [Google Scholar]
- Manigandan, T.; Mangaiyarkarasi, S.P.; Hemaltha, R.; Hemaltha, V.T.; Murali, N.P. Probiotics, prebiotics and synbiotics—A review. Biomed. Pharmacol. J. 2012, 5, 295–304. [Google Scholar] [CrossRef]
- Pandey, K.R.; Naik, S.R.; Babu, V.V. Probiotics, prebiotics and synbiotics—A review. J. Food. Sci. Technol. 2015, 52, 7577–7587. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.M.; Cheng, J.Q.; Lu, Y.R.; Yi, Z.H.; Yang, P.; Wu, X.T. Use of pre-, pro-and synbiotics in patients with acute pancreatitis: A meta-analysis. World J. Gastroenterol. 2010, 16, 3970. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Won, G.L.; Chim, A.M.; Chu, W.C.; Yeung, D.K.; Li, K.C.; Chan, L. Treatment of nonalcoholic steatohepatitis with probiotics. A proof-of-concept study. Ann. Hepatol. 2013, 12, 256–262. [Google Scholar] [PubMed]
- Eslamparast, T.; Poustchi, H.; Zamani, F.; Sharafkhah, M.; Malekzadeh, R.; Hetmatdoost, A. Synbiotic supplementation in nonalcoholic fatty liver disease: A randomized, double-blind, placebo-controlled pilot study. Am. J. Clin. Nutr. 2014, 99, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Pathmakanthan, S.; Walsh, M.; Bengmark, S. Efficacy and Tolerability Treating Acute Distal Ulcerative Colitis with Synbiotic Enemas: A Pilot Trial (Abstract); United European Gastroenterology Week: Geneva, Switzerland, 2002. [Google Scholar]
- Pérez-Conesa, D.; López, G.; Abellán, P.; Ros, G. Bioavailability of calcium, magnesium and phosphorus in rats fed probiotic, prebiotic and synbiotic powder follow-up infant formulas and their effect on physiological and nutritional parameters. J. Sci. Food Agric. 2006, 86, 2327–2336. [Google Scholar] [CrossRef]
- Danq, D.; Zhou, W.; Lun, Z.J.; Mu, X.; Wanq, D.X.; Wu, H. Meta-analysis of probiotics and/or prebiotics for the prevention of eczema. J. Int. Med. Res. 2013, 41, 1426–1436. [Google Scholar] [CrossRef] [PubMed]
- Rafter, J.; Bennett, M.; Caderni, G.; Clune, I.; Hughes, R.; Karlsson, P.C.; Klinder, A.; O’Riordan, M.; O’Sullivan, G.; Pool-Zobel, B.; et al. Dietary synbiotics reduce cancer risk factors in polypectomized and colon cancer patients. Am. J. Clin. Nutr. 2007, 85, 488–496. [Google Scholar] [PubMed]
- Sanchez, M.; Darimont, C.; Drapeau, V.; Emady-Azar, S.; Lepage, M.; Rezzonico, E.; Ngom-Bru, C.; Berger, B.; Philippe, L.; Ammon-Zuffrey, C.; et al. Effect of Lactobacillus rhamnosus CGMCC1.3724 supplementation on weight loss and maintenance in obese men and women. Br. J. Nutr. 2014, 111, 1507–1519. [Google Scholar] [CrossRef] [PubMed]
- Safavi, M.; Farajian, S.; Kelishadi, R.; Mirlohi, M.; Hashemipour, M. The effects of synbiotic supplementation on some cardio metabolic risk factors in overweight and obese children: A randomized triple-masked controlled trial. Int. J. Food Sci. Nutr. 2013, 64, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Ipar, N.; Aydogdu, S.D.; Yildirim, G.K.; Inal, M.; Gies, I.; Vandenplas, Y.; Dinleyici, E.C. Effects of symbiotic on anthropometry, lipid profile and oxidative stress in obese children. Benef. Microbes 2015, 6, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Eslamparast, T.; Zamani, F.; Hekmatdoost, A.; Sharafkhah, M.; Eghtesad, S.; Malekzadeh, R.; Poustchi, H. Effects of synbiotic supplementation on insulin resistance in subjects with the metabolic syndrome: A randomised, double-blind, placebo-controlled pilot study. Br. J. Nutr. 2014, 112, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Zohreh, Z.; Shakeri, H.; Sima-sadat Sabihi, S.S.; Esmaillzadeh, A. Effect of multispecies probiotic supplements on metabolic profiles, hs-CRP, and oxidative stress in patients with type 2 diabetes. Ann. Nutr. Metab. 2013, 63, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Tajadadi-Ebrahimi, M.; Bahmani, F.; Shakeri, H.; Hadaegh, H.; Hijijafari, M.; Abedi, F.; Asemi, Z. Effects of daily consumption of synbiotic bread on insulin metabolism and serum high-sensitivity C-reactive protein among diabetic patients: A double-blind, randomized, controlled clinical trial. Ann. Nutr. Metab. 2014, 65, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Shakeri, H.; Hadaegh, H.; Abedi, F.; Tajabadi-Ebrahimi, M.; Mazroii, N.; Ghandi, Y.; Asemi, Z. Consumption of synbiotic bread decreases triacylglycerol and VLDL levels while increasing HDL levels in serum from patients with type-2 diabetes. Lipids 2014, 49, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Moroti, C.; Souza Magri, L.F.; Rezende-Costa, M.; Cavallini, D.; Sivieri, K. Effect of the consumption of a new symbiotic shake on glycemia and cholesterol levels in elderly people with type 2 diabetes mellitus. Lipids Health Dis. 2012, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Šmid, A.; Strniša, L.; Bajc, K.; Vujić-Podlipec, D.; Bogovič Matijašić, B.; Rogelj, I. Randomized clinical trial: The effect of fermented milk with the probiotic cultures Lactobacillus acidophilus La-5® and Bifidobacterium BB-12® and Beneo dietary fibres on health-related quality of life and the symptoms of irritable bowel syndrome in adults. J. Funct. Foods 2016, 24, 549–557. [Google Scholar] [CrossRef]
- Ustundag, G.H.; Altuntas, H.; Soysal, Y.D.; Kokturk, F. The effects of synbiotic “Bifidobacterium lactis B94 plus Inulin” addition on standard triple therapy of Helicobacter pylori eradication in children. Can. J. Gastroenterol. Hepatol. 2017, 2017, 8130596. [Google Scholar] [CrossRef] [PubMed]
- Fujimori, S.; Gudis, K.; Mitsui, K.; Seo, T.; Yonezawa, M.; Tanaka, S.; Tatsuguchi, A.; Sakamoto, C. A randomized controlled trial on the efficacy of synbiotic versus probiotic or prebiotic treatment to improve the quality of life in patients with ulcerative colitis. Nutrition 2009, 25, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Van der Aa, L.B.; Heymans, H.S.A.; van Aalderen, W.M.C.; Sillevis Smitt, J.H.; Knol, J.; Ben Amor, K.; Goossens, D.A.; Sprikkelman, A.B. Effect of a new synbiotic mixture on atopic dermatitis in infants: A randomized controlled trial. Clin. Exp. Allergy 2010, 40, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Farid, R.; Ahanchian, H.; Jabbari, F.; Moghiman, T. Effect of a new synbiotic mixture on atopic dermatitis in children: A randomized-controlled trial. Iran. J. Pediatr. 2011, 21, 225–230. [Google Scholar] [PubMed]
- Post, J. Acceptability and Feasibility of Probiotic and Prebiotic Supplementation in Alleviating Symptoms of Lactose Maldigestion in Lactose Intolerant Subjects; Florida State University: Tallahassee, FL, USA, 2013. [Google Scholar]
- Nowak, A.; Śliżewska, K.; Libudzisz, Z. Probiotyki—Historia i mechanizmy działania. Żywność Nauka Technologia Jakość 2010, 4, 5–19. [Google Scholar]
- Bomba, A.; Nemcova, R.; Mudronova, D.; Guba, P. The possibilities of potentiating the efficacy of probiotics. Trends Food Sci. Technol. 2002, 13, 121–126. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Criterion | Required Properties |
|---|---|
| Safety |
|
| Functionality |
|
| Technological usability |
|
| Type Lactobacillus | Type Bifidobacterium | Other Lactic Acid Bacteria | Other Microorganisms |
|---|---|---|---|
| L. acidophilus (a),* L. amylovorus (b),* L. casei (a),(b),* L. gasseri (a),* L. helveticus (a),* L. johnsonii (b),* L. pentosus (b),* L. plantarum (b),* L. reuteri (a),* L. rhamnosus (a),(b),* | B. adolescentis (a) B. animalis (a),* B. bifidum (a) B. breve (b) B. infantis (a) B. longum (a),* | Enterococcus faecium (a) Lactococcus lactis (b),* Streptococcus thermophilus (a),* | Bacillus clausii (a),* Escherichia coli Nissle 1917 (a) Saccharomyces cerevisiae (boulardi) (a),* |
| References | Subjects | Microorganism | Time of Administration | Main Outcome |
|---|---|---|---|---|
| Obesity | ||||
| [90] | 50 obese adolescents | L. salivarius Ls-33 | 12 weeks | Increase in the ratios of Bacteroides, Prevotellae, and Porphyromonas. |
| [91] | 50 adolescents with obesity | L. salivarius Ls-33 | 12 weeks | No effect. |
| [92] | 87 subjects with high BMI | L. gasseri SBT2055 | 12 weeks | Reduction in BMI, waist, abdominal VFA, and hip circumference. |
| [93] | 210 adults with large VFA | L. gasseri SBT2055 | 12 weeks | Reduction in BMI and arterial BP values. |
| [94] | 40 adults with obesity | L. plantarum | 3 weeks | Reduction in BMI and arterial BP values. |
| [95,96,97] | 75 subjects with high BMI | L. acidophilus La5, B. lactis Bb12, L. casei DN001 | 8 weeks | Changes in gene expression in PBMCs as well as BMI, fat percentage, and leptin levels. |
| [98] | 70 overweight and obese subjects | E. faecium and 2, S. thermophilus strains | 8 weeks | Reduction in body weight, systolic BP, LDL-C, and increase in fibrinogen levels. |
| [99] | 60 overweight subjects | Bifidobacterium, Lactobacillus, S. thermophilus | 6 weeks | Improvement in lipid profile, insulin sensitivity, and decrease in CRP. |
| [100] | 58 obese PM women | L. paracasei N19 | 6 weeks | No effect. |
| [101] | 156 overweight adults | L. acidophilus La5, B. animalis subsp. lactis Bb12 | 6 weeks | Reduction in fasting glucose concentration and increase in HOMA-IR. |
| Insulin resistance syndrome | ||||
| [102] | 28 patients with IRS | L. casei Shirota | 12 weeks | No effect. |
| [103] | 30 patients with IRS | L. casei Shirota | 12 weeks | Significant reduction in the VCAM-1 level. |
| [104] | 24 PM women with IRS | L. plantarum | 12 weeks | Glucose and homocysteine levels were significantly reduced. |
| Type 2 diabetes | ||||
| [105] | 40 patients with T2D | L. planatarum A7 | 8 weeks | Decreased methylation process, SOD, and 8-OHDG. |
| [106] | 45 patients with T2D | L. acidophilus La-5, B. animalis subsp. lactis BB-12 | 6 weeks | Significant difference between groups concerning mean changes of HbA1c, TC, and LDL-C. |
| [107] | 44 patients with T2D | L. acidophilus La-5, B. animalis subsp. lactis BB-12 | 8 weeks | Increased HDL-C levels and decreased LDL-C/HDL-C ratio. |
| [108] | 64 patients with T2D | L. acidophilus La5, B. lactis Bb12 | 6 weeks | Reduced fasting blood glucose and antioxidant status. |
| [109] | 60 patients with T2D | L. acidophilus La5, B. lactis Bb12 | 6 weeks | TC and LDL-C improvement. |
| [110] | 45 males with T2D | L. acidophilus NCFM | 4 weeks | No effect. |
| Non-alcoholic fatty liver disease | ||||
| [111] | 20 obese children with NAFLD | L. rhamnosus GG | 8 weeks | Decreased ALT and PG-PS IgAg antibodies. |
| [112] | 28 adult individuals with NAFLD | L. bulgaris, S. thermophilus | 12 weeks | Decreased ALT and γ-GTP levels. |
| [113] | 72 patients with NAFLD | L.acidophilus La5, B. breve subsp. lactis Bb12 | 8 weeks | Reduced serum levels of ALT, ASP, TC, and LDL-C. |
| [114] | 44 obese children with NAFLD | Bifidobacterium, Lactobacillus, S. thermophilus | 16 weeks | Improved fatty liver severity, decreased BMI, and increased GLP1/aGLP1. |
| Irritable bowel syndrome (IBS), gastrointestinal disorders, elimination of Helicobacter, inflammatory bowel disease (IBD), diarrhoeas | ||||
| [115] | 59 adults infected with H. pylori | L. acidophilus La5, B. lactis Bb12 | 6 weeks | Inhibitory effect against Helicobacter pylori. |
| [116] | 16 patients infected with H. pylori | L. casei Shirota | 6 weeks | Inhibited growth of Helicobacter pylori (by 64% in the probiotic group, and by 33% in the control). |
| [117] | 269 children with otitis media and/or respiratory tract infections | S. cerevisiae (boulardii) | No data | Diarrhoea was less common in children receiving probiotic yeast (7.5%) compared to those receiving placebo (23%). No negative side effects were observed. |
| [118] | 77 patients with ulcerative colitis | Probiotic VSL#3 | 12 weeks | Remission in 42.9% of patients in the probiotic group, and in 15.7% of patients in the placebo group. |
| [119] | 90 breastfed neonates with intestinal colic | L. reuteri ATCC 55730 | 6 months | Elimination of pain and symptoms associated with intestinal colic already after one week of the use of the probiotic. |
| Atopic dermatitis | ||||
| [120] | 512 pregnant women and 474 their newborn infants | L. rhamnosus HN001 | women—from 35 weeks gestation until 6 months if breastfeeding, infants—from birth to 2 years | Substantially reduced the cumulative prevalence of eczema in infants. |
| [121] | 53 children with moderate of severe atopic dermatitis | L. fermentum VRI 033 PCCTM | 8 weeks | Reduction in SCORAD. |
| [122] | 156 mothers of high-risk children (i.e., positive family history of allergic disease) and their offspring | B. bifidum, B. lactis, L. lactis | Mothers—the last 6 weeks of pregnancy, offspring—12 months | Significantly reduction eczema in high-risk for a minimum of 2 years provided that the probiotic was administered to the infant within 3 months of birth. |
| [123] | 50 children with AD | B. animalis subsp lactis | 8 weeks | Significant reduction in the severity of AD with an improved ration of IFN-γ and IL-10. |
| Alleviation of lactose intolerance | ||||
| [124] | 15 healthy, free-living adults with lactose maldigestion | S. lactis, L. plantarum, S. cremoris, L. casei, S. diacetylactis, S. florentinus, L. cremoris | 1 day | Improved lactose digestion and tolerance. |
| [125] | 44 patients | B. animalis subsp. animalis IM386 (DSM 26137), L. plantarum MP2026 (DSM 26329) | 6 weeks | A significant lowering effect on diarrhoea and flatulence. |
| Different types of cancer and side effects associated with cancer | ||||
| [126] | 100 patients with colorectal carcinoma | L. plantarum CGMMCC No 1258, L. acidophilus LA-11, B. longum BL-88 | 16 days | Improvement in the integrity of gut mucosal barrier and decrease in infections complications. |
| [127] | 63 patients with diarrhoea during radiotherapy in cervical cancer | L. acidophilus, B. bifidum | 7 weeks | Reduction in incidence of diarrhoea and better stool consistency. |
| [128] | 150 patients diagnosed with colorectal cancer | L. rhamnosus 573 | 24 weeks | Patients had less grade 4 or 4 diarrhoea, less abdominal discomfort, needed less hospital care, and had fewer chemo dose reductions due to bowel toxicity. |
| Human Nutrition | |
|---|---|
| Prebiotics | Synbiotics |
| FOS GOS Inulin XOS Lactitol Lactosucrose Lactulose Soy oligosaccharides TOS | Lactobacillus genus bacteria + inulin Lactobacillus, Streptococcus and Bifidobacterium genus bacteria + FOS Lactobacillus, Bifidobacterium, Enterococcus genus bacteria + FOS Lactobacillus and Bifidobacterium genus bacteria + oligofructose Lactobacillus and Bifidobacterium genus bacteria + inulin |
| References | Subjects | Prebiotic | Time of Administration | Main Outcome |
|---|---|---|---|---|
| Obesity | ||||
| [166] | 48 healthy adults with a body mass index (in kg/m2) >25 | OFS | 12 weeks | There was a reduction in body weight of 1.03 ± 0.43 kg with oligofructose supplementation, whereas the control group experienced an increase in body weight of 0.45 ± 0.31 kg over 12 weeks (p = 0.01). Glucose decreased in the oligofructose group and increased in the control group between the initial and final tests (p ≤ 0.05). Insulin concentrations mirrored this pattern (p ≤ 0.05). Oligofructose supplementation did not affect plasma active glucagon-like peptide 1 secretion. According to a visual analogue scale designed to assess side effects, oligofructose was well tolerated. |
| Insulin resistance syndrome | ||||
| [167] | 10 patients with type 2 diabetes | FOS | 4 weeks (double repetition) | The plasma glucose response to a fixed exogenous insulin bolus did not differ at the end of the two periods. FOS had no effect on glucose and lipid metabolism in type 2 diabetics. |
| Type 2 diabetes | ||||
| [168] | 15 subjects with type 2 diabetes | AX | 5 weeks (double repetition) | A supplement of 15 g/day of AX-rich fibre can significantly improve glycaemic control in people with type 2 diabetes. |
| [169] | 11 patients with impaired glucose tolerance | AX | 6 weeks | No effects of arabinoxylan were observed for insulin, adiponectin, leptin, or resistin as well as for apolipoprotein B, and unesterified fatty acids. In conclusion, the consumption of AX in subjects with impaired glucose tolerance improved fasting serum glucose and triglycerides. However, this beneficial effect was not accompanied by changes in fasting adipokine concentrations. |
| Non-alcoholic fatty liver disease | ||||
| [170] | 7 patients with non-alcoholic steatohepatitis | OFS | 8 weeks | Compared to placebo, OFS significantly decreased serum aminotransferases, aspartate aminotransferase after 8 weeks, and insulin level after 4 weeks, but this could not be related to a significant effect on plasma lipids. |
| Irritable bowel syndrome (IBS), gastrointestinal disorders, elimination of Helicobacter, inflammatory bowel disease (IBD), diarrhoeas | ||||
| [171] | 281 healthy infants (15 to 120 days) | GOS, FOS | 12 months | Fewer episodes of acute diarrhoea, fewer upper respiratory tract infections. |
| [172] | 160 healthy bottle-fed infants within 0–14 days after birth | GOS, FOS | 3 months | Prebiotic formula well tolerated, normal growth trend toward a higher percentage of Bifidobacterium and a lower percentage of E. coli in stool, suppresses Clostridium in stool. |
| [173] | 215 healthy infants | GOS, FOS | 27 weeks | The concentration of secretory IgA was higher in the prebiotic group than the control; also, Bifidobacterium percentage was higher than the control and Clostridium was lower. |
| [174] | 24 patients with chronic pouchitis | inulin | 3 weeks | Inulin treatment resulted in decreased endoscopic and histological inflammation. This effect was associated with increased intestinal butyrate, lowered pH, and significantly decreased numbers of Bacteroides fragilis. |
| [175] | 10 Crohn’s disease patients | FOS | 3 weeks | Reduced disease activity index. |
| Atopic dermatitis | ||||
| [176] | 259 infants at risk for atopy | GOS, FOS | 6 months | Significant reduction of frequency of AD. |
| [177] | 259 healthy term infants with a parental history of atopy | GOS, FOS | 6 months | Prebiotic group had significantly lower allergic symptoms—AD, wheezing, urticaria, and fewer upper respiratory infections than controls during the first 2 years. |
| Alleviation of lactose intolerance | ||||
| [178] | 85 lactose intolerant participants | GOS | 36 days | 71% of subjects reported improvements in at least one symptom (pain, bloating, diarrhoea, cramping, or flatulence). Also on day 36, populations of bifidobacteria significantly increased by 90% in 27 of the 30 non-lactose tolerant participants who took GOS. Lactose fermenting Bifidobacterium, Faecalibacterium, and Lactobacillus were all significantly increased. |
| Different types of cancer and side effects associated with cancer | ||||
| [163] | Human L97 and HT29 cell lines (representing early and late stages of colorectal carcinoma) | inulin | No data | Growth inhibition and induction of apoptosis in human colorectal carcinoma. |
| References | Subjects | Composition of Synbiotic | Time of Administration | Main Outcome |
|---|---|---|---|---|
| Obesity | ||||
| [193] | 153 obese men and women | L. rhamnosus CGMCC1.3724, inulin | 36 weeks | Weight loss and reduction in leptin. Increase in Lachnospiraceae. |
| [194] | 70 children and adolescents with high BMI | L. casei, L. rhamnosus, S. thermophilus, B. breve, L. acidophilus, B. longum, L. bulgaricus, FOS | 8 weeks | Decrease in BMI z-score and waist circumference. |
| [195] | 77 obese children | L. acidophilus, L. rhamnosus, B. bifidum, B. longum, E. faecium, FOS | 4 weeks | Changes in anthropometric measurements. Decrease in TC, LDL-C, and total oxidative stress serum levels. |
| Insulin resistance syndrome | ||||
| [196] | 38 subjects with IRS | L. casei, L. rhamnosus, S. thermophilus, B. breve, L. acidophilus, B. longum, L. bulgaricus, FOS | 28 weeks | The levels of fasting blood sugar and insulin resistance improved significantly. |
| Type 2 diabetes | ||||
| [197] | 54 patients with T2D | L. acidophilus, L. casei, L. rhamnosus, L. bulgaricus, B. breve, B. longum, S. thermophilus, FOS | 8 weeks | Increased HOMA-IR and TGL plasma level; reduced CRP in serum. |
| [198] | 81 patients with T2D | L. sporogenes, inulin | 8 weeks | Significant reduction in serum insulin levels, HOMA-IR, and homeostatic model assessment cell function. |
| [199] | 78 patients with T2D | L. sporogenes, inulin | 8 weeks | Decrease in serum lipid profile (TAG, TC/HDL-C) and a significant increase in serum HDL-C levels. |
| [200] | 20 patients with T2D | L. acidophilus, B. bifidum, oligofructose | 2 weeks | Increased HDL-C and reduced fasting glycaemia. |
| Non-alcoholic fatty liver disease | ||||
| [187] | 20 individuals with NASH | L. plantarum, L. delbrueckii spp. bulgaricus, L. acidophilus, L. rhamnosus, B. bifidum, inulin | 26 weeks | Decreased IHTG content. |
| [188] | 52 adult individuals with NAFLD | L. casei, L. rhamnosus, S. thermophilus, B. breve, L. acidophilus, B. longum, L. bulgaricus, FOS | 30 weeks | Inhibition of NF-κB and reduction of TNF-α. |
| Irritable bowel syndrome (IBS), gastrointestinal disorders, elimination of Helicobacter, inflammatory bowel disease (IBD), diarrhoeas | ||||
| [201] | 76 patients with IBS | L. acidophilus La-5®, B. animalis ssp. lactis BB-12®, dietary fibres (Beneo) | 4 weeks | On average, an 18% improvement in total IBS-QoL score was reported and significant improvements in bloating severity, satisfaction with bowel movements, and the severity of IBS symptoms’ interference with patients’ everyday life were observed. However, there were no statistically significant differences between the synbiotic group and the placebo group. |
| [202] | 69 children aged 6–16 years who had biopsy proven H. pylori infection | B. lactis B94, inulin | 14 days | From a total of 69 H. pylori-infected children (female/male = 36/33; mean ± SD = 11.2 ± 3.0 years), eradication was achieved in 20 out of 34 participants in the standard therapy group and 27/35 participants in the synbiotic group. There were no significant differences in eradication rates between the standard therapy and the synbiotic groups. |
| [203] | 40 patients with UC | B. longum, psyllium | 4 weeks | Patients with UC on synbiotic therapy experienced greater quality-of-life changes than patients on probiotic or prebiotic treatment. |
| Atopic dermatitis | ||||
| [204] | 90 infants with AD | B. breve M-16V, GOS and FOS mixture (Immunofortis®) | 12 weeks | This synbiotic mixture did not have a beneficial effect on AD severity in infants, although it did successfully modulate their intestinal microbiota. |
| [205] | 40 infants and children aged 3 months to 6 years with AD | L. casei, L. rhamnosus, S. thermophilus, B. breve, L. acidophilus, B. infantis, L. bulgaricus, FOS | 8 weeks | A mixture of seven probiotic strains and FOS may clinically improve the severity of AD in young children. |
| Alleviation of lactose intolerance | ||||
| [206] | 20 females and males | Lactobacillus, Bifidobacterium, FOS | 5 weeks | Consumption of the probiotic mixture improved the gastrointestinal performance associated with lactose load in subjects with LI. Symptoms were additionally reduced by the addition of prebiotics. The supplementation was safe and well tolerated, with no significant adverse effect observed. |
| Different types of cancer and side effects associated with cancer | ||||
| [192] | 43 polypeptomized and 37 colon cancer patients | L. rhamnosus GG, B. lactis Bb12, inulin | 12 weeks | Increased L. rhamnosus and B. lactis in faeces, reduction in C. perfringens, prevents increased secretion of IL-2 in polypectomized patients, increased production of interferon-γ in cancer patients. |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markowiak, P.; Śliżewska, K. Effects of Probiotics, Prebiotics, and Synbiotics on Human Health. Nutrients 2017, 9, 1021. https://doi.org/10.3390/nu9091021
Markowiak P, Śliżewska K. Effects of Probiotics, Prebiotics, and Synbiotics on Human Health. Nutrients. 2017; 9(9):1021. https://doi.org/10.3390/nu9091021
Chicago/Turabian StyleMarkowiak, Paulina, and Katarzyna Śliżewska. 2017. "Effects of Probiotics, Prebiotics, and Synbiotics on Human Health" Nutrients 9, no. 9: 1021. https://doi.org/10.3390/nu9091021