
Beyond the Plate: Uncovering Inequalities in Fruit and Vegetable Intake across Indonesian Districts
 , , , and
, , , and
Abstract
:1. Background
2. Methods
2.1. Study Design
2.2. Independent Variables
2.3. Dependent Variables
2.4. Data Analysis
3. Results
3.1. Provincial-Level Results
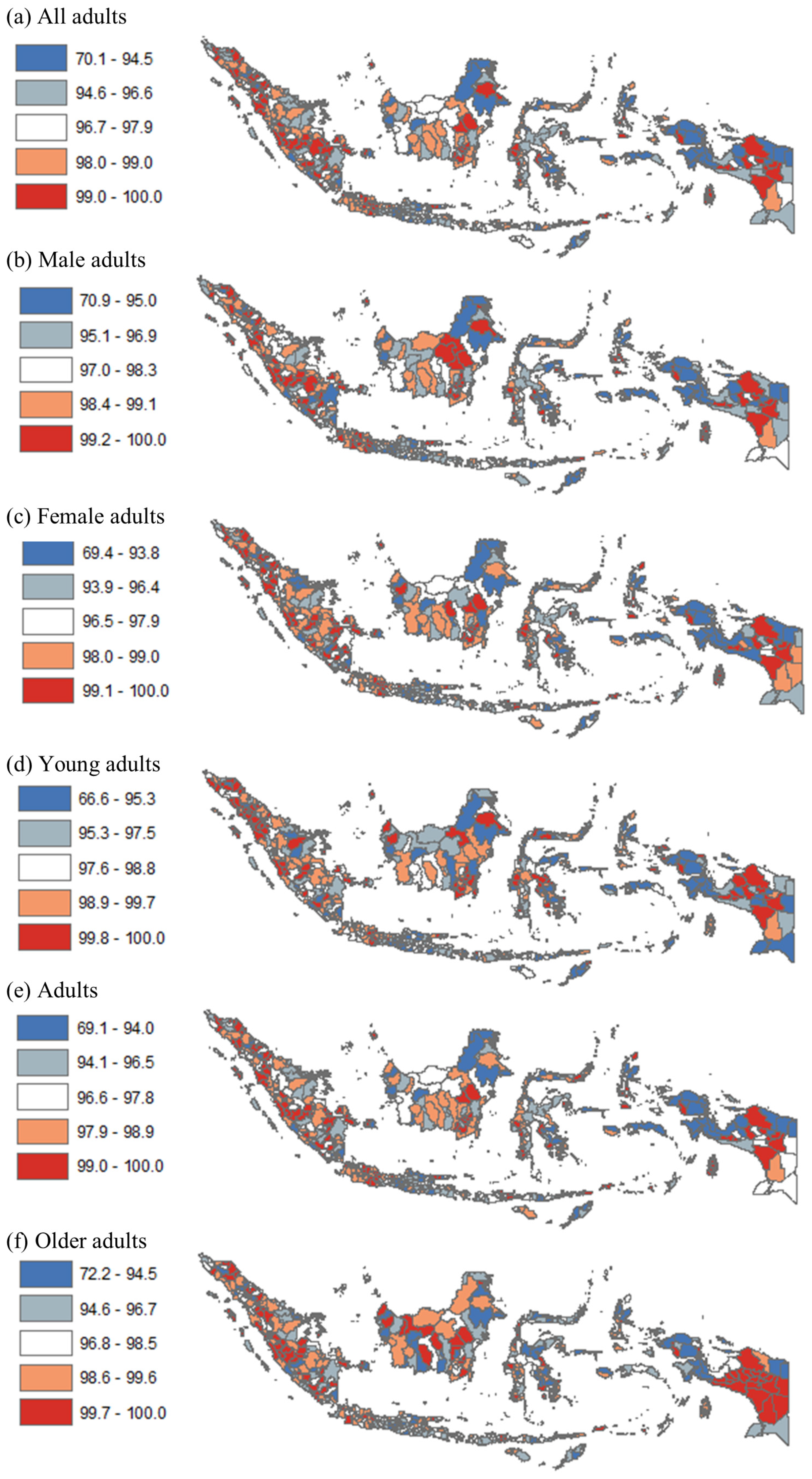
3.2. District-Level Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Noncommunicable Diseases: Childhood Overweight and Obesity. 2020. Available online: https://www.who.int/news-room/questions-and-answers/item/noncommunicable-diseases-childhood-overweight-and-obesity (accessed on 22 February 2023).
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health Research and Development (NIHRD). Report of Riskesdas. 2018. Available online: http://repository.bkpk.kemkes.go.id/3514/1/Laporan%20Riskesdas%202018%20Nasional.pdf (accessed on 15 April 2023).
- Jones, A.D.; Shrinivas, A.; Bezner-Kerr, R. Farm production diversity is associated with greater household dietary diversity in Malawi: Findings from nationally representative data. Food Policy 2014, 46, 1–12. [Google Scholar] [CrossRef]
- Drewnowski, A.; Darmon, N. The economics of obesity: Dietary energy density and energy cost. Am. J. Clin. Nutr. 2005, 82, 265S–273S. [Google Scholar] [CrossRef]
- Gibson, E.L.; Wardle, J.; Watts, C.J. Fruit and Vegetable Consumption, Nutritional Knowledge and Beliefs in Mothers and Children. Appetite 1998, 31, 205–228. [Google Scholar] [CrossRef] [Green Version]
- Bodor, J.N.; Rose, D.; AFarley, T.; Swalm, C.; Scott, S.K. Neighbourhood fruit and vegetable availability and consumption: The role of small food stores in an urban environment. Public Health Nutr. 2008, 11, 413–420. [Google Scholar] [CrossRef] [Green Version]
- Reicks, M.; Trofholz, A.C.; Stang, J.S.; Laska, M.N. Impact of Cooking and Home Food Preparation Interventions Among Adults: Outcomes and Implications forFuture Programs. J. Nutr. Educ. Behav. 2014, 46, 259–276. [Google Scholar] [CrossRef] [Green Version]
- Desbouys, L.; Méjean, C.; De Henauw, S.; Castetbon, K. Socio-economic and cultural disparities in diet among adolescents and young adults: A systematic review. Public Health Nutr. 2020, 23, 843–860. [Google Scholar] [CrossRef] [Green Version]
- Dubowitz, T.; Heron, M.; E Bird, C.; Lurie, N.; Finch, B.K.; Basurto-Dávila, R.; Hale, L.; Escarce, J.J. Neighborhood socioeconomic status and fruit and vegetable intake among whites, blacks, and Mexican Americans in the United States. Am. J. Clin. Nutr. 2008, 87, 1883–1891. [Google Scholar] [CrossRef] [Green Version]
- Menezes, M.C.; Costa, B.V.L.; Oliveira, C.D.L.; Lopes, A.C.S. Local food environment and fruit and vegetable consumption: An ecological study. Prev. Med. Rep. 2017, 5, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Hosseinpoor, A.R.; Bergen, N.; Kunst, A.; Harper, S.; Guthold, R.; Rekve, D.; D’Espaignet, E.T.; Naidoo, N.; Chatterji, S. Socioeconomic inequalities in risk factors for non communicable diseases in low-income and middle-income countries: Results from the World Health Survey. BMC Public Health 2012, 12, 912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giskes, K.; Van Lenthe, F.J.; Kamphuis, C.B.M.; Huisman, M.; Brug, J.; MacKenbach, J.P. Household and food shopping environments: Do they play a role in socioeconomic inequalities in fruit and vegetable consumption? A multilevel study among Dutch adults. J. Epidemiol. Community Health 2009, 63, 113–120. [Google Scholar] [CrossRef]
- de Azevedo Barros, M.B.; Lima, M.G.; Medina LD, P.B.; Szwarcwald, C.L.; Malta, D.C. Social inequalities in health behaviors among Brazilian adults: National Health Survey, 2013. Int. J. Equity Health 2016, 15, 148. [Google Scholar] [CrossRef] [Green Version]
- Amo-Adjei, J.; Kumi-Kyereme, A. Fruit and Vegetable Consumption by Ecological Zone and Socioeconomic Status in Ghana. J. Biosoc. Sci. 2015, 47, 613–631. [Google Scholar] [CrossRef] [PubMed]
- Ayuningtyas, D.; Hapsari, D.; Rachmalina, R.; Amir, V.; Rachmawati, R.; Kusuma, D. Geographic and Socioeconomic Disparity in Child Undernutrition across 514 Districts in Indonesia. Nutrients 2022, 14, 843. [Google Scholar] [CrossRef] [PubMed]
- Ayuningtyas, D.; Kusuma, D.; Amir, V.; Tjandrarini, D.H.; Andarwati, P. Disparities in Obesity Rates among Adults: Analysis of 514 Districts in Indonesia. Nutrients 2022, 14, 3332. [Google Scholar] [CrossRef]
- Bella, A.; Akbar, M.T.; Kusnadi, G.; Herlinda, O.; Regita, P.A.; Kusuma, D. Socioeconomic and Behavioral Correlates of COVID-19 Infections among Hospital Workers in the Greater Jakarta Area, Indonesia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5048. [Google Scholar] [CrossRef]
- Indonesian Statistics Bureau (BPS). [Poverty and Inequality Concept]. 2020. Available online: https://www.bps.go.id/subject/23/kemiskinan-dan-ketimpangan.html (accessed on 1 April 2023).
- Megatsari, H.; Kusuma, D.; Ernawaty, E.; Putri, N.K. Geographic and Socioeconomic Inequalities in Delays in COVID-19 Vaccinations: A Cross-Sectional Study in Indonesia. Vaccines 2022, 10, 1857. [Google Scholar] [CrossRef]
- Oktamianti, P.; Kusuma, D.; Amir, V.; Tjandrarini, D.H.; Paramita, A. District-Level Inequalities in Hypertension among Adults in Indonesia: A Cross-Sectional Analysis by Sex and Age Group. Int. J. Environ. Res. Public Health 2022, 19, 13268. [Google Scholar] [CrossRef]
- Song, P.; Gupta, A.; Goon, I.Y.; Hasan, M.; Mahmood, S.; Page, P.; Pradeepa, R.; Siddiqui, S.; Silva, W.; Aarthi, G.R.; et al. Data Resource Profile: Understanding the patterns and determinants of health in South Asians-South Asia Biobank. Int. J. Epidemiol. 2021, 50, 717–718e. [Google Scholar] [CrossRef]
- Kusuma, D.; Pradeepa, R.; Khawaja, K.I.; Hasan, M.; Siddiqui, S.; Mahmood, S.; Shah, S.M.A.; De Silva, C.K.; de Silva, L.; Gamage, M.; et al. Low uptake of COVID-19 prevention behaviours and high socioeconomic impact of lockdown measures in South Asia: Evidence from a large-scale multi-country surveillance programme. SSM—Popul. Health 2021, 13, 100751. [Google Scholar] [CrossRef] [PubMed]
- Di Cesare, M.; Khang, Y.-H.; Asaria, P.; Blakely, T.; Cowan, M.J.; Farzadfar, F.; Guerrero, R.; Ikeda, N.; Kyobutungi, C.; Msyamboza, K.P.; et al. Inequalities in non-communicable diseases and effective responses. Lancet 2013, 381, 585–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mwenda, V.; Mwangi, M.; Nyanjau, L.; Gichu, M.; Kyobutungi, C.; Kibachio, J. Dietary risk factors for non-communicable diseases in Kenya: Findings of the STEPS survey, 2015. BMC Public Health 2018, 18, 1218. [Google Scholar] [CrossRef] [Green Version]
- Gelibo, T.; Amenu, K.; Taddele, T.; Taye, G.; Getnet, M.; Getachew, T.; Defar, A.; Teklie, H.; Bekele, A.; Shiferaw, F.; et al. Low fruit and vegetable intake and its associated factors in Ethiopia: A community based cross sectional NCD steps survey. Ethiop. J. Health Dev. 2018, 31, 355–361. [Google Scholar]
- Rafique, I.; Saqib, M.A.; Munir, M.A.; Qureshi, H.; Rizwanullah, K.S.; Khan, S.A.; Fouad, H. Prevalence of risk factors for noncommunicable diseases in adults: Key findings from the Pakistan steps survey. East. Mediterr. Health J. 2018, 24, 33–41. [Google Scholar] [CrossRef]
- Tripathy, J.P.; Thakur, J.S.; Jeet, G.; Chawla, S.; Jain, S.; Prasad, R. Urban rural differences in diet, physical activity and obesity in India: Are we witnessing the great Indian equalisation? Results from a cross-sectional STEPS survey. BMC Public Health 2016, 16, 816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aryal, K.K.; Mehata, S.; Neupane, S.; Vaidya, A.; Dhimal, M.; Dhakal, P.; Rana, S.; Bhusal, C.L.; Lohani, G.R.; Paulin, F.H.; et al. The Burden and Determinants of Non Communicable Diseases Risk Factors in Nepal: Findings from a Nationwide STEPS Survey. PLoS ONE 2015, 10, e0134834. [Google Scholar] [CrossRef]
- Widener, M.J.; Metcalf, S.S.; Bar-Yam, Y. Dynamic Urban food environments: A temporal analysis of access to healthy foods. Am. J. Prev. Med. 2011, 41, 439–441. [Google Scholar] [CrossRef]
- Hawkes, C.; Smith, T.G.; Jewell, J.; Wardle, J.; Hammond, R.A.; Friel, S.; Thow, A.M.; Kain, J. Smart food policies for obesity prevention. Lancet 2015, 385, 2410–2421. [Google Scholar] [CrossRef]
- Miller, V.; Yusuf, S.; Chow, C.K.; Dehghan, M.; Corsi, D.J.; Lock, K.; Popkin, B.; Rangarajan, S.; Khatib, R.; A Lear, S.; et al. Availability, affordability, and consumption of fruits and vegetables in 18 countries across income levels: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet Glob. Health 2016, 4, e695–e703. [Google Scholar] [CrossRef] [Green Version]
- Adisasmito, W.; Amir, V.; Atin, A.; Megraini, A.; Kusuma, D. Geographic and socioeconomic disparity in cardiovascular risk factors in Indonesia: Analysis of the Basic Health Research 2018. BMC Public Health 2020, 20, 1004. [Google Scholar] [CrossRef] [PubMed]
- FAO. Nutrition and Food Systems. A Report by the High Level Panel of Experts on Food Security and Nutrition of the Committee on World Food Security. September 2017. Available online: https://www.fao.org/documents/card/en/c/I7846E (accessed on 8 April 2023).
- Story, M.; Kaphingst, K.M.; Robinson-O'Brien, R.; Glanz, K. Creating Healthy Food and Eating Environments: Policy and Environmental Approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drobniewski, F.; Kusuma, D.; Broda, A.; Castro-Sánchez, E.; Ahmad, R. COVID-19 Vaccine Hesitancy in Diverse Groups in the UK—Is the Driver Economic or Cultural in Student Populations. Vaccines 2022, 10, 501. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Low FV Intake Prevalence (%) | |||||||
|---|---|---|---|---|---|---|---|
| Poverty Rates (%) | All | Males | Females | Young Adults | Adults | Older Adults | |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | |
| Bali | 4.5 | 94.8 | 95.0 | 94.5 | 95.6 | 94.4 | 95.6 |
| South Kalimantan | 4.8 | 98.8 | 99.1 | 98.5 | 99.7 | 98.6 | 98.6 |
| Central Kalimantan | 5.0 | 97.5 | 97.9 | 97.1 | 98.2 | 97.4 | 97.0 |
| Jakarta | 5.0 | 95.9 | 96.6 | 95.3 | 97.7 | 96.1 | 92.6 |
| Banten | 5.3 | 97.7 | 98.3 | 97.1 | 98.3 | 97.5 | 97.8 |
| Bangka Belitung | 5.4 | 98.1 | 98.4 | 97.7 | 98.9 | 97.9 | 97.7 |
| West Sumatera | 6.6 | 98.0 | 98.3 | 97.7 | 98.5 | 97.8 | 98.1 |
| North Kalimantan | 7.0 | 94.6 | 95.4 | 93.7 | 96.4 | 94.0 | 95.7 |
| East Kalimantan | 7.1 | 96.2 | 96.3 | 96.0 | 97.2 | 96.0 | 95.6 |
| Riau Islands | 7.6 | 94.7 | 95.3 | 94.1 | 96.9 | 94.2 | 95.9 |
| Jambi | 7.8 | 98.1 | 98.2 | 98.0 | 98.6 | 97.9 | 98.6 |
| North Maluku | 7.9 | 94.5 | 94.7 | 94.3 | 96.2 | 93.9 | 96.1 |
| West Java | 7.9 | 98.6 | 98.8 | 98.3 | 99.1 | 98.4 | 98.6 |
| West Kalimantan | 8.1 | 94.7 | 95.0 | 94.4 | 95.4 | 94.4 | 95.6 |
| North Sulawesi | 8.5 | 97.3 | 97.7 | 96.9 | 98.0 | 97.3 | 96.8 |
| Riau | 8.8 | 97.0 | 97.5 | 96.4 | 97.7 | 96.8 | 97.0 |
| South Sulawesi | 9.8 | 97.9 | 97.9 | 97.9 | 97.9 | 97.9 | 98.0 |
| West Sulawesi | 10.3 | 95.0 | 95.4 | 94.6 | 96.0 | 94.6 | 95.7 |
| East Java | 10.9 | 96.0 | 96.4 | 95.7 | 96.8 | 95.8 | 96.2 |
| Central Java | 10.9 | 96.9 | 97.2 | 96.5 | 98.1 | 96.6 | 96.6 |
| North Sumatera | 11.3 | 95.5 | 95.9 | 95.0 | 96.4 | 95.2 | 95.6 |
| Lampung | 12.6 | 92.6 | 93.2 | 92.0 | 95.5 | 91.7 | 93.4 |
| Yogyakarta | 12.7 | 94.4 | 94.4 | 94.5 | 96.0 | 93.9 | 95.1 |
| Southeast Sulawesi | 13.0 | 96.9 | 97.3 | 96.6 | 97.1 | 96.8 | 97.6 |
| South Sumatera | 13.1 | 98.0 | 98.0 | 97.9 | 98.5 | 97.9 | 97.8 |
| Central Sulawesi | 14.6 | 95.7 | 96.1 | 95.3 | 96.3 | 95.4 | 96.4 |
| West Nusa Tenggara | 14.8 | 96.7 | 97.7 | 95.9 | 96.8 | 96.7 | 96.8 |
| Bengkulu | 15.0 | 96.1 | 96.2 | 95.9 | 96.7 | 95.9 | 96.5 |
| Aceh | 16.4 | 98.1 | 98.1 | 98.0 | 98.7 | 97.8 | 98.6 |
| Gorontalo | 16.8 | 95.7 | 95.9 | 95.6 | 97.0 | 95.3 | 96.1 |
| Maluku | 21.8 | 94.2 | 94.2 | 94.1 | 94.8 | 93.8 | 95.4 |
| East Nusa Tenggara | 22.0 | 94.9 | 95.4 | 94.3 | 95.9 | 94.6 | 94.9 |
| West Papua | 26.5 | 93.1 | 93.2 | 92.9 | 93.6 | 92.8 | 94.4 |
| Papua | 29.4 | 96.3 | 96.5 | 96.0 | 96.2 | 96.3 | 96.3 |
| Average | 96.2 | 96.5 | 95.8 | 97.1 | 95.9 | 96.4 | |
| All | Urban | Rural | Difference | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | % | p-Value | |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) = (4–6) | ||
| (a) Characteristics (#) | ||||||||
| Sample size district | 514 | 100% | 97 | 100% | 417 | 100% | 0% | |
| Region | ||||||||
| Papua | 95 | 18.5% | 9 | 9.3% | 86 | 20.6% | 11.3% | 0.008 |
| Java | 128 | 24.9% | 35 | 36.1% | 93 | 22.3% | −13.8% | |
| Sumatera | 154 | 30.0% | 33 | 34.0% | 121 | 29.0% | −5.0% | |
| Kalimantan | 56 | 10.9% | 9 | 9.3% | 47 | 11.3% | 2.0% | |
| Sulawesi | 81 | 15.8% | 11 | 11.3% | 70 | 16.8% | 5.4% | |
| 514 | 97 | 417 | ||||||
| Income | ||||||||
| Q1 poor | 102 | 19.8% | 3 | 3.1% | 99 | 23.7% | 20.6% | <0.001 |
| Q2 | 103 | 20.0% | 5 | 5.2% | 98 | 23.5% | 18.3% | |
| Q3 | 103 | 20.0% | 13 | 13.4% | 90 | 21.6% | 8.2% | |
| Q4 | 103 | 20.0% | 22 | 22.7% | 81 | 19.4% | −3.3% | |
| Q5 rich | 103 | 20.0% | 54 | 55.7% | 49 | 11.8% | −43.9% | |
| 514 | 97 | 417 | ||||||
| Education | ||||||||
| Q1 least | 103 | 20.0% | 0 | 0.0% | 103 | 24.7% | 24.7% | <0.001 |
| Q2 | 103 | 20.0% | 11 | 11.3% | 92 | 22.1% | 10.7% | |
| Q3 | 103 | 20.0% | 17 | 17.5% | 86 | 20.6% | 3.1% | |
| Q4 | 103 | 20.0% | 29 | 29.9% | 74 | 17.7% | −12.2% | |
| Q5 most | 102 | 19.8% | 40 | 41.2% | 62 | 14.9% | −26.4% | |
| 514 | 97 | 417 | ||||||
| (b) Inadequate FV intake (%) | ||||||||
| All adults | n/a | 96.3% | n/a | 95.8% | n/a | 96.5% | −0.7% | 0.093 |
| Male adults | n/a | 96.7% | n/a | 96.4% | n/a | 96.7% | −0.3% | 0.375 |
| Female adults | n/a | 96.0% | n/a | 95.2% | n/a | 96.2% | −1.0% | 0.020 |
| Young adults | n/a | 97.0% | n/a | 97.4% | n/a | 97.0% | 0.4% | 0.309 |
| Adults | n/a | 96.1% | n/a | 95.4% | n/a | 96.3% | −0.9% | 0.050 |
| Older adults | n/a | 96.7% | n/a | 95.2% | n/a | 97.0% | −1.8% | <0.001 |
| Inadequate FV Intake (N = 514 Districts) | ||||||
|---|---|---|---|---|---|---|
| All Adults | Males | Females | Young Adults | Adults | Older Adults | |
| Region | ||||||
| Papua | 94.9% | 95.1% | 94.6% | 95.2% | 94.6% | 95.9% |
| Sulawesi | 96.5% | 96.8% | 96.3% | 97.0% | 96.3% | 96.9% |
| Kalimantan | 96.8% | 97.2% | 96.4% | 97.6% | 96.6% | 97.1% |
| Sumatera | 97.2% | 97.5% | 97.0% | 98.0% | 97.1% | 97.2% |
| Java | 96.1% | 96.5% | 95.6% | 97.0% | 95.8% | 96.2% |
| Absolute | 1.2% | 1.4% | 1.0% | 1.8% | 1.2% | 0.3% |
| Relative | 1.01 | 1.01 | 1.01 | 1.02 | 1.01 | 1.00 |
| Income | ||||||
| Q1 poor | 95.7% | 95.8% | 95.6% | 95.9% | 95.6% | 96.5% |
| Q2 | 95.9% | 96.3% | 95.5% | 96.6% | 95.6% | 96.6% |
| Q3 | 96.7% | 97.1% | 96.4% | 97.5% | 96.5% | 96.8% |
| Q4 | 96.9% | 97.2% | 96.5% | 97.6% | 96.7% | 97.0% |
| Q5 rich | 96.5% | 96.9% | 96.2% | 97.6% | 96.3% | 96.4% |
| Absolute | 0.8% | 1.1% | 0.6% | 1.7% | 0.7% | −0.1% |
| Relative | 1.01 | 1.01 | 1.01 | 1.02 | 1.01 | 1.00 |
| Education | ||||||
| Q1 least | 96.6% | 96.8% | 96.5% | 96.8% | 96.5% | 97.2% |
| Q2 | 96.5% | 96.8% | 96.1% | 97.1% | 96.2% | 97.0% |
| Q3 | 96.0% | 96.3% | 95.7% | 96.7% | 95.8% | 96.2% |
| Q4 | 96.2% | 96.5% | 95.9% | 97.0% | 96.0% | 96.5% |
| Q5 most | 96.4% | 96.8% | 96.0% | 97.6% | 96.1% | 96.4% |
| Absolute | −0.2% | 0.0% | −0.5% | 0.8% | −0.4% | −0.8% |
| Relative | 1.00 | 1.00 | 0.99 | 1.01 | 1.00 | 0.99 |
| Inadequate FV intake (N = 514 districts) | ||||||
|---|---|---|---|---|---|---|
| All Adults | Males | Females | Young Adults | Adults | Older Adults | |
| Coef (p-Value) | Coef (p-Value) | Coef (p-Value) | Coef (p-Value) | Coef (p-Value) | Coef (p-Value) | |
| Region | ||||||
| Papua | Reference | |||||
| Java | 1.176 * | 1.130 * | 1.228 * | 1.274 * | 1.194 * | 0.583 |
| (0.042) | (0.047) | (0.047) | (0.037) | (0.047) | (0.343) | |
| Sumatera | 2.587 ** | 2.332 ** | 2.828 ** | 2.524 ** | 2.715 ** | 1.776 ** |
| (0.000) | (0.000) | (0.000) | (0.000) | (0.000) | (0.003) | |
| Kalimantan | 1.691 * | 1.617 * | 1.714 * | 1.633 * | 1.740 * | 1.365 |
| (0.020) | (0.023) | (0.027) | (0.032) | (0.021) | (0.077) | |
| Sulawesi | 1.859 ** | 1.647 ** | 2.075 ** | 1.618 * | 1.956 ** | 1.262 |
| (0.002) | (0.006) | (0.001) | (0.011) | (0.002) | (0.051) | |
| Income | ||||||
| Quintile 1 poor | Reference | |||||
| Quintile 2 | −0.359 | −0.040 | −0.683 | 0.013 | −0.491 | −0.135 |
| (0.521) | (0.942) | (0.254) | (0.983) | (0.401) | (0.822) | |
| Quintile 3 | 0.374 | 0.653 | 0.089 | 0.791 | 0.297 | 0.055 |
| (0.523) | (0.258) | (0.887) | (0.200) | (0.626) | (0.930) | |
| Quintile 4 | 0.389 | 0.710 | 0.058 | 0.808 | 0.321 | 0.094 |
| (0.507) | (0.218) | (0.926) | (0.191) | (0.598) | (0.881) | |
| Quintile 5 rich | 0.341 | 0.601 | 0.076 | 1.014 | 0.242 | −0.301 |
| (0.585) | (0.328) | (0.909) | (0.123) | (0.710) | (0.651) | |
| Education | ||||||
| Quintile 1 least | Reference | |||||
| Quintile 2 | −0.628 | −0.482 | −0.790 | −0.323 | −0.750 | −0.451 |
| (0.235) | (0.356) | (0.162) | (0.562) | (0.174) | (0.424) | |
| Quintile 3 | −1.171 * | −1.030 * | −1.319 * | −0.763 | −1.285 * | −1.336 * |
| (0.027) | (0.048) | (0.019) | (0.170) | (0.020) | (0.018) | |
| Quintile 4 | −1.059 * | −0.925 | −1.195 * | −0.581 | −1.197 * | −1.007 |
| (0.045) | (0.076) | (0.035) | (0.297) | (0.030) | (0.074) | |
| Quintile 5 most | −1.066 | −0.855 | −1.284 * | −0.262 | −1.280 * | −1.246 * |
| (0.057) | (0.122) | (0.032) | (0.657) | (0.029) | (0.038) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Darmawan, E.S.; Kusuma, D.; Permanasari, V.Y.; Amir, V.; Tjandrarini, D.H.; Dharmayanti, I. Beyond the Plate: Uncovering Inequalities in Fruit and Vegetable Intake across Indonesian Districts. Nutrients 2023, 15, 2160. https://doi.org/10.3390/nu15092160
Darmawan ES, Kusuma D, Permanasari VY, Amir V, Tjandrarini DH, Dharmayanti I. Beyond the Plate: Uncovering Inequalities in Fruit and Vegetable Intake across Indonesian Districts. Nutrients. 2023; 15(9):2160. https://doi.org/10.3390/nu15092160
Chicago/Turabian StyleDarmawan, Ede Surya, Dian Kusuma, Vetty Yulianty Permanasari, Vilda Amir, Dwi Hapsari Tjandrarini, and Ika Dharmayanti. 2023. "Beyond the Plate: Uncovering Inequalities in Fruit and Vegetable Intake across Indonesian Districts" Nutrients 15, no. 9: 2160. https://doi.org/10.3390/nu15092160