
The Effects of Creatine Supplementation Combined with Resistance Training on Regional Measures of Muscle Hypertrophy: A Systematic Review with Meta-Analysis
 , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Methods
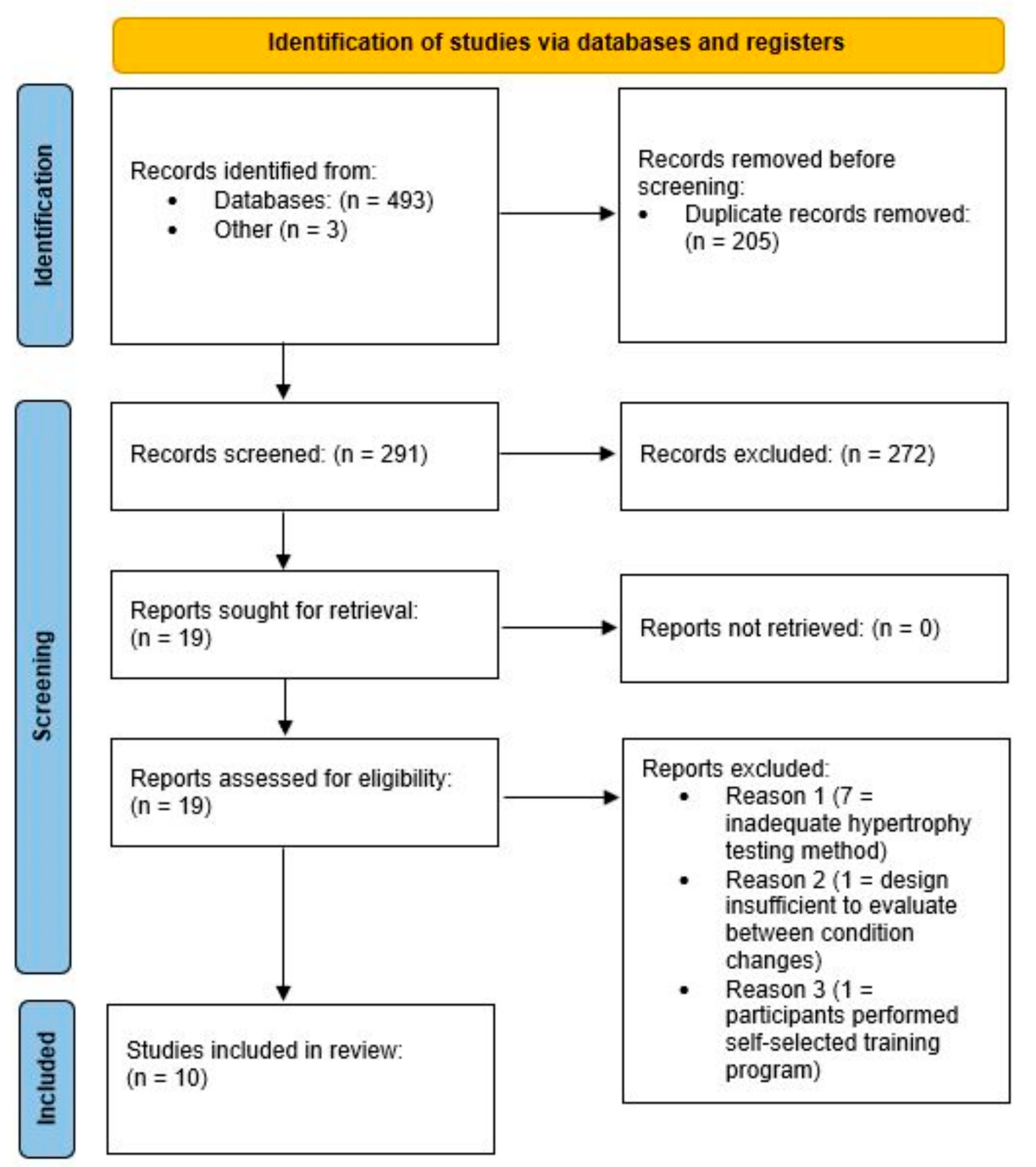
2.1. Literature Search
2.2. Inclusion/Exclusion Criteria
2.3. Data Coding and Analysis
2.4. Methodological Quality
2.5. Statistics
3. Results
3.1. Descriptive Data
3.2. Univariate Analysis of Standardized Differences
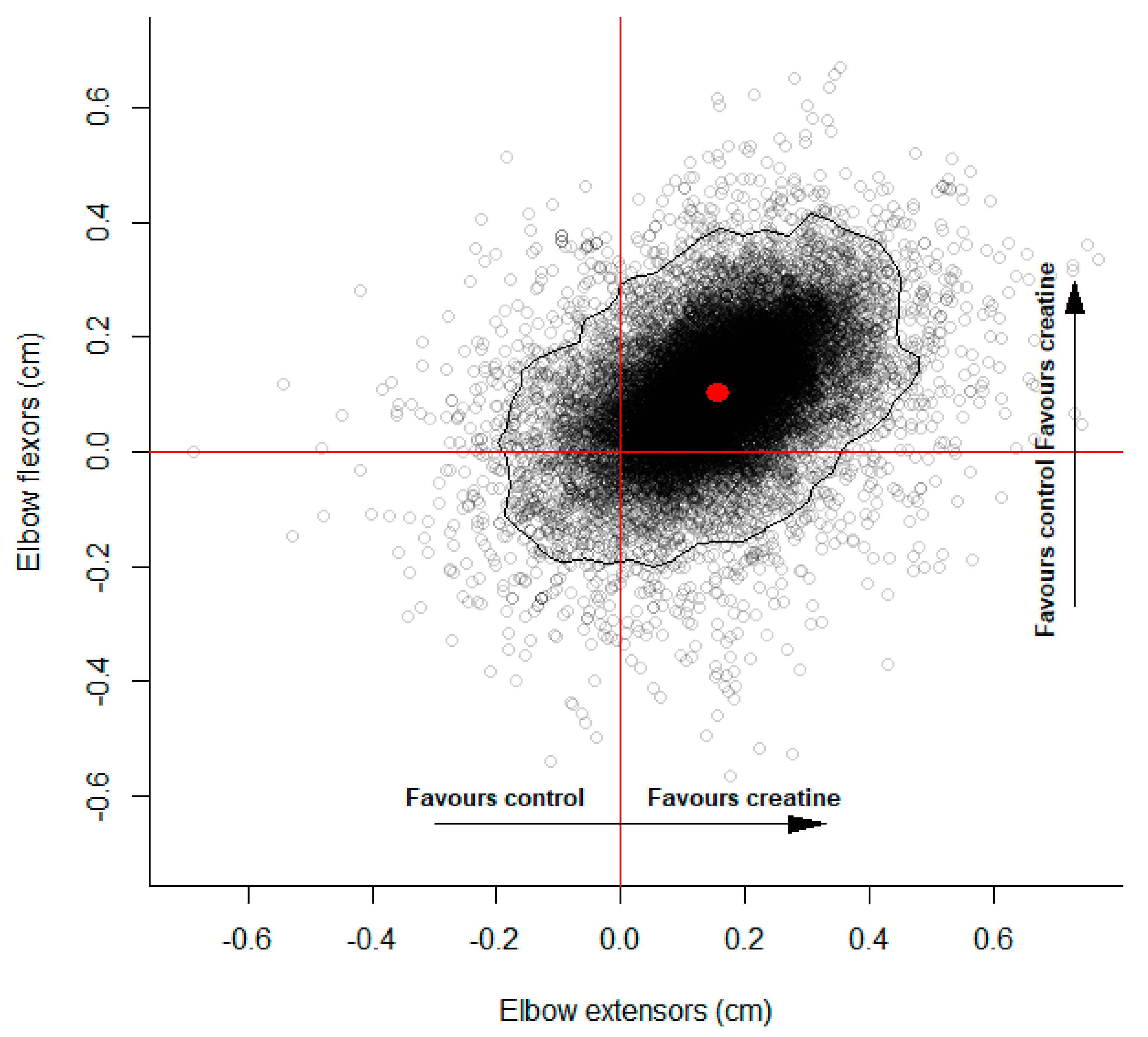
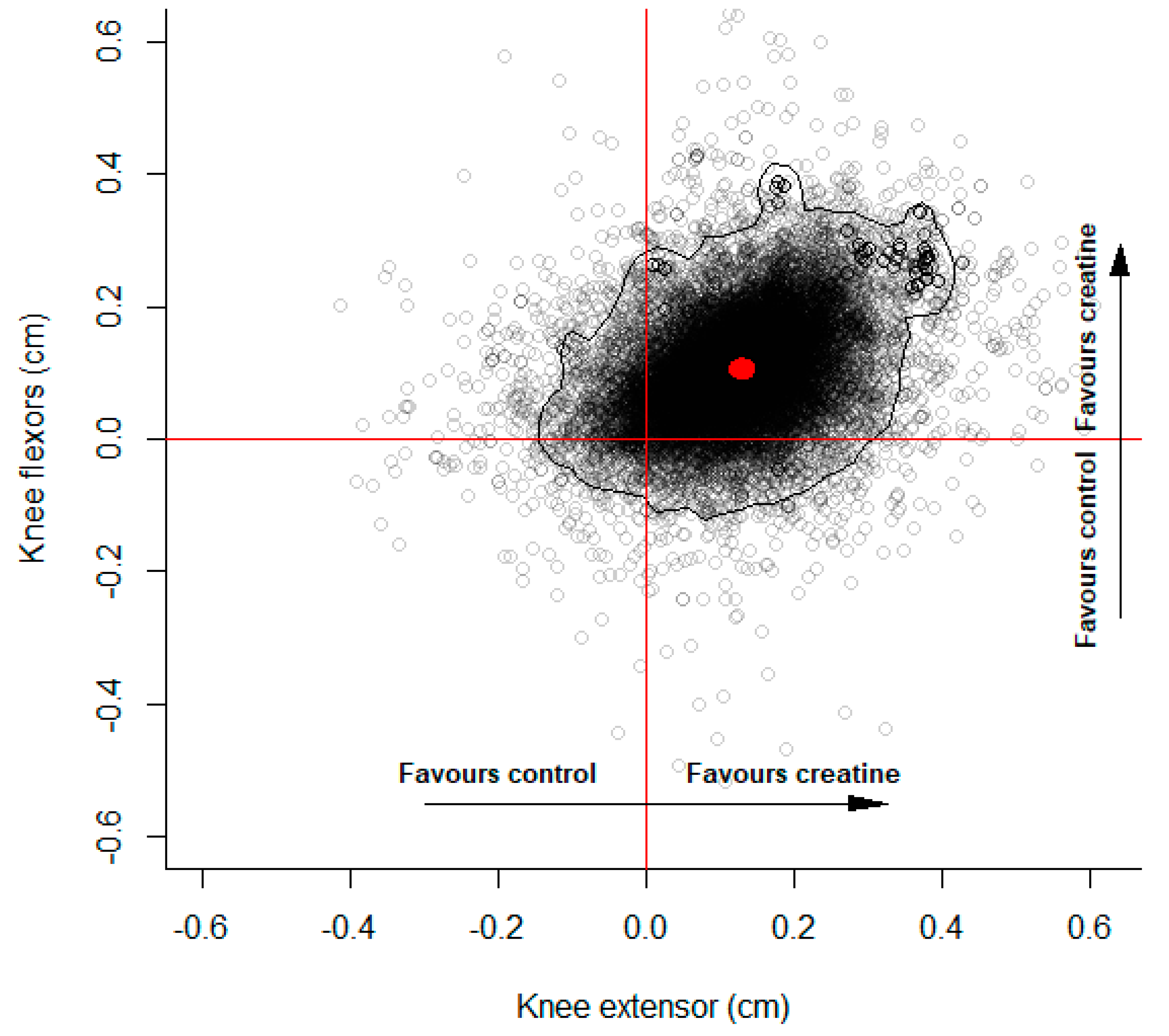
3.3. Multivariate Analysis of Absolute Differences
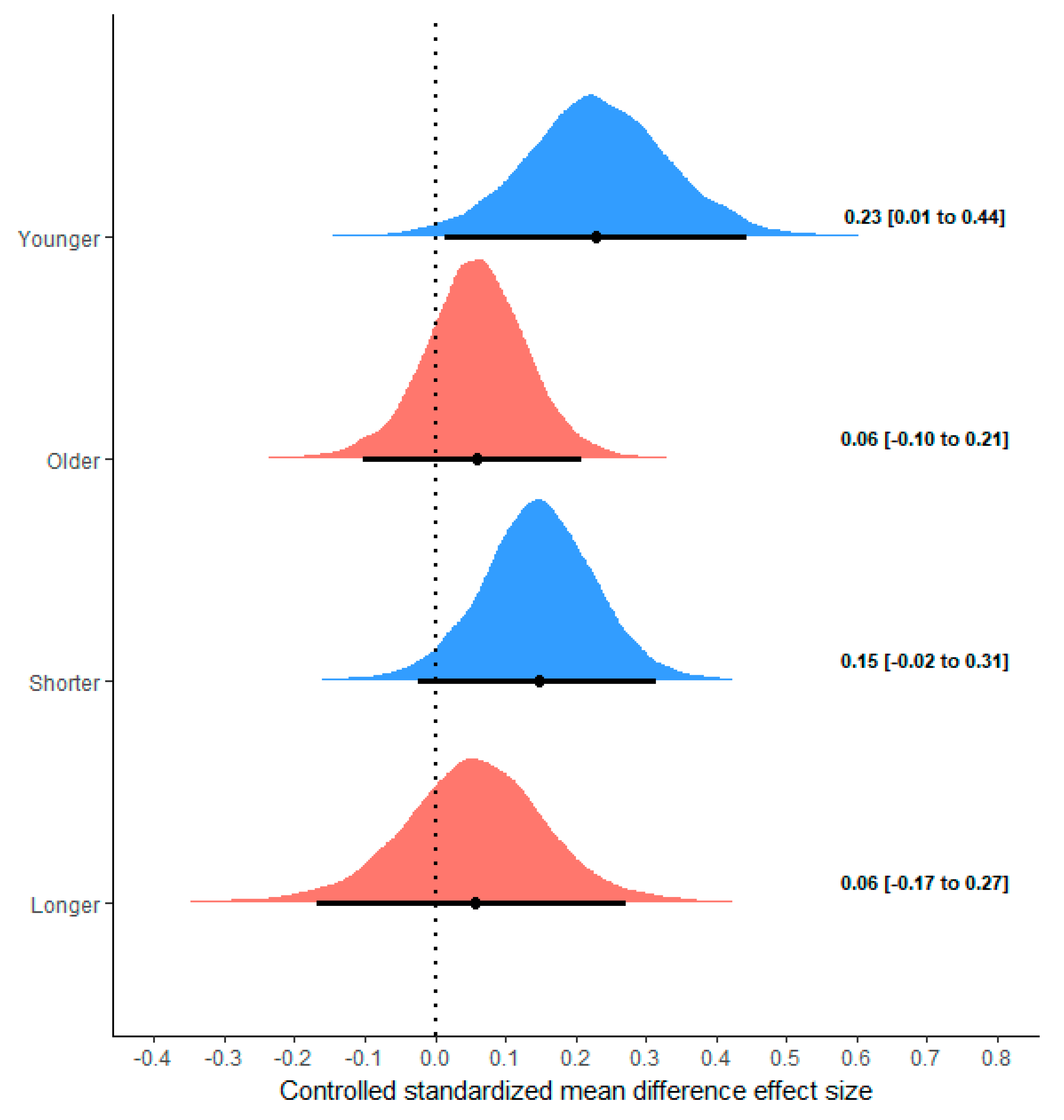
3.4. Analysis of Moderating Effects
3.5. Study Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kreider, R.B.; Kalman, D.S.; Antonio, J.; Ziegenfuss, T.N.; Wildman, R.; Collins, R.; Candow, D.G.; Kleiner, S.M.; Almada, A.L.; Lopez, H.L. International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. J. Int. Soc. Sports Nutr. 2017, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Chilibeck, P.D.; Kaviani, M.; Candow, D.G.; AZello, G. Effect of creatine supplementation during resistance training on lean tissue mass and muscular strength in older adults: A meta-analysis. Open Access J. Sports Med. 2017, 8, 213–226. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B. Science and Development of Muscle Hypertrophy, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2020. [Google Scholar] [CrossRef]
- Lanhers, C.; Pereira, B.; Naughton, G.; Trousselard, M.; Lesage, F.-X.; Dutheil, F. Creatine Supplementation and Lower Limb Strength Performance: A Systematic Review and Meta-Analyses. Sports Med. 2015, 45, 1285–1294. [Google Scholar] [CrossRef] [PubMed]
- Lanhers, C.; Pereira, B.; Naughton, G.; Trousselard, M.; Lesage, F.-X.; Dutheil, F. Creatine Supplementation and Upper Limb Strength Performance: A Systematic Review and Meta-Analysis. Sports Med. 2017, 47, 163–173. [Google Scholar] [CrossRef]
- Glaister, M.; Rhodes, L. Short-Term Creatine Supplementation and Repeated Sprint Ability—A Systematic Review and Meta-Analysis. Int. J. Sports Nutr. Exerc. Metab. 2022, 32, 491–500. [Google Scholar] [CrossRef]
- Mielgo-Ayuso, J.; Calleja-Gonzalez, J.; Marqués-Jiménez, D.; Caballero-García, A.; Córdova, A.; Fernández-Lázaro, D. Effects of Creatine Supplementation on Athletic Performance in Soccer Players: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 757. [Google Scholar] [CrossRef]
- Resistance Training for Health and Fitness. American College of Sports Medicine. 2013. Available online: https://www.acsm.org/docs/brochures/resistance-training.pdf (accessed on 7 April 2023).
- Delpino, F.M.; Figueiredo, L.M.; Forbes, S.C.; Candow, D.G.; Santos, H.O. Influence of age, sex, and type of exercise on the efficacy of creatine supplementation on lean body mass: A systematic review and meta-analysis of randomized clinical trials. Nutrition 2022, 103–104, 111791. [Google Scholar] [CrossRef]
- Forbes, S.C.; Candow, D.G.; Ostojic, S.M.; Roberts, M.D.; Chilibeck, P.D. Meta-Analysis Examining the Importance of Creatine Ingestion Strategies on Lean Tissue Mass and Strength in Older Adults. Nutrients 2021, 13, 1912. [Google Scholar] [CrossRef]
- Devries, M.C.; Phillips, S.M. Creatine Supplementation during Resistance Training in Older Adults—A Meta-analysis. Med. Sci. Sports Exerc. 2014, 46, 1194–1203. [Google Scholar] [CrossRef]
- Guglielmi, G.; Ponti, F.; Agostini, M.; Amadori, M.; Battista, G.; Bazzocchi, A. The role of DXA in sarcopenia. Aging Clin. Exp. Res. 2016, 28, 1047–1060. [Google Scholar] [CrossRef]
- Tavoian, D.; Ampomah, K.; Amano, S.; Law, T.D.; Clark, B.C. Changes in DXA-derived lean mass and MRI-derived cross-sectional area of the thigh are modestly associated. Sci. Rep. 2019, 9, 10028. [Google Scholar] [CrossRef] [PubMed]
- Delmonico, M.J.; Kostek, M.C.; Johns, J.; Hurley, B.F.; Conway, J.M. Can dual energy X-ray absorptiometry provide a valid assessment of changes in thigh muscle mass with strength training in older adults? Eur. J. Clin. Nutr. 2008, 62, 1372–1378. [Google Scholar] [CrossRef]
- Reeves, N.D.; Maganaris, C.N.; Narici, M.V. Ultrasonographic assessment of human skeletal muscle size. Eur. J. Appl. Physiol. 2004, 91, 116–118. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.J.; Candow, D.G.; Roe, A.J.; Fehrenkamp, B.D.; Wilk, V.C.; Bailey, J.P.; Krumpl, L.; Brown, A.F. Creatine monohydrate supplementation changes total body water and DXA lean mass estimates in female collegiate dancers. J. Int. Soc. Sports Nutr. 2023, 20, 2193556. [Google Scholar] [CrossRef] [PubMed]
- Safdar, A.; Yardley, N.J.; Snow, R.; Melov, S.; Tarnopolsky, M.A. Global and targeted gene expression and protein content in skeletal muscle of young men following short-term creatine monohydrate supplementation. Physiol. Genom. 2008, 32, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Trojian, T.H. Creatine supplementation. Curr. Sports Med. Rep. 2013, 12, 240–244. [Google Scholar] [CrossRef]
- Bone, J.L.; Ross, M.L.; Tomcik, K.A.; Jeacocke, N.A.; Hopkins, W.G.; Burke, L.M. Manipulation of Muscle Creatine and Glycogen Changes Dual X-ray Absorptiometry Estimates of Body Composition. Med. Sci. Sports Exerc. 2017, 49, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and me-ta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Cooper, H.; Hedges, L.; Valentine, J. The Handbook of Research Synthesis and Meta-Analysis, 2nd ed; Russell Sage Foundation: New York, NY, USA, 2009. [Google Scholar]
- Coleman, M.; Harrison, K.; Arias, R.; Johnson, E.; Grgic, J.; Orazem, J.; Schoenfeld, B. Muscular adaptations in drop set vs. traditional training: A meta-analysis. Int. J. Strength Cond. 2022, 2. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Grgic, J.; Schoenfeld, B.J.; Davies, T.B.; Lazinica, B.; Krieger, J.W.; Pedisic, Z. Effect of Resistance Training Frequency on Gains in Muscular Strength: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Schoenfeld, B.J.; Skrepnik, M.; Davies, T.B.; Mikulic, P. Effects of Rest Interval Duration in Resistance Training on Measures of Muscular Strength: A Systematic Review. Sports Med. 2018, 48, 137–151. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Garofolini, A.; Orazem, J.; Sabol, F.; Schoenfeld, B.J.; Pedisic, Z. Effects of Resistance Training on Muscle Size and Strength in Very Elderly Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sports Med. 2020, 50, 1983–1999. [Google Scholar] [CrossRef] [PubMed]
- Kruschke, J.; Liddell, T. The Bayesian New Statistics: Hypothesis testing, estimation, meta-analysis, and power analysis from a Bayesian perspective. Psychon. Bull. Rev. 2018, 25, 178–206. [Google Scholar] [CrossRef]
- Morris, B. Estimating effect sizes from pretest-posttest-control group designs. Organ. Res. Methods 2008, 11, 364–386. [Google Scholar] [CrossRef]
- Swinton, P.; Murphy, A. Comparative effect size distributions in strength and conditioning and implications for future research. SportRxiv 2022, arXiv:10.51224/srxiv.202. [Google Scholar]
- Fu, R.; Gartlehner, G.; Grant, M.; Shamliyan, T.; Sedrakyan, A.; Wilt, T.J.; Griffith, L.; Oremus, M.; Raina, P.; Ismaila, A.; et al. Conducting quantitative synthesis when comparing medical interventions: AHRQ and the Effective Health Care Program. J. Clin. Epidemiol. 2011, 64, 1187–1197. [Google Scholar] [CrossRef]
- Fernández-Castilla, B.; Declercq, L.; Jamshidi, L.; Beretvas, S.N.; Onghena, P.; Noortgate, W.V.D. Detecting Selection Bias in Meta-Analyses with Multiple Outcomes: A Simulation Study. J. Exp. Educ. 2021, 89, 125–144. [Google Scholar] [CrossRef]
- Bürkner, P. Brms: An R package for bayesian multilevel models using stan. J. Stat. Softw. 2017, 80, 1–28. [Google Scholar] [CrossRef]
- Candow, D.G.; Chilibeck, P.D.; Burke, D.G.; Mueller, K.D.; Lewis, J.D. Effect of different frequencies of creatine supplementation on muscle size and strength in young adults. J. Strength Cond. Res. 2011, 25, 1831–1838. [Google Scholar] [CrossRef]
- Mills, S.; Candow, D.G.; Forbes, S.C.; Neary, J.P.; Ormsbee, M.J.; Antonio, J. Effects of Creatine Supplementation during Resistance Training Sessions in Physically Active Young Adults. Nutrients 2020, 12, 1880. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Silva, R.; Cholewa, J.M.; Pessôa, K.d.A.; Xia, Z.; Lauver, J.D.; Rossi, F.E.; Zanchi, N.E. Creatine supplementation combined with blood flow restriction training enhances muscle thickness and performance: A randomized, placebo-controlled, and double-blind study. Appl. Physiol. Nutr. Metab. 2023. [Google Scholar] [CrossRef] [PubMed]
- Pakulak, A.; Candow, D.G.; de Zepetnek, J.T.; Forbes, S.C.; Basta, D. Effects of Creatine and Caffeine Supplementation During Resistance Training on Body Composition, Strength, Endurance, Rating of Perceived Exertion and Fatigue in Trained Young Adults. J. Diet. Suppl. 2022, 19, 587–602. [Google Scholar] [CrossRef] [PubMed]
- Bernat, P.; Candow, D.G.; Gryzb, K.; Butchart, S.; Schoenfeld, B.J.; Bruno, P. Effects of high-velocity resistance training and creatine supplementation in untrained healthy aging males. Appl. Physiol. Nutr. Metab. 2019, 44, 1246–1253. [Google Scholar] [CrossRef] [PubMed]
- Candow, D.G.; Chilibeck, P.D.; Gordon, J.; Vogt, E.; Landeryou, T.; Kaviani, M.; Paus-Jensen, L. Effect of 12 months of creatine supplementation and whole-body resistance training on measures of bone, muscle and strength in older males. Nutr. Health 2021, 27, 151–159. [Google Scholar] [CrossRef]
- Candow, D.G.; Little, J.P.; Chilibeck, P.D.; Abeysekara, S.; Zello, G.A.; Kazachkov, M.; Cornish, S.M.; Yu, P.H. Low-Dose Creatine Combined with Protein during Resistance Training in Older Men. Med. Sci. Sports Exerc. 2008, 40, 1645–1652. [Google Scholar] [CrossRef]
- Chilibeck, P.D.; Candow, D.G.; Landeryou, T.; Kaviani, M.; Paus-Jenssen, L. Effects of Creatine and Resistance Training on Bone Health in Postmenopausal Women. Med. Sci. Sports Exerc. 2015, 47, 1587–1595. [Google Scholar] [CrossRef]
- Roschel, H.; Hayashi, A.P.; Fernandes, A.L.; Jambassi-Filho, J.C.; Hevia-Larraín, V.; de Capitani, M.; Santana, D.A.; Gonçalves, L.S.; de Sá-Pinto, A.L.; Lima, F.R.; et al. Supplement-based nutritional strategies to tackle frailty: A multifactorial, double-blind, randomized placebo-controlled trial. Clin. Nutr. 2021, 40, 4849–4858. [Google Scholar] [CrossRef]
- Candow, D.G.; Chilibeck, P.D.; Gordon, J.J.; Kontulainen, S. Efficacy of Creatine Supplementation and Resistance Training on Area and Density of Bone and Muscle in Older Adults. Med. Sci. Sports Exerc. 2021, 53, 2388–2395. [Google Scholar] [CrossRef]
- Nunes, J.P.; Ribeiro, A.S.; Schoenfeld, B.J.; Tomeleri, C.M.; Avelar, A.; Trindade, M.C.; Nabuco, H.C.G.; Cavalcante, E.F.; Junior, P.S.; Fernandes, R.R.; et al. Creatine supplementation elicits greater muscle hypertrophy in upper than lower limbs and trunk in resistance-trained men. Nutr. Health 2017, 23, 223–229. [Google Scholar] [CrossRef]
- Syrotuik, D.G.; Bell, G.J. Acute creatine monohydrate supplementation: A descriptive physiological profile of responders vs. nonresponders. J. Strength Cond. Res. 2004, 18, 610–617. [Google Scholar] [PubMed]
- Elder, G.C.; Bradbury, K.; Roberts, R. Variability of fiber type distributions within human muscles. J. Appl. Physiol. 1982, 53, 1473–1480. [Google Scholar] [CrossRef] [PubMed]
- Greenhaff, P.L. Creatine supplementation: Recent developments. Br. J. Sports Med. 1996, 30, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Greenhaff, P.L.; Bodin, K.; Soderlund, K.; Hultman, E. Effect of oral creatine supplementation on skeletal muscle phosphocreatine resynthesis. Am. J. Physiol. Metab. 1994, 266 Pt 1, E725–E730. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Sample | Design | RT Protocol | CR Protocol | Duration | Results |
|---|---|---|---|---|---|---|
| Bernat et al. [37] | 24 older, untrained men | Random assignment to 1 of 2 groups: (1) CR + RT; (2) PLA + RT | Total body unsupervised protocol performed 2 d/wk consisting of 3–4 sets per exercise at 80% 1 RM with 2 min inter-set rest intervals | 0.1 g/kg/d consumed post-training and at participants’ leisure on non-training days | 8 wks |
|
| Candow et al. [33] | 38 young, physically active, untrained men and women | Random assignment to 1 of 4 groups: (1) CR + RT performed twice/wk; (2) CR + RT performed thrice/wk; (3) PLA + RT performed twice/wk; (4) PLA + RT performed thrice/wk | Total body protocol performed 2–3 d/wk consisting of 2–3 sets per exercise of 10 repetitions with 1–2 min inter-set rest intervals | 0.15 g/kg/d for participants in 2 d/wk RT and 0.10 g/kg for participants in 3 d/wk RT; no mention of supplementation on non-training days | 6 wks |
|
| Candow, Chilibeck, Gordon, Vogt et al. [38] | 46 older, untrained men | Random assignment to 1 of 2 groups: (1) CR + RT; (2) PLA + RT | Total body supervised protocol performed 3 d/wk consisting of 3 sets of 10 repetitions per exercise at 80% 1 RM | 0.1 g/kg/d consumed in 2 equal doses pre- and post-training and with food on non-training days | 12 months |
|
| Candow et al. [39] | 25 older, untrained men | Random assignment to 1 of 2 groups: (1) CR + RT; (2) PLA + RT | Total body supervised protocol performed 3 d/wk consisting of 3 sets of 10 repetitions with 2 min inter-set rest intervals | 0.1 g/kg/d consumed in 3 equal doses pre- and post-training and before bed on training days; no supplementation on non-training days | 10 wks |
|
| Candow, Chilibeck, Gordon & Kontulainen [42] | 52 older, untrained men and women | Random assignment to 1 of 2 groups: (1) CR + RT; (2) PLA + RT | Total body supervised protocol performed 3 d/wk consisting of 3 sets of 10 repetitions per exercise | 0.1 g/kg/d consumed in 2 equal doses pre- and post-training and with food on non-training days | 12 months |
|
| Chilibeck et al. [40] | 33 postmenopausal, untrained women | Random assignment to 1 of 2 groups: (1) CR + RT; (2) PLA + RT | Total body supervised protocol performed 3 d/wk consisting of 3 sets of 10 repetitions per exercise | 0.1 g/kg/d consumed in 2 equal doses pre- and post-training and with food on non-training days | 12 months |
|
| Mills et al. [34] | 22 young, recreationally trained men and women | Random assignment to 1 of 2 groups: (1) CR + RT; (2) PLA + RT | Total body protocol performed 5 d/wk consisting of 3 sets per exercise of 6–10 repetitions with 2 min inter-set rest intervals | 0.1 g/kg/d consumed during training sessions (5 d/wk); no supplementation on non-training days | 6 wks |
|
| Pakulak et al. [36] | 13 young, resistance-trained men and women | Random assignment to 1 of 2 groups: (1) CR + RT; (2) PLA + RT | Total body protocol performed 4 d/wk consisting of 3 sets per exercise of 6–10 repetitions with 2 min inter-set rest intervals | 0.1 g/kg/d consumed 60 min prior to training sessions (4 d/wk); no supplementation on non-training days | 6 wks |
|
| Roschel et al. [41] | 88 elderly, pre-frail and frail men and women | Random assignment to 1 of 4 groups: (1) CR + RT; (2) PLA + RT; (3) CR + Whey + RT; (4) Whey + RT | Total body supervised protocol performed 2 d/wk consisting of 2–4 sets at 50–70% 1 RM | 6 g/d in CR + RT and 6 g/d + 30 g Whey in CR + Whey + RT; supplements consumed 7 d/wk | 16 wks |
|
| Sousa-Silva et al. [35] | 17 young, untrained men | Random assignment to 1 of 2 groups: (1) CR + RT; (2) PLA + RT | Unilateral elbow flexion protocol (2 d/wk): One arm of each participant performed the biceps curl combined with blood flow restriction for 4 sets of 15–30 reps at 30% 1 RM with 30 s inter-set rest intervals and the other arm performed the biceps curl without blood flow restriction for 4 sets of 10–12 repetitions at 70% 1 RM with 2 min inter-set rest intervals | 20 g/d consumed for the first 5 days followed by 5 g/d consumed post-training and during regular training time on non-training days | 8 wks |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burke, R.; Piñero, A.; Coleman, M.; Mohan, A.; Sapuppo, M.; Augustin, F.; Aragon, A.A.; Candow, D.G.; Forbes, S.C.; Swinton, P.; et al. The Effects of Creatine Supplementation Combined with Resistance Training on Regional Measures of Muscle Hypertrophy: A Systematic Review with Meta-Analysis. Nutrients 2023, 15, 2116. https://doi.org/10.3390/nu15092116
Burke R, Piñero A, Coleman M, Mohan A, Sapuppo M, Augustin F, Aragon AA, Candow DG, Forbes SC, Swinton P, et al. The Effects of Creatine Supplementation Combined with Resistance Training on Regional Measures of Muscle Hypertrophy: A Systematic Review with Meta-Analysis. Nutrients. 2023; 15(9):2116. https://doi.org/10.3390/nu15092116
Chicago/Turabian StyleBurke, Ryan, Alec Piñero, Max Coleman, Adam Mohan, Max Sapuppo, Francesca Augustin, Alan A. Aragon, Darren G. Candow, Scott C. Forbes, Paul Swinton, and et al. 2023. "The Effects of Creatine Supplementation Combined with Resistance Training on Regional Measures of Muscle Hypertrophy: A Systematic Review with Meta-Analysis" Nutrients 15, no. 9: 2116. https://doi.org/10.3390/nu15092116