

Effectiveness of Positive Deviance Approach to Reduce Malnutrition among under Five Children: A Systematic Review and Meta-Analysis of Interventional Studies



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources, Search Strategies, and Serach Process
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias
2.5. Statistical Analysis
2.6. Ethical Clearence
3. Results
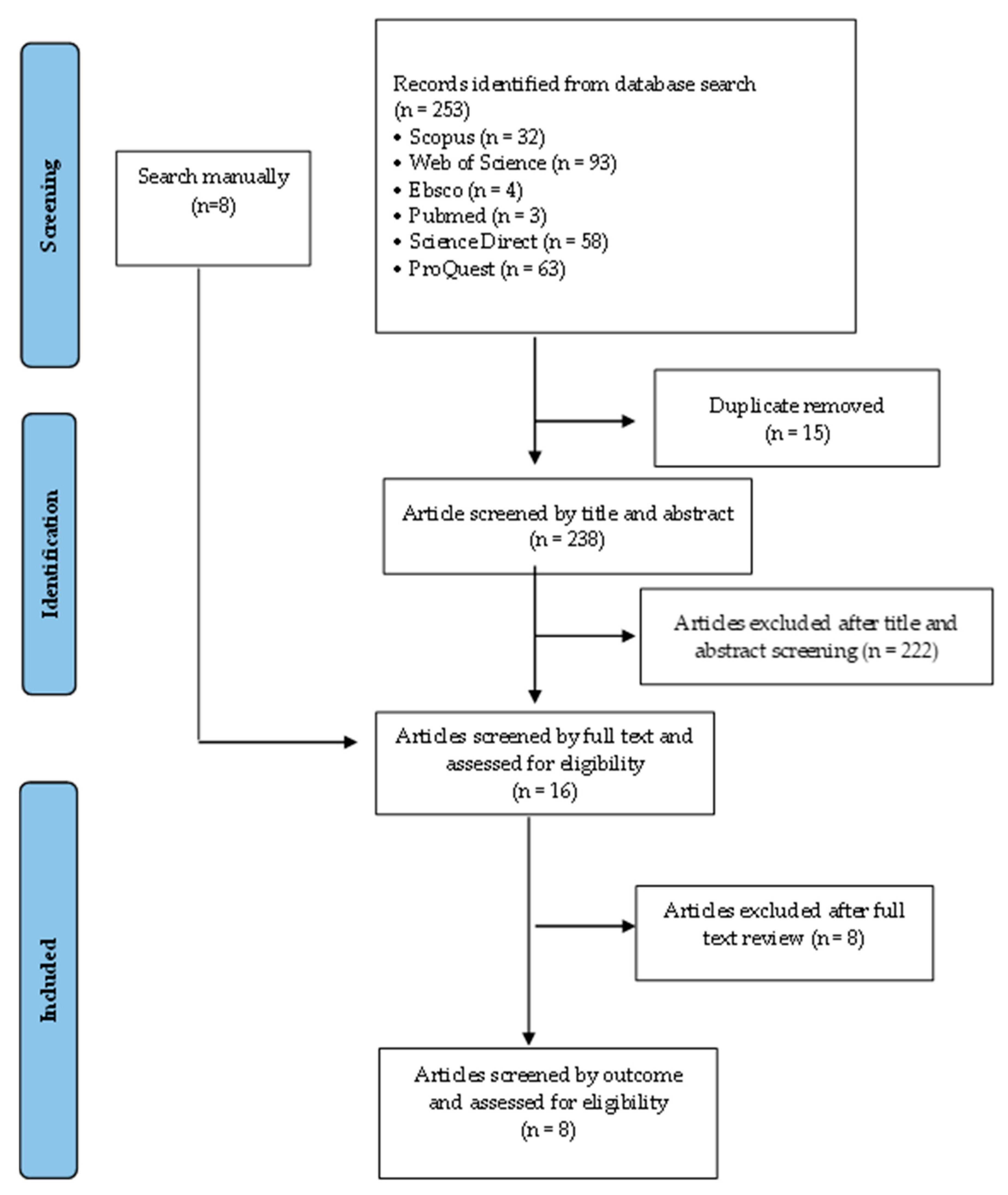
3.1. Database Search
3.2. Study Description
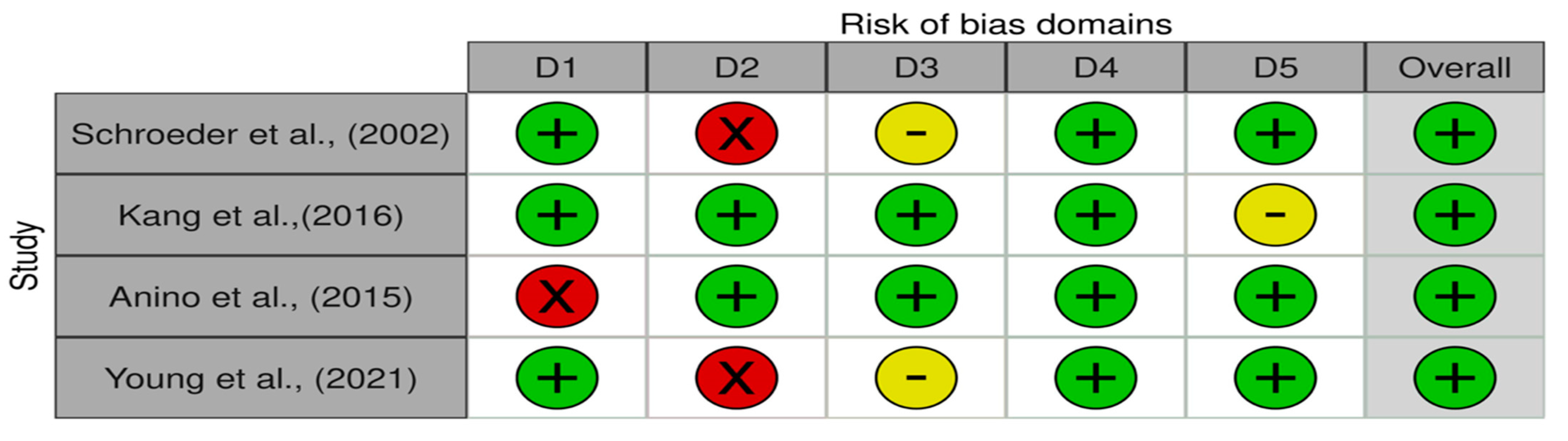
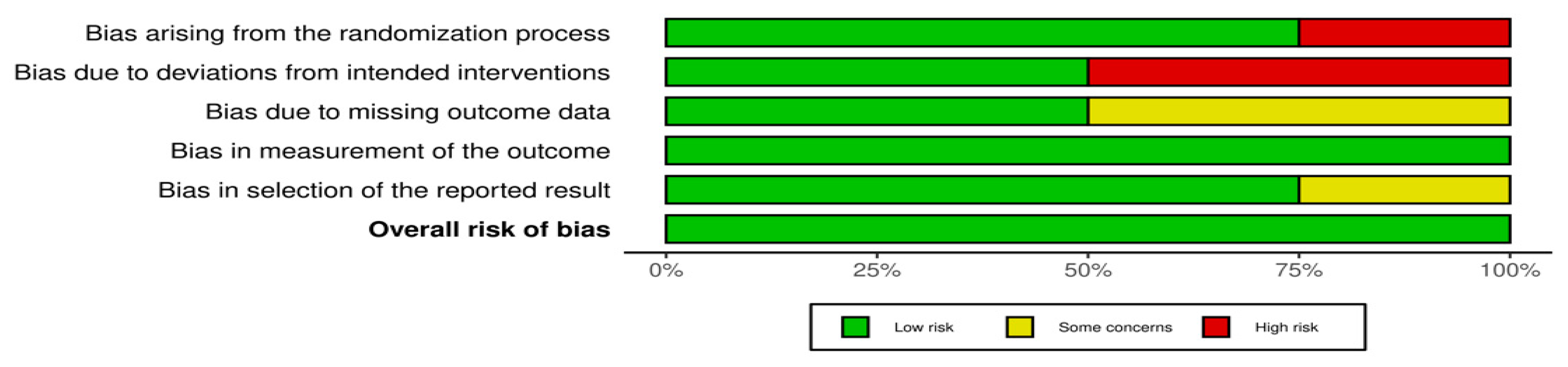
3.3. Risk of Bias
3.4. Meta-Analysis Results
3.4.1. Effect of Positive Deviance-Based Interventions on Length for Age Z-Score (LAZ)
3.4.2. Effect of Positive Deviance-Based Interventions on Weight for Age Z-Score (WAZ)
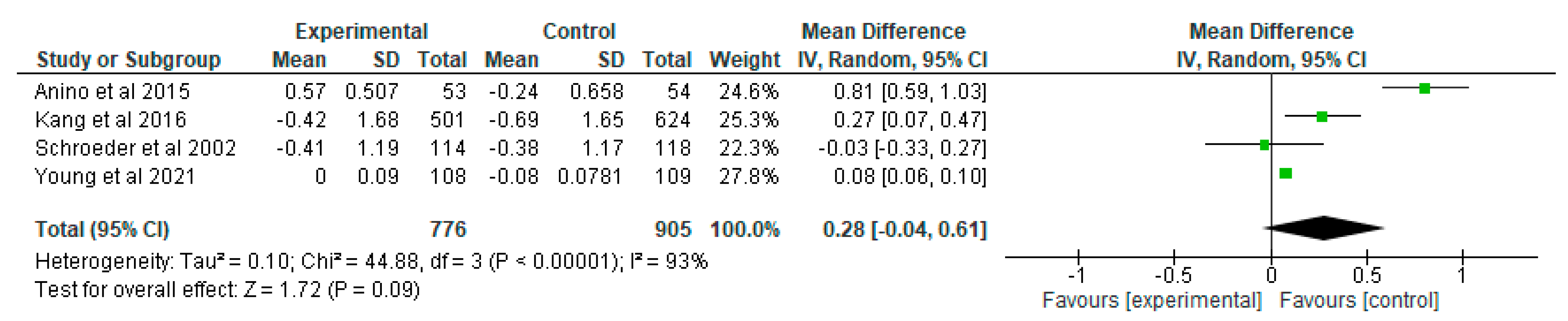
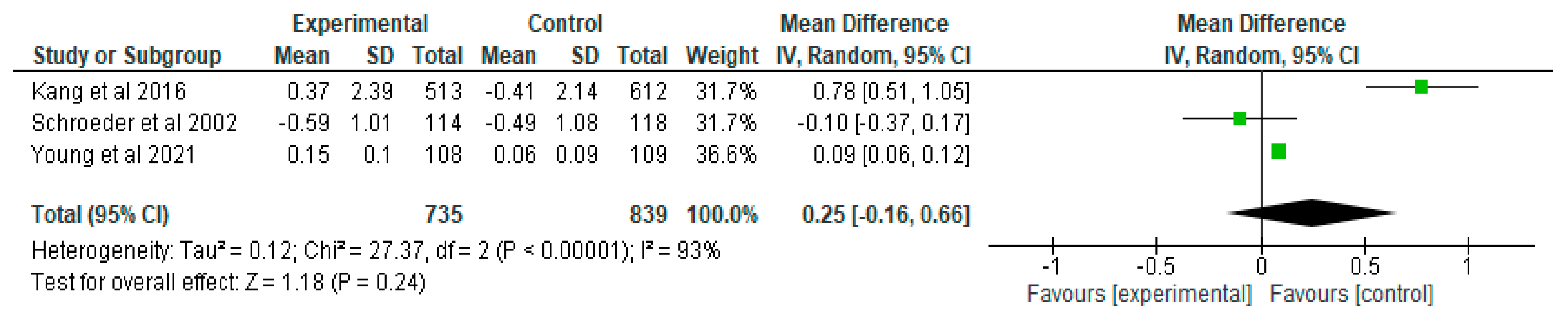
3.4.3. Effect of Positive Deviance-Based Interventions on Weight for Height Z-Score (WHZ)
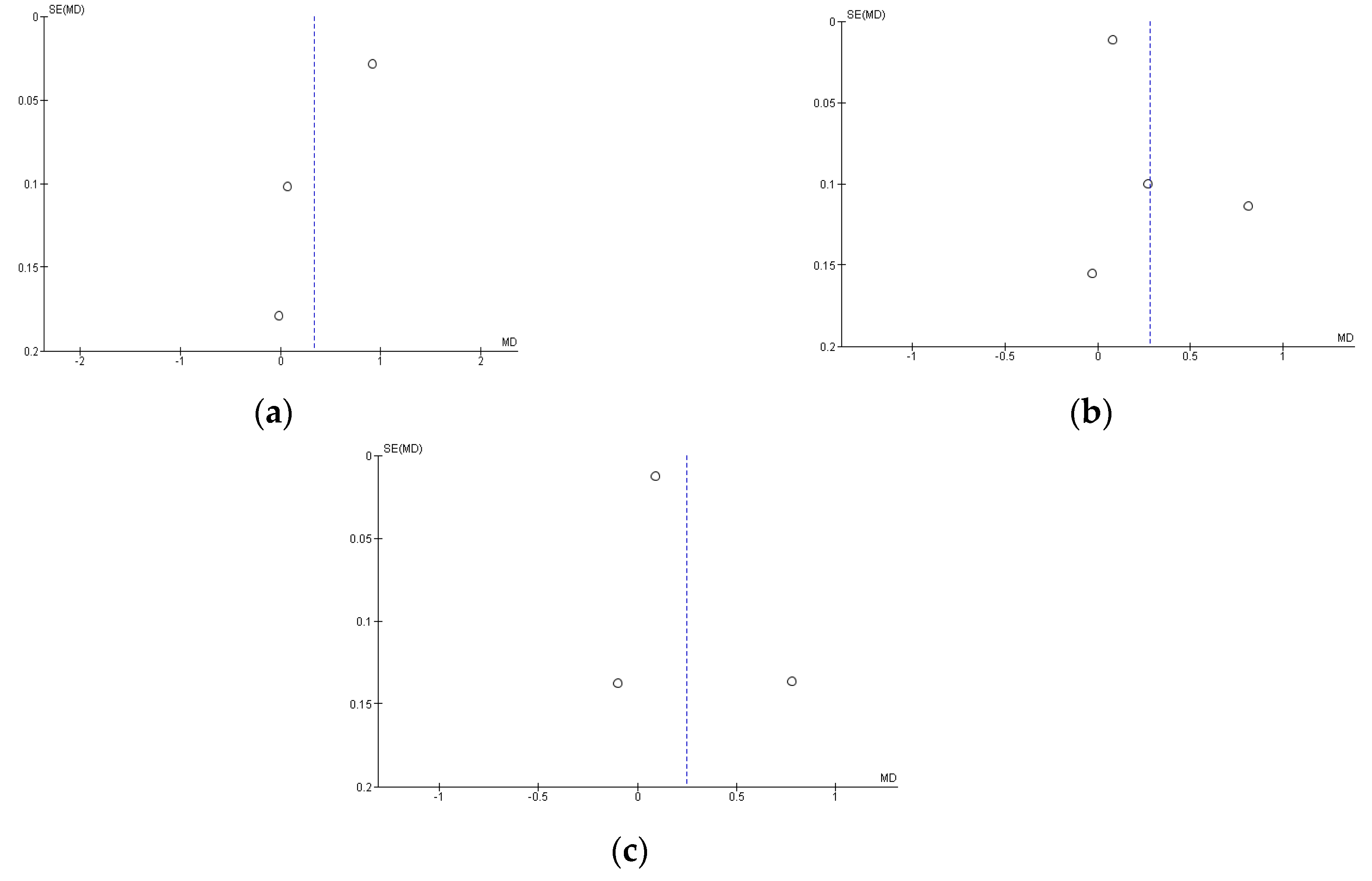
3.5. Risk of Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Stunting Prevalence among Children under 5 Years of Age.Pdf. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/gho-jme-stunting-prevalence (accessed on 6 October 2022).
- UNICEF; WHO; World Bank. Levels and Trends Child Malnutrition: Key Findings of the 2020 Edition of the Joint Child Malnutrition Estimate; WHO: Geneva, Switzerland, 2020; Volume 24, pp. 1–16. [Google Scholar]
- Moench-Pfanner, R.; Silo, S.; Laillou, A.; Wieringa, F.; Hong, R.; Hong, R.; Poirot, E.; Bagriansky, J. The Economic Burden of Malnutrition in Pregnant Women and Children under 5 Years of Age in Cambodia. Nutrients 2016, 8, 292. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, A.J.; Humphrey, J.H. The Stunting Syndrome in Developing Countries. Paediatr. Int. Child Health 2014, 34, 250–265. [Google Scholar] [CrossRef] [PubMed]
- Olofin, I.; McDonald, C.M.; Ezzati, M.; Flaxman, S.; Black, R.E.; Fawzi, W.W.; Caulfield, L.E.; Danaei, G.; Adair, L.; Arifeen, S.; et al. Associations of Suboptimal Growth with All-Cause and Cause-Specific Mortality in Children under Five Years: A Pooled Analysis of Ten Prospective Studies. PLoS ONE 2013, 8, e64636. [Google Scholar] [CrossRef] [PubMed]
- Grillo, L.P.; Gigante, D.P.; Horta, B.L.; De Barros, F.C.F. Childhood Stunting and the Metabolic Syndrome Components in Young Adults from a Brazilian Birth Cohort Study. Eur. J. Clin. Nutr. 2016, 70, 548–553. [Google Scholar] [CrossRef]
- De Lucia Rolfe, E.; de França GV, A.; Vianna, C.A.; Gigante, D.P.; Miranda, J.J.; Yudkin, J.S.; Horta, B.L.; Ong, K.K. Associations of Stunting in Early Childhood with Cardiometabolic Risk Factors in Adulthood. PLoS ONE 2018, 13, e0192196. [Google Scholar] [CrossRef]
- Mahmudiono, T.; Sumarmi, S.; Rosenkranz, R.R. Household Dietary Diversity and Child Stunting in East Java, Indonesia. Asia Pac. J. Clin. Nutr. 2017, 26, 317–325. [Google Scholar] [CrossRef]
- Mahmudiono, T.; Nindya, T.S.; Andrias, D.R.; Megatsari, H.; Rosenkranz, R.R. Household Food Insecurity as a Predictor of Stunted Children and Overweight/Obese Mothers (SCOWT) in Urban Indonesia. Nutrients 2018, 10, 535. [Google Scholar] [CrossRef]
- Stewart, C.P.; Iannotti, L.; Dewey, K.G.; Michaelsen, K.F.; Onyango, A.W. Contextualising Complementary Feeding in a Broader Framework for Stunting Prevention. Matern. Child Nutr. 2013, 9, 27–45. [Google Scholar] [CrossRef]
- Krasevec, J.; An, X.; Kumapley, R.; Bégin, F.; Frongillo, E.A. Diet Quality and Risk of Stunting among Infants and Young Children in Low- and Middle-Income Countries. Matern. Child Nutr. 2017, 13, e12430. [Google Scholar] [CrossRef]
- Mahmudiono, T.; Segalita, C.; Rosenkranz, R.R. Socio-Ecological Model of Correlates of Double Burden of Malnutrition in Developing Countries: A Narrative Review. Int. J. Environ. Res. Public Health 2019, 16, 3730. [Google Scholar] [CrossRef]
- Siswati, T.; Iskandar, S.; Pramestuti, N.; Raharjo, J.; Rubaya, A.K.; Wiratama, B.S. Impact of an Integrative Nutrition Package through Home Visit on Maternal and Children Outcome: Finding from Locus Stunting in Yogyakarta, Indonesia. Nutrients 2022, 14, 3448. [Google Scholar] [CrossRef] [PubMed]
- Sunardi, K.S.; Martha, E. Positive Deviance Behavior in the Low Economic Status Family with Non-Stunting Incidence in Sleman Regency, Yogyakarta, Indonesia. Univ. J. Public Health 2021, 9, 353–359. [Google Scholar] [CrossRef]
- Boulom, S.; Bon, D.M.; Essink, D.; Kounnavong, S.; Broerse, J.E.W. Understanding Discrepancies in Nutritional Outcomes Among Under-Fives in Laos: A Mixed-Methods Study Using the Positive Deviance Approach. Food Nutr. Bull. 2022, 43, 303–322. [Google Scholar] [CrossRef]
- Lapping, K.; Marsh, D.R.; Rosenbaum, J.; Swedberg, E.; Sternin, J.; Sternin, M.; Schroeder, D.G. The Positive Deviance Approach: Challenges and Opportunities for the Future. Food Nutr. Bull. 2002, 23 (Suppl. S4), 130–137. [Google Scholar] [CrossRef] [PubMed]
- Schooley, J.; Morales, L. Learning From the Community to Improve Maternal-Child Health and Nutrition: The Positive Deviance/Hearth Approach. J. Midwifery Women’s Health 2007, 52, 376–383. [Google Scholar] [CrossRef]
- Marsh, D.R.; Schroeder, D.G.; Dearden, K.A.; Sternin, J.; Sternin, M. The Power of Positive Deviance: How Does Positive Deviance Work? Experience and Evidence from the Field. Br. Med. J. 2004, 329, 1177–1179. [Google Scholar] [CrossRef]
- Kim, Y.; Biswas, J.P.; Hossain, M.I.; Baik, D.; Reinsma, K.; Min, S.; Kang, Y. Age Differences in the Impact of a Positive Deviance/Hearth Programme on the Nutritional Status of Children in Rural Bangladesh. Public Health Nutr. 2021, 24, 5514–5523. [Google Scholar] [CrossRef]
- Kang, Y.; Suh, Y.K.; Debele, L.; Juon, H.S.; Christian, P. Effects of a Community-Based Nutrition Promotion Programme on Child Feeding and Hygiene Practices among Caregivers in Rural Eastern Ethiopia. Public Health Nutr. 2017, 20, 1461–1472. [Google Scholar] [CrossRef]
- Roche, M.L.; Marquis, G.S.; Gyorkos, T.W.; Blouin, B.; Sarsoza, J.; Kuhnlein, H.V. A Community-Based Positive Deviance/Hearth Infant and Young Child Nutrition Intervention in Ecuador Improved Diet and Reduced Underweight. J. Nutr. Educ. Behav. 2017, 49, 196–203.e1. [Google Scholar] [CrossRef]
- Sripaipan, T.; Schroeder, D.G.; Marsh, D.R.; Pachón, H.; Dearden, K.A.; Ha, T.T.; Lang, T.T. Effect of an Integrated Nutrition Program on Child Morbidity Due to Respiratory Infection and Diarrhea in Northern Viet Nam. Food Nutr. Bull. 2002, 23 (Suppl. S4), 70–77. [Google Scholar] [CrossRef]
- Bisits Bullen, P.A. The Positive Deviance/Hearth Approach to Reducing Child Malnutrition: Systematic Review. Trop. Med. Int. Health 2011, 16, 1354–1366. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: New York, NY, USA, 2019; pp. 1–694. [Google Scholar] [CrossRef]
- Chittaranjan Andrade, M. Mean Difference, Standardized Mean Difference (SMD), and Their Use in Meta-Analysis: As Simple as It Gets. J. Clin. Psychiatry 2015, 77, 22–27. [Google Scholar]
- Chittaranjan Andrade, M. Understanding the Basics of Meta-Analysis and How to Read a Forest Plot. J. Clin. Psychiatry 2020, 81, 21858. [Google Scholar]
- Kang, Y.; Kim, S.; Sinamo, S.; Christian, P. Effectiveness of a Community-Based Nutrition Programme to Improve Child Growth in Rural Ethiopia: A Cluster Randomized Trial. Matern. Child Nutr. 2017, 13, 10. [Google Scholar] [CrossRef]
- Schroeder, D.G.; Pachón, H.; Dearden, K.A.; Kwon, C.B.; Ha, T.T.; Lang, T.T.; Marsh, D.R. An Integrated Child Nutrition Intervention Improved Growth of Younger, More Malnourished Children in Northern Viet Nam. Food Nutr. Bull. 2002, 23 (Suppl. S4), 53–61. [Google Scholar] [CrossRef]
- Young, M.F.; Baik, D.; Reinsma, K.; Gosdin, L.; Rogers, H.P.; Oy, S.; Invong, W.; Hen, H.; Ouk, S.; Chhorvann, C. Evaluation of Mobile Phone-Based Positive Deviance/Hearth Child Undernutrition Program in Cambodia. Matern. Child Nutr. 2021, 17, e13224. [Google Scholar] [CrossRef]
- Anino, O.; Were, G.; Khamasi, J. Impact Evaluation of Positive Deviance Hearth in Migori. Afr. J. Food Agric. Nutr. Dev. 2015, 15, 10578–10596. [Google Scholar]
- Seetha, A.; Tsusaka, T.W.; Munthali, T.W.; Musukwa, M.; Mwangwela, A.; Kalumikiza, Z.; Manani, T.; Kachulu, L.; Kumwenda, N.; Musoke, M.; et al. How Immediate and Significant Is the Outcome of Training on Diversified Diets, Hygiene and Food Safety? An Effort to Mitigate Child Undernutrition in Rural Malawi. Public Health Nutr. 2018, 21, 1156–1166. [Google Scholar] [CrossRef]
- le Roux, I.M.; le Roux, K.; Mbeutu, K.; Comulada, W.S.; Desmond, K.A.; Rotheram-Borus, M.J. A Randomized Controlled Trial of Home Visits by Neighborhood Mentor Mothers to Improve Children’s Nutrition in South Africa. Vulnerable Child. Youth Stud. 2011, 6, 91–102. [Google Scholar] [CrossRef]
- Le Roux, I.M.; Le Roux, K.; Comulada, W.S.; Greco, E.M.; Desmond, K.A.; Mbewu, N.; Rotheram-Borus, M.J. Home Visits by Neighborhood Mentor Mothers Provide Timely Recovery from Childhood Malnutrition in South Africa: Results from a Randomized Controlled Trial. Nutr. J. 2010, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for Examining and Interpreting Funnel Plot Asymmetry in Meta-Analyses of Randomised Controlled Trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [PubMed]
- Sedgwick, P.; Marston, L. How to Read a Funnel Plot in a Meta-Analysis. BMJ 2015, 351, h4718. [Google Scholar] [CrossRef] [PubMed]
- Pachón, H.; Schroeder, D.G.; Marsh, D.R.; Dearden, K.A.; Ha, T.T.; Lang, T.T. Effect of an Integrated Child Nutrition Intervention on the Complementary Food Intake Young Children in Rural North Viet Nam. Food Nutr. Bull. 2002, 23 (Suppl. S4), 62–69. [Google Scholar] [CrossRef]
- Marsh, D.R.; Pachón, H.; Schroeder, D.G.; Ha, T.T.; Dearden, K.; Lang, T.T.; Hien, N.D.; Tuan, D.A.; Thach, T.D.; Claussenius, D.R. Design of a Prospective, Randomized Evaluation of an Integrated Nutrition Program in Rural Viet Nam. Food Nutr. Bull. 2002, 23 (Suppl. S4), 36–47. [Google Scholar] [CrossRef]
- Baxter, R.; Lawton, R. The Positive Deviance Approach (Elements of Improving Quality and Safety in Healthcare; Cambridge University Press: Cambridge, UK, 2022; Volume 2912. [Google Scholar]
- Nutrition Working Group; CORE. Positive Deviance/Hearth A Resource Guide for Sustainably Rehabilitating Malnourished Children; USAID: Washington, DC, USA, 2002.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Strategy | Number of Articles |
|---|---|---|
| Scopus | TITLE-ABS-KEY (“positive deviance intervention” OR “hearth” AND (“under five children stunting” OR “wasting” OR “underweight” OR “children malnutrition” OR “nutritional status” OR “child growth”)) AND (LIMIT-TO (LANGUAGE, “English”)) | 32 |
| Web of Science | “positive deviance intervention” OR “hearth” AND (“under five children stunting” OR “wasting” OR “underweight” OR “children malnutrition” OR “nutritional status” | 93 |
| Proquest | “positive deviance intervention” OR “hearth intervention” AND “under five children stunting wasting underweight” OR “under five child malnutrition” OR “under five child nutritional status” NOT “literature review” NOT “systematic review” NOT “meta-analysis” | 63 |
| EBSCO | “positive deviance intervention” OR “hearth” AND (“under five children stunting” OR “wasting” OR “underweight” OR “child malnutrition” OR “nutritional status”) | 4 |
| Pubmed | “positive deviance intervention” OR “hearth” AND (“under five children stunting” OR “wasting” OR “underweight” OR “child malnutrition” OR “nutritional status”) | 3 |
| Science direct | “positive deviance” OR “hearth” AND “experimental trial” AND “under five children stunting” OR “under five children wasting” OR “under five children underweight” OR “under five child malnutrition” OR “under five child nutritional status” | 58 |
| Study | Study Design | Country | Sample (n) | Age | Intervention | Control | Duration | Outcome |
|---|---|---|---|---|---|---|---|---|
| Kang et al. (2016) [28] | community-based cluster randomized trial | Ethiopia | 1790 | 6–24 month | a community-based participatory nutrition promotion (CPNP) program adapting a Positive Deviance/Hearth approach | community-based nutrition programs in poor rural districts | 12 days intervention and 12 months follow-up | Mean of LAZ, WAZ, and LWZ |
| Schroeder et al. (2002) [29] | Longitudinal, randomized controlled design | Vietnam | 232 | 5–36 month | Positive deviance program | No Program | 12 days intervention and 12 months follow-up | Mean of LAZ, WAZ, and LWZ |
| Young et al. (2021) [30] | Longitudinal cluster randomized controlled trial | Kamboja | 330 | 6–23 month | (1) traditional Positive Deviance/Hearth (PDH) program with in-person visits, (2) Positive Deviance/Hearth with Interactive Voice Calling (PDH-IVC) program | the standard government Basic Health and Nutrition Package | 10 days intervention and 12 months follow-up | Mean of LAZ, WAZ, and LWZ |
| Anino et al. (2015) [31] | Quasy Experimental | Kenya | 107 | 6–59 month | Positive deviance program | No Program | 12 days intervention and 6 months follow-up | Mean of LAZ, WAZ, and LWZ |
| Seetha et al. (2018) [32] | Randomized controlled trial | Malawi | 179 | 0–23 month | Positive deviance/Hearth model | No program | 21 days | Difference of mean of LAZ, WAZ, and LWZ |
| Le Roux et al. (2011) [33] | Randomized controlled trial | Afrika Selatan | 635 | 6–12 month | Positive deviance/Hearth model | No program | 12 days intervention and 12 months follow-up | Mean of WAZ |
| Roche et al. (2016) [21] | Quasy experimental | Ecuador | 264 | 0–23 month | Positive deviance/Hearth model | No program | 12 days intervention and 6 months follow-up | Mean percentage of the recommended intake, Change of WAZ |
| Le Roux et al. (2010) [34] | Randomized controlled trial | South Africa | 788 | 0–5 years old | Mentor mother with positive deviance | community-based nutrition programs from government | 12 days intervention and 6 months follow-up | Weight rehabilitation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Triatmaja, N.T.; Mahmudiono, T.; Mamun, A.A.; Abdullah, N.A. Effectiveness of Positive Deviance Approach to Reduce Malnutrition among under Five Children: A Systematic Review and Meta-Analysis of Interventional Studies. Nutrients 2023, 15, 1961. https://doi.org/10.3390/nu15081961
Triatmaja NT, Mahmudiono T, Mamun AA, Abdullah NA. Effectiveness of Positive Deviance Approach to Reduce Malnutrition among under Five Children: A Systematic Review and Meta-Analysis of Interventional Studies. Nutrients. 2023; 15(8):1961. https://doi.org/10.3390/nu15081961
Chicago/Turabian StyleTriatmaja, Nining Tyas, Trias Mahmudiono, Abdullah Al Mamun, and Nurul Ashikin Abdullah. 2023. "Effectiveness of Positive Deviance Approach to Reduce Malnutrition among under Five Children: A Systematic Review and Meta-Analysis of Interventional Studies" Nutrients 15, no. 8: 1961. https://doi.org/10.3390/nu15081961