

Effects on Serum Hormone Concentrations after a Dietary Phytoestrogen Intervention in Patients with Prostate Cancer: A Randomized Controlled Trial

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
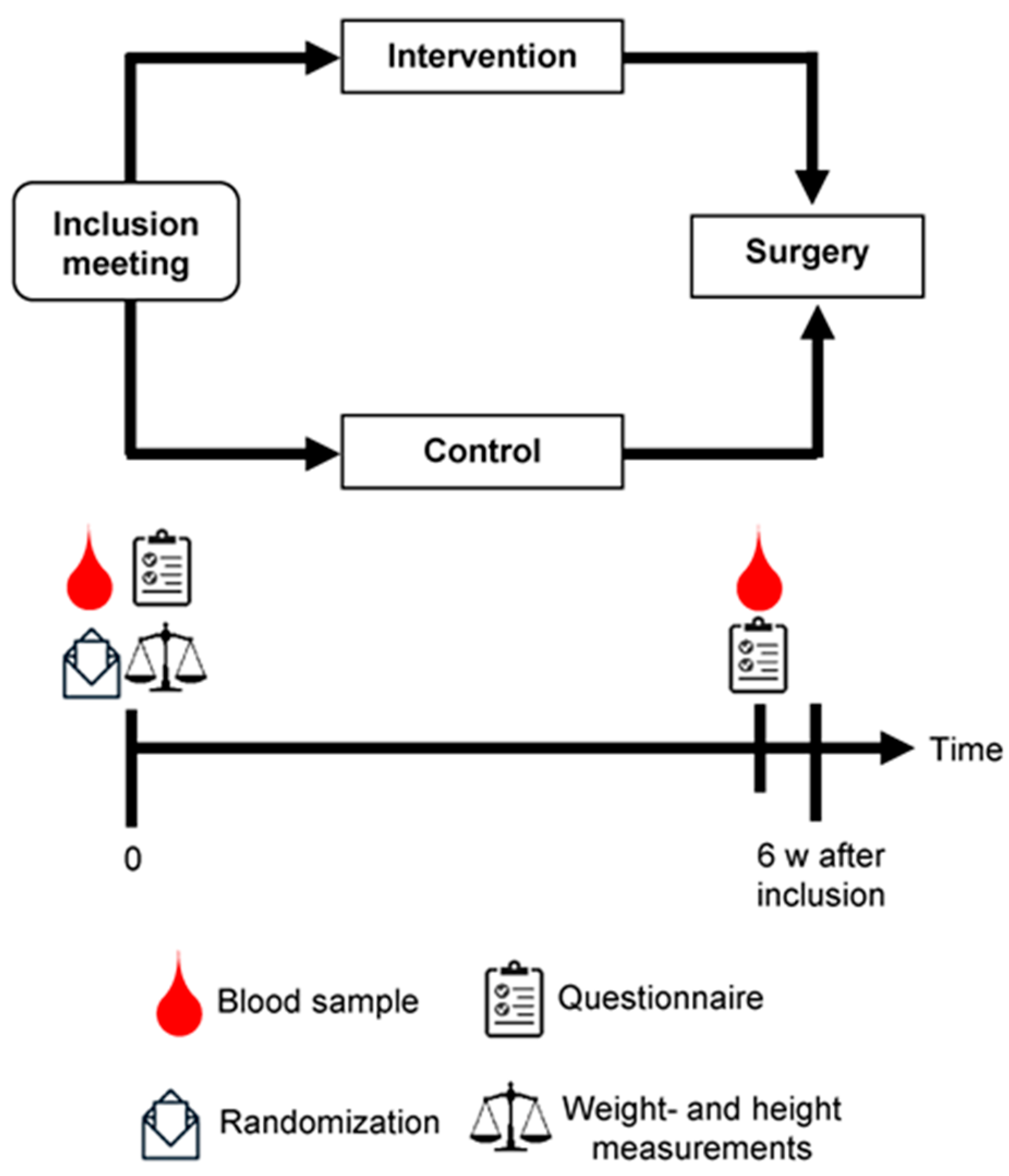
2.1. Study Population and Study Design
2.2. Intervention and Control Diets
2.3. Blood Samples
2.4. Statistical Analysis
3. Results
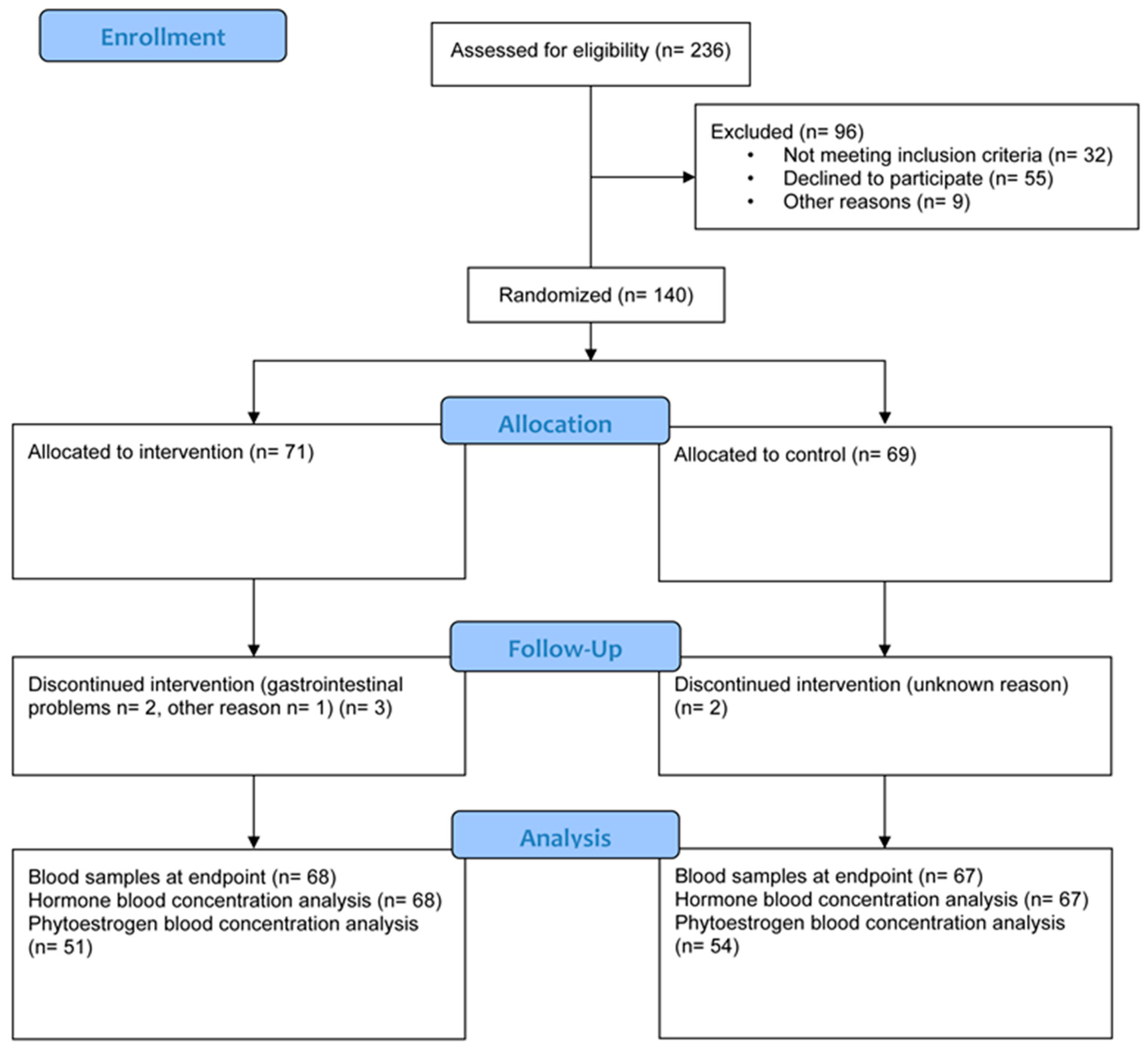
3.1. Population and Baseline Characteristics
3.2. Effects of the Intervention Diet on Hormone Concentrations
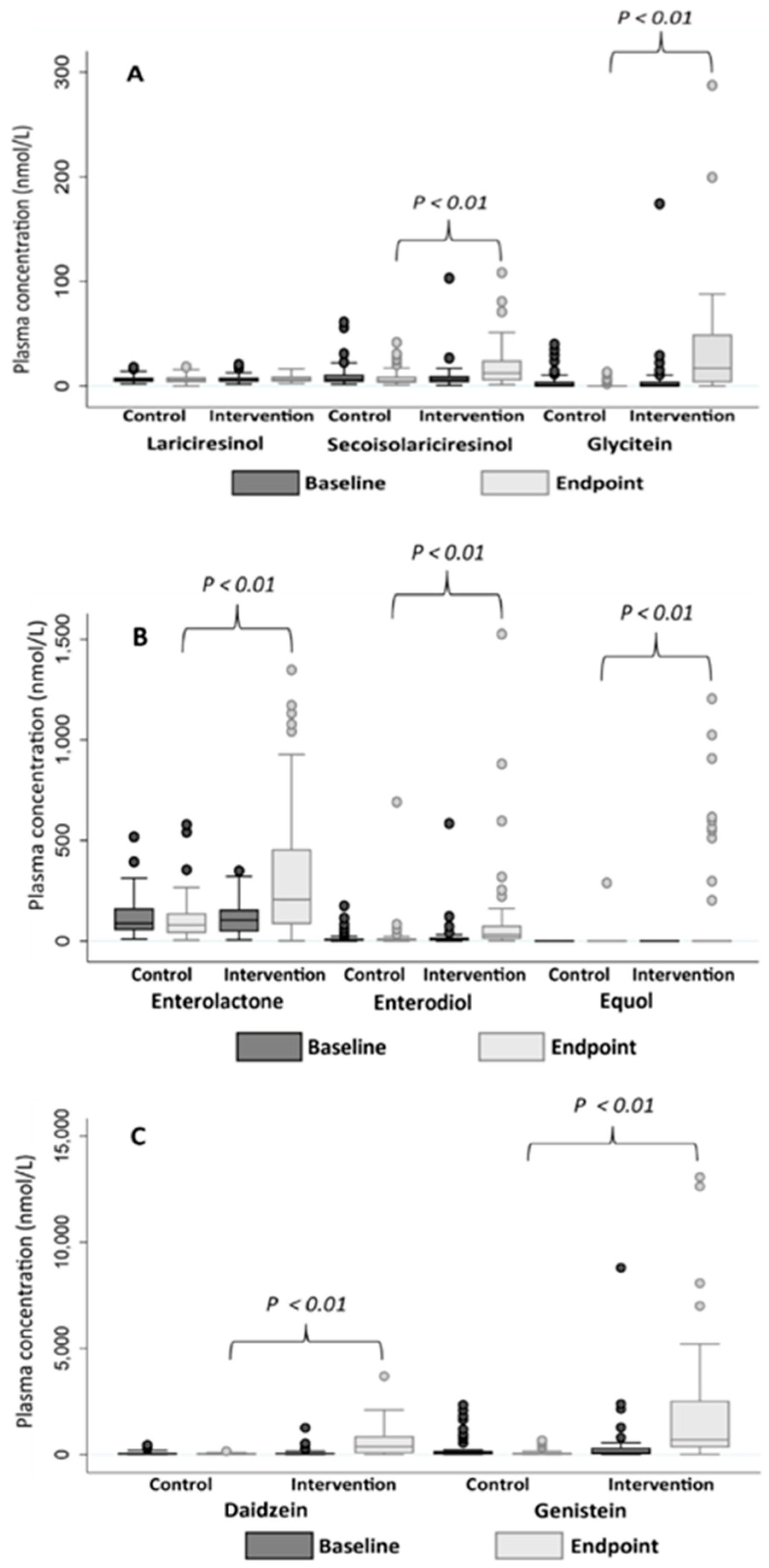
3.3. Plasma Concentrations of Phytoestrogens
3.4. The Relationship between Blood Concentrations of Phytoestrogens and Hormones
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huggins, C.; Hodges, C.V. Studies on prostatic cancer. I. The effect of castration, of estrogen and androgen injection on serum phosphatases in metastatic carcinoma of the prostate. CA Cancer J. Clin. 1972, 22, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Heinlein, C.A.; Chang, C. Androgen receptor in prostate cancer. Endocr. Rev. 2004, 25, 276–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Nunzio, C.; Lombardo, R.; Albisinni, S.; Gacci, M.; Tubaro, A. Serum levels of Sex Hormone Binding Globulin (SHBG) are not predictive of prostate cancer diagnosis and aggressiveness: Results from an italian biopsy cohort. Int. Braz. J. Urol. 2013, 39, 793–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojima, S.; Inahara, M.; Suzuki, H.; Ichikawa, T.; Furuya, Y. Implications of insulin-like growth factor-I for prostate cancer therapies. Int. J. Urol. 2009, 16, 161–167. [Google Scholar] [CrossRef]
- Roddam, A.W.; Allen, N.E.; Appleby, P.; Key, T.J. Endogenous sex hormones and prostate cancer: A collaborative analysis of 18 prospective studies. J. Natl. Cancer Inst. 2008, 100, 170–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Cruz, E.; Carrion Puig, A.; García-Larrosa, A.; Sallent, A.; Castañeda-Argáiz, R.; Piqueras, M.; Ribal, M.J.; Leibar-Tamayo, A.; Romero-Otero, J.; Alcaraz, A. Higher sex hormone-binding globulin and lower bioavailable testosterone are related to prostate cancer detection on prostate biopsy. Scand. J. Urol. 2013, 47, 282–289. [Google Scholar] [CrossRef]
- Dobbs, R.W.; Malhotra, N.R.; Greenwald, D.T.; Wang, A.Y.; Prins, G.S.; Abern, M.R. Estrogens and prostate cancer. Prostate Cancer Prostatic Dis. 2019, 22, 185–194. [Google Scholar] [CrossRef]
- Kurzer, M.S.; Xu, X. Dietary phytoestrogens. Annu. Rev. Nutr. 1997, 17, 353–381. [Google Scholar] [CrossRef]
- Mueller, S.O.; Simon, S.; Chae, K.; Metzler, M.; Korach, K.S.J.T.S. Phytoestrogens and their human metabolites show distinct agonistic and antagonistic properties on estrogen receptor α (ERα) and ERβ in human cells. Toxicol. Sci. 2004, 80, 14–25. [Google Scholar] [CrossRef] [Green Version]
- Hartman, J.; Strom, A.; Gustafsson, J.A. Current concepts and significance of estrogen receptor beta in prostate cancer. Steroids 2012, 77, 1262–1266. [Google Scholar] [CrossRef]
- Li, J.; Liu, Q.; Jiang, C. Signal Crosstalk and the Role of Estrogen Receptor beta (ERβ) in Prostate Cancer. Med. Sci. Monit. 2022, 28, e935599. [Google Scholar] [CrossRef]
- Setchell, K.; Adlercreutz, H. Mammalian Lignans and Phytooestrogens Recent Studies on their Formation, Metabolism and Biological Role in Health and Disease. Role Gut Flora Toxic. Cancer 1988, 14, 315–345. [Google Scholar]
- Kilkkinen, A.; Pietinen, P.; Klaukka, T.; Virtamo, J.; Korhonen, P.; Adlercreutz, H. Use of oral antimicrobials decreases serum enterolactone concentration. Am. J. Epidemiol. 2002, 155, 472–477. [Google Scholar] [CrossRef]
- Zhang, Q.; Feng, H.; Qluwakemi, B.; Wang, J.; Yao, S.; Cheng, G.; Xu, H.; Qiu, H.; Zhu, L.; Yuan, M. Phytoestrogens and risk of prostate cancer: An updated meta-analysis of epidemiologic studies. Int. J. Food Sci. Nutr. 2017, 68, 28–42. [Google Scholar] [CrossRef]
- Bylund, A.; Lundin, E.; Zhang, J.-X.; Nordin, A.; Kaaks, R.; Stenman, U.; Åman, P.; Adlercreutz, H.; Nilsson, T.; Hallmans, G. Randomised controlled short-term intervention pilot study on rye bran bread in prostate cancer. Eur. J. Cancer Prev. 2003, 12, 407–415. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Polascik, T.J.; George, S.L.; Switzer, B.R.; Madden, J.F.; Ruffin, M.T.; Snyder, D.C.; Owzar, K.; Hars, V.; Albala, D.M. Flaxseed supplementation (not dietary fat restriction) reduces prostate cancer proliferation rates in men presurgery. Cancer Epidemiol. Prev. Biomark. 2008, 17, 3577–3587. [Google Scholar] [CrossRef] [Green Version]
- Dalais, F.S.; Meliala, A.; Wattanapenpaiboon, N.; Frydenberg, M.; Suter, D.A.; Thomson, W.K.; Wahlqvist, M.L. Effects of a diet rich in phytoestrogens on prostate-specific antigen and sex hormones in men diagnosed with prostate cancer. Urology 2004, 64, 510–515. [Google Scholar] [CrossRef]
- Kumar, N.B.; Cantor, A.; Allen, K.; Riccardi, D.; Besterman-Dahan, K.; Seigne, J.; Helal, M.; Salup, R.; Pow-Sang, J. The specific role of isoflavones in reducing prostate cancer risk. Prostate 2004, 59, 141–147. [Google Scholar] [CrossRef]
- Kumar, N.B.; Kang, L.; Pow-Sang, J.; Xu, P.; Allen, K.; Riccardi, D.; Besterman-Dahan, K.; Krischer, J.P. Results of a randomized phase I dose-finding trial of several doses of isoflavones in men with localized prostate cancer: Administration prior to radical prostatectomy. J. Soc. Integr. Oncol. 2010, 8, 3–13. [Google Scholar]
- Kumar, N.B.; Pow-Sang, J.; Spiess, P.; Dickinson, S.; Schell, M.J. A phase II randomized clinical trial using aglycone isoflavones to treat patients with localized prostate cancer in the pre-surgical period prior to radical prostatectomy. Oncotarget 2020, 11, 1218–1234. [Google Scholar] [CrossRef] [Green Version]
- Grammatikopoulou, M.G.; Gkiouras, K.; Papageorgiou, S.; Myrogiannis, I.; Mykoniatis, I.; Papamitsou, T.; Bogdanos, D.P.; Goulis, D.G. Dietary Factors and Supplements Influencing Prostate Specific-Antigen (PSA) Concentrations in Men with Prostate Cancer and Increased Cancer Risk: An Evidence Analysis Review Based on Randomized Controlled Trials. Nutrients 2020, 12, 2985. [Google Scholar] [CrossRef] [PubMed]
- Hedelin, M.; Bälter, K.A.; Chang, E.T.; Bellocco, R.; Klint, Å.; Johansson, J.E.; Wiklund, F.; Thellenberg-Karlsson, C.; Adami, H.O.; Grönberg, H. Dietary intake of phytoestrogens, estrogen receptor-beta polymorphisms and the risk of prostate cancer. Prostate 2006, 66, 1512–1520. [Google Scholar] [CrossRef] [PubMed]
- Ahlin, R.; Nybacka, S.; Josefsson, A.; Stranne, J.; Steineck, G.; Hedelin, M. The effect of a phytoestrogen intervention and impact of genetic factors on tumor proliferation markers among Swedish patients with prostate cancer: Study protocol for the randomized controlled PRODICA trial. Trials 2022, 23, 1041. [Google Scholar] [CrossRef] [PubMed]
- Swedish Food Agency. Find Your Way to Eat Greener Not Too Much and Be Active; Livsmedelsverket: Uppsala Lan, Sweden. Available online: https://www.livsmedelsverket.se/globalassets/publikationsdatabas/andra-sprak/kostraden/kostrad-eng.pdf (accessed on 26 March 2023).
- Hedelin, M.; Löf, M.; Andersson, T.M.; Adlercreutz, H.; Weiderpass, E. Dietary phytoestrogens and the risk of ovarian cancer in the women’s lifestyle and health cohort study. Cancer Epidemiol. Biomarkers Prev. 2011, 20, 308–317. [Google Scholar] [CrossRef] [Green Version]
- Chain, E.P.o.C.i.t.F.; Schrenk, D.; Bignami, M.; Bodin, L.; Chipman, J.K.; del Mazo, J.; Grasl-Kraupp, B.; Hogstrand, C.; Hoogenboom, L.; Leblanc, J.C. Evaluation of the health risks related to the presence of cyanogenic glycosides in foods other than raw apricot kernels. EFSA J. 2019, 17, e05662. [Google Scholar] [CrossRef] [Green Version]
- Nørskov, N.P.; Olsen, A.; Tjønneland, A.; Bolvig, A.K.; Lærke, H.N.; Knudsen, K.E. Targeted LC-MS/MS Method for the Quantitation of Plant Lignans and Enterolignans in Biofluids from Humans and Pigs. J. Agric. Food Chem. 2015, 63, 6283–6292. [Google Scholar] [CrossRef]
- Nørskov, N.P.; Givens, I.; Purup, S.; Stergiadis, S. Concentrations of phytoestrogens in conventional, organic and free-range retail milk in England. Food Chem. 2019, 295, 1–9. [Google Scholar] [CrossRef]
- National Library of Medicine. PubChem—Explore Chemistry. Available online: https://pubchem.ncbi.nlm.nih.gov/ (accessed on 23 March 2023).
- World Health Organization. Body Mass Index—BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 5 April 2023).
- Hamilton-Reeves, J.M.; Rebello, S.A.; Thomas, W.; Slaton, J.W.; Kurzer, M.S. Soy protein isolate increases urinary estrogens and the ratio of 2: 16 α-hydroxyestrone in men at high risk of prostate cancer. J. Nutr. 2007, 137, 2258–2263. [Google Scholar] [CrossRef] [Green Version]
- Muti, P.; Westerlind, K.; Wu, T.; Grimaldi, T.; De Berry, J., 3rd; Schünemann, H.; Freudenheim, J.L.; Hill, H.; Carruba, G.; Bradlow, L. Urinary estrogen metabolites and prostate cancer: A case-control study in the United States. Cancer Causes Control. 2002, 13, 947–955. [Google Scholar] [CrossRef]
- Lee, J.K.; Byun, S.S.; Lee, S.E.; Hong, S.K. Preoperative Serum Sex Hormone-Binding Globulin Level Is an Independent Predictor of Biochemical Outcome After Radical Prostatectomy. Medicine 2015, 94, e1185. [Google Scholar] [CrossRef]
- Kumar, N.B.; Krischer, J.P.; Allen, K.; Riccardi, D.; Besterman-Dahan, K.; Salup, R.; Kang, L.; Xu, P.; Pow-Sang, J. A Phase II randomized, placebo-controlled clinical trial of purified isoflavones in modulating steroid hormones in men diagnosed with localized prostate cancer. Nutr. Cancer 2007, 59, 163–168. [Google Scholar] [CrossRef]
- Lampe, J.W.; Karr, S.C.; Hutchins, A.M.; Slavin, J.L. Urinary equol excretion with a soy challenge: Influence of habitual diet. Proc. Soc. Exp. Biol. Med. 1998, 217, 335–339. [Google Scholar] [CrossRef]
- Rowland, I.R.; Wiseman, H.; Sanders, T.A.; Adlercreutz, H.; Bowey, E.A. Interindividual variation in metabolism of soy isoflavones and lignans: Influence of habitual diet on equol production by the gut microflora. Nutr. Cancer 2000, 36, 27–32. [Google Scholar] [CrossRef]
- Akaza, H.; Miyanaga, N.; Takashima, N.; Naito, S.; Hirao, Y.; Tsukamoto, T.; Fujioka, T.; Mori, M.; Kim, W.J.; Song, J.M.; et al. Comparisons of percent equol producers between prostate cancer patients and controls: Case-controlled studies of isoflavones in Japanese, Korean and American residents. Jpn. J. Clin. Oncol. 2004, 34, 86–89. [Google Scholar] [CrossRef] [Green Version]
- Kuijsten, A.; Arts, I.C.; van’t Veer, P.; Hollman, P.C. The relative bioavailability of enterolignans in humans is enhanced by milling and crushing of flaxseed. J. Nutr. 2005, 135, 2812–2816. [Google Scholar] [CrossRef] [Green Version]
- Bolvig, A.K.; Nørskov, N.P.; van Vliet, S.; Foldager, L.; Curtasu, M.V.; Hedemann, M.S.; Sørensen, J.F.; Lærke, H.N.; Bach Knudsen, K.E. Rye Bran Modified with Cell Wall-Degrading Enzymes Influences the Kinetics of Plant Lignans but Not of Enterolignans in Multicatheterized Pigs. J. Nutr. 2017, 147, 2220–2227. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, S.; Yamaguchi, M.; Sobue, T.; Takahashi, T.; Miura, T.; Arai, Y.; Mazur, W.; Wähälä, K.; Adlercreutz, H. Pharmacokinetics of soybean isoflavones in plasma, urine and feces of men after ingestion of 60 g baked soybean powder (kinako). J. Nutr. 1998, 128, 1710–1715. [Google Scholar] [CrossRef] [Green Version]
- Cani, P.D. Human gut microbiome: Hopes, threats and promises. Gut 2018, 67, 1716–1725. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention (n = 68) | Control (n = 67) | |||||||
|---|---|---|---|---|---|---|---|---|
| Genotype TT 2 (n = 35) | Genotype TC/CC 2 (n = 33) | Genotype TT 2 (n = 26) | Genotype TC/CC 2 (n = 41) | |||||
| Median (IQR) | Range | Median (IQR) | Range | Median (IQR) | Range | Median (IQR) | Range | |
| Age, years | 65 (13) | 51–76 | 67 (8) | 43–76 | 66 (10) | 51–74 | 65 (10) | 40–75 |
| Intervention period, d | 47 (46) | 12–189 | 48 (28) | 7–146 | 46 (27) | 8–213 | 47 (29) | 14–583 |
| BMI, kg/m2 | 27.8 (5.2) | 21.7–37.4 | 28.1 (4.7) | 21.3–35.1 | 26.0 (3.9) | 20.0–40.0 | 25.5 (3.8) | 20.6–33.3 |
| n(%) | n(%) | n(%) | n(%) | |||||
| Tumor stage at diagnosis | ||||||||
| cT1 | 20 (57) | 20 (61) | 14 (54) | 31 (76) | ||||
| cT2 | 15 (43) | 12 (36) | 10 (38) | 10 (24) | ||||
| cTX | 0 (0) | 1 (3) | 2 (8) | 0 (0) | ||||
| ISUP grade at diagnosis | ||||||||
| 1 | 11 (31) | 14 (42) | 10 (38) | 19 (46) | ||||
| 2 | 19 (54) | 15 (45) | 11 (42) | 19 (46) | ||||
| 3 | 5 (14) | 4 (12) | 5 (19) | 3 (7) | ||||
| Physical activity 3 | ||||||||
| Low | 6 (17) | 8 (24) | 2 (8) | 4 (10) | ||||
| Moderate | 19 (54) | 16 (48) | 17 (65) | 19 (46) | ||||
| High | 10 (29) | 9 (27) | 7 (27) | 18 (44) | ||||
| Heredity | ||||||||
| Yes | 13 (37) | 12 (36) | 7 (27) | 14 (34) | ||||
| No | 9 (26) | 10 (30) | 4 (15) | 14 (34) | ||||
| Do not know | 13 (37) | 11 (33) | 15 (58) | 13 (32) | ||||
| Antibiotic treatment last year | ||||||||
| Yes | 12 (34) | 7 (21) | 11 (42) | 11 (27) | ||||
| No | 22 (63) | 25 (76) | 15 (58) | 29 (71) | ||||
| Do not know | 1 (3) | 1 (3) | 0 (0) | 1 (2) | ||||
| Antibiotic treatment last 2–5 years | ||||||||
| Yes | 14 (40) | 10 (30) | 13 (50) | 22 (54) | ||||
| No | 19 (54) | 17 (52) | 12 (46) | 14 (34) | ||||
| Do not know | 2 (6) | 6 (18) | 1 (4) | 5 (12) | ||||
| Antibiotic treatment during the intervention, n (%) | ||||||||
| Yes | 1 (3) | 3 (9) | 3 (12) | 4 (10) | ||||
| No | 34 (97) | 30 (91) | 23 (88) | 36 (88) | ||||
| Missing, n (%) | 0 (0) | 0 (0) | 0 (0) | 1 (2) | ||||
| Smoking | ||||||||
| Currently | 2 (6) | 1 (3) | 1 (4) | 2 (5) | ||||
| Previously | 16 (46) | 17 (52) | 12 (46) | 21 (51) | ||||
| Never | 17 (49) | 15 (45) | 13 (50) | 18 (44) | ||||
| Intervention (n = 68) | Control (n = 67) | p 1 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Genotype TT 2 (n = 35) | Genotype TC/CC 2 (n = 33) | Genotype TT 2 (n = 26) | Genotype TC/CC 2 (n = 41) | TT | TC/CC | |||||||
| Median (IQR) | Range | Median (IQR) | Range | p 3 | Median (IQR) | Range | Median (IQR) | Range | p 3 | |||
| Testosterone (nmol/L) | ||||||||||||
| Baseline | 15.3 (6.6) | 9.6–30.1 | 15.0 (6.4) | 5.1–26.2 | 0.710 5 | 15.6 (6.3) | 8.0–22.7 | 14.9 (7.5) | 8.4–32.6 | 0.889 | 0.521 5 | 0.699 5 |
| Endpoint | 14.8 (4.9) | 6.9–22.6 | 14.2 (6.4) | 5.1–30.0 | 0.566 5 | 14.4 (6.7) | 7.3–26.0 | 15.8 (8.8) | 5.4–30.5 | 0.331 5 | 0.483 5 | 0.362 5 |
| Change 4 | −0.5 (3.7) | −10.1–13.0 | 0.2 (4.8) | −9.0–9.0 | 0.854 5 | −0.8 (2.0) | −8.1–9.6 | −0.6 (3.8) | −7.7–18.3 | 0.648 | 0.814 | 0.865 |
| Estradiol (nmol/L) | ||||||||||||
| Baseline | 0.099 (0.034) | 0.069–0.18 | 0.10 (0.029) | 0.040–0.18 | 0.273 | 0.090 (0.040) | 0.049–0.15 | 0.092 (0.040) | 0.030–0.32 | 0.500 | 0.0137 5 | 0.546 |
| Endpoint | 0.10 (0.048) | 0.045–0.18 | 0.10 (0.034) | 0.048–0.16 | 0.9735 | 0.088 (0.035) | 0.023–0.15 | 0.10 (0.061) | 0.033–0.35 | 0.149 | 0.0625 5 | 0.727 |
| Change 4 | −0.0050 (0.027) | −0.050–0.055 | 0.0 (0.026) | −0.038–0.048 | 0.0725 | −0.0015 (0.027) | −0.026–0.034 | 0.0050 (0.032) | −0.046–0.089 | 0.159 | 0.679 5 | 0.657 5 |
| SHBG (nmol/L) | ||||||||||||
| Baseline | 49.0 (25.0) | 28.0–114.0 | 45.0 (25.0) | 21.0–110.0 | 0.640 | 50.0 (22.0) | 19.0–94.0 | 48.0 (32.0) | 22.0–126.0 | 0.947 | 0.848 | 0.744 |
| Endpoint | 51.0 (22.0) | 28.0–113.0 | 41.0 (22.0) | 20.0–96.0 | 0.0982 | 50.5 (29.0) | 24.0–96.0 | 51.0 (33.0) | 20.0–112.0 | 0.797 | 0.980 | 0.273 |
| Change 4 | 1.0 (8.0) | −25.0–16.0 | −2.0 (10.0) | −29.0–13.0 | 0.00390 | 0.0 (6.0) | −12.0–21.0 | −2.0 (8.0) | −20.0–25.0 | 0.189 | 0.502 | 0.418 |
| IGF−1 (µg/L) | ||||||||||||
| Baseline | 126.0 (62.0) | 75.0–280.0 | 138.0 (56.0) | 60.0–276.0 | 0.915 | 166.5 (44.0) | 90.0–274.0 | 146.0 (64.0) | 68.0–381.0 | 0.173 | 0.0973 | 0.536 |
| Endpoint | 135.0 (57.0) | 82.0–304.0 | 151.0 (64.0) | 59.0–266.0 | 0.819 | 161.0 (81.0) | 90.0–253.0 | 153.0 (85.0) | 63.0–340.0 | 0.864 | 0.301 | 0.499 5 |
| Change 4 | −1.0 (18.0) | −25.0–124.0 | 7.0 (23.0) | −66.0–41.0 | 0.281 | −0.5 (26.0) | −65.0–54.0 | 7.0 (31.0) | −45.0–55.0 | 0.232 | 0.656 | 0.955 5 |
| Testosterone/SHBG ratio | ||||||||||||
| Baseline | 0.33 (0.10) | 0.14–0.55 | 0.32 (0.080) | 0.16–0.49 | 0.826 5 | 0.30 (0.099) | 0.18–0.67 | 0.32 (0.12) | 0.17–0.56 | 0.426 | 0.319 | 0.828 5 |
| Endpoint | 0.30 (0.12) | 0.17–0.58 | 0.33 (0.12) | 0.19–0.59 | 0.215 5 | 0.28 (0.11) | 0.17–0.47 | 0.32 (0.12) | 0.17–0.60 | 0.0705 | 0.380 | 0.773 |
| Change 4 | 0.011 (0.090) | −0.19–0.17 | −0.0023 (0.088) | −0.12–0.094 | 0.0734 5 | 0.012 (0.068) | −0.092–0.26 | 0.00043 (0.067) | −0.29–0.12 | 0.145 | 0.789 | 0.462 |
| Testosterone/estradiol ratio | ||||||||||||
| Baseline | 134.9 (37.4) | 0.09–311.1 | 140.5 (77.8) | 0.09–348.5 | 0.637 | 166.1 (75.6) | 0.1–346.2 | 155.0 (12.6) | 0.09–380.0 | 0.280 | 0.0697 | 0.854 |
| Endpoint | 149.3 (69.9) | 0.1–322.2 | 140.4 (84.0) | 0.083–321.7 | 0.678 | 164.1 (102.1) | 0.1–487.0 | 138.8 (127.1) | 0.09–356.4 | 0.242 | 0.107 | 0.681 |
| Change 4 | 0.07 (46.4) | −70.1–68.9 | −6.4 (40.7) | −95.0–54.6 | 0.127 5 | −5.2 (48.4) | −106.3–225.7 | −2.8 (26.1) | −116.4–108.3 | 0.934 | 0.438 | 0.417 |
| Hormone Concentrations (nmol/L) | RD | 95% CI | Adjusted 1 RD | Adjusted 1 95% CI | p Additive Interaction | |
|---|---|---|---|---|---|---|
| Testosterone | All cases (n = 135) | 0.083 | −0.84, 0.25 | 0.067 | −0.10, 0.23 | 0.792 |
| TT (n = 61) | 0.12 | −0.12, 0.36 | 0.099 | −0.14, 0.34 | ||
| TC/CC (n = 74) | 0.076 | −0.15, 0.30 | 0.073 | −0.16, 0.31 | ||
| Estradiol | All cases (n = 135) | −0.11 | −0.28, 0.057 | −0.13 | −0.30, 0.045 | 0.424 |
| TT (n = 61) | −0.013 | −0.26, 0.23 | −0.027 | −0.27, 0.22 | ||
| TC/CC (n = 74) | −0.15 | −0.37, 0.076 | −0.22 | −0.45, 0.071 | ||
| SHBG | All cases (n = 135) | 0.038 | −0.13, 0.20 | 0.030 | −0.14, 0.20 | 0.149 |
| TT (n = 61) | 0.15 | −0.10, 0.40 | 0.13 | −0.12, 0.37 | ||
| TC/CC (n = 74) | −0.093 | −0.30, 0.12 | −0.11 | −0.33, 0.011 | ||
| IGF-1 | All cases (n = 135) | −0.038 | −0.21, 0.13 | −0.028 | −0.20, 0.14 | 0.386 |
| TT (n = 61) | −0.090 | −0.34, 0.16 | −0.076 | −0.31, 0.15 | ||
| TC/CC (n = 74) | 0.057 | −0.16, 0.28 | 0.068 | −0.16, 0.30 | ||
| Testosterone/SHBG ratio | All cases (n = 135) | 0.0061 | −0.16, 0.17 | 0.027 | −0.14, 0.20 | 0.632 |
| TT (n = 61) | 0.022 | −0.21, 0.25 | 0.028 | −0.20, 0.25 | ||
| TC/CC (n = 74) | −0.058 | −0.29, 0.17 | −0.083 | −0.31, 0.15 | ||
| Testosterone/estradiol ratio | All cases (n = 135) | 0.097 | −0.068, 0.26 | 0.081 | −0.090, 0.25 | 0.458 |
| TT (n = 61) | 0.15 | −0.10, 0.40 | 0.13 | −0.12, 0.39 | ||
| TC/CC (n = 74) | 0.022 | −0.20, 0.24 | −0.0050 2 0.0011 3 0.024 4 | −0.21, 0.22 2 −0.21, 0.21 3 −0.21, 0.25 4 |
| Intervention (n = 51) | Control (n = 54) | p 1 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Genotype TT 2 (n = 26) | Genotype TC/CC 2 (n = 25) | Genotype TT 2 (n = 24) | Genotype TC/CC 2 (n = 30) | TT | TC/CC | |||||||
| Plasma Concentrations (nmol/L) | Median (IQR) | Range | Median (IQR) | Range | p 3 | Median (IQR) | Range | Median (IQR) | Range | p 3 | ||
| Lariciresinol | ||||||||||||
| Baseline | 4.9 (4.1) | 1.8–17.0 | 5.2 (4.2) | 1.7–20.6 | 0.797 | 5.9 (2.5) | 3.1–12.2 | 5.7 (6.5) | 2.0–17.9 | 0.833 | 0.718 | 0.654 |
| Endpoint | 6.5 (4.9) | 2.6–12.0 | 6.0 (6.0) | 2.4–16.4 | 0.374 | 6.1 (5.5) | 1.2–18.4 | 4.6 (4.9) | 0.0–15.6 | 0.419 | 0.473 | 0.463 |
| Change 4 | 1.9 (5.8) | −11.0–8.5 | −0.02 (4.3) | −10.4–7.1 | 0.449 | 0.02 (5.8) | −6.7–11.8 | −1.3 (5.1) | −12.4–5.3 | 0.138 | 0.481 | 0.164 |
| Secoisolariciresinol | ||||||||||||
| Baseline | 6.5 (7.1) | 0.8–26.7 | 5.7 (5.5) | 0.6–103.1 | 0.664 | 6.0 (8.6) | 1.5–61.1 | 6.2 (6.9) | 1.8–31.0 | 0.883 | 0.859 | 0.507 |
| Endpoint | 13.9 (17.9) | 2.2–80.8 | 10.4 (9.9) | 1.2–108.3 | 0.275 | 5.5 (11.0) | 1.8–29.6 | 4.8 (4.5) | 0.9–41.6 | 0.766 | 0.0094 | 0.0314 |
| Change 4 | 5.0 (21.4) | −17.2–78.5 | 4.2 (11.1) | −90.3–98.5 | 0.647 | 0.08 (6.5) | −50.1–26.8 | −0.8 (5.2) | −25.4–18.9 | 0.506 | 0.0068 | 0.0045 |
| Enterodiol | ||||||||||||
| Baseline | 7.0 (10.2) | 0.8–122.0 | 5.7 (15.1) | 0.6–584.5 | 0.507 | 7.7 (23.0) | 1.2–175.0 | 4.5 (6.9) | 0.4–81.9 | 0.0932 | 0.683 | 0.694 |
| Endpoint | 25.5 (37.5) | 4.3–880.3 | 32.0 (122.4) | 1.2–1526.1 | 0.604 | 8.8 (11.6) | 0.5–691.3 | 4.5 (9.4) | 0.2–82.6 | 0.244 | <0.001 | <0.001 |
| Change 3 | 11.7 (32.6) | −87.9–876.8 | 17.1 (92.3) | −330.8–1501.2 | 0.395 | −1.6 (14.6) | −114.1–683.5 | −0.2 (5.7) | −52.0–77.4 | 0.264 | 0.0014 | 0.0014 |
| Enterolactone | ||||||||||||
| Baseline | 113.6 (123.0) | 10.7–348.7 | 71.2 (107.5) | 5.2–321.8 | 0.207 | 107.4 (144.3) | 8.6–517.7 | 66.0 (69.0) | 8.4–393.7 | 0.115 | 0.981 | 0.923 |
| Endpoint | 213.0 (404.8) | 0.8–1348.2 | 175.4 (371.7) | 5.3–1172.1 | 0.344 | 78.8 (123.6) | 4.5–578.8 | 78.1 (91.0) | 15.8–231.9 | 0.572 | <0.001 | 0.0048 |
| Change 4 | 109.1 (364.4) | −218.2–1264.5 | 109.1 (270.7) | −215.0–1052.0 | 0.993 | −29.2 (92.9) | −168.3–446.0 | −22.2 (61.9) | −213.9–203.8 | 0.714 | 0.0013 | <0.001 |
| Daidzein | ||||||||||||
| Baseline | 40.3 (112.1) | 0.0–477.8 | 32.4 (53.0) | 0.0–1257.5 | 0.426 | 16.4 (46.7) | 0.0–349.0 | 33.3 (94.7) | 0.0–453.0 | 0.776 | 0.372 | 0.792 |
| Endpoint | 579.2 (796.6) | 0.0–2096.7 | 250.0 (819.4) | 0.0–3688.4 | 0.384 | 10.2 (23.4) | 0.0–153.0 | 32.3 (38.3) | 0.0–157.7 | 0.124 | <0.001 | <0.001 |
| Change 4 | 499.1 (790.5) | −205.0–2093.2 | 132.3 (680.6) | −89.1–3655.4 | 0.472 | −7.6 (33.5) | −308.9–135.7 | −3.2 (66.9) | −365.9–142.5 | 0.554 | <0.001 | <0.001 |
| Genistein | ||||||||||||
| Baseline | 147.5 (325.1) | 0.0–8798.1 | 68.1 (163.4) | 0.0–2378.8 | 0.486 | 34.3 (150.6) | 0.0–2335.0 | 43.8 (157.1) | 0.0–2091.8 | 0.675 | 0.290 | 0.782 |
| Endpoint | 1055.5 (3141.7) | 4.4–8075.1 | 474.9 (1378.7) | 10.3–13,070.3 | 0.129 | 18.5 (127.4) | 0.0–667.7 | 29.3 (79.9) | 0.0–621.7 | 0.382 | <0.001 | <0.001 |
| Change 4 | 668.6 (3003.5) | −5060.9–8041.4 | 421.7 (692.8) | −322.1–12,911.8 | 0.438 | −13.6 (144.4) | −1667.3–201.1 | −14.2 (86.5) | −1470.1–438.2 | 0.982 | <0.001 | <0.001 |
| Glycitein | ||||||||||||
| Baseline | 0.0 (4.4) | 0.0–29.2 | 0.0 (3.4) | 0.0–174.3 | 0.853 | 0.0 (3.3) | 0.0–29.6 | 0.0 (4.4) | 0.0–40.0 | 0.905 | 0.834 | 0.678 |
| Endpoint | 20.9 (43.3) | 0.0–87.9 | 14.4 (42.7) | 0.0–287.4 | 0.406 | 0.0 (0.0) | 0.0–6.1 | 0.0 (2.2) | 0.0–13.2 | 0.130 | <0.001 | <0.001 |
| Change 4 | 17.3 (47.5) | −10.9–83.7 | 14.4 (40.0) | −5.0–287.4 | 0.604 | 0.0 (3.3) | −25.0–3.5 | 0.0 (4.1) | −40.0–13.2 | 0.816 | <0.001 | <0.001 |
| Equol | ||||||||||||
| Baseline | 0.0 (0.0) | 0.0–0.0 | 0.0 (0.0) | 0.0–0.0 | 1.000 | 0.0 (0.0) | 0.0–0.0 | 0.0 (0.0) | 0.0–0.0 | 1.000 | 1.000 | 1.000 |
| Endpoint | 0.0 (0.0) | 0.0–1204.9 | 0.0 (0.0) | 0.0–616.1 | 0.404 | 0.0 (0.0) | 0.0–0.0 | 0.0 (0.0) | 0.0–289.0 | 1.000 | 0.0290 | 0.0742 |
| Change 4 | 0.0 (0.0) | 0.0–1204.9 | 0.0 (0.0) | 0.0–616.1 | 0.404 | 0.0 (0.0) | 0.0–0.0 | 0.0 (0.0) | 0.0–289.0 | 1.000 | 0.0290 | 0.0742 |
| Hormone Concentrations (nmol/L) | Plasma Concentrations of Lignans 1 (nmol/L) β (95% CI) | Plasma Concentrations of Isoflavones 2 (nmol/L) β (95% CI) | Plasma Concentrations of Phytoestrogens 3 (nmol/L) β (95% CI) | |
|---|---|---|---|---|
| Testosterone | Unadjusted | 0.035 (−0.028, 0.099) | 0.0071 (−0.024, 0.039) 4 | 0.013 (−0.034, 0.059) |
| Adjusted 5 | 0.029 (−0.034, 0.092) | 0.0099 (−0.021, 0.041) 4 | 0.014 (−0.031, 0.059) | |
| Estradiol | Unadjusted | 0.019 (−0.051, 0.089) | −0.012 (−0.046, 0.022) 4 | −0.013 (−0.064, 0.037) |
| Adjusted 5 | 0.026 (−0.044, 0.097) | −0.015 (−0.050, 0.019) 4 | −0.014 (−0.65, 0.036) | |
| SHBG | Unadjusted | 0.071 (0.0013, 0.14) | −0.0090 (−0.044, 0.026) 4 | 0.011 (−0.040, 0.062) |
| Adjusted 5 | 0.055 (−0.013, 0.12) | −0.0048 (−0.038, 0.029) 4 | 0.010 (−0.039, 0.059) | |
| IGF-1 | Unadjusted | 0.0065 (−0.049, 0.062) | 0.012 (−0.015, 0.038) 4 | 0.0085 (−0.031, 0.048) |
| Adjusted 5 | 0.015 (−0.041, 0.071) | 0.0095 (−0.017, 0.036) 4 | 0.0093 (−0.031, 0.049) | |
| Testosterone/SHBG ratio | Unadjusted | −0.036 (−0.85, 0.014) | 0.016 (−0.0082, 0.040) 4 | 0.0017 (−0.034, 0.038) |
| Adjusted 5 | −0.026 (−0.075, 0.023) | 0.015 (−0.0093, 0.039) 4 | 0.0038 (−0.031, 0.039) | |
| Testosterone/estradiol ratio | Unadjusted | 0.016 (−0.057, 0.089) | 0.019 (−0.016, 0.055) 4 | 0.026 (−0.026, 0.078) |
| Adjusted 5 | 0.0031 (−0.064, 0.070) | 0.025 (−0.0071, 0.058) 4 | 0.028 (−0.019, 0.076) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahlin, R.; Nørskov, N.P.; Nybacka, S.; Landberg, R.; Skokic, V.; Stranne, J.; Josefsson, A.; Steineck, G.; Hedelin, M. Effects on Serum Hormone Concentrations after a Dietary Phytoestrogen Intervention in Patients with Prostate Cancer: A Randomized Controlled Trial. Nutrients 2023, 15, 1792. https://doi.org/10.3390/nu15071792
Ahlin R, Nørskov NP, Nybacka S, Landberg R, Skokic V, Stranne J, Josefsson A, Steineck G, Hedelin M. Effects on Serum Hormone Concentrations after a Dietary Phytoestrogen Intervention in Patients with Prostate Cancer: A Randomized Controlled Trial. Nutrients. 2023; 15(7):1792. https://doi.org/10.3390/nu15071792
Chicago/Turabian StyleAhlin, Rebecca, Natalja P. Nørskov, Sanna Nybacka, Rikard Landberg, Viktor Skokic, Johan Stranne, Andreas Josefsson, Gunnar Steineck, and Maria Hedelin. 2023. "Effects on Serum Hormone Concentrations after a Dietary Phytoestrogen Intervention in Patients with Prostate Cancer: A Randomized Controlled Trial" Nutrients 15, no. 7: 1792. https://doi.org/10.3390/nu15071792