
Phase Angle, Handgrip Strength, and Other Indicators of Nutritional Status in Cancer Patients Undergoing Different Nutritional Strategies: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
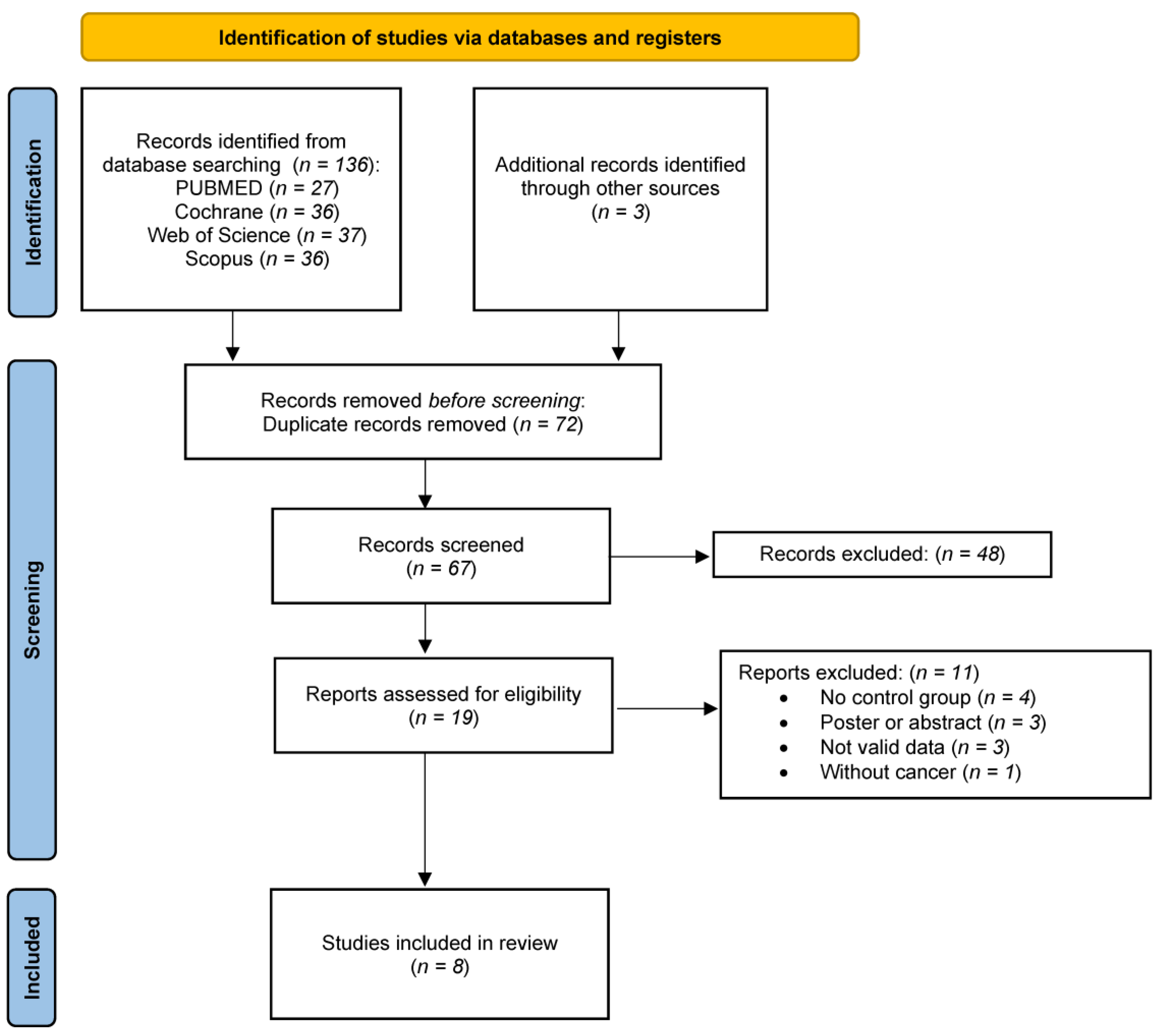
2.1. The Literature Search
2.2. Eligibility Criteria
2.3. Information Sources and Search Strategy
2.4. Selection Process
2.5. Data Items
2.6. Quality Assessment
2.7. Synthesis Methods
3. Results
3.1. Study Characteristics
3.2. Nutritional Intervention
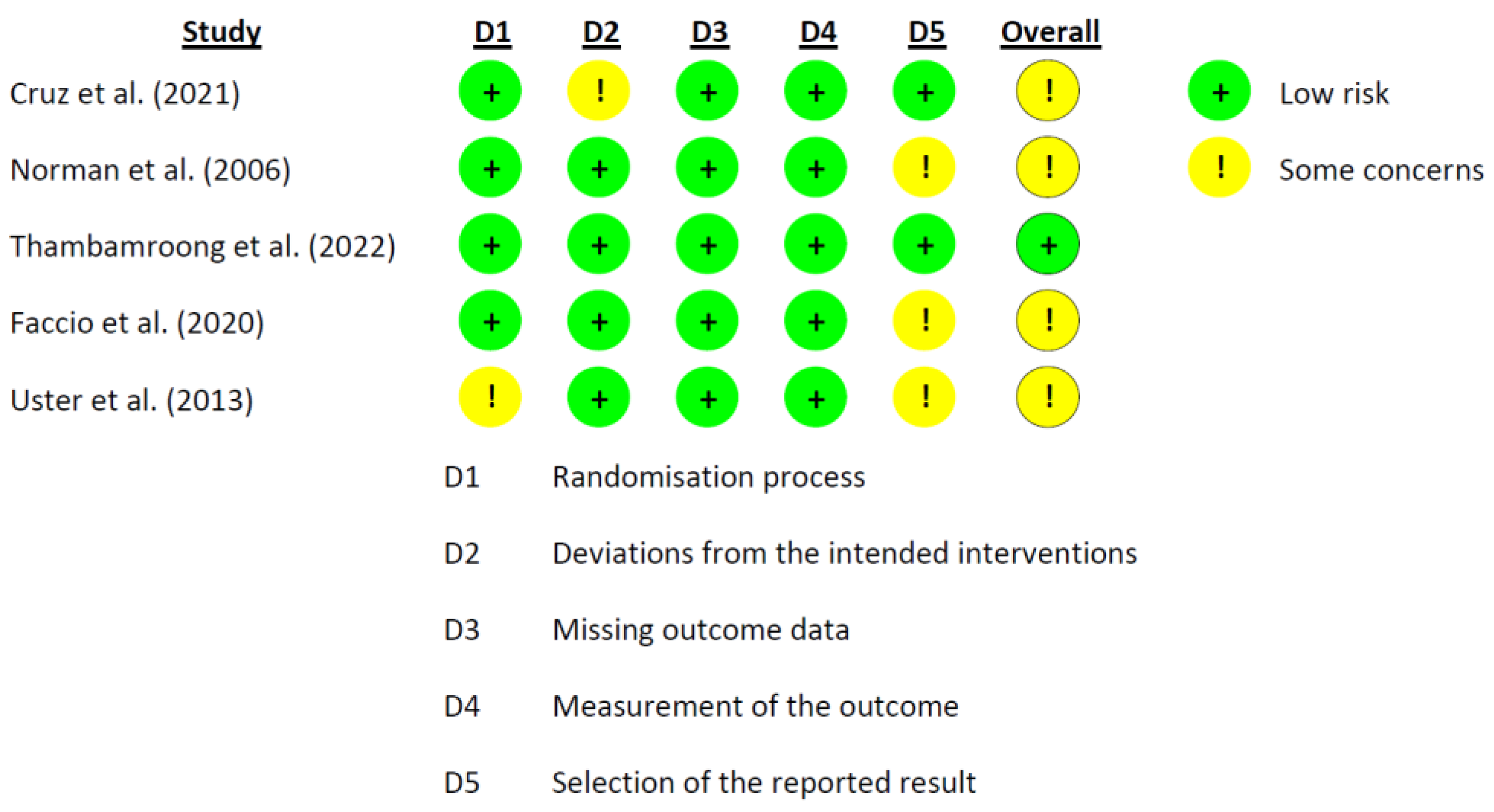
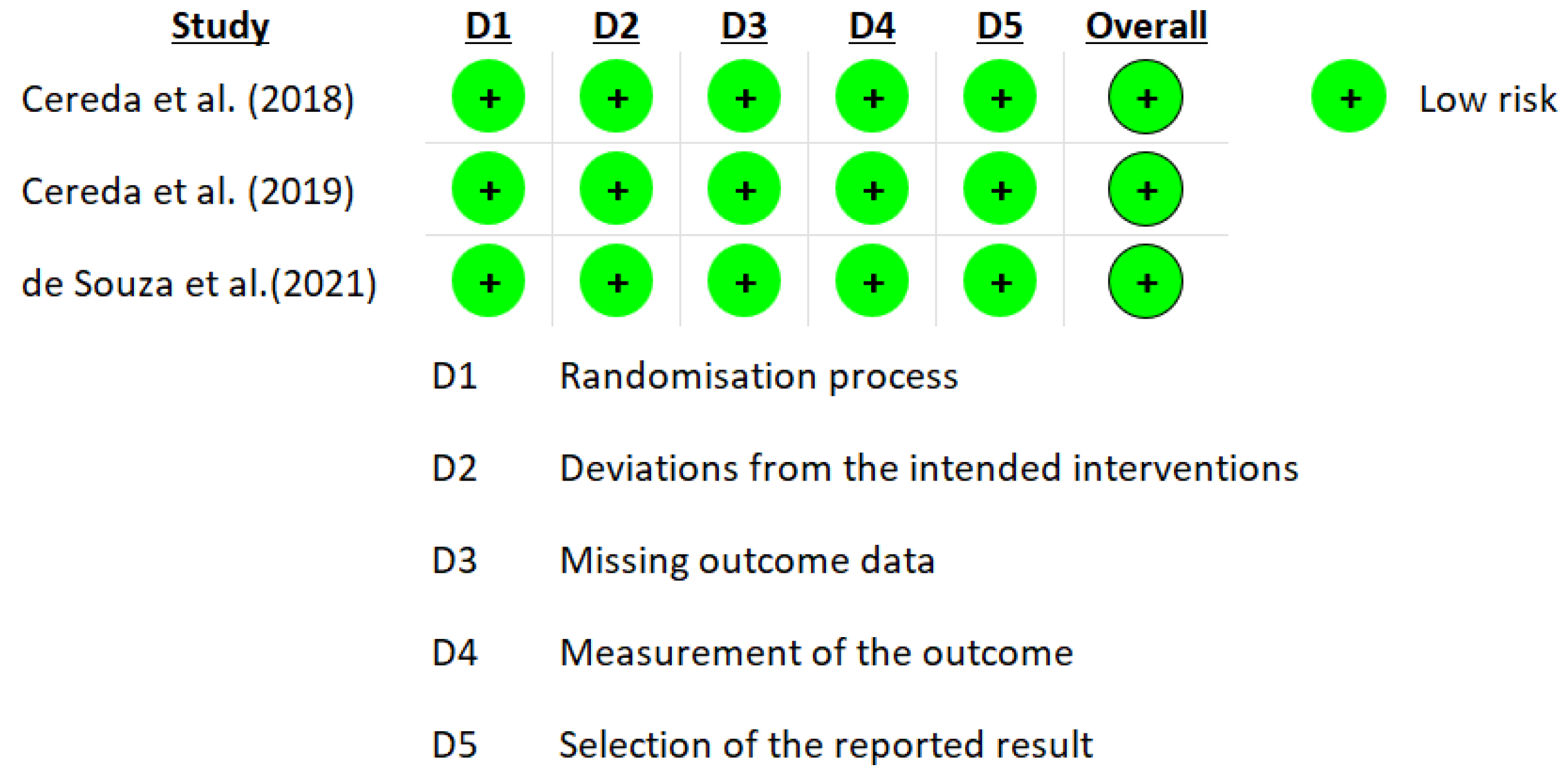
3.3. Risk of Study Bias
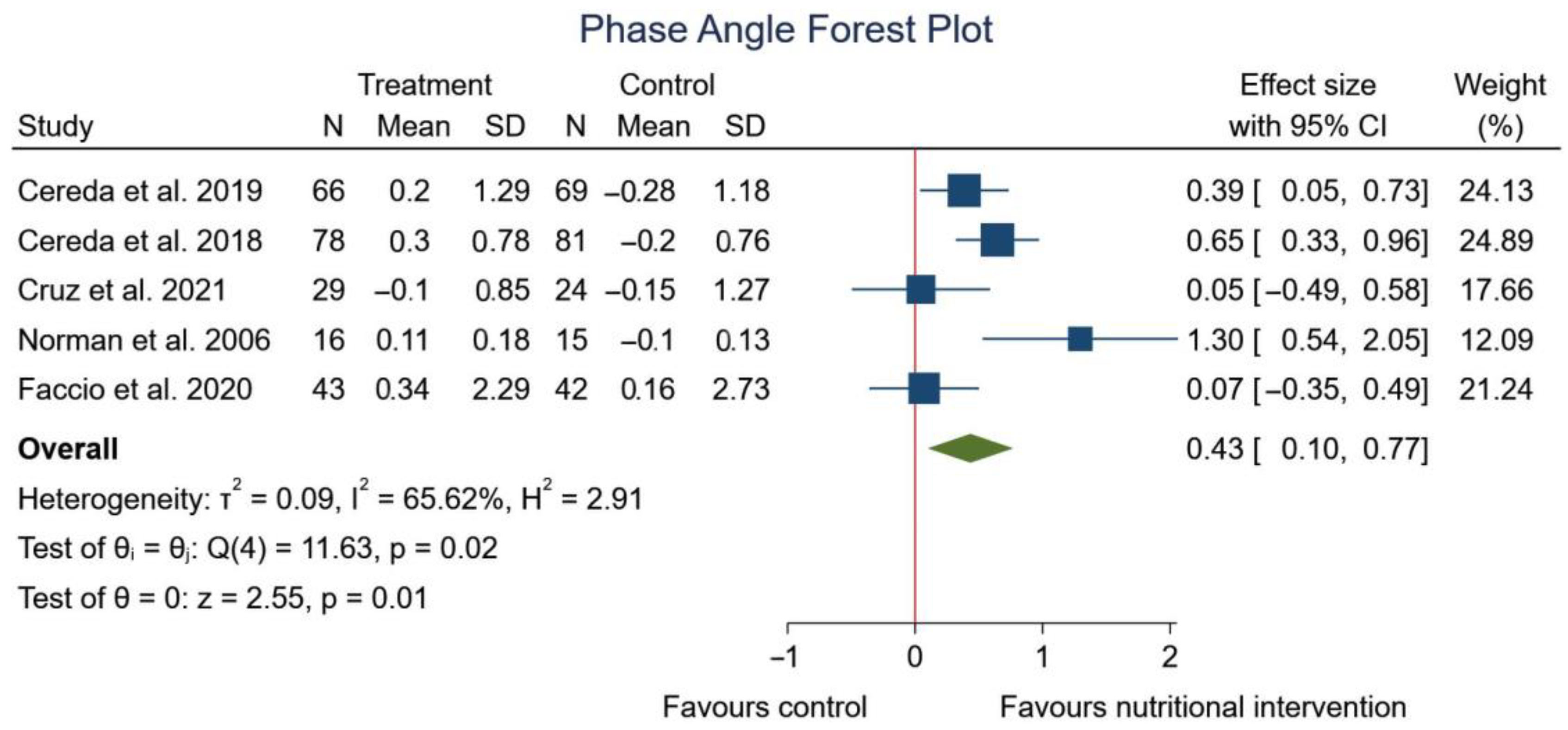
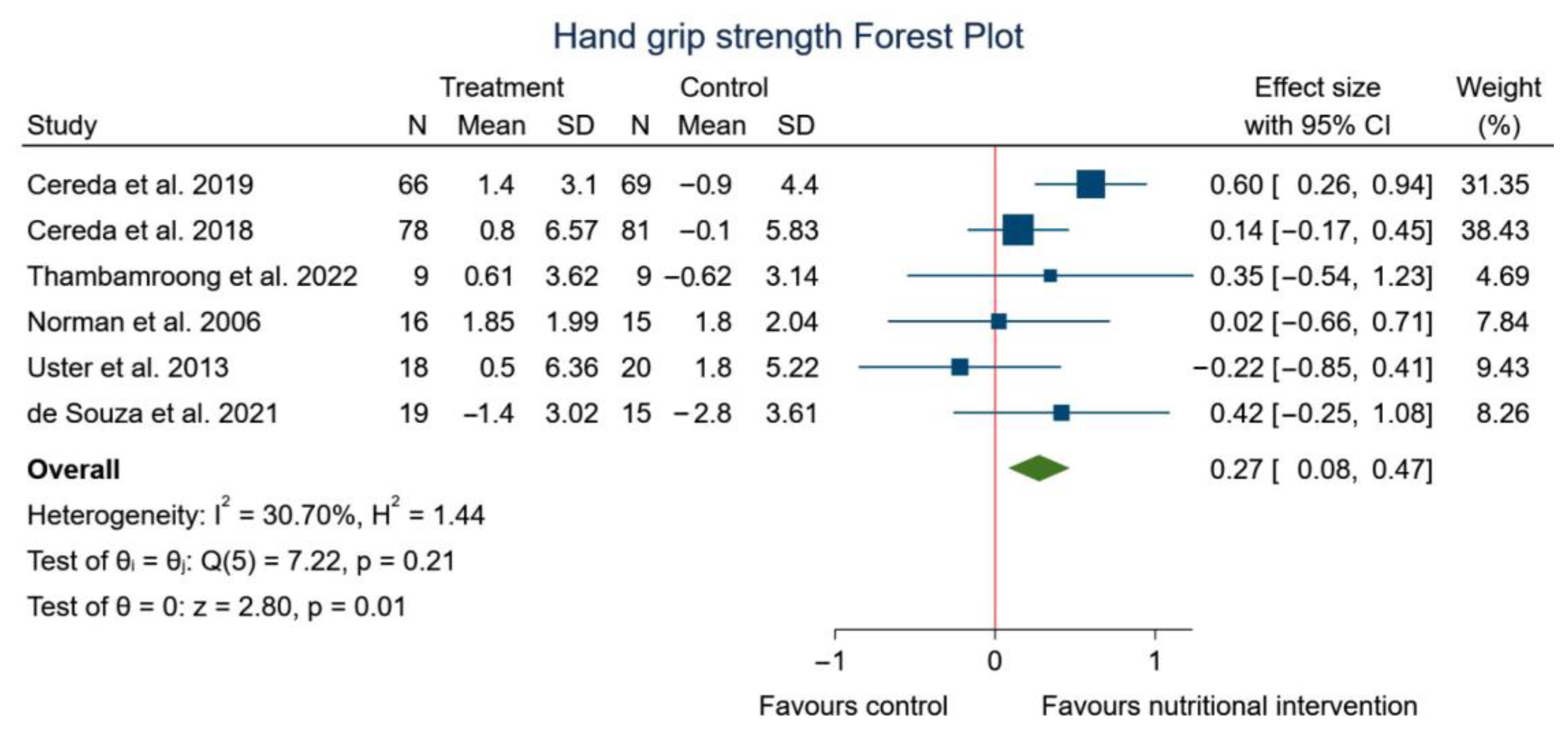
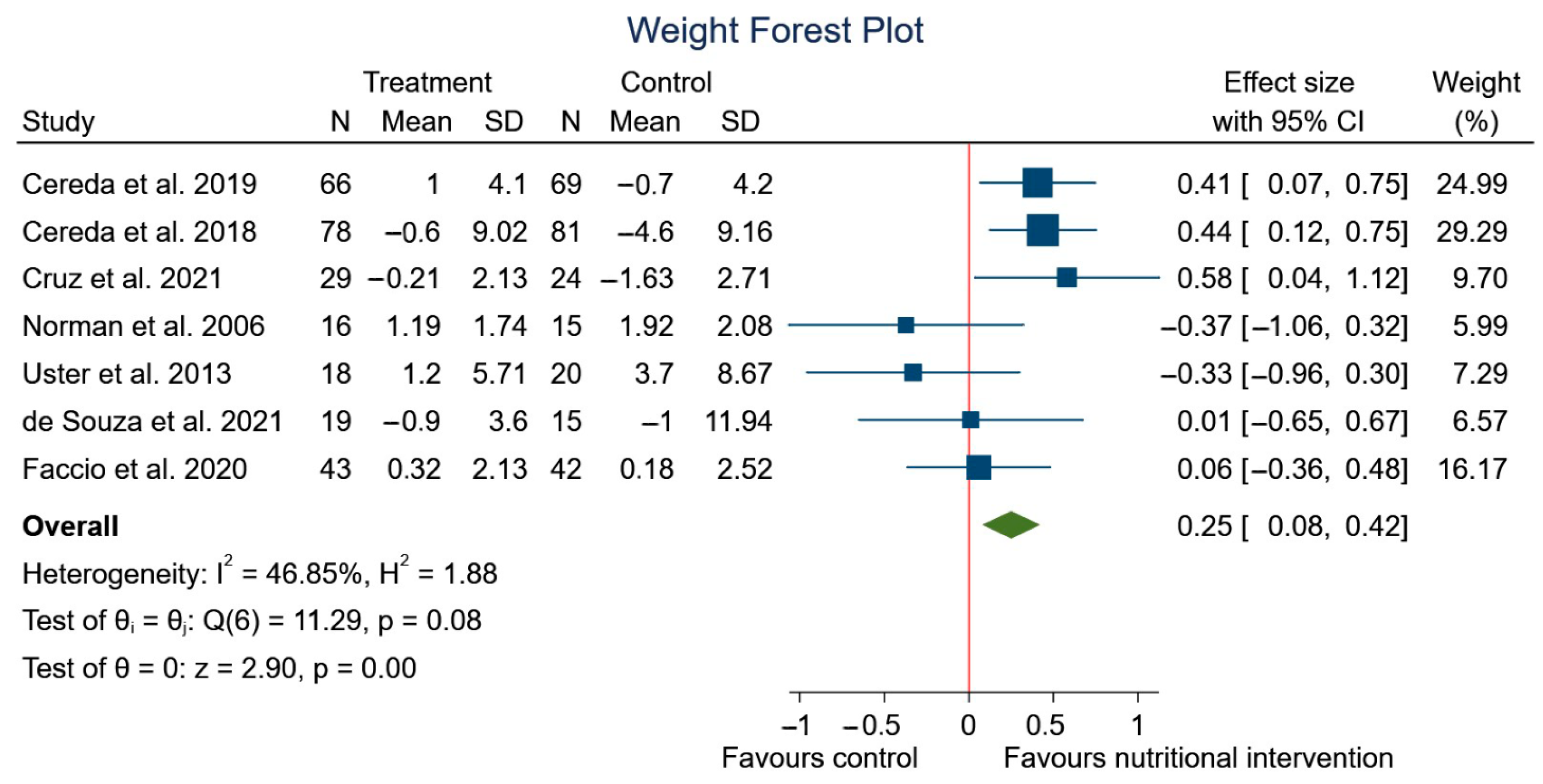
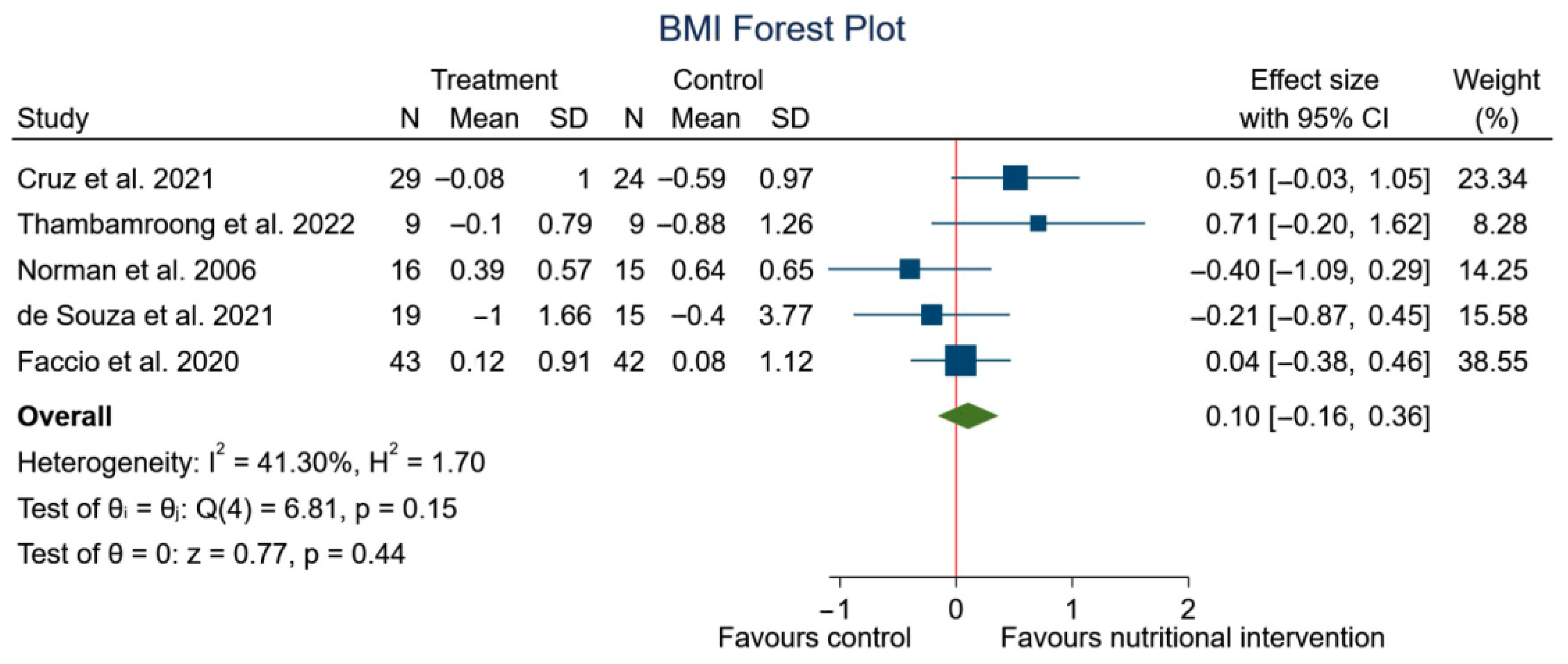
3.4. Findings from Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Institutes of Health (US); Biological Sciences Curriculum Study. NIH Curriculum Supplement Series [Internet]; Understanding Cancer; National Institutes of Health (US): Bethesda, MD, USA, 2007. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Brigden, M.; McKenzie, M. Treating Cancer Patients. Practical Monitoring and Management of Therapy-Related Complications. Can. Fam. Physician 2000, 46, 2258–2268. [Google Scholar] [PubMed]
- Beirer, A. Malnutrition and Cancer, Diagnosis and Treatment. MEMO Mag. Eur. Med. Oncol. 2021, 14, 168–173. [Google Scholar] [CrossRef]
- Benoist, S.; Brouquet, A. Nutritional Assessment and Screening for Malnutrition. J. Visc. Surg. 2015, 152, S3–S7. [Google Scholar] [CrossRef]
- Detopoulou, P.; Voulgaridou, G.; Papadopoulou, S. Cancer, Phase Angle and Sarcopenia: The Role of Diet in Connection with Lung Cancer Prognosis. Lung 2022, 200, 347–379. [Google Scholar] [CrossRef]
- Prado, C.M.; Purcell, S.A.; Laviano, A. Nutrition Interventions to Treat Low Muscle Mass in Cancer. J. Cachexia Sarcopenia Muscle 2020, 11, 366–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN Guidelines on Nutrition in Cancer Patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [Green Version]
- Arends, J.; Baracos, V.; Bertz, H.; Bozzetti, F.; Calder, P.C.; Deutz, N.E.P.; Erickson, N.; Laviano, A.; Lisanti, M.P.; Lobo, D.N.; et al. ESPEN Expert Group Recommendations for Action against Cancer-Related Malnutrition. Clin. Nutr. 2017, 36, 1187–1196. [Google Scholar] [CrossRef] [Green Version]
- Álvarez, J.; León, M.; Planas, M.; García de Lorenzo, A. The Importance of the Coding of Hospital Malnutrition in the Health Strategy of the European Union: A Spanish Contribution. Nutr. Hosp. 2010, 25, 873–880. [Google Scholar]
- Kabashneh, S.; Alkassis, S.; Shanah, L.; Ali, H. A Complete Guide to Identify and Manage Malnutrition in Hospitalized Patients. Cureus 2020, 12, e8486. [Google Scholar] [CrossRef]
- Truijen, S.P.M.; Hayhoe, R.P.G.; Hooper, L.; Schoenmakers, I.; Forbes, A.; Welch, A.A. Predicting Malnutrition Risk with Data from Routinely Measured Clinical Biochemical Diagnostic Tests in Free-Living Older Populations. Nutrients 2021, 13, 1883. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-Silva, M.C.G.; Barros, A.J.D. Bioelectrical Impedance Analysis in Clinical Practice: A New Perspective on Its Use beyond Body Composition Equations. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 311–317. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical Phase Angle and Impedance Vector Analysis--Clinical Relevance and Applicability of Impedance Parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C. Evolution of Bioimpedance: A Circuitous Journey from Estimation of Physiological Function to Assessment of Body Composition and a Return to Clinical Research. Eur. J. Clin. Nutr. 2013, 67, S2–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genton, L.; Norman, K.; Spoerri, A.; Pichard, C.; Karsegard, V.L.; Herrmann, F.R.; Graf, C.E. Bioimpedance-Derived Phase Angle and Mortality Among Older People. Rejuvenation Res. 2017, 20, 118–124. [Google Scholar] [CrossRef] [PubMed]
- García Almeida, J.M.; García García, C.; Bellido Castañeda, V.; Bellido Guerrero, D.; García Almeida, J.M.; García García, C.; Bellido Castañeda, V.; Bellido Guerrero, D. Nuevo Enfoque de La Nutrición. Valoración Del Estado Nutricional Del Paciente: Función y Composición Corporal. Nutr. Hosp. 2018, 35, 1–14. [Google Scholar] [CrossRef]
- Peixoto da Silva, S.; Santos, J.M.O.; Costa E Silva, M.P.; Gil da Costa, R.M.; Medeiros, R. Cancer Cachexia and Its Pathophysiology: Links with Sarcopenia, Anorexia and Asthenia. J. Cachexia Sarcopenia Muscle 2020, 11, 619–635. [Google Scholar] [CrossRef]
- Della Valle, S.; Colatruglio, S.; La Vela, V.; Tagliabue, E.; Mariani, L.; Gavazzi, C. Nutritional Intervention in Head and Neck Cancer Patients during Chemo-Radiotherapy. Nutrition 2018, 51–52, 95–97. [Google Scholar] [CrossRef]
- Di Renzo, L.; Marchetti, M.; Cioccoloni, G.; Gratteri, S.; Capria, G.; Romano, L.; Soldati, L.; Mele, M.C.; Merra, G.; Cintoni, M.; et al. Role of Phase Angle in the Evaluation of Effect of an Immuno-Enhanced Formula in Post-Surgical Cancer Patients: A Randomized Clinical Trial. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1322–1334. [Google Scholar] [CrossRef]
- Stegel, P.; Kozjek, N.R.; Brumen, B.A.; Strojan, P. Bioelectrical Impedance Phase Angle as Indicator and Predictor of Cachexia in Head and Neck Cancer Patients Treated with (Chemo)Radiotherapy. Eur. J. Clin. Nutr. 2016, 70, 602–606. [Google Scholar] [CrossRef]
- Tzelnick, S.; Singer, P.; Shopen, Y.; Moshkovitz, L.; Fireman, S.; Shpitzer, T.; Mizrachi, A.; Bachar, G. Bioelectrical Impedance Analysis in Patients Undergoing Major Head and Neck Surgery: A Prospective Observational Pilot Study. J. Clin. Med. 2021, 10, 539. [Google Scholar] [CrossRef] [PubMed]
- Małecka-Massalska, T.; Powrózek, T.; Prendecka, M.; Mlak, R.; Sobieszek, G.; Brzozowski, W.; Brzozowska, A. Phase Angle as an Objective and Predictive Factor of Radiotherapy-Induced Changes in Body Composition of Male Patients with Head and Neck Cancer. Vivo 2019, 33, 1645–1651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arab, A.; Karimi, E.; Vingrys, K.; Shirani, F. Is Phase Angle a Valuable Prognostic Tool in Cancer Patients’ Survival? A Systematic Review and Meta-Analysis of Available Literature. Clin. Nutr. 2021, 40, 3182–3190. [Google Scholar] [CrossRef]
- Di Vincenzo, O.; Marra, M.; Sacco, A.M.; Pasanisi, F.; Scalfi, L. Bioelectrical Impedance (BIA)-Derived Phase Angle in Adults with Obesity: A Systematic Review. Clin. Nutr. 2021, 40, 5238–5248. [Google Scholar] [CrossRef]
- Matthews, L.; Bates, A.; Wootton, S.A.; Levett, D. The Use of Bioelectrical Impedance Analysis to Predict Post-Operative Complications in Adult Patients Having Surgery for Cancer: A Systematic Review. Clin. Nutr. 2021, 40, 2914–2922. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.M.E.; Queiroz, M.D.S.C.; de Albuquerque, N.M.C.; Rodrigues, J.; Wiegert, E.V.M.; Calixto-Lima, L.; de Oliveira, L.C. The Prognostic Role of Phase Angle in Advanced Cancer Patients: A Systematic Review. Nutr. Clin. Pract. 2018, 33, 813–824. [Google Scholar] [CrossRef]
- de Almeida, C.; Penna, P.M.; Pereira, S.S.; Rosa, C.D.; Franceschini, S.D. Relationship between Phase Angle and Objective and Subjective Indicators of Nutritional Status in Cancer Patients: A Systematic Review. Nutr. Cancer 2021, 73, 2201–2210. [Google Scholar] [CrossRef]
- Xie, H.; Ruan, G.; Deng, L.; Zhang, H.; Ge, Y.; Zhang, Q.; Lin, S.; Song, M.; Zhang, X.; Liu, X.; et al. Comparison of Absolute and Relative Handgrip Strength to Predict Cancer Prognosis: A Prospective Multicenter Cohort Study. Clin. Nutr. 2022, 41, 1636–1643. [Google Scholar] [CrossRef]
- Mendes, N.P.; de Barros, T.A.; Faria, B.S.; Aguiar, E.S.; de Oliveira, C.A.; de Souza, E.C.; Pereira, S.S.; Rosa, C.D. Hand Grip Strength as Predictor of Undernutrition in Hospitalized Patients with Cancer and a Proposal of Cut-Off. Clin. Nutr. ESPEN 2020, 39, 210–214. [Google Scholar] [CrossRef]
- Barata, A.T.; Santos, C.; Cravo, M.; Vinhas, M.D.C.; Morais, C.; Carolino, E.; Mendes, L.; Vieira, J.R.; Fonseca, J. Handgrip Dynamometry and Patient-Generated Subjective Global Assessment in Patients with Nonresectable Lung Cancer. Nutr. Cancer 2017, 69, 154–158. [Google Scholar] [CrossRef]
- Kilgour, R.D.; Vigano, A.; Trutschnigg, B.; Lucar, E.; Borod, M.; Morais, J.A. Handgrip Strength Predicts Survival and Is Associated with Markers of Clinical and Functional Outcomes in Advanced Cancer Patients. Support Care Cancer 2013, 21, 3261–3270. [Google Scholar] [CrossRef]
- López-Bueno, R.; Andersen, L.L.; Koyanagi, A.; Núñez-Cortés, R.; Calatayud, J.; Casaña, J.; Cruz, B.D.P. Thresholds of handgrip strength for all-cause, cancer, and cardiovascular mortality: A systematic review with dose-response meta-analysis. Ageing Res. Rev. 2022, 82, 101778. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, M.B.; Frandsen, T.F. The Impact of Patient, Intervention, Comparison, Outcome (PICO) as a Search Strategy Tool on Literature Search Quality: A Systematic Review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Alarcón, M.; Ojeda, R.; Huaricancha, I.; Hilario, K. Análisis Crítico de Ensayos Clínicos Aleatorizados: Riesgo de Sesgo. Rev. Estomatológica Hered. 2016, 25, 304. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cereda, E.; Turri, A.; Klersy, C.; Cappello, S.; Ferrari, A.; Filippi, A.R.; Brugnatelli, S.; Caraccia, M.; Chiellino, S.; Borioli, V.; et al. Whey Protein Isolate Supplementation Improves Body Composition, Muscle Strength, and Treatment Tolerance in Malnourished Advanced Cancer Patients Undergoing Chemotherapy. Cancer Med. 2019, 8, 6923–6932. [Google Scholar] [CrossRef]
- Cereda, E.; Cappello, S.; Colombo, S.; Klersy, C.; Imarisio, I.; Turri, A.; Caraccia, M.; Borioli, V.; Monaco, T.; Benazzo, M.; et al. Nutritional Counseling with or without Systematic Use of Oral Nutritional Supplements in Head and Neck Cancer Patients Undergoing Radiotherapy. Radiother. Oncol. 2018, 126, 81–88. [Google Scholar] [CrossRef]
- Norman, K.; Stübler, D.; Baier, P.; Schütz, T.; Ocran, K.; Holm, E.; Lochs, H.; Pirlich, M. Effects of Creatine Supplementation on Nutritional Status, Muscle Function and Quality of Life in Patients with Colorectal Cancer--a Double Blind Randomised Controlled Trial. Clin. Nutr. 2006, 25, 596–605. [Google Scholar] [CrossRef]
- dos Santos Cruz, B.C.; de Carvalho, T.C.; Saraiva, D.D.; dos Santos, A.; dos Reis, P.F. Efeito Do Suplemento Nutricional Enriquecido Com Ácido Eicosapentaenoico Na Massa Magra de Indivíduos Com Câncer de Cavidade Oral Em Pré-Tratamento Oncológico: Um Ensaio Clínico. Rev. Bras. De Cancerol. 2021, 67, e-05868. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 1–694. [Google Scholar] [CrossRef]
- Löser, A.; Abel, J.; Kutz, L.M.; Krause, L.; Finger, A.; Greinert, F.; Sommer, M.; Lorenz, T.; Culmann, E.; von Grundherr, J.; et al. Head and Neck Cancer Patients under (Chemo-)Radiotherapy Undergoing Nutritional Intervention: Results from the Prospective Randomized HEADNUT-Trial. Radiother. Oncol. 2021, 159, 82–90. [Google Scholar] [CrossRef]
- Kutz, L.M.; Abel, J.; Schweizer, D.; Tribius, S.; Krüll, A.; Petersen, C.; Löser, A. Quality of Life, HPV-Status and Phase Angle Predict Survival in Head and Neck Cancer Patients under (Chemo)Radiotherapy Undergoing Nutritional Intervention: Results from the Prospective Randomized HEADNUT-Trial. Radiother. Oncol. 2022, 166, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Tumas, J.; Tumiene, B.; Jurkeviciene, J.; Jasiunas, E.; Sileikis, A. Nutritional and Immune Impairments and Their Effects on Outcomes in Early Pancreatic Cancer Patients Undergoing Pancreatoduodenectomy. Clin. Nutr. 2020, 39, 3385–3394. [Google Scholar] [CrossRef]
- Capello, S.; Cereda, E.; Colombo, S.; Klersy, C.; Imarisio, I. Counseling with or without systematic use of oral supplements in head-neck cancer patients undergoing radiotherapy. Nutrition 2018, 50, e1. [Google Scholar] [CrossRef]
- Finger, A.E. 917P Head and Neck Cancer Patients under (Chemo-)Radiotherapy Undergoing Nutritional Intervention: Results from the Prospective Randomized HEADNUT-Trial. Ann. Oncol. 2021, 32, S810. [Google Scholar] [CrossRef]
- Caccialanza, R.; Cereda, E.; Caraccia, M.; Klersy, C.; Nardi, M.; Cappello, S.; Borioli, V.; Turri, A.; Imarisio, I.; Lasagna, A.; et al. Early 7-Day Supplemental Parenteral Nutrition Improves Body Composition and Muscle Strength in Hypophagic Cancer Patients at Nutritional Risk. Support Care Cancer 2019, 27, 2497–2506. [Google Scholar] [CrossRef] [PubMed]
- Orell, H.; Schwab, U.; Saarilahti, K.; Österlund, P.; Ravasco, P.; Mäkitie, A. Nutritional Counseling for Head and Neck Cancer Patients Undergoing (Chemo) Radiotherapy-A Prospective Randomized Trial. Front. Nutr. 2019, 6, 22. [Google Scholar] [CrossRef]
- Cornejo-Pareja, I.; Ramirez, M.; Camprubi-Robles, M.; Rueda, R.; Vegas-Aguilar, I.M.; Garcia-Almeida, J.M. Effect on an Oral Nutritional Supplement with β-Hydroxy-β-Methylbutyrate and Vitamin D on Morphofunctional Aspects, Body Composition, and Phase Angle in Malnourished Patients. Nutrients 2021, 13, 4355. [Google Scholar] [CrossRef]
- Faccio, A.A.; de Sampaio Mattos, C.H.P.; dos Santos, E.A.S.; Neto, N.R.M.; Moreira, R.P.; Batella, L.T.; Dos Santos, H.; Celes, A.P.M. Oral Nutritional Supplementation in Cancer Patients Who Were Receiving Chemo/Chemoradiation Therapy: A Multicenter, Randomized Phase II Study. Nutr. Cancer 2021, 73, 442–449. [Google Scholar] [CrossRef]
- Thambamroong, T.; Seetalarom, K.; Saichaemchan, S.; Pumsutas, Y.; Prasongsook, N. Efficacy of Curcumin on Treating Cancer Anorexia-Cachexia Syndrome in Locally or Advanced Head and Neck Cancer: A Double-Blind, Placebo-Controlled Randomised Phase IIa Trial (CurChexia). J. Nutr. Metab. 2022, 2022, 5425619. [Google Scholar] [CrossRef] [PubMed]
- Uster, A.; Ruefenacht, U.; Ruehlin, M.; Pless, M.; Siano, M.; Haefner, M.; Imoberdorf, R.; Ballmer, P.E. Influence of a Nutritional Intervention on Dietary Intake and Quality of Life in Cancer Patients: A Randomized Controlled Trial. Nutrition 2013, 29, 1342–1349. [Google Scholar] [CrossRef]
- De Souza, A.P.S.; da Silva, L.C.; Fayh, A.P.T. Nutritional Intervention Contributes to the Improvement of Symptoms Related to Quality of Life in Breast Cancer Patients Undergoing Neoadjuvant Chemotherapy: A Randomized Clinical Trial. Nutrients 2021, 13, 589. [Google Scholar] [CrossRef]
- Giles, K.H.; Kubrak, C.; Baracos, V.E.; Olson, K.; Mazurak, V.C. Recommended European Society of Parenteral and Enteral Nutrition Protein and Energy Intakes and Weight Loss in Patients with Head and Neck Cancer. Head Neck 2016, 38, 1248–1257. [Google Scholar] [CrossRef] [PubMed]
- De Aguiar Pastore Silva, J.; Emilia de Souza Fabre, M.; Waitzberg, D.L. Omega-3 Supplements for Patients in Chemotherapy and/or Radiotherapy: A Systematic Review. Clin. Nutr. 2015, 34, 359–366. [Google Scholar] [CrossRef]
- Morland, S.L.; Martins, K.J.B.; Mazurak, V.C. N-3 Polyunsaturated Fatty Acid Supplementation during Cancer Chemotherapy. J. Nutr. Intermed. Metab. 2016, 5, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Schiessel, D.L.; Baracos, V.E. Barriers to Cancer Nutrition Therapy: Excess Catabolism of Muscle and Adipose Tissues Induced by Tumour Products and Chemotherapy. Proc. Nutr. Soc. 2018, 77, 394–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, D.; Bansal, S.; Morgado, M.; Dev, R.; Chisholm, G.; Bruera, E. Phase Angle for Prognostication of Survival in Patients with Advanced Cancer: Preliminary Findings. Cancer 2014, 120, 2207–2214. [Google Scholar] [CrossRef] [Green Version]
- Ozorio, G.A.; Barão, K.; Forones, N.M. Cachexia Stage, Patient-Generated Subjective Global Assessment, Phase Angle, and Handgrip Strength in Patients with Gastrointestinal Cancer. Nutr. Cancer 2017, 69, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Stobäus, N.; Zocher, D.; Bosy-Westphal, A.; Szramek, A.; Scheufele, R.; Smoliner, C.; Pirlich, M. Cutoff Percentiles of Bioelectrical Phase Angle Predict Functionality, Quality of Life, and Mortality in Patients with Cancer. Am. J. Clin. Nutr. 2010, 92, 612–619. [Google Scholar] [CrossRef] [Green Version]
- Tsai, S. Importance of Lean Body Mass in the Oncologic Patient. Nutr. Clin. Pract. 2012, 27, 593–598. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Ramírez-Vélez, R.; Peterson, M.D.; Lobelo, F.; Cavero-Redondo, I.; Correa-Bautista, J.E.; Martínez-Vizcaíno, V. Handgrip and Knee Extension Strength as Predictors of Cancer Mortality: A Systematic Review and Meta-Analysis. Scand. J. Med. Sci. Sport. 2018, 28, 1852–1858. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Hand-Grip Dynamometry Provides a Valid Indication of Upper Extremity Strength Impairment in Home Care Patients. J. Hand. Ther. 1998, 11, 258–260. [Google Scholar] [CrossRef]
- Hébuterne, X.; Lemarié, E.; Michallet, M.; de Montreuil, C.B.; Schneider, S.M.; Goldwasser, F. Prevalence of Malnutrition and Current Use of Nutrition Support in Patients with Cancer. JPEN J. Parenter. Enteral. Nutr. 2014, 38, 196–204. [Google Scholar] [CrossRef]
- Prado, C.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and Clinical Implications of Sarcopenic Obesity in Patients with Solid Tumours of the Respiratory and Gastrointestinal Tracts: A Population-Based Study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Martin, L.; Birdsell, L.; MacDonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer Cachexia in the Age of Obesity: Skeletal Muscle Depletion Is a Powerful Prognostic Factor, Independent of Body Mass Index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and Classification of Cancer Cachexia: An International Consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European Consensus on Definition and Diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Year | Study Groups | Total (n) | Women (%) | Age (Mean) | BMI (kg/m2) | Cancer | Current Treatment | BIA Methods/Instrument | Nutritional Intervention | Hydraulic Hand Dynamometer |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cereda et al. [40] | 2018 | CS (n = 81) CS + ONS (n = 78) | 159 | 28.3 | 65.1 | 24.2 | Head and neck | Conventional (1.8-to-2 Gy/fraction) 3D conformal RT | NutriLAB, Akern/RJL | ONS (energy-dense, high-protein, omega-3-enriched oral formula) | DynEx |
| Cereda et al. [39] | 2019 | CS (n = 84) CS + WP (n = 82) | 166 | 39.8 | 65.4 | 22.2 | Lung, stomach, esophagus, pancreas, colon, blood, breast, head, and neck | Standard chemotherapy regimens | NutriLAB, Akern/RJL | Two sachets/day of cow milk WP (20 g of proteins) | DynEx |
| Norman et al. [41] | 2006 | Cr (n = 16) C (n = 15) | 31 | 35.5 | 63.4 | 24.9 | Colorectal cancer | Chemotherapy | BIA 2000 M | Creatine supplementation | Digimax electronic dynamometer |
| Cruz et al. [42] | 2017 | EPA (n = 29) C (n = 24) | 53 | 20.8 | 55.5 | 21.6 | Oral cavity | Without treatment | Biodynamics Model 450 | EPA-enriched supplement from fish oil (2 g) | NR |
| Faccio et al. [52] | 2020 | C (n = 42) ONS (n = 43) | 85 | 60 | 58.8 | 25 | Colorectal, breast, lung, upper digestive tract, ovarian and other cancers | Chemo/radiotherapy | Biodynamics, 310 | ONS (hyper-protein supplement, enriched with L-leucine, vitamins, and minerals | NR |
| Thambamroong et al. [53] | 2022 | C (n = 10) Cur (n = 10) | 20 | NR | 59 | NR | Head and neck cancer | Chemo/radiotherapy | InBody | Curcumin (4000 mg) | NR |
| Uster et al. [54] | 2013 | UC (n = 28) NT (n = 30) | 58 | 20.7 | 65 | 22.8 | Breast, lung, head and neck, pancreatic, colorectal, gastrointestinal, renal, prostate, and endometrium cancer. Sarcoma, lymphoma, myeloma, mesothelioma, neuroendocrine tumor, and unknown | NR | NR | Oral nutritional supplements and individual nutritional plan | Jamar |
| De Souza et al. [55] | 2021 | C (n = 15) NT (n = 19) | 34 | 100 | 44.8 | 27.3 | Breast cancer | Chemotherapy | NR | Hyper-protein personalized diet | Jamar |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Victoria-Montesinos, D.; García-Muñoz, A.M.; Navarro-Marroco, J.; Lucas-Abellán, C.; Mercader-Ros, M.T.; Serrano-Martínez, A.; Abellán-Aynés, O.; Barcina-Pérez, P.; Hernández-Sánchez, P. Phase Angle, Handgrip Strength, and Other Indicators of Nutritional Status in Cancer Patients Undergoing Different Nutritional Strategies: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 1790. https://doi.org/10.3390/nu15071790
Victoria-Montesinos D, García-Muñoz AM, Navarro-Marroco J, Lucas-Abellán C, Mercader-Ros MT, Serrano-Martínez A, Abellán-Aynés O, Barcina-Pérez P, Hernández-Sánchez P. Phase Angle, Handgrip Strength, and Other Indicators of Nutritional Status in Cancer Patients Undergoing Different Nutritional Strategies: A Systematic Review and Meta-Analysis. Nutrients. 2023; 15(7):1790. https://doi.org/10.3390/nu15071790
Chicago/Turabian StyleVictoria-Montesinos, Desirée, Ana María García-Muñoz, Julia Navarro-Marroco, Carmen Lucas-Abellán, María Teresa Mercader-Ros, Ana Serrano-Martínez, Oriol Abellán-Aynés, Pablo Barcina-Pérez, and Pilar Hernández-Sánchez. 2023. "Phase Angle, Handgrip Strength, and Other Indicators of Nutritional Status in Cancer Patients Undergoing Different Nutritional Strategies: A Systematic Review and Meta-Analysis" Nutrients 15, no. 7: 1790. https://doi.org/10.3390/nu15071790