
Lipid Profiling Reveals Lipidomic Signatures of Weight Loss Interventions
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Demographic Characteristics
2.2. Lipid Extraction and LC-MS Analyses
2.3. Statistical Analysis
3. Results
3.1. Study Populations
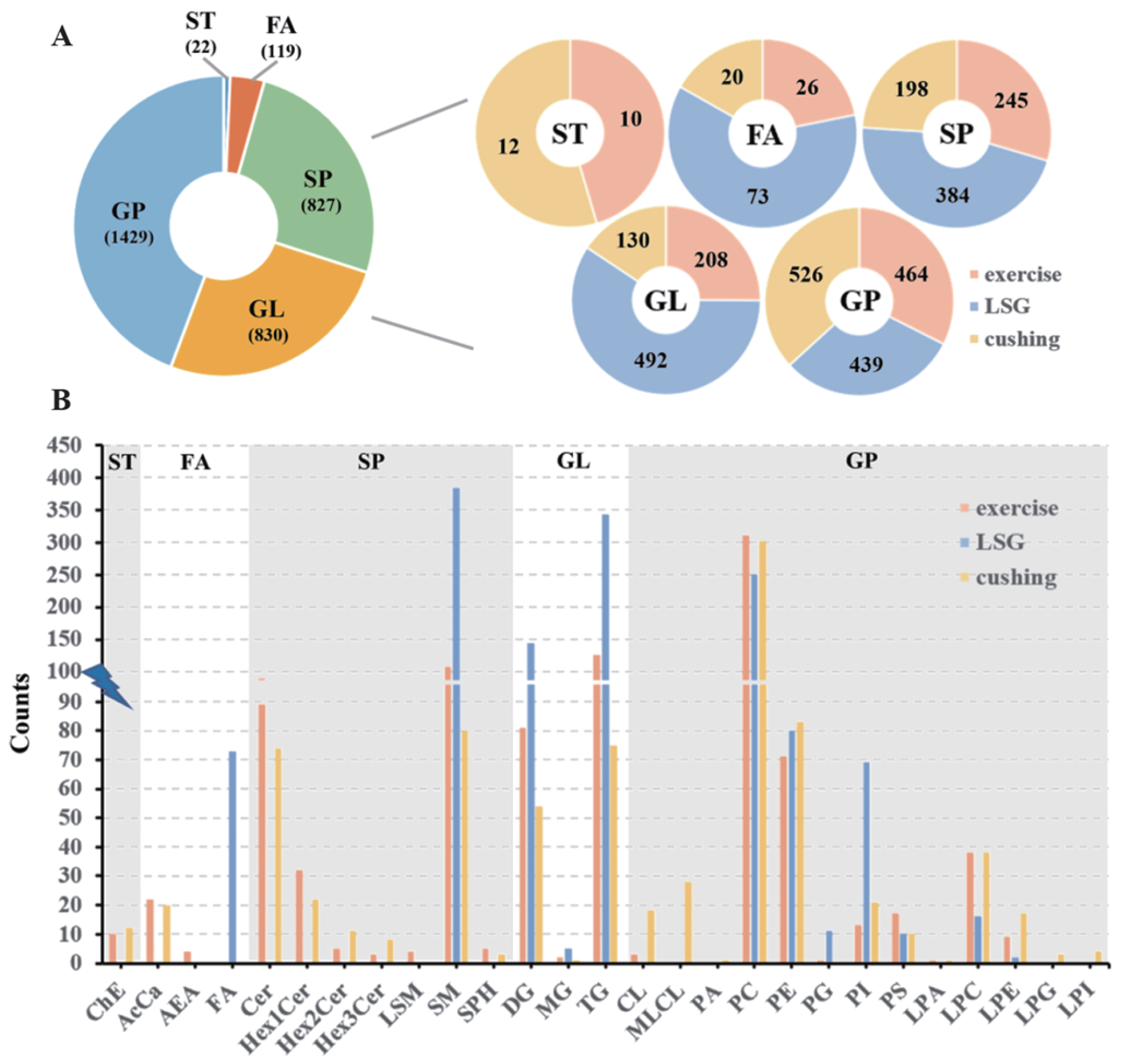
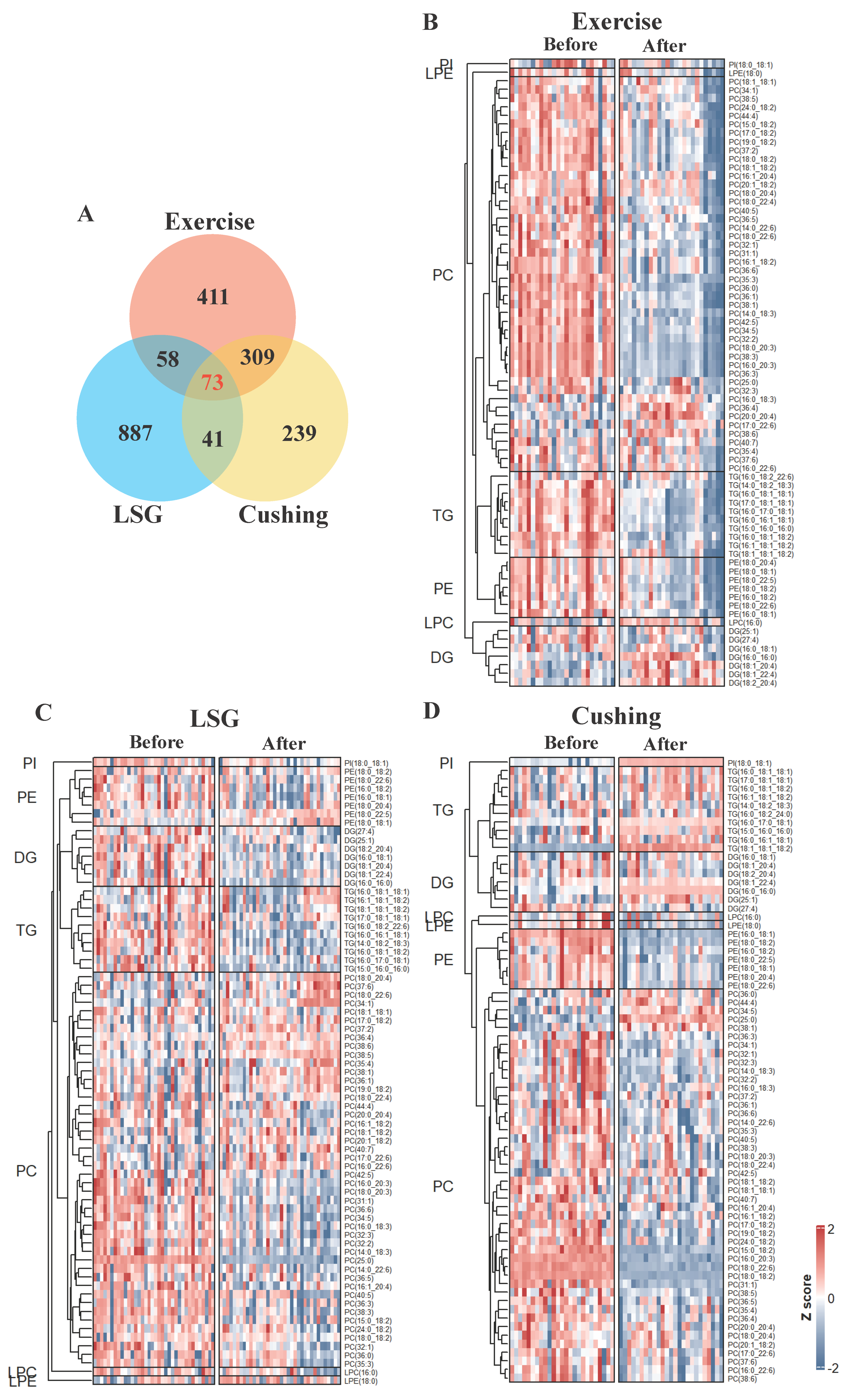
3.2. Overview of Lipidomic Profiling
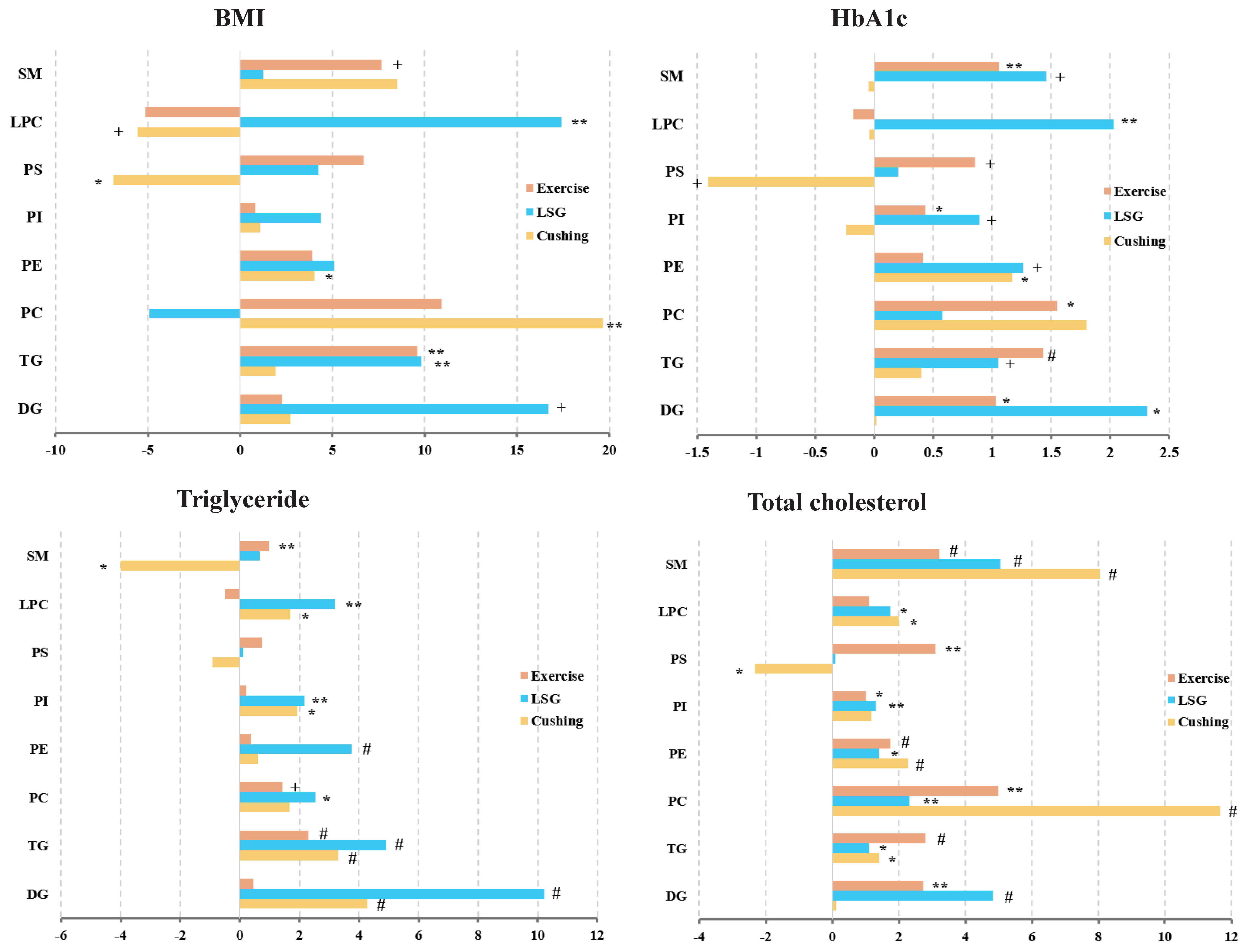
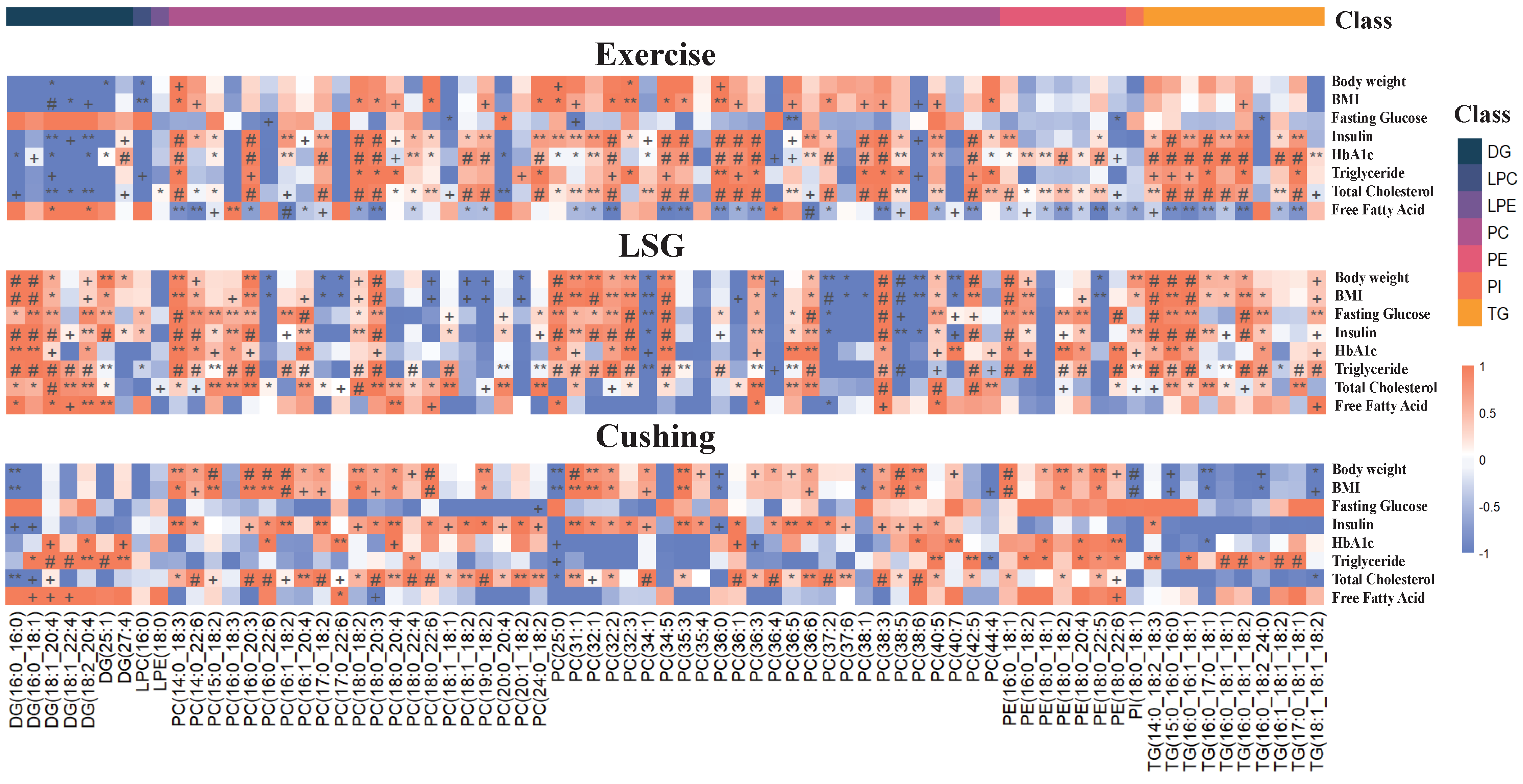
3.3. Lipid Subclasses with Significant Relationships to BMI, HbA1c, Triglyceride, and Total Cholesterol
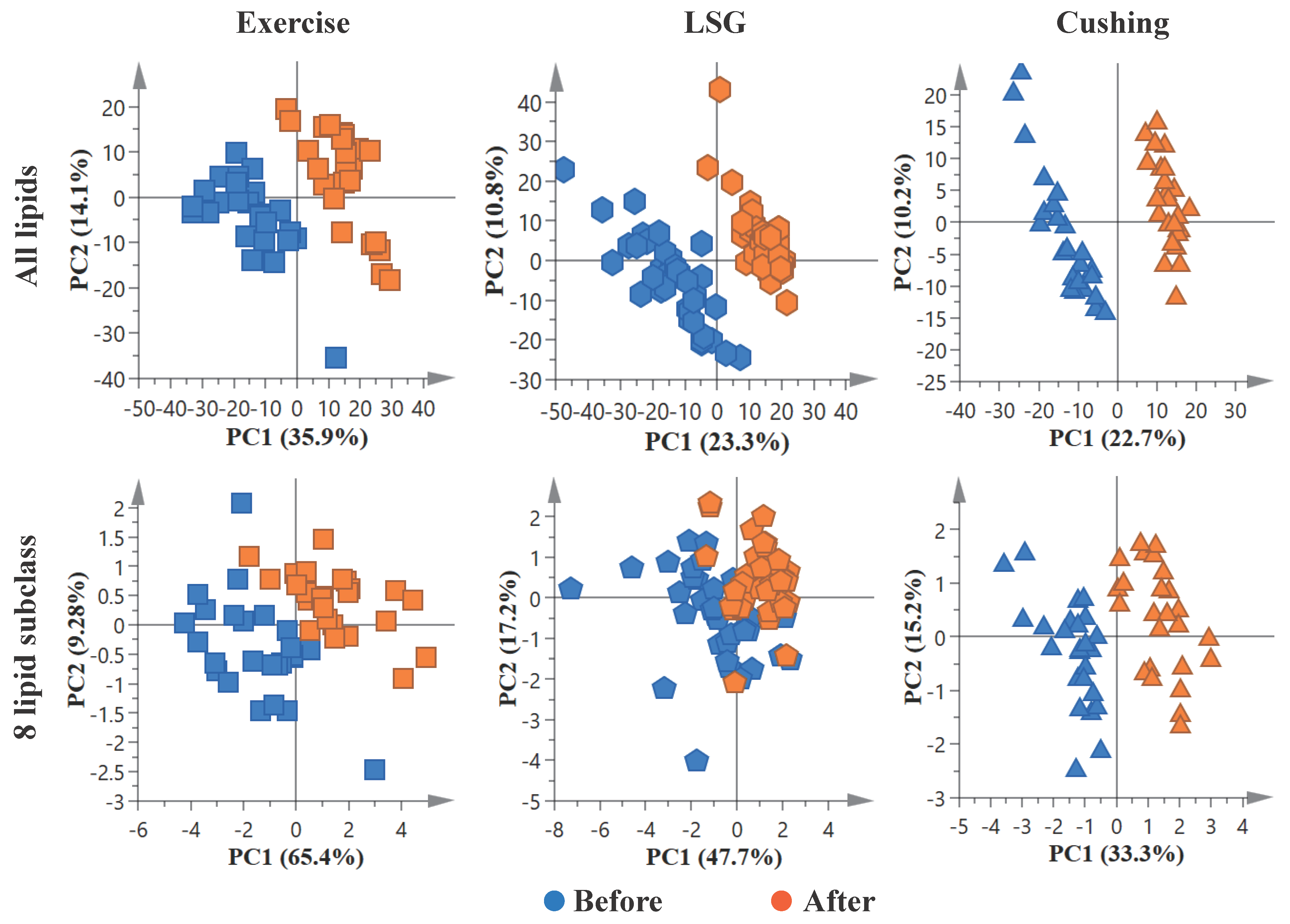
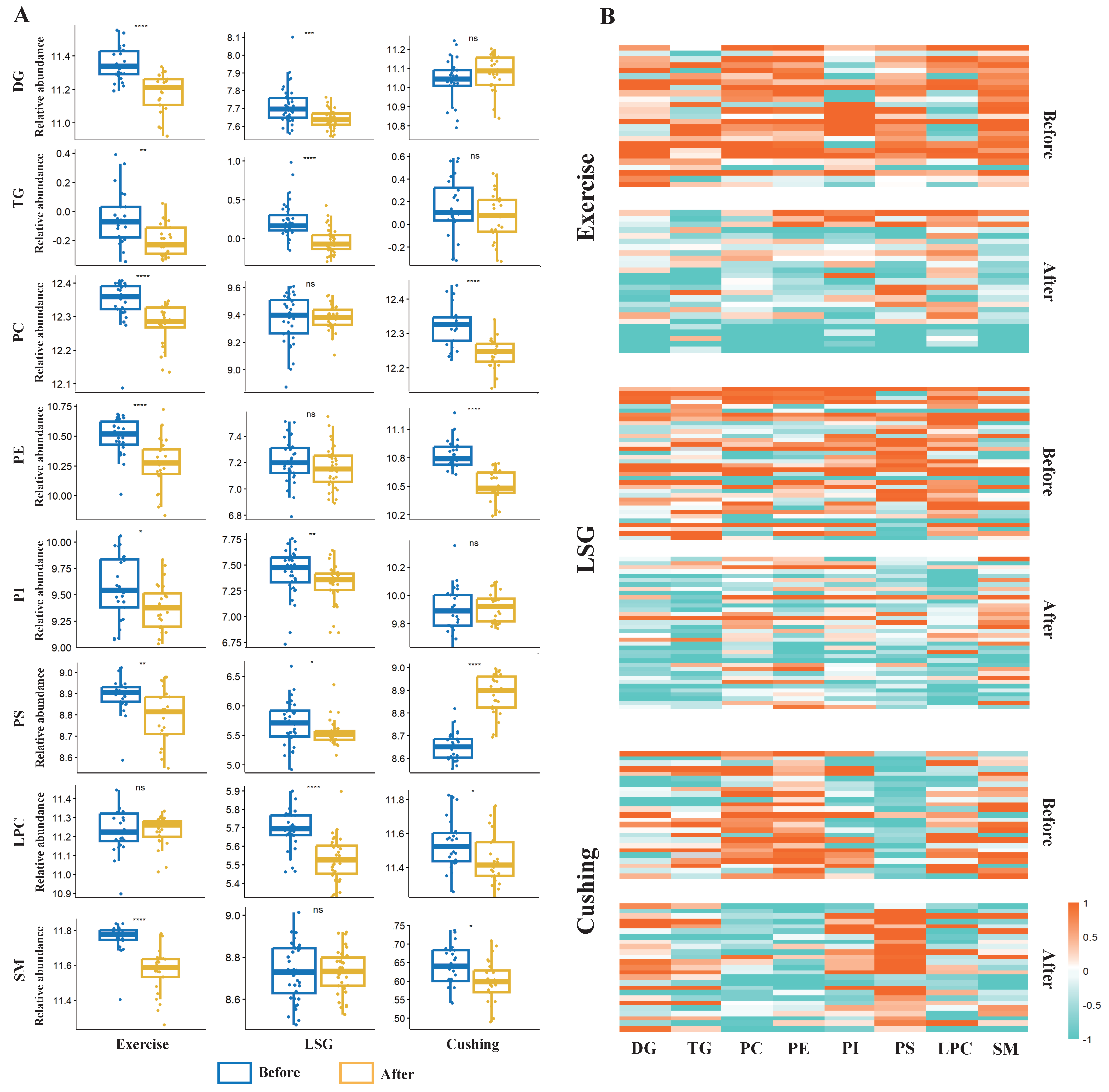
3.4. Exercise and Surgical Interventions Induce Marked Changes in the Lipidome
3.5. Correlations between Lipid Species and Clinical Characteristics
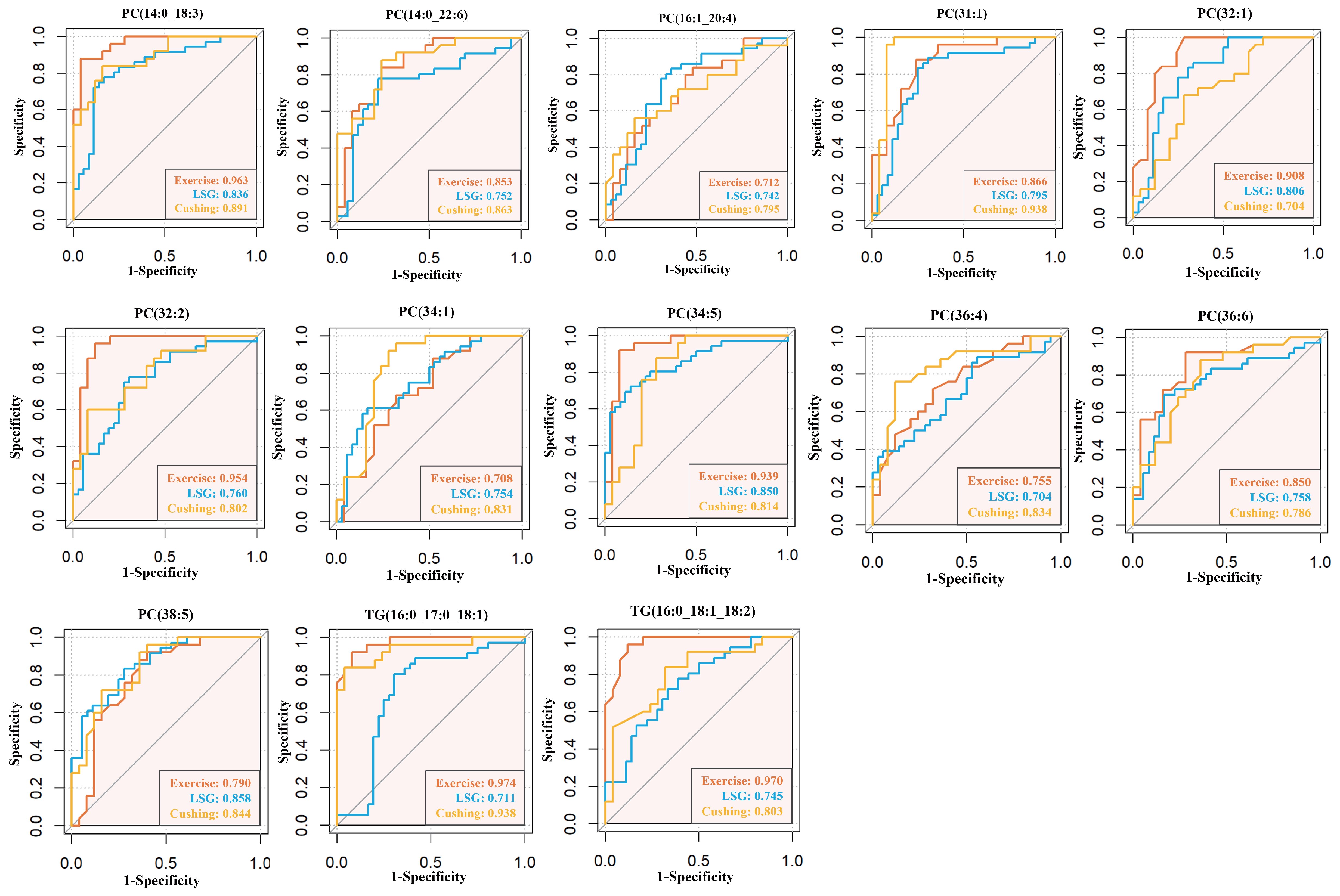
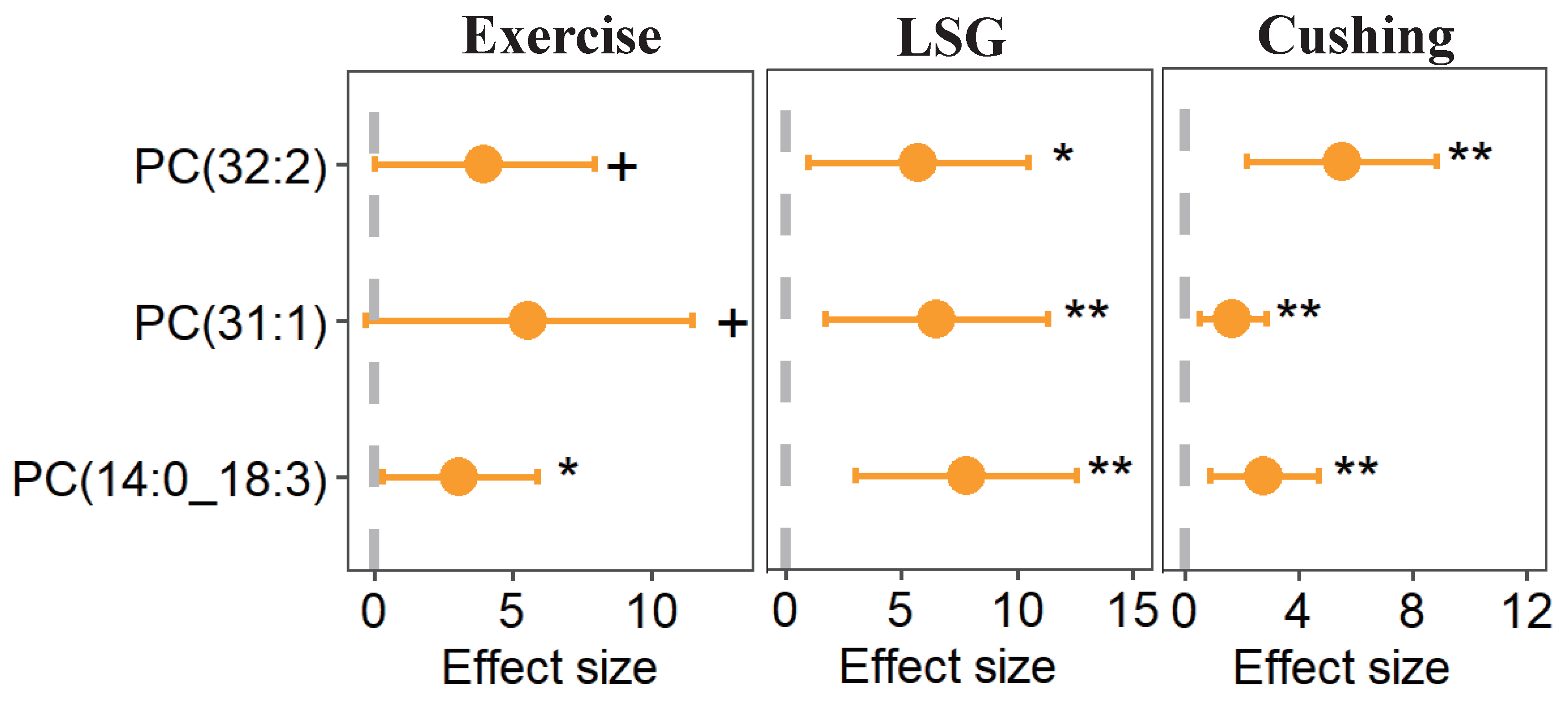
3.6. Utility of Lipid Species as Biomarkers of Weight Loss
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Allison, D.B.; Fontaine, K.R.; Manson, J.E.; Stevens, J.; VanItallie, T.B. Annual deaths attributable to obesity in the United States. JAMA 1999, 282, 1530–1538. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, K.R.; Redden, D.T.; Wang, C.; Westfall, A.O.; Allison, D.B. Years of life lost due to obesity. JAMA 2003, 289, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Willett, W.C.; Li, T.; Stampfer, M.J.; Colditz, G.A.; Manson, J.E. Adiposity as compared with physical activity in predicting mortality among women. N. Engl. J. Med. 2004, 351, 2694–2703. [Google Scholar] [CrossRef] [PubMed]
- Calle, E.E.; Thun, M.J.; Petrelli, J.M.; Rodriguez, C.; Heath, C.W. Body-mass index and mortality in a prospective cohort of U.S. adults. N. Engl. J. Med. 1999, 341, 1097–1105. [Google Scholar] [CrossRef]
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Ogden, C.L. Trends in Obesity and Severe Obesity Prevalence in US Youth and Adults by Sex and Age, 2007–2008 to 2015–2016. JAMA 2018, 319, 1723–1725. [Google Scholar] [CrossRef] [Green Version]
- Pan, X.; Wang, L.; Pan, A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 373–392. [Google Scholar] [CrossRef]
- Prague, J.K.; May, S.; Whitelaw, B.C. Cushing’s syndrome. BMJ 2013, 346, f945. [Google Scholar] [CrossRef]
- Mazziotti, G.; Gazzaruso, C.; Giustina, A. Diabetes in Cushing syndrome: Basic and clinical aspects. Trends Endocrinol. Metab. 2011, 22, 499–506. [Google Scholar] [CrossRef]
- Emmerich, J.; Hu, Q.; Hanke, N.; Hartmann, R.W. Cushing’s Syndrome: Development of Highly Potent and Selective CYP11B1 Inhibitors of the (Pyridylmethyl)pyridine Type. J. Med. Chem. 2013, 56, 6022–6032. [Google Scholar] [CrossRef]
- Contrepois, K.; Wu, S.; Moneghetti, K.J.; Hornburg, D.; Ahadi, S.; Tsai, M.; Metwally, A.A.; Wei, E.; Lee-McMullen, B.; Quijada, J.V.; et al. Molecular Choreography of Acute Exercise. Cell 2020, 181, 1112–1130. [Google Scholar] [CrossRef] [PubMed]
- Long, J.Z. Molecular transducers and the cardiometabolic benefits of exercise. Nat. Rev. Endocrinol. 2022, 18, 77–78. [Google Scholar] [CrossRef] [PubMed]
- Colleluori, G.; Aguirre, L.; Phadnis, U.; Fowler, K.; Armamento-Villareal, R.; Sun, Z.; Brunetti, L.; Hyoung Park, J.; Kaipparettu, B.A.; Putluri, N.; et al. Aerobic Plus Resistance Exercise in Obese Older Adults Improves Muscle Protein Synthesis and Preserves Myocellular Quality Despite Weight Loss. Cell Metab. 2019, 30, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Yao, T.; Wang, H.; Lin, K.; Wang, R.; Guo, S.; Chen, P.; Wu, H.; Liu, T.; Wang, R. Exercise-induced microbial changes in preventing type 2 diabetes. Sci. China Life Sci. 2023. [Google Scholar] [CrossRef]
- Luan, X.; Tian, X.; Zhang, H.; Huang, R.; Li, N.; Chen, P.; Wang, R. Exercise as a prescription for patients with various diseases. J. Sport Health Sci. 2019, 8, 422–441. [Google Scholar] [CrossRef]
- Keating, S.E.; Hackett, D.A.; Parker, H.M.; O Connor, H.T.; Gerofi, J.A.; Sainsbury, A.; Baker, M.K.; Chuter, V.H.; Caterson, I.D.; George, J.; et al. Effect of aerobic exercise training dose on liver fat and visceral adiposity. J. Hepatol. 2015, 63, 174–182. [Google Scholar] [CrossRef]
- Keating, S.E.; Hackett, D.A.; George, J.; Johnson, N.A. Exercise and non-alcoholic fatty liver disease: A systematic review and meta-analysis. J. Hepatol. 2012, 57, 157–166. [Google Scholar] [CrossRef]
- Wolfe, B.M.; Kvach, E.; Eckel, R.H. Treatment of Obesity. Circ. Res. 2016, 118, 1844–1855. [Google Scholar] [CrossRef]
- Kibbe, M.R.; Gerber, D.A. Bariatric Surgeons Should Operate on Patients With Obesity Who Are Receiving Dialysis. JAMA Surg. 2020, 155, 588. [Google Scholar] [CrossRef]
- O’Brien, P.E.; Brown, W.A.; Dixon, J.B. Obesity, weight loss and bariatric surgery. Med. J. Aust. 2005, 183, 310–314. [Google Scholar] [CrossRef]
- Bennett, B.L.; Lawson, J.L.; Funaro, M.C.; Ivezaj, V. Examining weight bias before and/or after bariatric surgery: A systematic review. Obes. Rev. 2022, 23, e13500. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Smith, J.C. Biological Membrane Organization and Cellular Signaling. Chem. Rev. 2019, 119, 5849–5880. [Google Scholar] [CrossRef]
- Vanni, S.; Riccardi, L.; Palermo, G.; De Vivo, M. Structure and Dynamics of the Acyl Chains in the Membrane Trafficking and Enzymatic Processing of Lipids. Acc. Chem. Res. 2019, 52, 3087–3096. [Google Scholar] [CrossRef] [Green Version]
- Mann, R.K.; Beachy, P.A. Novel lipid modifications of secreted protein signals. Annu. Rev. Biochem. 2004, 73, 891–923. [Google Scholar] [CrossRef] [PubMed]
- Kwan, B.C.H.; Kronenberg, F.; Beddhu, S.; Cheung, A.K. Lipoprotein metabolism and lipid management in chronic kidney disease. J. Am. Soc. Nephrol. 2007, 18, 1246–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, K.; Han, X. Lipidomics: Techniques, Applications, and Outcomes Related to Biomedical Sciences. Trends Biochem. Sci. 2016, 41, 954–969. [Google Scholar] [CrossRef] [Green Version]
- Santos, C.R.; Schulze, A. Lipid metabolism in cancer. FEBS J. 2012, 279, 2610–2623. [Google Scholar] [CrossRef]
- Ooi, G.J.; Meikle, P.J.; Huynh, K.; Earnest, A.; Roberts, S.K.; Kemp, W.; Parker, B.L.; Brown, W.; Burton, P.; Watt, M.J. Hepatic lipidomic remodeling in severe obesity manifests with steatosis and does not evolve with non-alcoholic steatohepatitis. J. Hepatol. 2021, 75, 524–535. [Google Scholar] [CrossRef] [PubMed]
- Eichelmann, F.; Sellem, L.; Wittenbecher, C.; Jäger, S.; Kuxhaus, O.; Prada, M.; Cuadrat, R.; Jackson, K.G.; Lovegrove, J.A.; Schulze, M.B. Deep Lipidomics in Human Plasma: Cardiometabolic Disease Risk and Effect of Dietary Fat Modulation. Circulation 2022, 146, 21–35. [Google Scholar] [CrossRef]
- Wu, J.; Cyr, A.; Gruen, D.S.; Lovelace, T.C.; Benos, P.V.; Das, J.; Kar, U.K.; Chen, T.; Guyette, F.X.; Yazer, M.H.; et al. Lipidomic signatures align with inflammatory patterns and outcomes in critical illness. Nat. Commun. 2022, 13, 6789. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Martin, C.K.; Newton, R.L., Jr.; Apolzan, J.W.; Arnold, C.L.; Davis, T.C.; Price-Haywood, E.G.; Denstel, K.D.; Mire, E.F.; Thethi, T.K.; et al. Weight Loss in Underserved Patients—A Cluster-Randomized Trial. N. Engl. J. Med. 2020, 383, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R. American association of clinical endocrinologists and American college of endocrinology comprehensive clinical practice guidelines formedical care of patients with obesity. Endocr. Pract. 2016, 22 (Suppl. S3), 1–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, F.; He, L.; Zhao, L.; Guo, Q.; Yu, D.; Ju, L.; Fang, H. The Status of Dietary Energy and Nutrients Intakes among Chinese Elderly Aged 80 and Above: Data from the CACDNS 2015. Nutrients 2021, 13, 1622. [Google Scholar] [CrossRef] [PubMed]
- Chinese Nutrition Society. Chinese Dietary Reference Intakes (2013); Science Press: Beijing, China, 2014. [Google Scholar]
- Team, R.C. R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing). MSOR Connections, 2014. Available online: https://www.R-project.org/ (accessed on 3 October 2022).
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. S1), S17–S38. [Google Scholar] [CrossRef] [PubMed]
- Crook, T.H.; Tinklenberg, J.; Yesavage, J.; Petrie, W.; Nunzi, M.G.; Massari, D.C. Effects of phosphatidylserine in age-associated memory impairment. Neurology 1991, 41, 644–649. [Google Scholar] [CrossRef]
- Valadas, J.S.; Esposito, G.; Vandekerkhove, D.; Miskiewicz, K.; Deaulmerie, L.; Raitano, S.; Seibler, P.; Klein, C.; Verstreken, P. ER Lipid Defects in Neuropeptidergic Neurons Impair Sleep Patterns in Parkinson’s Disease. Neuron 2018, 27, 98, 1155–1169.e6. [Google Scholar] [CrossRef] [Green Version]
- Zhang, E.; Chai, J.C.; Deik, A.A.; Hua, S.; Sharma, A.; Schneider, M.F.; Gustafson, D.; Hanna, D.B.; Lake, J.E.; Rubin, L.H.; et al. Plasma Lipidomic Profiles and Risk of Diabetes: 2 Prospective Cohorts of HIV-Infected and HIV-Uninfected Individuals. J. Clin. Endocrinol. Metab. 2021, 106, 999–1010. [Google Scholar] [CrossRef]
- Lee, G.B.; Lee, J.C.; Moon, M.H. Plasma lipid profile comparison of five different cancers by nanoflow ultrahigh performance liquid chromatography-tandem mass spectrometry. Anal. Chim. Acta 2019, 1063, 117–126. [Google Scholar] [CrossRef]
- Papandreou, C.; Harrold, J.A.; Hansen, T.T.; Halford, J.C.G.; Sjödin, A.; Bulló, M. Changes in Circulating Metabolites during Weight Loss and Weight Loss Maintenance in Relation to Cardiometabolic Risk. Nutrients 2021, 13, 4289. [Google Scholar] [CrossRef]
- Anjani, K.; Lhomme, M.; Sokolovska, N.; Poitou, C.; Aron-Wisnewsky, J.; Bouillot, J.; Lesnik, P.; Bedossa, P.; Kontush, A.; Clement, K.; et al. Circulating phospholipid profiling identifies portal contribution to NASH signature in obesity. J. Hepatol. 2015, 62, 905–912. [Google Scholar] [CrossRef] [Green Version]
- Yun, H.; Sun, L.; Wu, Q.; Zong, G.; Qi, Q.; Li, H.; Zheng, H.; Zeng, R.; Liang, L.; Lin, X. Associations among circulating sphingolipids, β-cell function, and risk of developing type 2 diabetes: A population-based cohort study in China. PLoS Med. 2020, 17, e1003451. [Google Scholar] [CrossRef] [PubMed]
- Wittenbecher, C.; Guasch-Ferré, M.; Haslam, D.E.; Dennis, C.; Li, J.; Bhupathiraju, S.N.; Lee, C.; Qi, Q.; Liang, L.; Eliassen, A.H.; et al. Changes in metabolomics profiles over ten years and subsequent risk of developing type 2 diabetes: Results from the Nurses’ Health Study. Ebiomedicine 2022, 75, 103799. [Google Scholar] [CrossRef] [PubMed]
- Suvitaival, T.; Bondia-Pons, I.; Yetukuri, L.; Pöhö, P.; Nolan, J.J.; Hyötyläinen, T.; Kuusisto, J.; Orešič, M. Lipidome as a predictive tool in progression to type 2 diabetes in Finnish men. Metabolism 2018, 78, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Rhee, E.P.; Cheng, S.; Larson, M.G.; Walford, G.A.; Lewis, G.D.; McCabe, E.; Yang, E.; Farrell, L.; Fox, C.S.; O Donnell, C.J.; et al. Lipid profiling identifies a triacylglycerol signature of insulin resistance and improves diabetes prediction in humans. J. Clin. Investig. 2011, 121, 1402–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotronen, A.; Velagapudi, V.R.; Yetukuri, L.; Westerbacka, J.; Bergholm, R.; Ekroos, K.; Makkonen, J.; Taskinen, M.R.; Orešič, M.; Yki-Järvinen, H. Serum saturated fatty acids containing triacylglycerols are better markers of insulin resistance than total serum triacylglycerol concentrations. Diabetologia 2009, 52, 684–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kingsley, M. Effects of phosphatidylserine supplementation on exercising humans. Sports Med. 2006, 36, 657–669. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T.; Wolters, B.; Knop, C.; Lass, N.; Hellmuth, C.; Harder, U.; Peissner, W.; Wahl, S.; Grallert, H.; Adamski, J.; et al. Changes in the serum metabolite profile in obese children with weight loss. Eur. J. Nutr. 2015, 54, 173–181. [Google Scholar] [CrossRef]
- Trovato, F.M.; Zia, R.; Artru, F.; Mujib, S.; Jerome, E.; Cavazza, A.; Coen, M.; Wilson, I.; Holmes, E.; Morgan, P.; et al. Lysophosphatidylcholines modulate immunoregulatory checkpoints in peripheral monocytes and are associated with mortality in people with acute liver failure. J. Hepatol. 2023, 78, 558–573. [Google Scholar] [CrossRef]
- Heimerl, S.; Fischer, M.; Baessler, A.; Liebisch, G.; Sigruener, A.; Wallner, S.; Schmitz, G. Alterations of plasma lysophosphatidylcholine species in obesity and weight loss. PLoS ONE 2014, 9, e111348. [Google Scholar] [CrossRef] [Green Version]
- Carayol, M.; Leitzmann, M.F.; Ferrari, P.; Zamora-Ros, R.; Achaintre, D.; Stepien, M.; Schmidt, J.A.; Travis, R.C.; Overvad, K.; Tjønneland, A.; et al. Blood Metabolic Signatures of Body Mass Index: A Targeted Metabolomics Study in the EPIC Cohort. J. Proteome Res. 2017, 16, 3137–3146. [Google Scholar] [CrossRef]
- Frigerio, G.; Favero, C.; Savino, D.; Mercadante, R.; Albetti, B.; Dioni, L.; Vigna, L.; Bollati, V.; Pesatori, A.C.; Fustinoni, S. Plasma Metabolomic Profiling in 1391 Subjects with Overweight and Obesity from the SPHERE Study. Metabolites 2021, 11, 194. [Google Scholar] [CrossRef]
- Bagheri, M.; Djazayery, A.; Farzadfar, F.; Qi, L.; Yekaninejad, M.S.; Aslibekyan, S.; Chamari, M.; Hassani, H.; Koletzko, B.; Uhl, O. Plasma metabolomic profiling of amino acids and polar lipids in Iranian obese adults. Lipids Health Dis. 2019, 18, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, M.; Morris, C.; O’Grada, C.M.; Ryan, M.; Dillon, E.T.; Coleman, E.; Gibney, E.R.; Gibney, M.J.; Roche, H.M.; Brennan, L. Relationship between the lipidome, inflammatory markers and insulin resistance. Mol. Biosyst. 2014, 10, 1586–1595. [Google Scholar] [CrossRef] [PubMed]
- Pikó, P.; Pál, L.; Szűcs, S.; Kósa, Z.; Sándor, J.; Ádány, R. Obesity-Related Changes in Human Plasma Lipidome Determined by the Lipidyzer Platform. Biomolecules 2021, 11, 326. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J.; Oh, J.Y.; Lee, K.S.; Lim, H.K.; Lee, J.; Yoon, H.; Jung, J. Lipid Profiles Obtained from MALDI Mass Spectrometric Imaging in Liver Cancer Metastasis Model. Int. J. Anal. Chem. 2022, 2022, 1–5. [Google Scholar] [CrossRef]
- Papandreou, C.; García Gavilán, J.; Camacho Barcia, L.; Toft Hansen, T.; Harrold, J.A.; Sjödin, A.; Halford, J.C.G.; Bulló, M. Changes in Circulating Metabolites During Weight Loss are Associated with Adiposity Improvement, and Body Weight and Adiposity Regain During Weight Loss Maintenance: The SATIN Study. Mol. Nutr. Food Res. 2021, 65, 2001154. [Google Scholar] [CrossRef]
- Wahl, S.; Holzapfel, C.; Yu, Z.; Breier, M.; Kondofersky, I.; Fuchs, C.; Singmann, P.; Prehn, C.; Adamski, J.; Grallert, H.; et al. Metabolomics reveals determinants of weight loss during lifestyle intervention in obese children. Metabolomics 2013, 9, 1157–1167. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Exercise | LSG | Cushing | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | p Value 2 | Before | After | p Value | Before | After | p Value | |
| N | 25 | 36 | 25 | ||||||
| female (%) | 32% | 47.2% | 100% | ||||||
| age (years) | 12.8 ± 0.36 | 32.64 ± 1.77 | 39.84 ± 2.33 | ||||||
| Body Weight (kg) | 83.61 ± 3.98 | 75.12 ± 3.58 | *** | 112.53 ± 3.00 | 83.13 ± 2.41 | *** | 65.67 ± 2.15 | 58.79 ± 1.92 | * |
| BMI (kg/m2) | 29.87 ± 0.81 | 27.32 ± 0.74 | * | 38.9 ± 0.89 | 28.69 ± 0.76 | *** | 25.28 ± 0.55 | 22.81 ± 0.54 | ** |
| FBG (mmol/L) | 4.16 ± 0.12 | 4.23 ± 0.07 | 5.61 ± 0.18 | 4.86 ± 0.16 | *** | 5.43 ± 0.24 | 4.94 ± 0.14 | ||
| Insulin (pmol/L) | 12.48 ± 1.14 | 7.1 ± 0.63 | *** | 24.87 ± 2.80 | 9.88 ± 1.10 | *** | 17.52 ± 2.60 | 9.96 ± 1.65 | ** |
| HbA1c (%) | 5.74 ± 0.07 | 5.32 ± 0.06 | *** | 6.12 ± 0.16 | 5.52 ± 0.10 | *** | 6.15 ± 0.15 | 5.69 ± 0.12 | * |
| HDL (mmol/L) | 1.29 ± 0.06 | 1.14 ± 0.04 | 1.01 ± 0.03 | 1.16 ± 0.04 | ** | 1.5 ± 0.07 | 1.2 ± 0.04 | *** | |
| LDL (mmol/L) | 2.73 ± 0.12 | 2.02 ± 0.08 | *** | 3.31 ± 0.16 | 3.1 ± 0.12 | 3.08 ± 0.17 | 2.5 ± 0.11 | ** | |
| Triglyceride (mmol/L) | 0.96 ± 0.10 | 0.66 ± 0.03 | ** | 2.07 ± 0.28 | 0.99 ± 0.07 | *** | 1.58 ± 0.21 | 1.30 ± 0.13 | |
| Total Cholesterol (mmol/L) | 4.43 ± 0.16 | 3.41 ± 0.10 | *** | 4.96 ± 0.17 | 4.73 ± 0.13 | 4.94 ± 0.30 | 4.21 ± 0.15 | ** | |
| Free Fatty Acids (mmol/L) | 0.89 ± 0.05 | 1.16 ± 0.07 | ** | 0.62 ± 0.04 | 0.51 ± 0.03 | * | 0.460 ± 0.03 | 0.55 ± 0.022 | * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, K.; Cheng, W.; Shen, Q.; Wang, H.; Wang, R.; Guo, S.; Wu, X.; Wu, W.; Chen, P.; Wang, Y.; et al. Lipid Profiling Reveals Lipidomic Signatures of Weight Loss Interventions. Nutrients 2023, 15, 1784. https://doi.org/10.3390/nu15071784
Lin K, Cheng W, Shen Q, Wang H, Wang R, Guo S, Wu X, Wu W, Chen P, Wang Y, et al. Lipid Profiling Reveals Lipidomic Signatures of Weight Loss Interventions. Nutrients. 2023; 15(7):1784. https://doi.org/10.3390/nu15071784
Chicago/Turabian StyleLin, Kaiqing, Wei Cheng, Qiwei Shen, Hui Wang, Ruwen Wang, Shanshan Guo, Xianmin Wu, Wei Wu, Peijie Chen, Yongfei Wang, and et al. 2023. "Lipid Profiling Reveals Lipidomic Signatures of Weight Loss Interventions" Nutrients 15, no. 7: 1784. https://doi.org/10.3390/nu15071784