
Interleukin-18 Is a Potential Biomarker Linking Dietary Fatty Acid Quality and Insulin Resistance: Results from a Cross-Sectional Study in Northern Italy

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Participants
2.2. Dietary Assessment
2.3. Biochemical Analysis
2.4. Metabolic Syndrome
2.5. Statistical Analysis
3. Results
3.1. Study Participant Characteristics
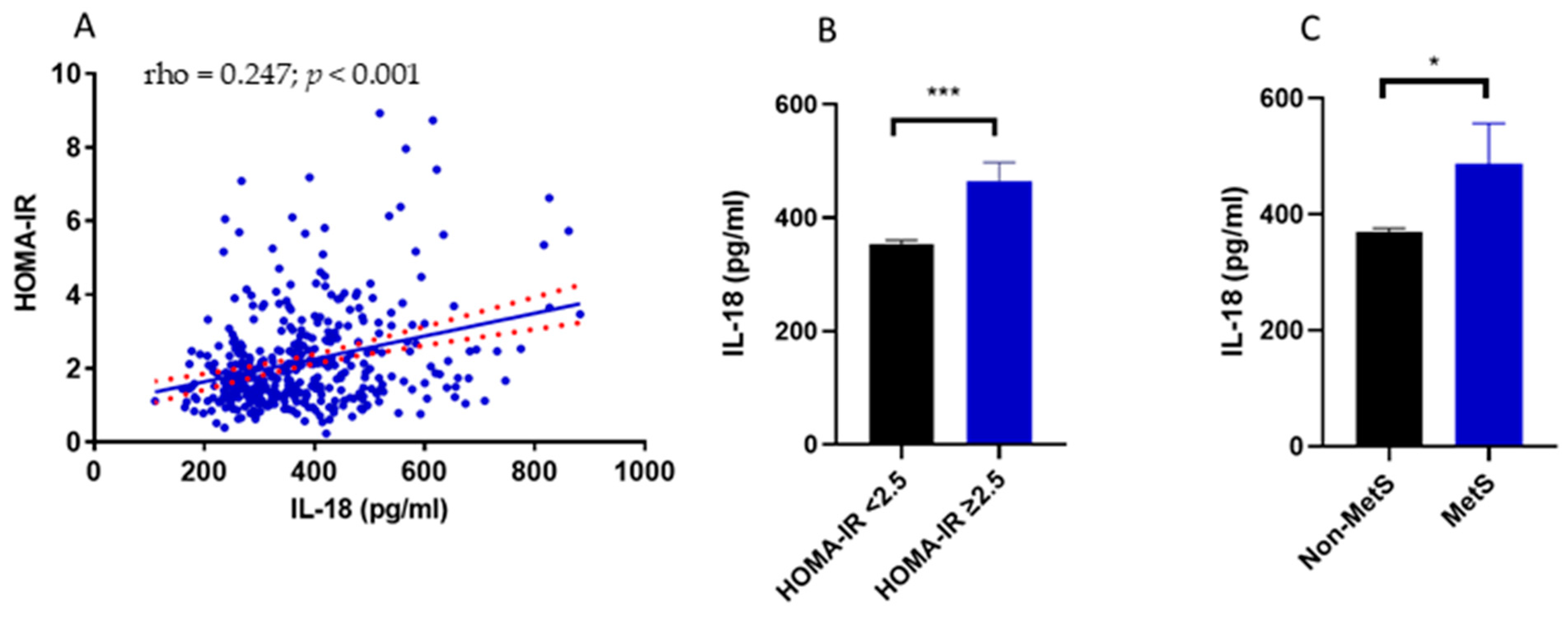
3.2. Relationship between IL-18 Circulating Levels, Insulin Resistance, Metabolic Syndrome and Body Composition
3.3. Dietary Fatty Acids and Their Impact on IL-18 Circulating Levels
3.4. Dietary Fatty Acid Intake and Insulin Resistance
3.5. Dietary Fatty Acid Quality as a Predictor of IL-18 Circulating Levels
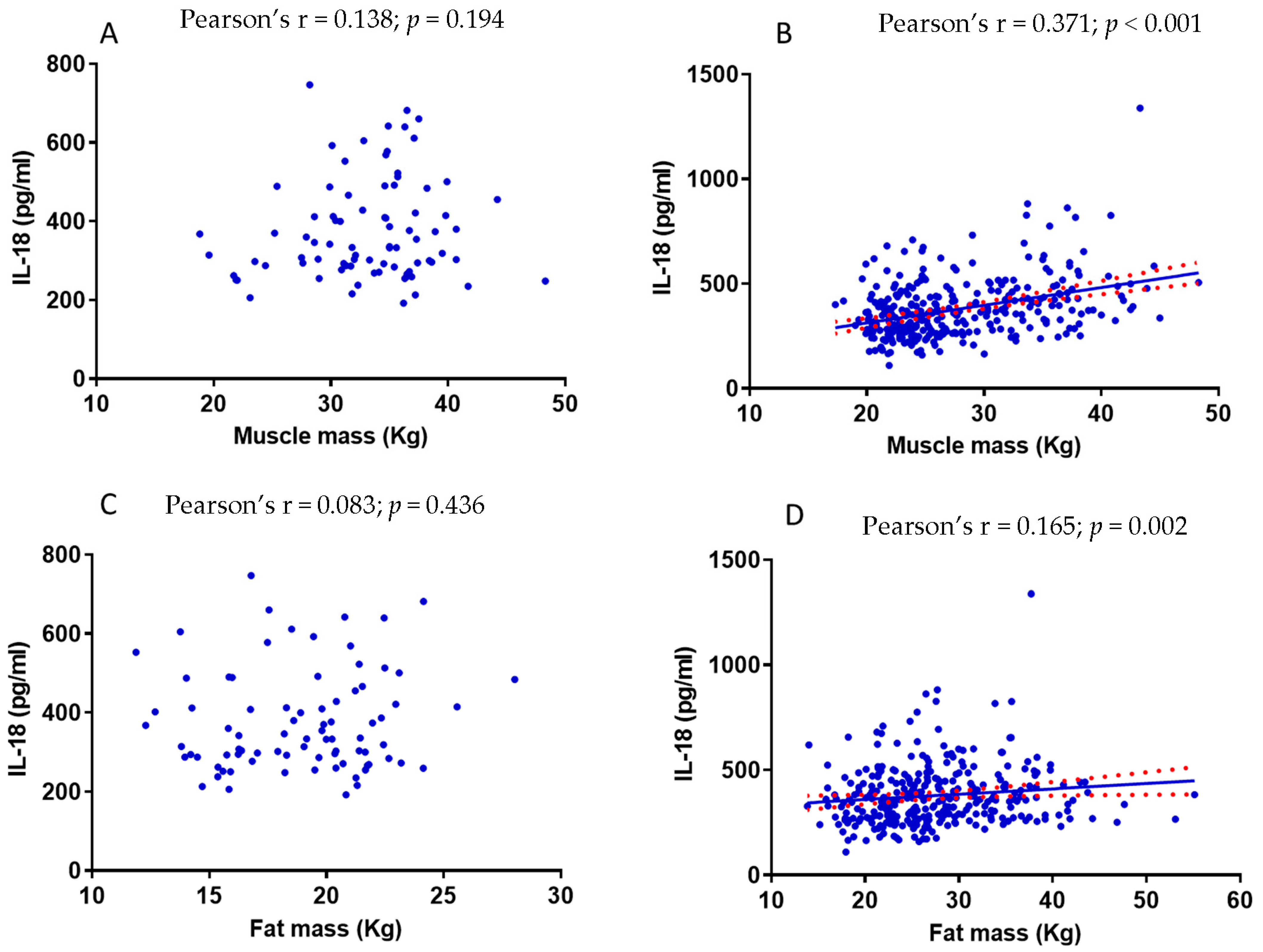
3.6. The Relationship between Muscle Mass and IL-18 Is Influenced by Fat Mass
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Friedrich, M.J. Global Obesity Epidemic Worsening. JAMA 2017, 318, 603. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.V.; Fujioka, K.; Wilson, P.W.; Woodworth, K.A. Obesity: Why be concerned? Am. J. Med. 2009, 122, S4–S11. [Google Scholar] [CrossRef] [PubMed]
- Mazon, J.N.; de Mello, A.H.; Ferreira, G.K.; Rezin, G.T. The impact of obesity on neurodegenerative diseases. Life Sci. 2017, 182, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Gregor, M.F.; Hotamisligil, G. Inflammatory Mechanisms in Obesity. Annu. Rev. Immunol. 2011, 29, 415–445. [Google Scholar] [CrossRef] [Green Version]
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol. Cell Physiol. 2021, 320, C375–C391. [Google Scholar] [CrossRef]
- de Luca, C.; Olefsky, J.M. Inflammation and insulin resistance. FEBS Lett. 2008, 582, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Plomgaard, P.; Bouzakri, K.; Krogh-Madsen, R.; Mittendorfer, B.; Zierath, J.R.; Pedersen, B.K. Tumor necrosis factor-alpha induces skeletal muscle insulin resistance in healthy human subjects via inhibition of Akt substrate 160 phosphorylation. Diabetes 2005, 54, 2939–2945. [Google Scholar] [CrossRef] [Green Version]
- Mohallem, R.; Aryal, U.K. Regulators of TNFalpha mediated insulin resistance elucidated by quantitative proteomics. Sci. Rep. 2020, 10, 20878. [Google Scholar] [CrossRef]
- Sergi, D.; Luscombe-Marsh, N.; Heilbronn, L.K.; Birch-Machin, M.; Naumovski, N.; Lionetti, L.; Proud, C.G.; Abeywardena, M.Y.; O’Callaghan, N. The Inhibition of Metabolic Inflammation by EPA Is Associated with Enhanced Mitochondrial Fusion and Insulin Signaling in Human Primary Myotubes. J. Nutr. 2021, 151, 810–819. [Google Scholar] [CrossRef]
- Hotamisligil, G.S. Inflammatory pathways and insulin action. Int. J. Obes. Relat. Metab. Disord. 2003, 27, S53–S55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruun, J.M.; Stallknecht, B.; Helge, J.W.; Richelsen, B. Interleukin-18 in plasma and adipose tissue: Effects of obesity, insulin resistance, and weight loss. Eur. J. Endocrinol. 2007, 157, 465–471. [Google Scholar] [CrossRef] [Green Version]
- Hung, J.; McQuillan, B.M.; Chapman, C.M.; Thompson, P.L.; Beilby, J.P. Elevated interleukin-18 levels are associated with the metabolic syndrome independent of obesity and insulin resistance. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1268–1273. [Google Scholar] [CrossRef] [Green Version]
- Zirlik, A.; Abdullah, S.M.; Gerdes, N.; MacFarlane, L.; Schonbeck, U.; Khera, A.; McGuire, D.K.; Vega, G.L.; Grundy, S.; Libby, P.; et al. Interleukin-18, the metabolic syndrome, and subclinical atherosclerosis: Results from the Dallas Heart Study. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 2043–2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, R.; Thomas, R.; Kochumon, S.; Sindhu, S. Increased adipose tissue expression of IL-18R and its ligand IL-18 associates with inflammation and insulin resistance in obesity. Immun. Inflamm. Dis. 2017, 5, 318–335. [Google Scholar] [CrossRef]
- Van Guilder, G.P.; Hoetzer, G.L.; Greiner, J.J.; Stauffer, B.L.; Desouza, C.A. Influence of metabolic syndrome on biomarkers of oxidative stress and inflammation in obese adults. Obesity 2006, 14, 2127–2131. [Google Scholar] [CrossRef]
- Rabkin, S.W. The role of interleukin 18 in the pathogenesis of hypertension-induced vascular disease. Nat. Clin. Pract. Cardiovasc. Med. 2009, 6, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.; Collins, M.; Jennings, C.; van der Merwe, L.; Soderstrom, I.; Olsson, T.; Levitt, N.S.; Lambert, E.V.; Goedecke, J.H. The association of interleukin-18 genotype and serum levels with metabolic risk factors for cardiovascular disease. Eur. J. Endocrinol. 2007, 157, 633–640. [Google Scholar] [CrossRef] [Green Version]
- Espinola-Klein, C.; Rupprecht, H.J.; Bickel, C.; Lackner, K.; Genth-Zotz, S.; Post, F.; Munzel, T.; Blankenberg, S.; Athero Gene, I. Impact of inflammatory markers on cardiovascular mortality in patients with metabolic syndrome. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 278–284. [Google Scholar] [CrossRef]
- Presta, I.; Andreozzi, F.; Succurro, E.; Marini, M.A.; Laratta, E.; Lauro, R.; Hribal, M.L.; Perticone, F.; Sesti, G. IL-18 gene polymorphism and metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2009, 19, e5–e6. [Google Scholar] [CrossRef]
- Hart, M.J.; Torres, S.J.; McNaughton, S.A.; Milte, C.M. Dietary patterns and associations with biomarkers of inflammation in adults: A systematic review of observational studies. Nutr. J. 2021, 20, 24. [Google Scholar] [CrossRef]
- Bonaccio, M.; Cerletti, C.; Iacoviello, L.; de Gaetano, G. Mediterranean diet and low-grade subclinical inflammation: The Moli-sani study. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Christ, A.; Lauterbach, M.; Latz, E. Western Diet and the Immune System: An Inflammatory Connection. Immunity 2019, 51, 794–811. [Google Scholar] [CrossRef] [PubMed]
- Troseid, M.; Arnesen, H.; Hjerkinn, E.M.; Seljeflot, I. Serum levels of interleukin-18 are reduced by diet and n-3 fatty acid intervention in elderly high-risk men. Metabolism 2009, 58, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Sergi, D.; Luscombe-Marsh, N.; Naumovski, N.; Abeywardena, M.; O’Callaghan, N. Palmitic Acid, but Not Lauric Acid, Induces Metabolic Inflammation, Mitochondrial Fragmentation, and a Drop in Mitochondrial Membrane Potential in Human Primary Myotubes. Front. Nutr. 2021, 8, 663838. [Google Scholar] [CrossRef]
- Zhou, H.; Urso, C.J.; Jadeja, V. Saturated Fatty Acids in Obesity-Associated Inflammation. J. Inflamm. Res. 2020, 13, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Mu, L.; Mukamal, K.J.; Naqvi, A.Z. Erythrocyte saturated fatty acids and systemic inflammation in adults. Nutrition 2014, 30, 1404–1408. [Google Scholar] [CrossRef] [Green Version]
- Santamarina, A.B.; Pisani, L.P.; Baker, E.J.; Marat, A.D.; Valenzuela, C.A.; Miles, E.A.; Calder, P.C. Anti-inflammatory effects of oleic acid and the anthocyanin keracyanin alone and in combination: Effects on monocyte and macrophage responses and the NF-kappaB pathway. Food Funct. 2021, 12, 7909–7922. [Google Scholar] [CrossRef]
- Sears, B.; Perry, M. The role of fatty acids in insulin resistance. Lipids Health Dis. 2015, 14, 121. [Google Scholar] [CrossRef] [Green Version]
- Palomer, X.; Pizarro-Delgado, J.; Barroso, E.; Vazquez-Carrera, M. Palmitic and Oleic Acid: The Yin and Yang of Fatty Acids in Type 2 Diabetes Mellitus. Trends Endocrinol. Metab. 2018, 29, 178–190. [Google Scholar] [CrossRef]
- Yong, K.; Mori, T.; Chew, G.; Beilin, L.J.; Puddey, I.; Watts, G.F.; Irish, A.; Dogra, G.; Boudville, N.; Lim, W. The Effects of OMEGA-3 Fatty Acid Supplementation Upon Interleukin-12 and Interleukin-18 in Chronic Kidney Disease Patients. J. Ren. Nutr. 2019, 29, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Sanz, J.M.; Sergi, D.; Colombari, S.; Capatti, E.; Situlin, R.; Biolo, G.; Di Girolamo, F.G.; Lazzer, S.; Šimunič, B.; Pišot, R. Dietary Acid Load but Not Mediterranean Diet Adherence Score Is Associated with Metabolic and Cardiovascular Health State: A Population Observational Study from Northern Italy. Front. Nutr. 2022, 617, 828587. [Google Scholar] [CrossRef]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.K.; Huh, J.H.; Yoo, J.S.; Kim, J.W.; Lee, K.J. HOMA-estimated insulin resistance as an independent prognostic factor in patients with acute pancreatitis. Sci. Rep. 2019, 9, 14894. [Google Scholar] [CrossRef] [Green Version]
- Teng, K.T.; Chang, C.Y.; Chang, L.F.; Nesaretnam, K. Modulation of obesity-induced inflammation by dietary fats: Mechanisms and clinical evidence. Nutr. J. 2014, 13, 12. [Google Scholar] [CrossRef] [Green Version]
- Reilly, S.M.; Saltiel, A.R. Adapting to obesity with adipose tissue inflammation. Nat. Rev. Endocrinol. 2017, 13, 633–643. [Google Scholar] [CrossRef]
- Solinas, G.; Karin, M. JNK1 and IKKbeta: Molecular links between obesity and metabolic dysfunction. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2010, 24, 2596–2611. [Google Scholar] [CrossRef]
- Krogh-Madsen, R.; Plomgaard, P.; Moller, K.; Mittendorfer, B.; Pedersen, B.K. Influence of TNF-alpha and IL-6 infusions on insulin sensitivity and expression of IL-18 in humans. Am. J. Physiol. Endocrinol. Metab. 2006, 291, E108–E114. [Google Scholar] [CrossRef]
- Hivert, M.F.; Sun, Q.; Shrader, P.; Mantzoros, C.S.; Meigs, J.B.; Hu, F.B. Circulating IL-18 and the risk of type 2 diabetes in women. Diabetologia 2009, 52, 2101–2108. [Google Scholar] [CrossRef] [Green Version]
- Thorand, B.; Kolb, H.; Baumert, J.; Koenig, W.; Chambless, L.; Meisinger, C.; Illig, T.; Martin, S.; Herder, C. Elevated levels of interleukin-18 predict the development of type 2 diabetes: Results from the MONICA/KORA Augsburg Study, 1984–2002. Diabetes 2005, 54, 2932–2938. [Google Scholar] [CrossRef]
- Ruiz-Nunez, B.; Dijck-Brouwer, D.A.; Muskiet, F.A. The relation of saturated fatty acids with low-grade inflammation and cardiovascular disease. J. Nutr. Biochem. 2016, 36, 1–20. [Google Scholar] [CrossRef]
- Baer, D.J.; Judd, J.T.; Clevidence, B.A.; Tracy, R.P. Dietary fatty acids affect plasma markers of inflammation in healthy men fed controlled diets: A randomized crossover study. Am. J. Clin. Nutr. 2004, 79, 969–973. [Google Scholar] [CrossRef] [Green Version]
- Weaver, K.L.; Ivester, P.; Seeds, M.; Case, L.D.; Arm, J.P.; Chilton, F.H. Effect of dietary fatty acids on inflammatory gene expression in healthy humans. J. Biol. Chem. 2009, 284, 15400–15407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravaut, G.; Legiot, A.; Bergeron, K.F.; Mounier, C. Monounsaturated Fatty Acids in Obesity-Related Inflammation. Int. J. Mol. Sci. 2020, 22, 330. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, J.; Costa, G.; Renaud, J.; Moitie, A.; Glemet, H.; Sergi, D.; Martinoli, M.G. The Neuroinflammatory and Neurotoxic Potential of Palmitic Acid Is Mitigated by Oleic Acid in Microglial Cells and Microglial-Neuronal Co-cultures. Mol. Neurobiol. 2021, 58, 3000–3014. [Google Scholar] [CrossRef] [PubMed]
- Salvado, L.; Coll, T.; Gomez-Foix, A.M.; Salmeron, E.; Barroso, E.; Palomer, X.; Vazquez-Carrera, M. Oleate prevents saturated-fatty-acid-induced ER stress, inflammation and insulin resistance in skeletal muscle cells through an AMPK-dependent mechanism. Diabetologia 2013, 56, 1372–1382. [Google Scholar] [CrossRef] [PubMed]
- Peng, G.; Li, L.; Liu, Y.; Pu, J.; Zhang, S.; Yu, J.; Zhao, J.; Liu, P. Oleate blocks palmitate-induced abnormal lipid distribution, endoplasmic reticulum expansion and stress, and insulin resistance in skeletal muscle. Endocrinology 2011, 152, 2206–2218. [Google Scholar] [CrossRef] [Green Version]
- Sergi, D.; Morris, A.C.; Kahn, D.E.; McLean, F.H.; Hay, E.A.; Kubitz, P.; MacKenzie, A.; Martinoli, M.G.; Drew, J.E.; Williams, L.M. Palmitic acid triggers inflammatory responses in N42 cultured hypothalamic cells partially via ceramide synthesis but not via TLR4. Nutr. Neurosci. 2018, 23, 321–334. [Google Scholar] [CrossRef]
- Lim, J.H.; Gerhart-Hines, Z.; Dominy, J.E.; Lee, Y.; Kim, S.; Tabata, M.; Xiang, Y.K.; Puigserver, P. Oleic acid stimulates complete oxidation of fatty acids through protein kinase A-dependent activation of SIRT1-PGC1alpha complex. J. Biol. Chem. 2013, 288, 7117–7126. [Google Scholar] [CrossRef] [Green Version]
- Bertrand, C.; Pignalosa, A.; Wanecq, E.; Rancoule, C.; Batut, A.; Deleruyelle, S.; Lionetti, L.; Valet, P.; Castan-Laurell, I. Effects of dietary eicosapentaenoic acid (EPA) supplementation in high-fat fed mice on lipid metabolism and apelin/APJ system in skeletal muscle. PLoS ONE 2013, 8, e78874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makinen, S.; Nguyen, Y.H.; Skrobuk, P.; Koistinen, H.A. Palmitate and oleate exert differential effects on insulin signalling and glucose uptake in human skeletal muscle cells. Endocr. Connect. 2017, 6, 331–339. [Google Scholar] [CrossRef] [Green Version]
- Luukkonen, P.K.; Sadevirta, S.; Zhou, Y.; Kayser, B.; Ali, A.; Ahonen, L.; Lallukka, S.; Pelloux, V.; Gaggini, M.; Jian, C.; et al. Saturated Fat Is More Metabolically Harmful for the Human Liver Than Unsaturated Fat or Simple Sugars. Diabetes Care 2018, 41, 1732–1739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Funaki, M. Saturated fatty acids and insulin resistance. J. Med. Investig. 2009, 56, 88–92. [Google Scholar] [CrossRef] [Green Version]
- Abbott, K.A.; Burrows, T.L.; Acharya, S.; Thota, R.N.; Garg, M.L. DHA-enriched fish oil reduces insulin resistance in overweight and obese adults. Prostaglandins Leukot. Essent. Fat. Acids 2020, 159, 102154. [Google Scholar] [CrossRef] [PubMed]
- Fretts, A.M.; Jensen, P.N.; Hoofnagle, A.N.; McKnight, B.; Howard, B.V.; Umans, J.; Sitlani, C.M.; Siscovick, D.S.; King, I.B.; Djousse, L.; et al. Plasma ceramides containing saturated fatty acids are associated with risk of type 2 diabetes. J. Lipid Res. 2021, 62, 100119. [Google Scholar] [CrossRef]
- Rosqvist, F.; Kullberg, J.; Stahlman, M.; Cedernaes, J.; Heurling, K.; Johansson, H.E.; Iggman, D.; Wilking, H.; Larsson, A.; Eriksson, O.; et al. Overeating Saturated Fat Promotes Fatty Liver and Ceramides Compared with Polyunsaturated Fat: A Randomized Trial. J. Clin. Endocrinol. Metab. 2019, 104, 6207–6219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, B.; Leung, J.C.K.; Chan, L.Y.Y.; Yiu, W.H.; Tang, S.C.W. A global perspective on the crosstalk between saturated fatty acids and Toll-like receptor 4 in the etiology of inflammation and insulin resistance. Prog. Lipid Res. 2020, 77, 101020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Subjects, number | 403 |
| Female, number (%) | 230 (57) |
| Age (years) | 66 ± 5 |
| Systolic blood pressure (mmHg) | 138 ± 19 |
| Diastolic blood pressure (mmHg) | 85 ± 10 |
| Body mass index (kg/m2) | 26.5 ± 3.7 |
| Waist circumference (cm) | 92.1 ± 10.3 |
| Fat-free mass (%) | 64.6 ± 6.6 |
| Fat-free mass (kg) | 46.2 ± 9.3 |
| Fat mass (%) | 35.4 ± 6.6 |
| Fat mass (kg) | 25.5 ± 7.2 |
| Muscle mass (kg) | 28.8 ± 6.5 |
| Glucose (mg/dL) | 96.3 ± 10.6 |
| Insulin (U/L) | 9.0 ± 5.0 |
| HOMA-IR | 2.2 ± 1.4 |
| Total cholesterol (mg/dL) | 218.8 ± 37.7 |
| HDL cholesterol (mg/dL) | 67.6 ± 17.3 |
| LDL cholesterol (mg/dL) | 131.6 ± 33.0 |
| Triglycerides (mg/dL) | 98.5 ± 42.6 |
| hsCPR (mg/dL) | 0.207 ± 0.306 |
| IL-18 (pg/mL) | 377.6 ± 139.1 |
| MetS, number (%) | 49 (12.2) |
| Subjects therapy: | |
| Antihypertensive drugs, number (%) | 109 (27) |
| Beta blockers, number (%) | 24 (6) |
| Hypolipidemic therapy, number (%) | 64 (15.9) |
| HOMA-IR | IL-18 | |||
|---|---|---|---|---|
| rho | p Value | rho | p Value | |
| Age (years) | 0.048 | 0.346 | 0.025 | 0.617 |
| Systolic blood pressure (mmHg) | 0.148 | 0.003 | 0.086 | 0.084 |
| Diastolic blood pressure (mmHg) | 0.130 | 0.010 | 0.136 | 0.006 |
| Body mass index (kg/mq) | 0.515 | <0.001 | 0.176 | <0.001 |
| Waist circumference (cm) | 0.503 | <0.001 | 0.232 | <0.001 |
| Fat-free mass (%) | −0.224 | <0.001 | 0.085 | 0.089 |
| Fat-free mass (Kg) | 0.287 | <0.001 | 0.266 | <0.001 |
| Fat mass (%) | 0.224 | <0.001 | −0.085 | 0.089 |
| Fat mass (Kg) | 0.458 | <0.001 | 0.124 | 0.013 |
| Muscle mass (Kg) | 0.304 | <0.001 | 0.292 | <0.001 |
| Glucose (mg/dL) | 0.529 | <0.001 | 0.180 | <0.001 |
| Insulin (U/L) | 0.979 | <0.001 | 0.234 | <0.001 |
| HOMA-IR | - | - | 0.247 | <0.001 |
| Total cholesterol (mg/dL) | −0.081 | 0.106 | −0.138 | 0.006 |
| LDL cholesterol (mg/dL) | −0.033 | 0.514 | −0.066 | 0.188 |
| HDL cholesterol (mg/dL) | −0.266 | <0.001 | −0.217 | <0.001 |
| Triglycerides (mg/dL) | 0.320 | <0.001 | 0.104 | 0.039 |
| IL-18 (pg/mL) | 0.247 | <0.001 | - | - |
| hsCRP (mg/L) | 0.206 | <0.001 | 0.202 | <0.001 |
| HOMA-IR | IL-18 | |||
|---|---|---|---|---|
| rho | p Value | rho | p Value | |
| Total calories (kcal/day) | −0.003 | 0.958 | 0.083 | 0.097 |
| Alcohol (kcal/day) | 0.018 | 0.724 | 0.037 | 0.462 |
| Protein (g/day) | −0.005 | 0.917 | 0.007 | 0.889 |
| Lipid (g/day) | 0.034 | 0.496 | 0.031 | 0.541 |
| Available carbohydrates (g/day) | −0.044 | 0.380 | 0.071 | 0.154 |
| Starch (g/day) | 0.070 | 0.166 | 0.061 | 0.218 |
| Total fibre (g/day) | −0.153 | 0.002 | −0.066 | 0.186 |
| Cholesterol (mg/day) | 0.114 | 0.023 | 0.051 | 0.311 |
| SFA (g/day) | 0.068 | 0.174 | 0.091 | 0.068 |
| MUFA (g/day) | −0.048 | 0.336 | −0.029 | 0.556 |
| PUFA (g/day) | −0.019 | 0.704 | −0.015 | 0.760 |
| MUFA/SFA ratio | −0.163 | 0.001 | −0.167 | 0.001 |
| PUFA/SFA ratio | −0.092 | 0.068 | −0.142 | 0.004 |
| (MUFA + PUFA)/SFA ratio | −0.166 | 0.001 | −0.169 | <0.001 |
| C20:5 EPA (g/day) | −0.094 | 0.061 | −0.100 | 0.045 |
| C22:6 DHA (g/day) | −0.128 | 0.011 | −0.137 | 0.006 |
| Omega-3/SFA ratio | −0.166 | 0.001 | −0.204 | <0.001 |
| Omega-6/Omega-3 ratio | 0.129 | 0.011 | 0.095 | 0.057 |
| Mediterranean diet adherence | −0.084 | 0.094 | −0.101 | 0.044 |
| Model | R2 | p Value Model | Predictor | Unstandardized B Coefficient | p Value |
|---|---|---|---|---|---|
| 1 | 0.257 | <0.001 | Waist circumference (cm) | 0.011 | <0.001 |
| 2 | 0.311 | <0.001 | Waist circumference (cm) | 0.010 | <0.001 |
| Triglycerides (mg/dL) | 0.270 | 0.001 | |||
| 3 | 0.334 | <0.001 | Waist circumference (cm) | 0.005 | 0.001 |
| Triglycerides (mg/dL) | 0.285 | 0.002 | |||
| IL-18 (pg/mL) | 0.017 | 0.031 |
| Model | R2 | p Value Model | Predictor | Unstandardized B Coefficient | p Value |
|---|---|---|---|---|---|
| 1 | 0.126 | <0.001 | Muscle Mass (kg) | 0.007 | <0.001 |
| 2 | 0.182 | <0.001 | Muscle Mass (kg) | 0.007 | <0.001 |
| Omega-3/SFA Ratio | −0.073 | 0.003 | |||
| 3 | 0.211 | <0.001 | Muscle Mass (kg) | 0.005 | 0.006 |
| Omega-3/SFA Ratio | 0.285 | 0.002 | |||
| HDL Cholesterol (mg/dL) | 0.017 | 0.027 | |||
| 4 | 0.239 | <0.001 | Muscle Mass (kg) | 0.006 | 0.001 |
| Omega-3/SFA Ratio | −0.069 | 0.001 | |||
| Cholesterol HDL (mg/dL) | −0.001 | 0.011 | |||
| Total Cholesterol (mg/dL) | −0.027 | 0.027 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sergi, D.; Sanz, J.M.; Lazzer, S.; Brombo, G.; Zuliani, G.; Biolo, G.; Šimunič, B.; Pišot, R.; Dalla Nora, E.; Passaro, A. Interleukin-18 Is a Potential Biomarker Linking Dietary Fatty Acid Quality and Insulin Resistance: Results from a Cross-Sectional Study in Northern Italy. Nutrients 2023, 15, 1782. https://doi.org/10.3390/nu15071782
Sergi D, Sanz JM, Lazzer S, Brombo G, Zuliani G, Biolo G, Šimunič B, Pišot R, Dalla Nora E, Passaro A. Interleukin-18 Is a Potential Biomarker Linking Dietary Fatty Acid Quality and Insulin Resistance: Results from a Cross-Sectional Study in Northern Italy. Nutrients. 2023; 15(7):1782. https://doi.org/10.3390/nu15071782
Chicago/Turabian StyleSergi, Domenico, Juana Maria Sanz, Stefano Lazzer, Gloria Brombo, Giovanni Zuliani, Gianni Biolo, Boštjan Šimunič, Rado Pišot, Edoardo Dalla Nora, and Angelina Passaro. 2023. "Interleukin-18 Is a Potential Biomarker Linking Dietary Fatty Acid Quality and Insulin Resistance: Results from a Cross-Sectional Study in Northern Italy" Nutrients 15, no. 7: 1782. https://doi.org/10.3390/nu15071782