
Recent Progress on Fructose Metabolism—Chrebp, Fructolysis, and Polyol Pathway


1
Department of Clinical Nutrition, Fujita Health University, Toyoake 470-1192, Japan
2
Food and Nutrition Service Department, Fujita Health University Hospital, Toyoake 470-1192, Japan
Nutrients 2023, 15(7), 1778; https://doi.org/10.3390/nu15071778
Submission received: 20 February 2023
/
Revised: 26 March 2023
/
Accepted: 29 March 2023
/
Published: 5 April 2023
(This article belongs to the Special Issue Fructose Metabolism and Diabetes – Where Do We Stand Now?)
{kind=link}
{kind=link}
Abstract
:Excess fructose intake is associated with obesity, fatty liver, tooth decay, cancer, and cardiovascular diseases. Even after the ingestion of fructose, fructose concentration in the portal blood is never high; fructose is further metabolized in the liver, and the blood fructose concentration is 1/100th of the glucose concentration. It was previously thought that fructose was metabolized in the liver and not in the small intestine, but it has been reported that metabolism in the small intestine also plays an important role in fructose metabolism. Glut5 knockout mice exhibit poor fructose absorption. In addition, endogenous fructose production via the polyol pathway has also received attention; gene deletion of aldose reductase (Ar), ketohexokinase (Khk), and triokinase (Tkfc) has been found to prevent the development of fructose-induced liver lipidosis. Carbohydrate response element-binding protein (Chrebp) regulates the expression of Glut5, Khk, aldolase b, and Tkfc. We review fructose metabolism with a focus on the roles of the glucose-activating transcription factor Chrebp, fructolysis, and the polyol pathway.
1. Introduction
Added sugars (free fructose, sucrose, and glucose) is the name given to sugars that are added to a food by the person or manufacturer preparing it. Added sugars are included in several processed foods, such as sugar-sweetened beverages (SSBs), candies and sugars, desserts and sweet snacks, breakfast cereals and bars, coffee and teas, high-fat- milk, and yogurts. The amount of added sugar intake is associated with the risk of obesity, tooth decay, fatty liver, cancer, and cardiovascular diseases [1,2]. The amount of added sugar intake is also associated with all-cause mortality [3]. The association with all-cause mortality was shown to be significant and dose-dependent for added sugars in beverages (soda/fruit drinks, milk-based drinks, juices, and coffee/teas) but not in solids (treats, cereals, toppings, and sauces) [3]. Indeed, a new WHO guideline recommends that adults and children reduce their daily intake of free sugars to less than 10% of their total energy intake. A further reduction to below 5% or approximately 25 grams per day would provide additional health benefits [1]. Thus, reducing the added sugar intake is beneficial for a healthy life.
Among added sugars with detrimental effects, fructose has an important role in the development of metabolic syndrome diseases [4]. Recently, endogenous fructose production via the polyol pathway has received attention [5]. Fructose is metabolized to pyruvate at a much faster rate than glucose and is used for lipogenesis and gluconeogenesis. As fructose activates carbohydrate response element-binding protein (Chrebp, also called Mlxipl), Chrebp contributes to the pathogenesis of fructose-associated obesity and fatty liver [6,7,8,9,10,11].
Former reviews focused on, especially, exogenous fructose metabolism with special reference to intestinal Chrebp [7,10,11]. However, recent studies have also focused on the relationship between the polyol pathway and fructolysis [5,12]. In this review, we will summarize the role of exogenous and endogenous fructose metabolism in regulating lipogenesis, with special refences to Chrebp (Figure 1).
2. Exogenous Fructose Metabolism and Chrebp
2.1. Fructose, a Potent Inducer of Lipogenesis
Previously, fructose was considered to be metabolized mainly in the liver; however, the plasma fructose levels are much lower than those in the portal vein and gut lumen [13,14]. Recent findings have shown that the intestine also plays an important role in fructose metabolism [15]. Recently, fructose was shown to be converted into glucose derivatives in the intestine [15]. Fructose enters the enterocytes through the fructose transporter Glut5 (Slc2a5, is converted into fructose-1-phosphate by ketohexokinase (Khk, also called fructokinase), and is then metabolized into glyceraldehyde and dihydroxyacetone phosphate (DHAP) by Aldob [4]. Aldob also catalyzes the reversible cleavage of fructose 1,6-bisphosphate (FBP) into glyceraldehyde 3-phosphate (GA3P) and DHAP [4]. Therefore, Aldob plays a key role in fructolysis and gluconeogenesis [4]. Moreover, Tkfc (triokinase and FMN cyclase) catalyzes the ATP-dependent phosphorylation of the trioses D-glyceraldehyde (GA) and dihydroxy-acetone (DHA) and the cyclizing lyase splitting of FAD (flavin adenine dinucleotide) to AMP (adenosine triphosphate) and riboflavin cyclic-4,5-phosphate (cyclic FMN or cFMN). Among these functions, GA kinase constitutes the third reaction of the Hers pathway for fructose metabolism [16]. Glut5, Khk, Aldob, and Tkfc are expressed in the intestine [17,18,19]; however, under normal feeding conditions, the fructose intake does not increase the plasma glucose levels because of suppressed gluconeogenesis. Therefore, fructose has a lower glycemic index than glucose. In contrast, intravenous or peritoneal fructose injection causes increased plasma glucose levels [20]. Interestingly, when fructose or glucose is administered, fructose disappears much more rapidly than glucose, which suggests that fructolysis occurs at a much faster rate than glycolysis [20].
Added sugars include free fructose and sucrose. Although fructose does not affect the plasma glucose levels, it potently induces de novo lipogenesis [21,22,23]. In rats, some reports have compared the potency of fructose on Chrebp transcriptional activity with that of glucose [21]. Two weeks of fructose administration increased Chrebp DNA binding by 3.9 times. In humans, some studies have reported the effects of sugar-sweetened beverages on plasma lipid levels and hepatic lipid synthesis. First, a study was performed to investigate the effect of different types of sugars in SSBs on fatty acid synthesis and oxidation in 34 healthy young men with normal body weight. The relative abundance of palmitate (16:0) and the molar fatty acid ratio of palmitate to linoleic acid (16:0 to 18:2) as markers of fatty acid synthesis were increased after a high fructose ingestion (80 g/d) and a medium fructose ingestion (40 g/d) compared with high sucrose ingestion, high glucose ingestion, or baseline levels. The fasting levels of palmitoylcarnitine, an indicator of impaired fatty acid oxidation flux, were significantly increased after high fructose and high sucrose ingestion [22]. Thus, only fructose in SSBs increases fatty acid synthesis, while fructose and sucrose suppress fatty acid oxidation. Another study also aimed to investigate whether sucrose or fructose induces fat synthesis in 94 healthy men [23]. Seven weeks of administration of SSBs containing moderate amounts of fructose, sucrose (fructose–glucose disaccharide), or glucose (80 g/day) showed that the daily intake of beverages sweetened with free fructose and fructose combined with glucose (sucrose) led to a 2-fold increase in basal hepatic palmitate synthesis compared to the control [23]. Conversely, the same amounts of glucose did not change hepatic palmitate synthesis. Among these groups, there were no differences regarding resting energy expenditure, total fat and carbohydrate oxidation, or the nonprotein respiratory quotient [23]. These results suggest that fructose and sucrose induce de novo lipogenesis much more potently than glucose.
2.2. Chrebp, a Regulator of Fructose Metabolism
Why does Chrebp regulate fructose uptake and metabolism? Carbohydrate response element-binding protein (Chrebp) has an important role in regulating Glut5, Khk, Aldob, and Tkfc expression [18,24,25]. Chrebp contains two nuclear export signals and one nuclear localization signal near the N-terminal, proline-rich domains, a basic helix–loop–helix leucine-zipper domain, and a leucine-zipper-like domain. Glucose and fructose activate Chrebp transcriptional activity and thereby glucose-regulated gene expression, such as fatty acid synthase, acetyl-CoA carboxylase, stearoyl CoA desaturase 1, and Elovl6 [26]. In the livers of Chrebp−/− mice, Glut2, Khk, and Tkfc mRNA levels were lower than those in the livers of WT mice [24]. The Glut5 and Khk genes contain carbohydrate response elements (ChoREs), that is, a Chrebp binding site, in their promoter regions [18,27]. Chrebp is abundantly expressed in the liver, kidney, intestine, muscle, adipose tissues, adrenal glands, and pancreatic β cells [24,26,28,29,30,31,32,33,34,35,36]. In the intestine, Chrebp also regulates Glut5, Khk, Aldob, and Tkfc gene expression [17,18,19]. Chrebp has two isoforms, Chrebpα and Chrebpβ [31,37,38]. Chrebpβ is much more potent than Chrebpα, and Chrebpα protein induces Chrebpβ mRNA expression [31]. The effects of ChREBPα protein on Chrebpβ mRNA induction show positive feedback, while Chrebpβ suppresses Chrebpα mRNA expression [35,37]. As Chrebpβ is a target gene for Chrebpα, Chrebpβ expression is positively correlated with Chrebp transcriptional activity [31]. However, some studies have reported that Chrebpβ is dispensable for lipogenesis. Chrebpβ-specific knockout mice have been developed. Interestingly, the lack of the Chrebpβ gene showed modest effects on gene expression in the adipose tissues and the liver [38]. Consistent with these findings, in mice fed chow and two types of high-fat diets, a lack of Chrebpβ had moderate effects on body composition and insulin sensitivity [38]. The lipid profiles of Chrebpβ−/− mice were also similar to those of WT mice [38]. These results suggested that Chrebpα rather than Chrebpβ has at least a dominant role in regulating lipid metabolism in the liver [38].
Which metabolites activate Chrebp transcriptional activity is a difficult question to answer. Chrebp activity is regulated by posttranslational modifications such as phosphorylation/dephosphorylation, acetylation, and O-GlcNAcylation [6,39]. Glucagon and AMP suppress Chrebp transcriptional activity through phosphorylation and allosteric changes in Chrebp [26,40,41,42]. In contrast, some activators exist, such as xylulose-5-phosphate (Xu-5-P) and glucose-6-phosphate (G-6-P) [43,44,45,46]. Uyeda et al. reported that Xu-5-P activates Chrebp transcriptional activity via protein phosphatase 2A (PP2A)-mediated Chrebp dephosphorylation [43]. PP2A also activates phosphofructokinase 2 (PFK2) activity via dephosphorylation [47]. PFK2 catalyzes the formation of a significant allosteric regulator, fructose-2,6-bisphosphate (Fru-2,6-P2) [48]. Fru-2,6-P2 contributes to the rate-determining step of glycolysis, as it activates the enzyme phosphofructokinase 1 in the glycolysis pathway and inhibits fructose-1,6-bisphosphatase 1 in gluconeogenesis [6]. Thus, Xu-5-P regulates both glycolysis and de novo lipogenesis through PFK2 and Chrebp dephosphorylation mediated by PP2A. Moreover, xylulokinase overexpression caused an increase in Chrebp activity by converting xylitol into Xu-5-P [46]. Last, Tkfc gene deletion suppressed fructose-mediated Chrebp activation [49]. These results suggest that xylulose-5-phosphate is an activator of Chrebp.
G-6-P is also an activator of Chrebp [44,50]. Chrebp has a binding site for G-6-P, and G-6-P may activate Chrebp through allosteric effects [50]. In Chrebp−/− mice, the intracellular G-6-P levels are increased, and G-6-P may also be an activator of Chrebp. Some studies have reported that fructose 2,6-bisphosphate is essential for the glucose-regulated gene transcription of glucose-6-phosphatase and other Chrebp target genes in hepatocytes [51]. However, it is impossible to examine the effects of G6P or Xu-5-P alone at the cellular level, since G-6-P and Xu-5-P are linked to each other, and their levels fluctuate simultaneously.
2.3. Chrebp Gene Deletion and Phenotypes
Chrebp has an important role in regulating glucose and lipid metabolism, especially lipogenesis, glycogen synthesis, and gluconeogenesis. Therefore, through the suppression of Chrebp and the reduction in fatty acid content, improvement in fatty liver is expected. Chrebp gene deletion protected ob/ob mice from fatty liver and body weight gain [52]. Ob/ob Chrebp −/− mice showed improved insulin sensitivity and liver triglyceride content [52]. However, massive glycogen accumulation was observed in ob/ob Chrebp−/− mice. Similarly, the adenoviral delivery of shRNA against Chrebp improved insulin resistance and hepatic steatosis in ob/ob mice [53]. In liver-specific Chrebp−/− mice, a high-fructose feed did not induce either body weight gain or Chrebp-targeted gene induction [24,54]. Thus, the liver Chrebp gene causes the development of fructose-induced fatty liver changes.
A high-fructose-feed in the presence of Chrebp gene deletion also caused hepatomegaly due to massive glycogen accumulation [18,54]. Interestingly, liver glycogen accumulation in Chrebp−/− mice disappeared during fasting, and liver histology showed neither inflammation nor fibrosis [55]. These responses are different from those of glycogen storage disease. Liver-type pyruvate kinase overexpression rescues liver cell damage and liver glycogen accumulation [55]. Chrebp regulates glucose 6 phosphatase catalytic subunit (G6pc) at the transcriptional level [56], but G6pc expression is not completely blunted in Chrebp−/− mice [24]. These results suggest that Lpk suppression causes decreased glycolysis instead of an increased gluconeogenic flux [55]. However, importantly, fibrosis due to massive glycogen storage was not observed. Another study reported that G6pc−/− mice showed higher Chrebp activity and increased de novo lipogenesis [57,58,59]. Chrebp suppression caused a decrease in the hepatic TG content in G6pc−/− mice but accelerated liver glycogen accumulation and lowered the plasma glucose levels [58,59]. These results suggest the essential role of the Chrebp/G6pc couple and lipogenesis in maintaining liver homeostasis by preventing glycogen-induced hepatomegaly [58,59]. However, the degree of inflammation and fibrosis was much less impressive, considering that in humans, type 1 glycogenic disease can lead to cirrhosis of the liver [60]. Interestingly, some groups have reported the protective role of Chrebp in fructose-mediated steatosis [61]. In Chrebp−/− mice, a high-fructose diet reduced the levels of molecular chaperones and activated the C/EBP homologous protein-dependent (CCAAT enhancer-binding protein homologous protein (CHOP)-dependent) unfolded protein response [61]. Moreover, a high-fructose diet induced cholesterol synthesis due to sterol regulatory element-binding protein 2 (Srebp2) activation. The liver free cholesterol, but not total cholesterol, was higher in fructose diet-fed Chrebp−/− mice [56]. Thus, Chrebp provides hepatoprotection against a high-fructose diet by preventing the overactivation of cholesterol biosynthesis and the subsequent CHOP-mediated, proapoptotic unfolded protein response [61]. It is an interesting idea that Chrebp may protect against fructose-mediated liver damage. However, some questions remain. Why does Chrebp gene deletion activate SREBP2 transcriptional activity in high-fructose-feed conditions? Why is the free cholesterol content higher in fructose-fed Chrebp−/− mice? Why do fructose-fed Chrebp−/− mice not show severe inflammation or fibrosis despite increased glycogen accumulation and free cholesterol content? The relationship between cholesterol metabolism and Chrebp may be unclear. Thus, Chrebp gene deletion has both beneficial effects (lowering the liver triacylglycerol content) and harmful effects (increasing the glycogen content and free cholesterol) in relation to fructose toxicity.
As another characteristic, in both global and intestinal Chrebp−/− mice, only 7 days of sucrose administration caused cecal enlargement, diarrhea, and body weight loss [17]. The simple fructose administration also caused similar phenotypes in Chrebp−/− mice [18,19]. Moreover, sucrose or fructose feeding was lethal to Chrebp−/− mice [17,18,19]. Considering that fructose malabsorption does not cause lethality, high-fructose-fed Chrebp−/− mice are a model for not only fructose malnutrition but also hereditary fructose intolerance, which is a life-threatening disease. Moreover, intestine-specific Chrebp−/− mice showed fructose intolerance. Therefore, intestinal Chrebp has an important role in fructose absorption (Figure 2). Moreover, in the liver, fructose is metabolized into glucose and acetyl coA and thereby used for de novo lipogenesis and glucose output. In the liver, Chrebp regulates not only olfactory fructolytic enzymes but also lipogenic and gluconeogenic enzymes at the transcriptional level [24,25]. Indeed, the changes in fructose concentrations after fructose loading in the portal vein are much larger than those in the peripheral vein in sucrose-fed rats [13,62]. Moreover, after intraperitoneal fructose injection, the hepatic fructose content in Chrebp−/− mice was much higher than in WT mice. Thus, Chrebp also has an important role in liver fructose metabolism. In the kidney, fructose is reabsorbed from urine [63]. In seminal vesicles, fructose is endogenously synthesized via the polyol pathway and secreted [64]. It is the major carbohydrate source in seminal plasma and is essential for normal sperm motility [65]. In fact, the fructose concentration in the seminal fluid was found to be as high as 15 mM. Chrebp is also expressed in the testis, but Chrebp−/− mice are normally fertile. Further investigation will be needed to clarify the relationship between fructose metabolism and Chrebp in these tissues.
2.4. Phenotypes Induced by Glut5, Khk, Aldob, and Triokinase Mutations
Glut5 is the primary transporter responsible for the facilitative absorption of fructose. Glut5 is expressed in the small intestine (duodenum), testis, and kidney to a lesser extent. Sugars and cAMP induce Glut5 expression [66,67]. Chrebp binding sites are found in the Glut5 promoter, and Chrebp gene deletion causes decreased Glut5 expression [17,18,19]. Moreover, the posttranscriptional regulation of human GLUT5 by fructose involves increases in mRNA stability mediated by the cAMP pathway and Paip2 (PABP-interacting protein 2) binding [68]. Human GLUT5 expression can also be induced by thyroid hormone (triiodothyronine, T3) and glucocorticoids through the activation of the thyroid hormone receptor (THR) and the glucocorticoid receptor (GR), respectively [69]. Recently, LXR was reported to induce human GLUT5 expression [70]. Glucose and thyroid hormone, as well as glucose and cAMP, coregulate the expression of the intestinal fructose transporter GLUT5 [69]. The human GLUT5 gene was cloned in a patient with isolated fructose malabsorption; however, the human GLUT5 mutation did not contribute to acquired fructose malabsorption [71]. Glut5−/− mice fed a normal diet had normal blood pressure and displayed a normal weight gain. In contrast, a high-fructose diet caused hypotension and massive dilatation of the cecum and colon due to fructose malabsorption [72]. Moreover, Glut5−/− mice exhibited no facilitative fructose transport and no compensatory increases in the activity and expression of Sglt1 and other glucose transporters [72]. Consistent with these findings, fructose could not upregulate Glut5 in Khk−/− mice. These results are consistent with the finding that glucose derivatives induce Glut5 gene expression via Chrebp activation.
Khk is an enzyme that catalyzes the phosphorylation of fructose to produce fructose-1-phosphate [73,74]. A human KHK gene mutation causes only essential fructosuria [73,74,75,76]. In patients with Khk gene mutations, ingested fructose is partly (10–20%) excreted in urine, and the rest is slowly metabolized by an alternative pathway, namely, it is converted into fructose-6-phosphate by hexokinase in the adipose tissue and muscle [73,74,75,76]. The mode of inheritance is autosomal recessive, and the homozygote frequency has been estimated at 1:130,000. Interestingly, an intravenous fructose injection causes no hepatic metabolic changes (phosphomonoester, ATP, and Pi) in patients with essential fructosuria [77]. Thus, essential fructosuria is a harmless anomaly characterized by the appearance of fructose in the urine after the intake of fructose-containing food.
In mice, Khk gene suppression may also be beneficial for liver steatosis and hyperuricemia. However, the suppression of the polyol pathway does not improve glucose clearance and partly decreases glucose clearance. Moreover, after glucose feeding, Khk-A/C suppression did not improve either insulin tolerance or HbA1c levels [78]. However, excess fructose intake will increase the plasma fructose levels and the accumulation of advanced glycation end products (AGEs) because fructose-derived AGEs may be involved via the Maillard reaction, and fructose is 10 times more reactive than glucose, although the plasma fructose concentration is only 1% of that of glucose [79]. If the plasma fructose levels continue to increase, fructose-derived AGEs are increased and may cause cell damage due to intracellular AGEs in vascular cells [79]. Although Khk deficiency is a benign disease that causes fructosuria, it is expected that the continuous intake of excess fructose can lead to hyperfructosemia, a health problem caused by protein glycation, as seen in diabetes mellitus patients.
Aldob plays a key role in both glycolysis and gluconeogenesis. A human ALDOB gene mutation causes hereditary fructose intolerance [75,80,81]. Fructose intolerance presents with abdominal pain, nausea, and hypoglycemia symptoms, as well as shock-like syndrome after fructose ingestion [80]. The incidence of hereditary fructose intolerance, which is an autosomal recessive disease, is estimated to be 1 in 20,000 to 30,000 individuals each year worldwide. A lack of Aldob results in the accumulation of fructose-1-phosphate (F-1-P) in liver and renal cells. F-1-P is toxic and causes cell damage. As Aldob regulates fructolysis (energy production) and gluconeogenesis, Aldob gene deletion causes decreased cellular energy, low blood sugar levels, renal tubular acidosis, and severe liver dysfunction. Thus, in hereditary fructose intolerance, fructose may provoke prompt gastrointestinal discomfort and hypoglycemia upon ingestion. Fructose-fed Aldob−/− mice showed similar phenotypes to humans [80]. Interestingly, some studies reported that Aldob gene depletion promotes hepatocellular carcinogenesis by activating insulin receptor signaling and lipogenesis [81]. Another group also reported that hepatic Aldob gene deletion activates Akt and promotes hepatocellular carcinogenesis by destabilizing the Aldob/Akt/PP2A protein complex. These results are consistent with the inverse correlation between Aldob and p-Akt expression in human HCC tissues [82].
Triokinase/FMN cyclase is an enzyme that in humans is encoded by the TKFC gene [83]. This is a homodimeric protein with subunits containing two domains (K and L domains or N-terminal and C-terminal). Both domains are needed for triokinase activity, while the L domain suffices for FMN cyclase activity [83]. Triokinase and FMN cyclase (TKFC) encode a bifunctional enzyme involved in fructose metabolism through its glyceraldehyde kinase activity and in the generation of riboflavin cyclic 4′,5′-phosphate (cyclic FMN) [83].
Triokinase and FMN cyclase deficiency syndrome (TKFCD) is a multisystem disease. In addition to cataracts and developmental delays of varying severity, other features include liver dysfunction, microcytic anemia, and cerebellar hypoplasia [84]. Fatal cardiomyopathy with lactic acidosis has been observed. These phenotypes are due to the biallelic mutations c.1628G>T or c.1333G>A in the C-terminal region. In contrast, biallelic mutations of the N-terminal domain caused only hypotrichosis [85]. A patient with both c.574G>C and c.682C>T mutations showed hypotrichosis, while the patient’s father and mother with heterogenous mutations of either c.574G>C or c.682C>T did not show hypotrichosis [85]. These results indicate that TKFC functions as a homodimer and that patients with genetic mutations in the C-terminal domain show more severe phenotypes.
In Tkfc−/− mice, fructose diets cause diarrhea and cecal enlargement, which is consistent with the fructose malabsorption phenotypes observed in Glut5−/− and Chrebp−/− mice [50]. High fructose diet-induced hepatic lipogenesis and steatosis were effectively reduced by Tkfc knockdown [50]. Interestingly, triokinase gene deletion suppressed Chrebp transcriptional activity. Moreover, the highly prevalent human variant Ala185Thr-TKFC has been reported to be ‘null’ for fructose metabolism, since Ala185-TKFC rescues the mouse TKFC-deficient phenotype, whereas Ala185Thr-TKFC does not. In contrast, Thr185-TKFC is actually fully active as a triokinase/FMN cyclase, and a yeast growth assay revealed that Ala185-TKFC and Ala185Thr-TKFC overexpression rescued growth in Δdak1 yeast cells. These results suggest that human Thr185-TKFC cannot be considered a ‘null’ variant in terms of triokinase activity [86].
2.5. Comparison between Chrebp−/− and Fructose-Regulated Gene Knockout Mice
Chrebp regulates Glut5, Khk, Aldob, and Tkfc expression [17,18,19,24], and Chrebp gene deletion is predicted to worsen fructose insufficiency. Gene deletion of ketohexokinase (Khk), an enzyme upstream of Aldob, is sufficient to prevent hypoglycemia and liver and intestinal injury associated with feeding Aldob−/− mice fructose [80]. Moreover, only Khkc suppression rescued the phenotypes of hereditary fructose intolerance in fructose-fed Aldob−/− mice [80]. Considering that the phenotypes associated with alterations of downstream enzymes (Aldob and Tkfc) are more life-threatening than those associated with Glut5 and Khk alteration, decreased Khk and Glut5 expression may alleviate fructose insufficiency due to Aldob or Tkfc suppression. However, fructose-fed Chrebp−/− mice showed lethality, and the effects of Khk and Glut5 may be limited. Thus, as Chrebp gene deletion suppresses multiple fructolytic steps, Chrebp gene deletion led to a phenotype characterized by both fructose malabsorption and fructose intolerance.
2.6. Other Transcription Factors (ATF3, Srebp1c, AhR) and Fructose
Activating transcription factor 3 (ATF3) is a member of the ATF/cAMP responsive element-binding protein family of transcription factors with the basic region leucine zipper (bZip) DNA-binding domain [87]. In combination with a homodimer and various heterodimers with other bZip proteins, such as ATF2, c-Jun, JunB, and JunD, ATF3 can function as a transcriptional activator or repressor [87]. Some studies have reported the role of ATF3 in the pathogenesis of metabolic syndrome induced by a high-fructose diet. ATF3 KO in mice increased the serum levels of glucose, insulin, triglycerides, and inflammation markers (tumor necrosis factor-alpha and intercellular adhesion molecule-1), with increased visceral adiposity [87]. ATF3 gene deletion did not ameliorate the metabolic parameters or inflammatory cytokines. The authors concluded that ATF3 deficiency is involved in the pathogenesis of metabolic syndrome. However, the changes in ATF3 activity in metabolic syndrome remain unclear [87]. Srebp1c is also a transcription factor that regulates lipogenic gene expression in the liver [88]. Fructose induces Srebp1c mRNA levels in a time-dependent manner, but the time course changes in Srebp1c mRNA induced by fructose are different from those induced by glucose. In insulin-deficient streptozotocin-injected mice, fructose also increases Srebp1c mRNA levels [88]. These results suggest that fructose also activates the transcription factor sterol regulatory element-binding protein 1c (Srebp-1c), independent of insulin action [88]. Pgc-1β is a coactivator of SREBP1c [88]. The administration of antisense oligonucleotide against Pgc-1β mRNA improved the phenotypes (hepatic lipid synthesis, hepatic glucose production) caused by a high-fructose diet, which was due to reduced Srebp1c expression [89]. Another study reported that feeding fructose-containing water caused an increase in Srebp1c mRNA levels in the hypothalamus of Wistar rats [90]. Thus, the relationship between Srebp1c and fructose intake is observed in several tissues. Aryl hydroxycarbon receptor (AhR) functions primarily as a sensor of xenobiotic chemicals and as a regulator of enzymes such as cytochrome P450s that metabolize these chemicals [91]. Interestingly, some studies have reported that xenobiotic signaling pathways are interlinked with fructose consumption. Fructose suppressed AhR signaling by modulating the expression of transcription factors (AhR nuclear translocator) and upstream regulators (Ncor2 and Rb1) [91]. As a result, fructose suppressed biotransformation gene expression (Cyp1a2, Ugt1a1, Nqo1, and Gsts). Considering that Chrebp is a negative regulator of ARNT/HIF-1β gene expression in pancreatic islet β-cells [92], fructose may also inhibit AhR expression via Chrebp activation in the liver.
3. Endogenous Fructose Production
3.1. The Polyol Pathway and Endogenous Fructose Production
When the glucose levels become greatly elevated, other pathways are upregulated. These pathways include the glycation pathway, the hexosamine pathway, the protein kinase C pathway, the alpha-ketoaldehyde pathway, and the sorbitol pathway [93,94,95].
The polyol pathway converts excess glucose into sorbitol and fructose. In diabetic conditions, the polyol pathway is activated and accelerates diabetic microvascular complications such as diabetic neuropathy [93,94,95]. Under normal conditions, the polyol pathway has a low flux because Ar has higher KM for glucose, and the conversion of glucose into sorbitol requires high glucose concentrations. The polyol pathway contains two enzymes, aldose reductase and sorbitol dehydrogenase [93,94,95].
3.2. Findings in Sorbitol Dehydrogenase Knockout Mice
Sorbitol dehydrogenase is expressed in only limited tissues, such as the ovaries, seminal vesicles, liver, kidney, and lens, and is not expressed in the retina or Schwann cells. Recently, Sano et al. reported that gene deletion of sorbitol dehydrogenase (Sord) caused a decrease in glucose-induced Chrebp nuclear translocation in the liver, while the effect of fructose on Chrebp nuclear translocation was preserved in Sord−/− mice [96]. Sord−/− mice are glucose-intolerant, which reveals that the glucose flux partly bypasses the glycolytic pathway into polyol pathways [96]. Despite these interesting results, we should interpret the data cautiously because much of the fructose injected is converted into glucose and its derivatives in the intestine. Therefore, the effect of glucose and fructose on Chrebp nuclear translocation using isolated primary hepatocytes should be examined. Moreover, although the nuclear translocation of Chrebp was suppressed, the triacylglycerol levels were unchanged, and the authors did not show the effect of Chrebp-targeted gene expression [96]. These results suggested that glucose fluctuation by the polyol pathway is transient and that the effect of the polyol pathway on Chrebp activation may also be transient. However, persistent hyperglycemia may increase the contribution of the polyol pathway to Chrebp activation because persistent hyperglycemia causes increased NADPH production via the pentose phosphate shunt (Figure 1).
3.3. Findings in Aldose Reductase Knockout Mice
Aldose reductase (Ar) is a rate-limiting enzyme in the polyol pathway. When feeding a glucose solution, Ar protein density was increased 1.5-fold, but Ar (Akr1b1) mRNA levels were unchanged [97]. Consistently, the sorbitol and fructose levels also increased. In Ar−/− mice, glucose solution feeding prevented body weight gain and hepatic lipid accumulation compared with WT mice [97]. However, glucose feeding did not affect insulin tolerance, and the plasma glucose levels were also higher. These results suggest that Ar inhibition does not improve glucose tolerance.
In contrast, the relationship between liver disease and Ar is controversial. Some authors reported that Ar protein expression was significantly higher in genetically obese mice with leptin receptor mutation, db/db mice, fed a methionine–choline-deficient (MCD) diet than in mice fed a control diet [98]. Ar gene silencing decreased the levels of serum alanine aminotransferase and hepatic lipoperoxides, reduced the mRNA and protein expression of hepatic cytochrome P450 2E1 (CYP2E1), and decreased the mRNA expression of proinflammatory tumor necrosis factor-a (TNF-a) and interleukin-6 (IL-6) [98]. A relationship between alcoholic fatty liver and aldose reductase has been reported. Alcohol ingestion induces Ar mRNA expression in the liver. Zopolrestat, an AR-specific inhibitor, improved ethanol-induced steatosis and hepatic oxidative stress by suppressing adenosine monophosphate-activated protein kinase (AMPK) activation and Srebp1c expression in C57BL/6J mice and HepG2 cells [99,100]. Inconsistent with these data, others have reported that epalrestat (EPS), an aldose reductase inhibitor, increased oxidative stress, as indicated by the increased expression of manganese superoxide dismutase (heme oxygenase-1 and NAD(P)H quinone oxidoreductase-1)-induced inflammation, and the infiltration of inflammatory cells and induced the expression of tumor necrosis factor-alpha, CD11b, and CD11c, leading to fibrosis in mouse liver [101]. Further investigation should be conducted to clarify the relationship between Ar and liver dysfunction. Moreover, the relationship between Chrebp and Ar has not been reported. While chronic alcohol consumption induces Chrebp activity through dephosphorylation [102], binge drinking induces Chrebp through acetylation [103]. Since alcohol ingestion induces Ar mRNA expression in the liver, Ar inhibition may also suppress Chrebp activation. The relationship between Ar and liver diseases remains unclear.
3.4. The Polyol Pathway and Endogenous Fructose Metabolism
Some groups have mentioned that the polyol pathway in the kidney plays an important role in kidney disease. Their hypothesis is based on the activation of the polyol pathway, as evidenced by high levels of aldose reductase, sorbitol, and endogenous fructose. The plasma fructose levels (10 μM) are much lower than the plasma glucose levels (5~10 mM) [104]. Considering that fructose is converted into glucose in the intestine and that the portal fructose levels are much lower than the glucose levels, hepatic endogenous fructose production via the polyol pathway may be an attractive candidate as the causative pathway of obesity, fatty liver, and hyperuricemia in patients consuming excess sugar-sweetened beverages. However, the role of the polyol pathway in the liver is not yet well studied [5]. Lanaspa et al. reported interesting findings, showing that Khk gene deletion prevented glucose-induced body weight gain and hepatic lipid accumulation [97]. Despite Khk suppression in Khk−/− mice, the hepatic fructose content in Khk−/− mice fed glucose were similar to those in WT mice. However, the fatty acid synthase and ATP citrate lyase levels in Khk−/− mice were similar to those in WT mice. These results are not consistent with those of another paper showing that uric acid activated ChREBP through Khk induction [105]. Moreover, gene deletion of aldose reductase also prevented glucose-induced body weight gain and fatty liver development [89]. The effects of Ar gene suppression on body weight gain and hepatic liver accumulation seem to be superior to those of Khk gene suppression. Considering that Ar is a first step in the polyol pathway, Ar gene suppression may be more effective as anti-obesity therapy than Khk suppression.
Sanchez-Lozada et al. also reported that uric acid activates Ar [105]. However, the sorbitol and fructose content in HepG2 cells also increased despite increased Khk activity. They also reported that uric acid stimulates Khk activity and fructose metabolism through Chrebp activation. Moreover, they speculated that uric acid could increase Chrebp activity through Khk activation. However, the increase in Khk levels was very low, so the contribution of uric acid to Chrebp-mediated Khk induction may be low, and its clinical significance seems to be minimal [105]. Taken together with the findings on the sorbitol and fructose content, these results suggest that the potency of Khk activated by uric acid is lower than that of aldose reductase in HepG2 cells, which is why sorbitol and fructose accumulate in HepG2 cells [97]. If the authors had used primary hepatocytes, their results could have been different and more convincing, because Chrebp activation in HepG2 cells is much weaker than in primary hepatocytes. In obese patients, overproduction and hyposecretion of uric acid vary. Moreover, uric acid levels are generally decreased during the development of diabetes mellitus, and this mechanism may be active only in the glucose intolerance stage, when urinary glucose and uric acid excretion is not increased.
Considering that aldose reductase, sorbitol dehydrogenase, and ketohexokinase are highly expressed in the liver, it is an interesting idea that uric acid promotes the polyol pathway and endogenous fructose production. Further investigation will be needed to clarify the role of the hepatic polyol pathway and endogenous fructose production in hyperuricemia.
3.5. Effects of Suppressing the Polyol Pathway on Glucose Tolerance
As the polyol pathway is a bypass to deal with excess glucose, the polyol pathway can be described as a pathway that allows excess incoming glucose to escape through the bypass, so that glucose that is not fully taken up remains in the blood and hyperglycemia can occur. Indeed, Sord−/− mice showed glucose intolerance. Therefore, it is very important to note that the endogenous fructose production pathway via the polyol pathway does not necessarily improve glucose tolerance.
4. Conclusions
The recent findings on exogenous and endogenous fructose metabolism are very interesting topics. Although the relationship between fructose intake and various metabolic diseases has been reported, the fact that the small intestine acts as a fructose barrier and that fatty liver occurs despite a low fructose concentration in the portal vein after fructose loading suggests the role of metabolites such as pyruvate, which is metabolized from fructose in the small intestine. It may be necessary to investigate the role of metabolites such as pyruvate that are generated from fructose in the small intestine. Furthermore, the role of the endogenous fructose pathways, including the polyol pathway, may also be important when excessive glucose is ingested. The relationship between fructose intake and metabolic diseases is still largely unknown. Further research is needed to elucidate the molecular mechanisms of fructose intake-induced diseases, as this is important not only for drug development but also for patient education.
Funding
This research was funded by THE PUBLIC FOUNDATION OF ELIZABETH ARNOLD- FUJI (2022), the Japan Diabetes Society Carrier Development Award supported by Sanofi (2022–2024), and the Japan Society for the Promotion of Science KAKENHI Grant Number 20K11645.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO Guidelines. Available online: https://www.who.int/news/item/04-03-2015-who-calls-on-countries-to-reduce-sugars-intake-among-adults-and-children (accessed on 5 February 2023).
- Dietary Guidelines Advisory Committee. Scientific Report of the 2020 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Agriculture and the Secretary of Health and Human Services. US Department of Agriculture; Agricultural Research Service: Washington, DC, USA, 2020.
- Kaiser, A.; Schaefer, S.; Behrendt, I.; Eichner, G.; Fasshauer, M. Association of all-cause mortality with sugar intake from different sources in the prospective cohort of UK Biobank participants. Br. J. Nutr. 2022, 62, 727–738. [Google Scholar] [CrossRef]
- Jung, S.; Bae, H.; Song, W.S.; Jang, C. Dietary Fructose and Fructose-Induced Pathologies. Annu. Rev. Nutr. 2022, 42, 45–66. [Google Scholar] [CrossRef]
- Hotta, N.; Kawamura, T.; Umemura, T. Does the breakdown of the detoxification system for aldehydes as a result of aldose reductase upregulation lead to alcohol-induced liver injury in humans and mice? J. Diabetes Investig. 2020, 11, 1426–1430. [Google Scholar] [CrossRef] [PubMed]
- Uyeda, K. Short- and Long-Term Adaptation to Altered Levels of Glucose: Fifty Years of Scientific Adventure. Annu. Rev. Biochem. 2021, 90, 31–55. [Google Scholar] [CrossRef] [PubMed]
- Iizuka, K. The Roles of Carbohydrate Response Element Binding Protein in the Relationship between Carbohydrate Intake and Diseases. Int. J. Mol. Sci. 2021, 22, 12058. [Google Scholar] [CrossRef]
- Parlati, L.; Régnier, M.; Guillou, H.; Postic, C. New targets for NAFLD. JHEP Rep. 2021, 3, 100346. [Google Scholar] [CrossRef] [PubMed]
- Herman, M.A.; Birnbaum, M.J. Molecular aspects of fructose metabolism and metabolic disease. Cell Metab. 2021, 33, 2329–2354. [Google Scholar] [CrossRef]
- Iizuka, K. The Role of Carbohydrate Response Element Binding Protein in Intestinal and Hepatic Fructose Metabolism. Nutrients 2017, 9, 181. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Cha, J.Y. Recent insights into the role of ChREBP in intestinal fructose absorption and metabolism. BMB Rep. 2018, 51, 429–436. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.J.; Stenvinkel, P.; Andrews, P.; Sánchez-Lozada, L.G.; Nakagawa, T.; Gaucher, E.; Andres-Hernando, A.; Rodriguez-Iturbe, B.; Jimenez, C.R.; Garcia, G.; et al. Fructose metabolism as a common evolutionary pathway of survival associated with climate change, food shortage and droughts. J. Intern. Med. 2020, 287, 252–262. [Google Scholar] [CrossRef] [Green Version]
- Laughlin, M.R. Normal roles for dietary fructose in carbohydrate metabolism. Nutrients 2014, 6, 3117–3129. [Google Scholar] [CrossRef] [Green Version]
- Patel, C.; Sugimoto, K.; Douard, V.; Shah, A.; Inui, H.; Yamanouchi, T.; Ferraris, R.P. Effect of dietary fructose on portal and systemic serum fructose levels in rats and in KHK−/− and GLUT5−/− mice. Am. J. Physiol. Gastrointest. Liver Physiol. 2015, 309, G779–G790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, C.; Hui, S.; Lu, W.; Cowan, A.J.; Morscher, R.J.; Lee, G.; Liu, W.; Tesz, G.J.; Birnbaum, M.J.; Rabinowitz, J.D. The Small Intestine Converts Dietary Fructose into Glucose and Organic Acids. Cell Metab. 2018, 27, 351–361.e3. [Google Scholar] [CrossRef] [Green Version]
- Sillero, M.A.; Sillero, A.; Sols, A. Enzymes involved in fructose metabolism in liver and the glyceraldehyde metabolic crossroads. Eur. J. Biochem. 1969, 10, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Iizuka, K.; Takao, K.; Horikawa, Y.; Kitamura, T.; Takeda, J. ChREBP-Knockout Mice Show Sucrose Intolerance and Fructose Malabsorption. Nutrients 2018, 10, 340. [Google Scholar] [CrossRef]
- Kim, M.; Astapova, I.I.; Flier, S.N.; Hannou, S.A.; Doridot, L.; Sargsyan, A.; Kou, H.H.; Fowler, A.J.; Liang, G.; Herman, M.A. Intestinal, but not hepatic, ChREBP is required for fructose tolerance. JCI Insight 2017, 2, e96703. [Google Scholar] [CrossRef] [Green Version]
- Oh, A.R.; Sohn, S.; Lee, J.; Park, J.M.; Nam, K.T.; Hahm, K.B.; Kim, Y.B.; Lee, H.J.; Cha, J.Y. ChREBP deficiency leads to diarrhea-predominant irritable bowel syndrome. Metabolism 2018, 85, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.; Drucker, W.R.; Owens, J.E.; Craig, J.W.; Woodward, H., Jr. Metabolism of intravenous fructose and glucose in normal and diabetic subjects. J. Clin. Investig. 1952, 31, 115–125. [Google Scholar] [CrossRef]
- Koo, H.Y.; Miyashita, M.; Cho, B.H.; Nakamura, M.T. Replacing dietary glucose with fructose increases ChREBP activity and SREBP-1 protein in rat liver nucleus. Biochem. Biophys. Res. Commun. 2009, 390, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Hochuli, M.; Aeberli, I.; Weiss, A.; Hersberger, M.; Troxler, H.; Gerber, P.A.; Spinas, G.A.; Berneis, K. Spinas, Kaspar Berneis, Sugar-Sweetened Beverages With Moderate Amounts of Fructose, but Not Sucrose, Induce Fatty Acid Synthesis in Healthy Young Men: A Randomized Crossover Study. J. Clin. Endocrinol. Metab. 2014, 99, 2164–2172. [Google Scholar] [CrossRef] [Green Version]
- Geidl-Flueck, B.; Hochuli, M.; Németh, Á.; Eberl, A.; Derron, N.; Köfeler, H.C.; Tappy, L.; Berneis, K.; Spinas, G.A.; Gerber, P.A. Fructose- and sucrose- but not glucose-sweetened beverages promote hepatic de novo lipogenesis: A randomized controlled trial. J. Hepatol. 2021, 75, 46–54. [Google Scholar] [CrossRef]
- Iizuka, K.; Bruick, R.K.; Liang, G.; Horton, J.D.; Uyeda, K. Deficiency of carbohydrate response element-binding protein (ChREBP) reduces lipogenesis as well as glycolysis. Proc. Natl. Acad. Sci. USA 2004, 101, 7281–7286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.; Robinson, L.N.; Towle, H.C. ChREBP*Mlx is the principal mediator of glucose-induced gene expression in the liver. J. Biol. Chem. 2006, 281, 28721–28730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, H.; Takenoshita, M.; Sakurai, M.; Bruick, R.K.; Henzel, W.J.; Shillinglaw, W.; Arnot, D.; Uyeda, K. A glucose-responsive transcription factor that regulates carbohydrate metabolism in the liver. Proc. Natl. Acad. Sci. USA 2001, 98, 9116–9121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanaspa, M.A.; Sanchez-Lozada, L.G.; Cicerchi, C.; Li, N.; Roncal-Jimenez, C.A.; Ishimoto, T.; Le, M.; Garcia, G.E.; Thomas, J.B.; Rivard, C.J.; et al. Uric acid stimulates fructokinase and accelerates fructose metabolism in the development of fatty liver. PLoS ONE 2012, 7, e47948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Wollheim, C.B. ChREBP rather than USF2 regulates glucose stimulation of endogenous L-pyruvate kinase expression in insulin-secreting cells. J. Biol. Chem. 2002, 277, 32746–32752. [Google Scholar] [CrossRef] [Green Version]
- Da Silva Xavier, G.; Rutter, G.A.; Diraison, F.; Andreolas, C.; Leclerc, I. ChREBP binding to fatty acid synthase and L-type pyruvate kinase genes is stimulated by glucose in pancreatic beta-cells. J. Lipid Res. 2006, 47, 2482–2491. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Kumar, A.; Katz, L.S.; Li, L.; Paulynice, M.; Herman, M.A.; Scott, D.K. Induction of the ChREBPβ Isoform Is Essential for Glucose-Stimulated β-Cell Proliferation. Diabetes 2015, 64, 4158–4170. [Google Scholar] [CrossRef] [Green Version]
- Herman, M.A.; Peroni, O.D.; Villoria, J.; Schön, M.R.; Abumrad, N.A.; Blüher, M.; Klein, S.; Kahn, B.B. A novel ChREBP isoform in adipose tissue regulates systemic glucose metabolism. Nature 2012, 484, 333–338. [Google Scholar] [CrossRef] [Green Version]
- Wei, C.; Wang, P.; Dong, Q.; Ma, X.H.; Lu, M.; Qi, S.; Shi, J.H.; Xie, Z.; Ren, A.J.; Zhang, W.J. ChREBP-regulated lipogenesis is not required for the thermogenesis of brown adipose tissue. Int. J. Obes. 2022, 46, 1068–1075. [Google Scholar] [CrossRef]
- Sanchez-Gurmaches, J.; Tang, Y.; Jespersen, N.Z.; Wallace, M.; Martinez Calejman, C.; Gujja, S.; Li, H.; Edwards, Y.J.K.; Wolfrum, C.; Metallo, C.M.; et al. Brown Fat AKT2 Is a Cold-Induced Kinase that Stimulates ChREBP-Mediated De Novo Lipogenesis to Optimize Fuel Storage and Thermogenesis. Cell Metab. 2018, 27, 195–209.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takao, K.; Iizuka, K.; Liu, Y.; Sakurai, T.; Kubota, S.; Kubota-Okamoto, S.; Imaizumi, T.; Takahashi, Y.; Rakhat, Y.; Komori, S.; et al. Effects of ChREBP deficiency on adrenal lipogenesis and steroidogenesis. J. Endocrinol. 2021, 248, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Iizuka, K.; Wu, W.; Horikawa, Y.; Saito, M.; Takeda, J. Feedback looping between ChREBP and PPARα in the regulation of lipid metabolism in brown adipose tissues. Endocr. J. 2013, 60, 1145–1153. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Song, S.; Yang, Z.; Wu, M.; Mu, L.; Zhou, T.; Shi, Y. ChREBP deficiency alleviates apoptosis by inhibiting TXNIP/oxidative stress in diabetic nephropathy. J. Diabetes Complicat. 2021, 35, 108050. [Google Scholar] [CrossRef]
- Jing, G.; Chen, J.; Xu, G.; Shalev, A. Islet ChREBP-β is increased in diabetes and controls ChREBP-α and glucose-induced gene expression via a negative feedback loop. Mol. Metab. 2016, 5, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Recazens, E.; Tavernier, G.; Dufau, J.; Bergoglio, C.; Benhamed, F.; Cassant-Sourdy, S.; Marques, M.A.; Caspar-Bauguil, S.; Brion, A.; Monbrun, L.; et al. ChREBPβ is dispensable for the control of glucose homeostasis and energy balance. JCI Insight 2022, 7, e153431. [Google Scholar] [CrossRef] [PubMed]
- Filhoulaud, G.; Guilmeau, S.; Dentin, R.; Girard, J.; Postic, C. Novel insights into ChREBP regulation and function. Trends Endocrinol. Metab. 2013, 24, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Jung, H.; Nakagawa, T.; Pawlosky, R.; Takeshima, T.; Lee, W.R.; Sakiyama, H.; Laxman, S.; Wynn, R.M.; Tu, B.P.; et al. Metabolite Regulation of Nuclear Localization of Carbohydrate-response Element-binding Protein (ChREBP): Role of AMP as an allosteric inhibitor. J. Biol. Chem. 2016, 291, 10515–10527. [Google Scholar] [CrossRef] [Green Version]
- Kawaguchi, T.; Osatomi, K.; Yamashita, H.; Kabashima, T.; Uyeda, K. Mechanism for fatty acid “sparing” effect on glucose-induced transcription: Regulation of carbohydrate-responsive element-binding protein by AMP-activated protein kinase. J. Biol. Chem. 2002, 277, 3829–3835. [Google Scholar] [CrossRef] [Green Version]
- Kawaguchi, T.; Takenoshita, M.; Kabashima, T.; Uyeda, K. Glucose and cAMP regulate the L-type pyruvate kinase gene by phosphorylation/dephosphorylation of the carbohydrate response element binding protein. Proc. Natl. Acad. Sci. USA 2001, 98, 13710–13715. [Google Scholar] [CrossRef] [Green Version]
- Kabashima, T.; Kawaguchi, T.; Wadzinski, B.E.; Uyeda, K. Xylulose 5-phosphate mediates glucose-induced lipogenesis by xylulose 5-phosphate-activated protein phosphatase in rat liver. Proc. Natl. Acad. Sci. USA 2003, 100, 5107–5112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.V.; Chen, W.; Harmancey, R.N.; Nuotio-Antar, A.M.; Imamura, M.; Saha, P.; Taegtmeyer, H.; Chan, L. Glucose-6-phosphate mediates activation of the carbohydrate responsive binding protein (ChREBP). Biochem. Biophys. Res. Commun. 2010, 395, 395–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dentin, R.; Tomas-Cobos, L.; Foufelle, F.; Leopold, J.; Girard, J.; Postic, C.; Ferré, P. Glucose 6-phosphate, rather than xylulose 5-phosphate, is required for the activation of ChREBP in response to glucose in the liver. J. Hepatol. 2012, 56, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Iizuka, K.; Wu, W.; Horikawa, Y.; Takeda, J. Role of glucose-6-phosphate and xylulose-5-phosphate in the regulation of glucose-stimulated gene expression in the pancreatic β cell line, INS-1E. Endocr. J. 2013, 60, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, M.; Uyeda, K. Purification and characterization of a novel xylulose 5-phosphate-activated protein phosphatase catalyzing dephosphorylation of fructose-6-phosphate,2-kinase:fructose-2,6-bisphosphatase. J. Biol. Chem. 1995, 270, 26341–26346. [Google Scholar] [CrossRef] [Green Version]
- Uyeda, K.; Furuya, E.; Luby, L.J. The effect of natural and synthetic D-fructose 2,6-bisphosphate on the regulatory kinetic properties of liver and muscle phosphofructokinases. J. Biol. Chem. 1981, 256, 8394–8399. [Google Scholar] [CrossRef]
- Liu, L.; Li, T.; Liao, Y.; Wang, Y.; Gao, Y.; Hu, H.; Huang, H.; Wu, F.; Chen, Y.G.; Xu, S.; et al. Triose Kinase Controls the Lipogenic Potential of Fructose and Dietary Tolerance. Cell Metab. 2020, 32, 605–618.e7. [Google Scholar] [CrossRef]
- McFerrin, L.G.; Atchley, W.R. A novel N-terminal domain may dictate the glucose response of Mondo proteins. PLoS ONE 2012, 7, e34803. [Google Scholar] [CrossRef]
- Arden, C.; Tudhope, S.J.; Petrie, J.L.; Al-Oanzi, Z.H.; Cullen, K.S.; Lange, A.J.; Towle, H.C.; Agius, L. Fructose 2,6-bisphosphate is essential for glucose-regulated gene transcription of glucose-6-phosphatase and other ChREBP target genes in hepatocytes. Biochem. J. 2012, 443, 111–123. [Google Scholar] [CrossRef] [Green Version]
- Iizuka, K.; Miller, B.; Uyeda, K. Deficiency of carbohydrate-activated transcription factor ChREBP prevents obesity and improves plasma glucose control in leptin-deficient (ob/ob) mice. Am. J. Physiol. Endocrinol. Metab. 2006, 291, E358–E364. [Google Scholar] [CrossRef] [Green Version]
- Dentin, R.; Benhamed, F.; Hainault, I.; Fauveau, V.; Foufelle, F.; Dyck, J.R.; Girard, J.; Postic, C. Liver-specific inhibition of ChREBP improves hepatic steatosis and insulin resistance in ob/ob mice. Diabetes 2006, 55, 2159–2170. [Google Scholar] [CrossRef] [Green Version]
- Linden, A.G.; Li, S.; Choi, H.Y.; Fang, F.; Fukasawa, M.; Uyeda, K.; Hammer, R.E.; Horton, J.D.; Engelking, L.J.; Liang, G. Interplay between ChREBP and SREBP-1c coordinates postprandial glycolysis and lipogenesis in livers of mice. J. Lipid Res. 2018, 59, 475–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, J.H.; Lu, J.Y.; Chen, H.Y.; Wei, C.C.; Xu, X.; Li, H.; Bai, Q.; Xia, F.Z.; Lam, S.M.; Zhang, H.; et al. Liver ChREBP Protects Against Fructose-Induced Glycogenic Hepatotoxicity by Regulating L-Type Pyruvate Kinase. Diabetes 2020, 69, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, K.B.; Zhang, P.; Doumen, C.; Charbonnet, M.; Lu, D.; Newgard, C.B.; Haycock, J.W.; Lange, A.J.; Scott, D.K. The promoter for the gene encoding the catalytic subunit of rat glucose-6-phosphatase contains two distinct glucose-responsive regions. Am. J. Physiol. Endocrinol. Metab. 2007, 292, E788–E801. [Google Scholar] [CrossRef] [PubMed]
- Grefhorst, A.; Schreurs, M.; Oosterveer, M.H.; Cortés, V.A.; Havinga, R.; Herling, A.W.; Reijngoud, D.J.; Groen, A.K.; Kuipers, F. Carbohydrate-response-element-binding protein (ChREBP) and not the liver X receptor α (LXRα) mediates elevated hepatic lipogenic gene expression in a mouse model of glycogen storage disease type 1. Biochem. J. 2010, 432, 249–254. [Google Scholar] [CrossRef]
- Lei, Y.; Hoogerland, J.A.; Bloks, V.W.; Bos, T.; Bleeker, A.; Wolters, H.; Wolters, J.C.; Hijmans, B.S.; van Dijk, T.H.; Thomas, R.; et al. Hepatic Carbohydrate Response Element Binding Protein Activation Limits Nonalcoholic Fatty Liver Disease Development in a Mouse Model for Glycogen Storage Disease Type 1a. Hepatology 2020, 72, 1638–1653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajas, F.; Dentin, R.; Cannella Miliano, A.; Silva, M.; Raffin, M.; Levavasseur, F.; Gautier-Stein, A.; Postic, C.; Mithieux, G. The absence of hepatic glucose-6 phosphatase/ChREBP couple is incompatible with survival in mice. Mol. Metab. 2021, 43, 101108. [Google Scholar] [CrossRef]
- Göğüş, S.; Koçak, N.; Ciliv, G.; Karabulut, E.; Akçören, Z.; Kale, G.; Cağlar, M. Histologic features of the liver in type Ia glycogen storage disease: Comparative study between different age groups and consecutive biopsies. Pediatr. Dev. Pathol. 2002, 5, 299–304. [Google Scholar] [CrossRef]
- Zhang, D.; Tong, X.; VanDommelen, K.; Gupta, N.; Stamper, K.; Brady, G.F.; Meng, Z.; Lin, J.; Rui, L.; Omary, M.B.; et al. Lipogenic transcription factor ChREBP mediates fructose-induced metabolic adaptations to prevent hepatotoxicity. J. Clin. Investig. 2017, 127, 2855–2867. [Google Scholar] [CrossRef] [Green Version]
- Sugimoto, K.; Hosotani, T.; Kawasaki, T.; Nakagawa, K.; Hayashi, S.; Nakano, Y.; Inui, H.; Yamanouchi, T. Eucalyptus leaf extract suppresses the postprandial elevation of portal, cardiac, and peripheral fructose concentrations after sucrose ingestion in rats. J. Clin. Biochem. Nutr. 2012, 46, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, T.; Johnson, R.J.; Andres-Hernando, A.; Roncal-Jimenez, C.; Sanchez-Lozada, L.G.; Tolan, D.R.; Lanaspa, M.A. Fructose Production and Metabolism in the Kidney. J. Am. Soc. Nephrol. 2020, 31, 898–906. [Google Scholar] [CrossRef] [PubMed]
- Lewis-Jones, D.I.; Aird, I.A.; Biljan, M.M.; Kingsland, C.R. Effects of sperm activity on zinc and fructose concentrations in seminal plasma. Hum. Reprod. 1996, 11, 2465–2467. [Google Scholar] [CrossRef] [Green Version]
- Buckett, W.M.; Lewis-Jones, D.I. Fructose concentrations in seminal plasma from men with nonobstructive azoospermia. Arch. Androl. 2002, 48, 23–27. [Google Scholar] [CrossRef] [Green Version]
- Mesonero, J.; Matosin, M.; Cambier, D.; Rodriguez-Yoldi, M.J.; Brot-Laroche, E. Sugar-dependent expression of the fructose transporter GLUT5 in Caco-2 cells. Biochem. J. 1995, 312 Pt 3, 757–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahraoui, L.; Takeda, J.; Mesonero, J.; Chantret, I.; Dussaulx, E.; Bell, G.I.; Brot-Laroche, E. Regulation of expression of the human fructose transporter (GLUT5) by cyclic AMP. Biochem. J. 1994, 301 Pt 1, 169–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gouyon, F.; Onesto, C.; Dalet, V.; Pages, G.; Leturque, A.; Brot-Laroche, E. Fructose modulates GLUT5 mRNA stability in differentiated Caco-2 cells: Role of cAMP-signaling pathway and PABP (polyadenylated-binding protein)-interacting protein (Paip) 2. Biochem. J. 2003, 375 Pt 1, 167–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matosin-Matekalo, M.; Mesonero, J.E.; Laroche, T.J.; Lacasa, M.; Brot-Laroche, E. Glucose and thyroid hormone coregulate the expression of the intestinal fructose transporter GLUT5. Biochem J. 1999, 339 Pt 2, 233–239. [Google Scholar] [CrossRef]
- Zwarts, I.; van Zutphen, T.; Kruit, J.K.; Liu, W.; Oosterveer, M.H.; Verkade, H.J.; Uhlenhaut, N.H.; Jonker, J.W. Identification of the fructose transporter GLUT5 (SLC2A5) as a novel target of nuclear receptor LXR. Sci. Rep. 2019, 9, 9299. [Google Scholar] [CrossRef] [Green Version]
- Taneva, I.; Grumann, D.; Schmidt, D.; Taneva, E.; von Arnim, U.; Ansorge, T.; Wex, T. Gene variants of the SLC2A5 gene encoding GLUT5, the major fructose transporter, do not contribute to clinical presentation of acquired fructose malabsorption. BMC Gastroenterol. 2022, 22, 167. [Google Scholar] [CrossRef]
- Barone, S.; Fussell, S.L.; Singh, A.K.; Lucas, F.; Xu, J.; Kim, C.; Wu, X.; Yu, Y.; Amlal, H.; Seidler, U.; et al. Slc2a5 (Glut5) is essential for the absorption of fructose in the intestine and generation of fructose-induced hypertension. J. Biol. Chem. 2009, 284, 5056–5066. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, E.L.; Saborano, R.; Northall, E.; Matsuda, K.; Ogino, H.; Yashiro, H.; Pickens, J.; Feaver, R.E.; Cole, B.K.; Hoang, S.A.; et al. Ketohexokinase inhibition improves NASH by reducing fructose-induced steatosis and fibrogenesis. JHEP Rep. 2020, 3, 100217. [Google Scholar] [CrossRef] [PubMed]
- Bonthron, D.T.; Brady, N.; Donaldson, I.A.; Steinmann, B. Molecular basis of essential fructosuria: Molecular cloning and mutational analysis of human ketohexokinase (fructokinase). Hum. Mol. Genet. 1994, 3, 1627–1631. [Google Scholar] [CrossRef] [PubMed]
- Tran, C. Inborn Errors of Fructose Metabolism. What Can We Learn from Them? Nutrients 2017, 9, 356. [Google Scholar] [CrossRef]
- Laron, Z. Essential benign fructosuria. Arch. Dis. Child. 1961, 36, 273–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boesiger, P.; Buchli, R.; Meier, D.; Steinmann, B.; Gitzelmann, R. Changes of liver metabolite concentrations in adults with disorders of fructose metabolism after intravenous fructose by 31P magnetic resonance spectroscopy. Pediatr. Res. 1994, 36, 436–440. [Google Scholar] [CrossRef]
- Lanaspa, M.A.; Andres-Hernando, A.; Orlicky, D.J.; Cicerchi, C.; Jang, C.; Li, N.; Milagres, T.; Kuwabara, M.; Wempe, M.F.; Rabinowitz, J.D.; et al. Ketohexokinase C blockade ameliorates fructose-induced metabolic dysfunction in fructose-sensitive mice. J. Clin. Investig. 2018, 128, 2226–2238. [Google Scholar] [CrossRef] [Green Version]
- Gugliucci, A. Formation of Fructose-Mediated Advanced Glycation End Products and Their Roles in Metabolic and Inflammatory Diseases. Adv. Nutr. 2017, 8, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Oppelt, S.A.; Sennott, E.M.; Tolan, D.R. Aldolase-B knockout in mice phenocopies hereditary fructose intolerance in humans. Mol. Genet. Metab. 2015, 114, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Wang, N.; Zhang, C.; Li, M.; He, X.; Yin, C.; Tu, Q.; Shen, X.; Zhang, L.; Lv, J.; et al. Fructose-1,6-Bisphosphate Aldolase B Depletion Promotes Hepatocellular Carcinogenesis Through Activating Insulin Receptor Signaling and Lipogenesis. Hepatology 2021, 74, 3037–3055. [Google Scholar] [CrossRef]
- He, X.; Li, M.; Yu, H.; Liu, G.; Wang, N.; Yin, C.; Tu, Q.; Narla, G.; Tao, Y.; Cheng, S.; et al. Loss of hepatic aldolase B activates Akt and promotes hepatocellular carcinogenesis by destabilizing the Aldob/Akt/PP2A protein complex. PLoS Biol. 2020, 18, e3000803. [Google Scholar] [CrossRef]
- Rodrigues, J.R.; Couto, A.; Cabezas, A.; Pinto, R.M.; Ribeiro, J.M.; Canales, J.; Costas, M.J.; Cameselle, J.C. Bifunctional homodimeric triokinase/FMN cyclase: Contribution of protein domains to the activities of the human enzyme and molecular dynamics simulation of domain movements. J. Biol. Chem. 2014, 289, 10620–10636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wortmann, S.B.; Meunier, B.; Mestek-Boukhibar, L.; van den Broek, F.; Maldonado, E.M.; Clement, E.; Weghuber, D.; Spenger, J.; Jaros, Z.; Taha, F.; et al. Biallelic Variants in TKFC Encoding Triokinase/FMN Cyclase Are Associated with Cataracts and Multisystem Disease. Am. J. Hum. Genet. 2020, 106, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Onoufriadis, A.; Cabezas, A.; Ng, J.C.F.; Canales, J.; Costas, M.J.; Ribeiro, J.M.; Rodrigues, J.R.; McAleer, M.A.; Castelo-Soccio, L.; Simpson, M.A.; et al. Autosomal recessive hypotrichosis with loose anagen hairs associated with TKFC mutations. Br. J. Dermatol. 2021, 184, 935–943. [Google Scholar] [CrossRef]
- Ribeiro, J.M.; Costas, M.J.; Cabezas, A.; Meunier, B.; Onoufriadis, A.; Cameselle, J.C. The TKFC Ala185Thr variant, reported as ‘null’ for fructose metabolism, is fully active as triokinase. FEBS Lett. 2022, 596, 1453–1457. [Google Scholar] [CrossRef]
- Chou, C.L.; Li, C.H.; Lin, H.; Liao, M.H.; Wu, C.C.; Chen, J.S.; Sue, Y.M.; Fang, T.C. Role of activating transcription factor 3 in fructose-induced metabolic syndrome in mice. Hypertens. Res. 2018, 41, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaka, T.; Shimano, H.; Yahagi, N.; Amemiya-Kudo, M.; Okazaki, H.; Tamura, Y.; Iizuka, Y.; Ohashi, K.; Tomita, S.; Sekiya, M.; et al. Insulin-independent induction of sterol regulatory element-binding protein-1c expression in the livers of streptozotocin-treated mice. Diabetes 2004, 53, 560–569. [Google Scholar] [CrossRef] [Green Version]
- Nagai, Y.; Yonemitsu, S.; Erion, D.M.; Iwasaki, T.; Stark, R.; Weismann, D.; Dong, J.; Zhang, D.; Jurczak, M.J.; Löffler, M.G.; et al. The role of peroxisome proliferator-activated receptor gamma coactivator-1 beta in the pathogenesis of fructose-induced insulin resistance. Cell Metab. 2009, 9, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Batista, L.O.; Ramos, V.W.; Rosas Fernández, M.A.; Concha Vilca, C.M.; Albuquerque, K.T. Oral solution of fructose promotes SREBP-1c high-expression in the hypothalamus of Wistar rats. Nutr. Neurosci. 2019, 22, 648–654. [Google Scholar] [CrossRef]
- Pan, J.H.; Tang, J.; Beane, K.E.; Redding, M.C.; Cho, Y.J.; Kim, Y.J.; Zhao, J.; Shin, E.C.; Lee, J.H.; Kong, B.C.; et al. Hepatic transcriptomics analysis reveals that fructose intervention down-regulated xenobiotics-metabolising enzymes through aryl hydrocarbon receptor signalling suppression in C57BL/6N mice. Br. J. Nutr. 2019, 122, 769–779. [Google Scholar] [CrossRef]
- Noordeen, N.A.; Khera, T.K.; Sun, G.; Longbottom, E.R.; Pullen, T.J.; da Silva Xavier, G.; Rutter, G.A.; Leclerc, I. Carbohydrate-responsive element-binding protein (ChREBP) is a negative regulator of ARNT/HIF-1beta gene expression in pancreatic islet beta-cells. Diabetes 2010, 59, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Clements, R.S., Jr. The polyol pathway. A historical review. Drugs 1986, 32 (Suppl. S2), 3–5. [Google Scholar] [CrossRef] [PubMed]
- Garg, S.S.; Gupta, J. Polyol pathway and redox balance in diabetes. Pharmacol. Res. 2022, 182, 106326. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Kapoor, A.; Bhatnagar, A. Physiological and Pathological Roles of Aldose Reductase. Metabolites 2021, 11, 655. [Google Scholar] [CrossRef]
- Sano, H.; Nakamura, A.; Yamane, M.; Niwa, H.; Nishimura, T.; Araki, K.; Takemoto, K.; Ishiguro, K.I.; Aoki, H.; Kato, Y.; et al. The polyol pathway is an evolutionarily conserved system for sensing glucose uptake. PLoS Biol. 2022, 20, e3001678. [Google Scholar] [CrossRef] [PubMed]
- Lanaspa, M.; Ishimoto, T.; Li, N.; Cicerchi, C.; Orlicky, D.J.; Ruzycki, P.; Rivard, C.; Inaba, S.; Roncal-Jimenez, C.A.; Bales, E.S.; et al. Endogenous fructose production and metabolism in the liver contributes to the development of metabolic syndrome. Nat. Commun. 2013, 4, 2434. [Google Scholar] [CrossRef] [Green Version]
- Qiu, L.; Lin, J.; Ying, M.; Chen, W.; Yang, J.; Deng, T.; Chen, J.; Shi, D.; Yang, J.Y. Aldose Reductase Is Involved in the Development of Murine Diet-Induced Nonalcoholic Steatohepatitis. PLoS ONE 2013, 8, e73591. [Google Scholar] [CrossRef]
- Shi, C.; Wang, Y.; Gao, J.; Chen, S.; Zhao, X.; Cai, C.; Guo, C.; Qiu, L. Inhibition of aldose reductase ameliorates alcoholic liver disease by activating AMPK and modulating oxidative stress and inflammatory cytokines. Mol. Med. Rep. 2017, 16, 2767–2772. [Google Scholar] [CrossRef] [Green Version]
- Qiu, L.; Cai, C.; Zhao, X.; Fang, Y.; Tang, W.; Guo, C. Inhibition of aldose reductase ameliorates ethanol-induced steatosis in HepG2 cells. Mol. Med. Rep. 2017, 15, 2732–2736. [Google Scholar] [CrossRef] [Green Version]
- Le, Y.; Chen, L.; Zhang, Y.; Bu, P.; Dai, G.; Cheng, X. Epalrestat Stimulated Oxidative Stress, Inflammation, and Fibrogenesis in Mouse Liver. Toxicol. Sci. 2018, 163, 397–408. [Google Scholar] [CrossRef]
- Liangpunsakul, S.; Ross, R.A.; Crabb, D.W. Activation of carbohydrate response element-binding protein by ethanol. J. Investig. Med. 2013, 61, 270–277. [Google Scholar] [CrossRef]
- Liangpunsakul, S. Carbohydrate-responsive element-binding protein, Sirtuin 1, and ethanol metabolism: A complicated network in alcohol-induced hepatic steatosis. Hepatology 2015, 62, 946–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douard, V.; Ferraris, R.P. Regulation of the fructose transporter GLUT5 in health and disease. Am. J. Physiol. Endocrinol. Metab. 2008, 295, E227–E237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Lozada, L.G.; Andres-Hernando, A.; Garcia-Arroyo, F.E.; Cicerchi, C.; Li, N.; Kuwabara, M.; Roncal-Jimenez, C.A.; Johnson, R.J.; Lanaspa, M.A. Uric acid activates aldose reductase and the polyol pathway for endogenous fructose and fat production causing development of fatty liver in rats. J. Biol. Chem. 2019, 294, 4272–4281. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
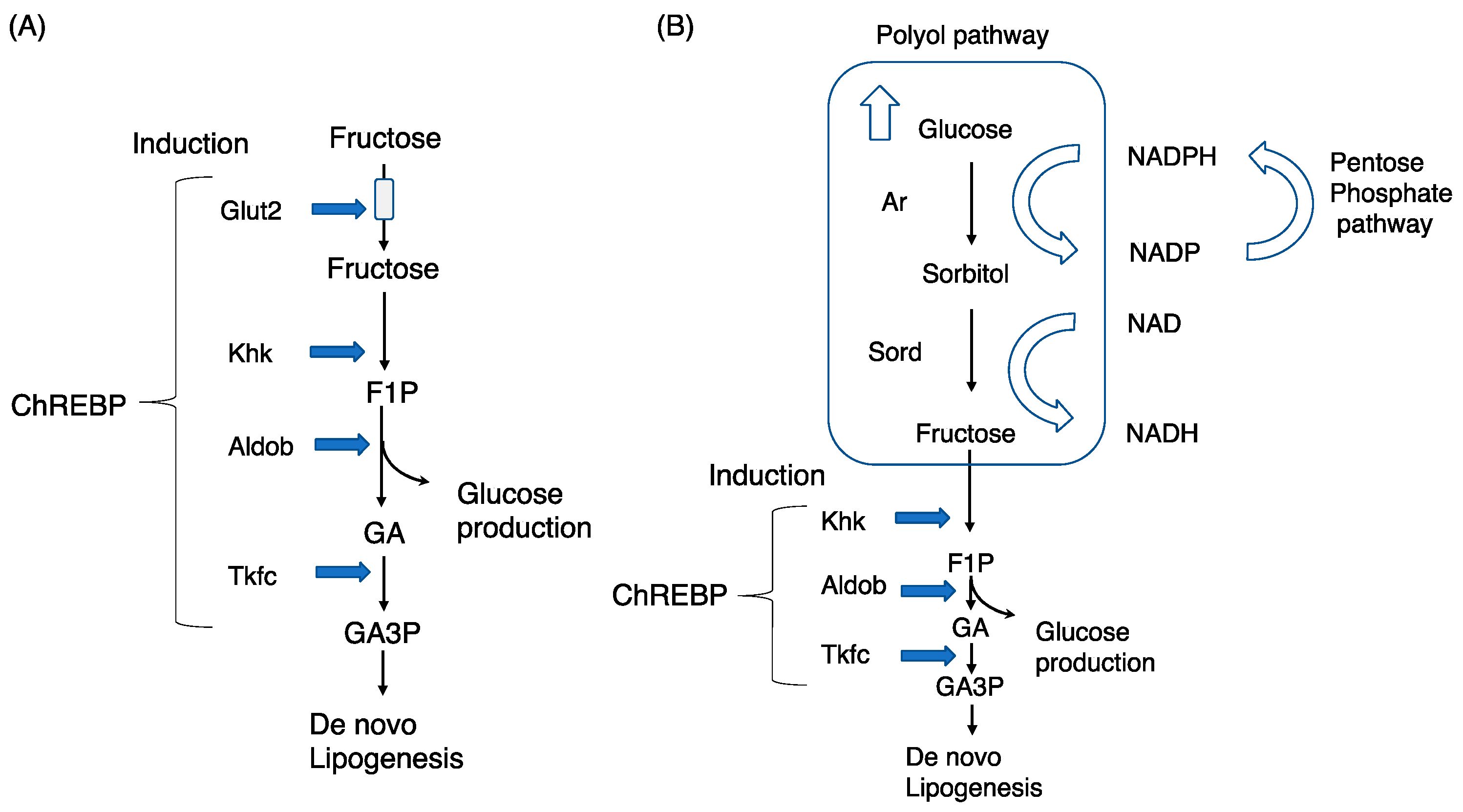
Chrebp regulates exogenous and endogenous fructose metabolism in the liver. (A) Exogenous fructose metabolism: fructose is transported into the cytosol via Glut2 (liver) and is then converted into fructose-1-phosphate (F1P), glyceraldehyde (GA), and GA3P via ketohexokinase (Khk), aldolase b (Aldob), and triokinase/FMN cyclase (Tkfc), respectively. (B) Endogenous fructose metabolism: the polyol pathway comprises aldose reductase (Ar) and sorbitol dehydrogenase (Sord). Excess glucose is converted into sorbitol and fructose via Ar and Sord, respectively. Fructose is similarly converted into F1P, GA, and GA3P.
Figure 1.
Chrebp regulates exogenous and endogenous fructose metabolism in the liver. (A) Exogenous fructose metabolism: fructose is transported into the cytosol via Glut2 (liver) and is then converted into fructose-1-phosphate (F1P), glyceraldehyde (GA), and GA3P via ketohexokinase (Khk), aldolase b (Aldob), and triokinase/FMN cyclase (Tkfc), respectively. (B) Endogenous fructose metabolism: the polyol pathway comprises aldose reductase (Ar) and sorbitol dehydrogenase (Sord). Excess glucose is converted into sorbitol and fructose via Ar and Sord, respectively. Fructose is similarly converted into F1P, GA, and GA3P.

Figure 2.
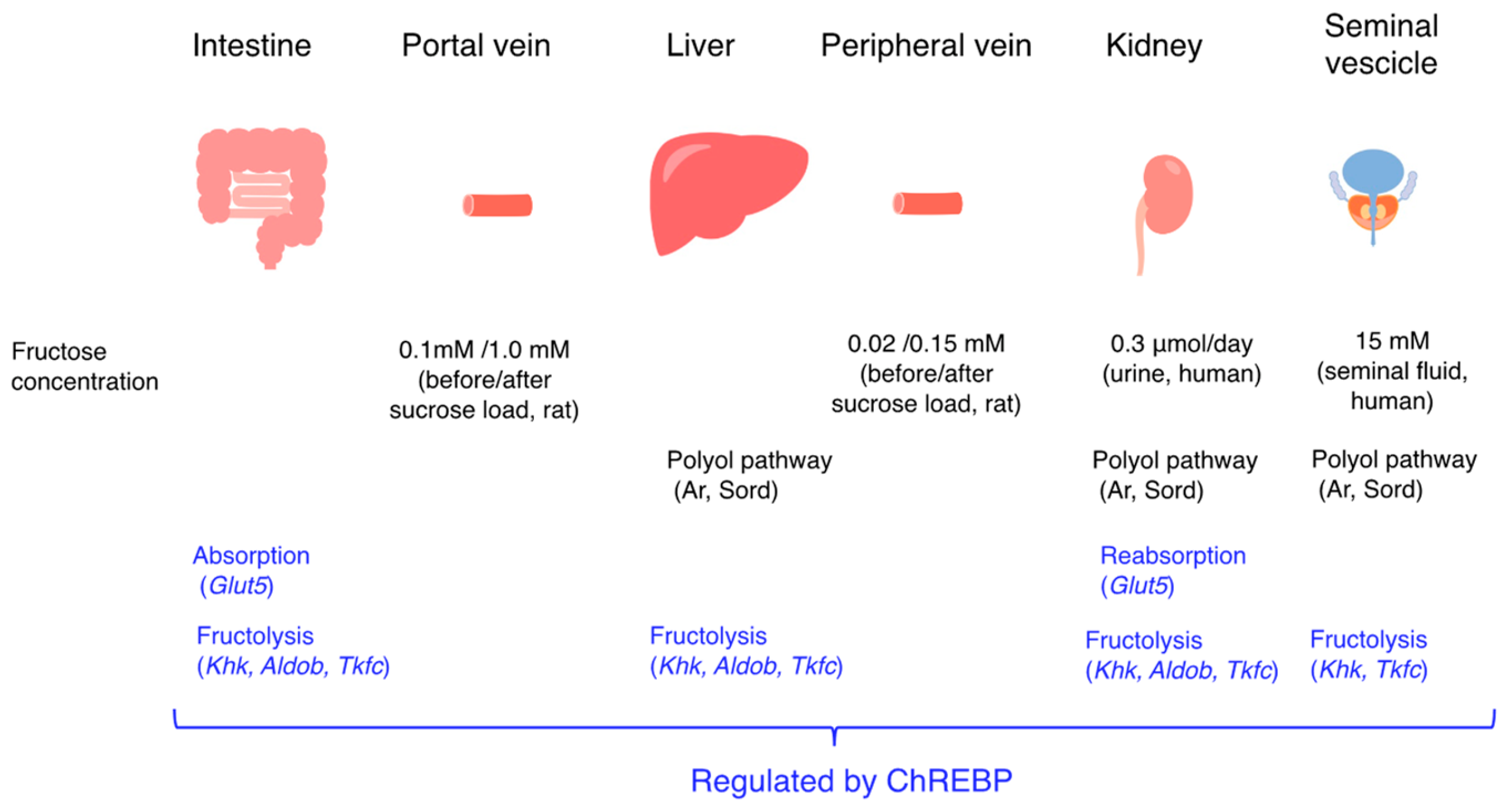
Fructose promotes intestinal and liver fructose metabolism through Chrebp activation. Chrebp regulates Glut5, Khk, and Aldob expression and then promotes intestinal fructose absorption and hepatic fructose metabolism (de novo lipogenesis and glucose production). The changes in fructose concentration in the portal vein and in the peripheral vein after sucrose loading are also indicated. Fructose concentrations in human urine and seminal fluid are also indicated. In the seminal vesicles, Aldob was not detected.
Figure 2.
Fructose promotes intestinal and liver fructose metabolism through Chrebp activation. Chrebp regulates Glut5, Khk, and Aldob expression and then promotes intestinal fructose absorption and hepatic fructose metabolism (de novo lipogenesis and glucose production). The changes in fructose concentration in the portal vein and in the peripheral vein after sucrose loading are also indicated. Fructose concentrations in human urine and seminal fluid are also indicated. In the seminal vesicles, Aldob was not detected.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Iizuka, K. Recent Progress on Fructose Metabolism—Chrebp, Fructolysis, and Polyol Pathway. Nutrients 2023, 15, 1778. https://doi.org/10.3390/nu15071778
AMA Style
Iizuka K. Recent Progress on Fructose Metabolism—Chrebp, Fructolysis, and Polyol Pathway. Nutrients. 2023; 15(7):1778. https://doi.org/10.3390/nu15071778
Chicago/Turabian StyleIizuka, Katsumi. 2023. "Recent Progress on Fructose Metabolism—Chrebp, Fructolysis, and Polyol Pathway" Nutrients 15, no. 7: 1778. https://doi.org/10.3390/nu15071778
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.