

The Importance of an Early Evaluation after Establishing a Gluten-Free Diet in Children with Celiac Disease

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Stool Collection and Analysis
2.3. Anthropometric Measures
2.4. Dietary Assessment
2.5. Statistical Analyses
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schuppan, D. Current Concepts of Celiac Disease Pathogenesis. Gastroenterology 2000, 119, 234–242. [Google Scholar] [CrossRef]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; de Giorgio, R.; Catassi, C.; Fasano, A. Celiac Disease: A Comprehensive Current Review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Carnicer, A.; Garzon-Benavides, M.; Fombuena, B.; Segura, V.; Garcia-Fernandez, F.; Sobrino-Rodriguez, S.; Gomez-Izquierdo, L.; Montes-Cano, M.A.; Rodriguez-Herrera, A.; Millan, R.; et al. Negative Predictive Value of the Repeated Absence of Gluten Immunogenic Peptides in the Urisne of Treated Celiac Patients in Predicting Mucosal Healing: New Proposals for Follow-up in Celiac Disease. Am. J. Clin. Nutr. 2020, 112, 1240–1251. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, J.A.; Jeong, J.; Underwood, F.E.; Quan, J.; Panaccione, N.; Windsor, J.W.; Coward, S.; Debruyn, J.; Ronksley, P.E.; Shaheen, A.A.; et al. Incidence of Celiac Disease Is Increasing Over Time: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2020, 115, 507–525. [Google Scholar] [CrossRef]
- Coto, L.; Sousa, C.; Cebolla, A. Individual Variability in Patterns and Dynamics of Fecal Gluten Immunogenic Peptides Excretion after Low Gluten Intake. Eur. J. Nutr. 2022, 61, 2033–2049. [Google Scholar] [CrossRef] [PubMed]
- Myléus, A.; Reilly, N.R.; Green, P.H.R. Rate, Risk Factors, and Outcomes of Nonadherence in Pediatric Patients with Celiac Disease: A Systematic Review. Clin. Gastroenterol. Hepatol. 2020, 18, 562–573. [Google Scholar] [CrossRef]
- Muhammad, H.; Reeves, S.; Jeanes, Y.M. Identifying and Improving Adherence to the Gluten-Free Diet in People with Coeliac Disease. Proc. Nutr. Soc. 2019, 78, 418–425. [Google Scholar] [CrossRef]
- Volta, U.; Caio, G.; Stanghellini, V.; de Giorgio, R. The Changing Clinical Profile of Celiac Disease: A 15-Year Experience (1998–2012) in an Italian Referral Center. BMC Gastroenterol. 2014, 14, 194. [Google Scholar] [CrossRef] [Green Version]
- El Péptido del Gluten en Heces Puede Ser Útil en el Seguimiento de la Enfermedad Celíaca—Evidencias en Pediatría. Available online: https://evidenciasenpediatria.es/articulo/7328/el-peptido-del-gluten-en-heces-puede-ser-util-en-el-seguimiento-de-la-enfermedad-celiaca?id=7328&titulo=el-peptido-del-gluten-en-heces-puede-ser-util-en-el-seguimiento-de-la-enfermedad-celiaca (accessed on 8 February 2023).
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef] [Green Version]
- Silvester, J.A.; Kurada, S.; Szwajcer, A.; Kelly, C.P.; Leffler, D.A.; Duerksen, D.R. Tests for Serum Transglutaminase and Endomysial Antibodies Do Not Detect Most Patients with Celiac Disease and Persistent Villous Atrophy on Gluten-Free Diets: A Meta-Analysis. Gastroenterology 2017, 153, 689. [Google Scholar] [CrossRef] [PubMed]
- Comino, I.; Real, A.; Vivas, S.; Síglez, M.Á.; Caminero, A.; Nistal, E.; Casqueiro, J.; Rodríguez-Herrera, A.; Cebolla, Á.; Sousa, C. Monitoring of Gluten-Free Diet Compliance in Celiac Patients by Assessment of Gliadin 33-Mer Equivalent Epitopes in Feces. Am. J. Clin. Nutr. 2012, 95, 670–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laserna-Mendieta, E.J.; Casanova, M.J.; Arias, Á.; Arias-González, L.; Majano, P.; Mate, L.A.; Gordillo-Vélez, C.H.; Jiménez, M.; Angueira, T.; Tébar-Romero, E.; et al. Poor Sensitivity of Fecal Gluten Immunogenic Peptides and Serum Antibodies to Detect Duodenal Mucosal Damage in Celiac Disease Monitoring. Nutrients 2020, 13, 98. [Google Scholar] [CrossRef] [PubMed]
- Syage, J.A.; Kelly, C.P.; Dickason, M.A.; Ramirez, A.C.; Leon, F.; Dominguez, R.; Sealey-Voyksner, J.A. Determination of Gluten Consumption in Celiac Disease Patients on a Gluten-Free Diet. Am. J. Clin. Nutr. 2018, 107, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvester, J.A.; Comino, I.; Kelly, C.P.; Sousa, C.; Duerksen, D.R.; Bernstein, C.N.; Cebolla, A.; Comino, I.; Dominguez, M.R.; Duerksen, D.R.; et al. Most Patients with Celiac Disease on Gluten-Free Diets Consume Measurable Amounts of Gluten. Gastroenterology 2020, 158, 1497–1499.e1. [Google Scholar] [CrossRef] [PubMed]
- Moreno, M.D.L.; Sánchez-Muñoz, D.; Sanders, D.; Rodríguez-Herrera, A.; Sousa, C. Verifying Diagnosis of Refractory Celiac Disease with Urine Gluten Immunogenic Peptides as Biomarker. Front. Med. 2021, 7, 601854. [Google Scholar] [CrossRef]
- Moreno, M.D.L.; Cebolla, Á.; Munõz-Suano, A.; Carrillo-Carrion, C.; Comino, I.; Pizarro, Á.; León, F.; Rodríguez-Herrera, A.; Sousa, C. Detection of Gluten Immunogenic Peptides in the Urine of Patients with Coeliac Disease Reveals Transgressions in the Gluten-Free Diet and Incomplete Mucosal Healing. Gut 2017, 66, 250–257. [Google Scholar] [CrossRef] [Green Version]
- Comino, I.; Segura, V.; Ortigosa, L.; Espín, B.; Castillejo, G.; Garrote, J.A.; Sierra, C.; Millán, A.; Ribes-Koninckx, C.; Román, E.; et al. Prospective Longitudinal Study: Use of Faecal Gluten Immunogenic Peptides to Monitor Children Diagnosed with Coeliac Disease during Transition to a Gluten-Free Diet. Aliment. Pharmacol. Ther. 2019, 49, 1484–1492. [Google Scholar] [CrossRef] [Green Version]
- Stefanolo, J.P.; Tálamo, M.; Dodds, S.; de la Paz Temprano, M.; Costa, A.F.; Moreno, M.L.; Pinto-Sánchez, M.I.; Smecuol, E.; Vázquez, H.; Gonzalez, A.; et al. Real-World Gluten Exposure in Patients with Celiac Disease on Gluten-Free Diets, Determined From Gliadin Immunogenic Peptides in Urine and Fecal Samples. Clin. Gastroenterol. Hepatol. 2021, 19, 484–491.e1. [Google Scholar] [CrossRef]
- Coto, L.; Mendia, I.; Sousa, C.; Bai, J.C.; Cebolla, A. Determination of Gluten Immunogenic Peptides for the Management of the Treatment Adherence of Celiac Disease: A Systematic Review. World J. Gastroenterol. 2021, 27, 6306–6321. [Google Scholar] [CrossRef]
- Salazar Quero, J.C.; Espín Jaime, B.; Rodríguez Martínez, A.; Argüelles Martín, F.; García Jiménez, R.; Rubio Murillo, M.; Pizarro Martín, A. Valoración Nutricional de La Dieta Sin Gluten. ¿Es La Dieta Sin Gluten Deficitaria En Algún Nutriente? An. Pediatr. 2015, 83, 33–39. [Google Scholar] [CrossRef]
- di Nardo, G.; Villa, M.P.; Conti, L.; Ranucci, G.; Pacchiarotti, C.; Principessa, L.; Raucci, U.; Parisi, P. Nutritional Deficiencies in Children with Celiac Disease Resulting from a Gluten-Free Diet: A Systematic Review. Nutrients 2019, 11, 1588. [Google Scholar] [CrossRef] [Green Version]
- Babio, N.; Alcázar, M.; Castillejo, G.; Recasens, M.; Martínez-Cerezo, F.; Gutiérrez-Pensado, V.; Masip, G.; Vaqué, C.; Vila-Martí, A.; Torres-Moreno, M.; et al. Patients with Celiac Disease Reported Higher Consumption of Added Sugar and Total Fat Than Healthy Individuals. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Zuccotti, G.; Fabiano, V.; Dilillo, D.; Picca, M.; Cravidi, C.; Brambilla, P. Intakes of Nutrients in Italian Children with Celiac Disease and the Role of Commercially Available Gluten-Free Products. J. Hum. Nutr. Diet 2013, 26, 436–444. [Google Scholar] [CrossRef]
- Gerasimidis, K.; Zafeiropoulou, K.; Mackinder, M.; Ijaz, U.Z.; Duncan, H.; Buchanan, E.; Cardigan, T.; Edwards, C.A.; McGrogan, P.; Russell, R.K. Comparison of Clinical Methods with the Faecal Gluten Immunogenic Peptide to Assess Gluten Intake in Coeliac Disease. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 356–360. [Google Scholar] [CrossRef] [Green Version]
- Roca, M.; Donat, E.; Masip, E.; Crespo-Escobar, P.; Fornes-Ferrer, V.; Polo, B.; Ribes-Koninckx, C. Detection and Quantification of Gluten Immunogenic Peptides in Feces of Infants and Their Relationship with Diet. Rev. Esp. Enferm. Dig. 2019, 111, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Guía Para Estudios Dietéticos. Albúm Fotográfico de Alimentos—Universidad de Granada. Available online: https://editorial.ugr.es/libro/guia-para-estudios-dieteticos_137495/ (accessed on 10 February 2023).
- Moreiras, O.; Carbajal, Á.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos; Pirámide: Madrid, Spain, 2018; p. 496. [Google Scholar]
- Moubarac, J.C.; Batal, M.; Louzada, M.L.; Martinez Steele, E.; Monteiro, C.A. Consumption of Ultra-Processed Foods Predicts Diet Quality in Canada. Appetite 2017, 108, 512–520. [Google Scholar] [CrossRef]
- OPS. Alimentos y Bebidas Ultraprocesados en América Latina: Tendencias, Efecto Sobre la Obesidad e Implicaciones Para las Políticas Públicas; Departamento de Enfermedades no Transmisibles y Salud Mental: Washington, DC, USA, 2015; p. 76. [Google Scholar]
- FAO. Guidelines on the Collection of Information on Food Processing through Food Consumption Surveys; FAO: Rome, Italy, 2015. [Google Scholar]
- Monteiro, C.A.; Moubarac, J.C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-Processed Products Are Becoming Dominant in the Global Food System. Obes. Rev. 2013, 14 (Suppl. S2), 21–28. [Google Scholar] [CrossRef] [PubMed]
- Madrigal, C.; Soto-Méndez, M.J.; Hernández-Ruiz, Á.; Valero, T.; Ávila, J.M.; Ruiz, E.; Villoslada, F.L.; Leis, R.; de Victoria, E.M.; Moreno, J.M.; et al. Energy Intake, Macronutrient Profile and Food Sources of Spanish Children Aged One To. Nutrients 2020, 12, 893. [Google Scholar] [CrossRef] [Green Version]
- Dietary Reference Values|EFSA. Available online: https://www.efsa.europa.eu/en/topics/topic/dietary-reference-values (accessed on 10 February 2023).
- Ferrara, P.; Cicala, M.; Tiberi, E.; Spadaccio, C.; Marcella, L.; Gatto, A.; Calzolari, P.; Castellucci, G. High Fat Consumption in Children with Celiac Disease. Acta Gastroenterol. Belg. 2009, 72, 296–300. [Google Scholar]
- Forchielli, M.L.; Diani, L.; Labriola, F.; Bolasco, G.; Rocca, A.; Salfi, N.C.; Leone, A.; Miserocchi, C.; Andreozzi, L.; Levi Della Vida, F.; et al. Gluten Deprivation: What Nutritional Changes Are Found During the First Year in Newly Diagnosed Coeliac Children? Nutrients 2019, 12, 60. [Google Scholar] [CrossRef] [Green Version]
- Fernández Miaja, M.; Díaz Martín, J.J.; Jiménez Treviño, S.; Suárez González, M.; Bousoño García, C. Estudio de La Adherencia a La Dieta Sin Gluten En Pacientes Celiacos. An. Pediatr. 2021, 94, 377–384. [Google Scholar] [CrossRef]
- Al Sarkhy, A.; El Mouzan, M.I.; Saeed, E.; Alanazi, A.; Alghamdi, S.; Anil, S.; Assiri, A. Clinical Characteristics of Celiac Disease and Dietary Adherence to Gluten-Free Diet among Saudi Children. Pediatr. Gastroenterol. Hepatol. Nutr. 2015, 18, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comino, I.; Fernández-Bañares, F.; Esteve, M.; Ortigosa, L.; Castillejo, G.; Fambuena, B.; Ribes-Koninckx, C.; Sierra, C.; Rodríguez-Herrera, A.; Salazar, J.C.; et al. Fecal Gluten Peptides Reveal Limitations of Serological Tests and Food Questionnaires for Monitoring Gluten-Free Diet in Celiac Disease Patients. Am. J. Gastroenterol. 2016, 111, 1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shepherd, S.J.; Gibson, P.R. Nutritional Inadequacies of the Gluten-Free Diet in Both Recently-Diagnosed and Long-Term Patients with Coeliac Disease. J. Hum. Nutr. Diet. 2013, 26, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Nestares, T.; Martín-Masot, R.; Flor-Alemany, M.; Bonavita, A.; Maldonado, J.; Aparicio, V.A. Influence of Ultra-Processed Foods Consumption on Redox Status and Inflammatory Signaling in Young Celiac Patients. Nutrients 2021, 13, 156. [Google Scholar] [CrossRef]
- Penagini, F.; Dilillo, D.; Meneghin, F.; Mameli, C.; Fabiano, V.; Zuccotti, G.V. Gluten-Free Diet in Children: An Approach to a Nutritionally Adequate and Balanced Diet. Nutrients 2013, 5, 4553–4565. [Google Scholar] [CrossRef] [Green Version]
- Kabbani, T.A.; Goldberg, A.; Kelly, C.P.; Pallav, K.; Tariq, S.; Peer, A.; Hansen, J.; Dennis, M.; Leffler, D.A. Body Mass Index and the Risk of Obesity in Coeliac Disease Treated with the Gluten-Free Diet. Aliment. Pharmacol. Ther. 2012, 35, 723–729. [Google Scholar] [CrossRef]
- Lane, M.M.; Davis, J.A.; Beattie, S.; Gómez-Donoso, C.; Loughman, A.; O’Neil, A.; Jacka, F.; Berk, M.; Page, R.; Marx, W.; et al. Ultraprocessed Food and Chronic Noncommunicable Diseases: A Systematic Review and Meta-Analysis of 43 Observational Studies. Obes. Rev. 2021, 22, e13146. [Google Scholar] [CrossRef]
- Aguayo-Patrón, S.V.; Calderón de la Barca, A.M. Old Fashioned vs. Ultra-Processed-Based Current Diets: Possible Implication in the Increased Susceptibility to Type 1 Diabetes and Celiac Disease in Childhood. Foods 2017, 6, 100. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD) |
|---|---|
| Age (years) | 7.5 (3.9) |
| Sex (n [%]) | |
| Male | 24 (39.3) |
| Female | 37 (60.7) |
| Weight (kg) | 25.9 (13.3) |
| Height (m) | 1.2 (0.2) |
| Body mass index categories (n [%]) | |
| Underweight | 2 (3.3) |
| Normoweight | 44 (72.1) |
| Overweight | 11 (18.0) |
| Obese | 4 (6.6) |
| Energy (kcal) (n = 58) | 1543.9 (462.2) |
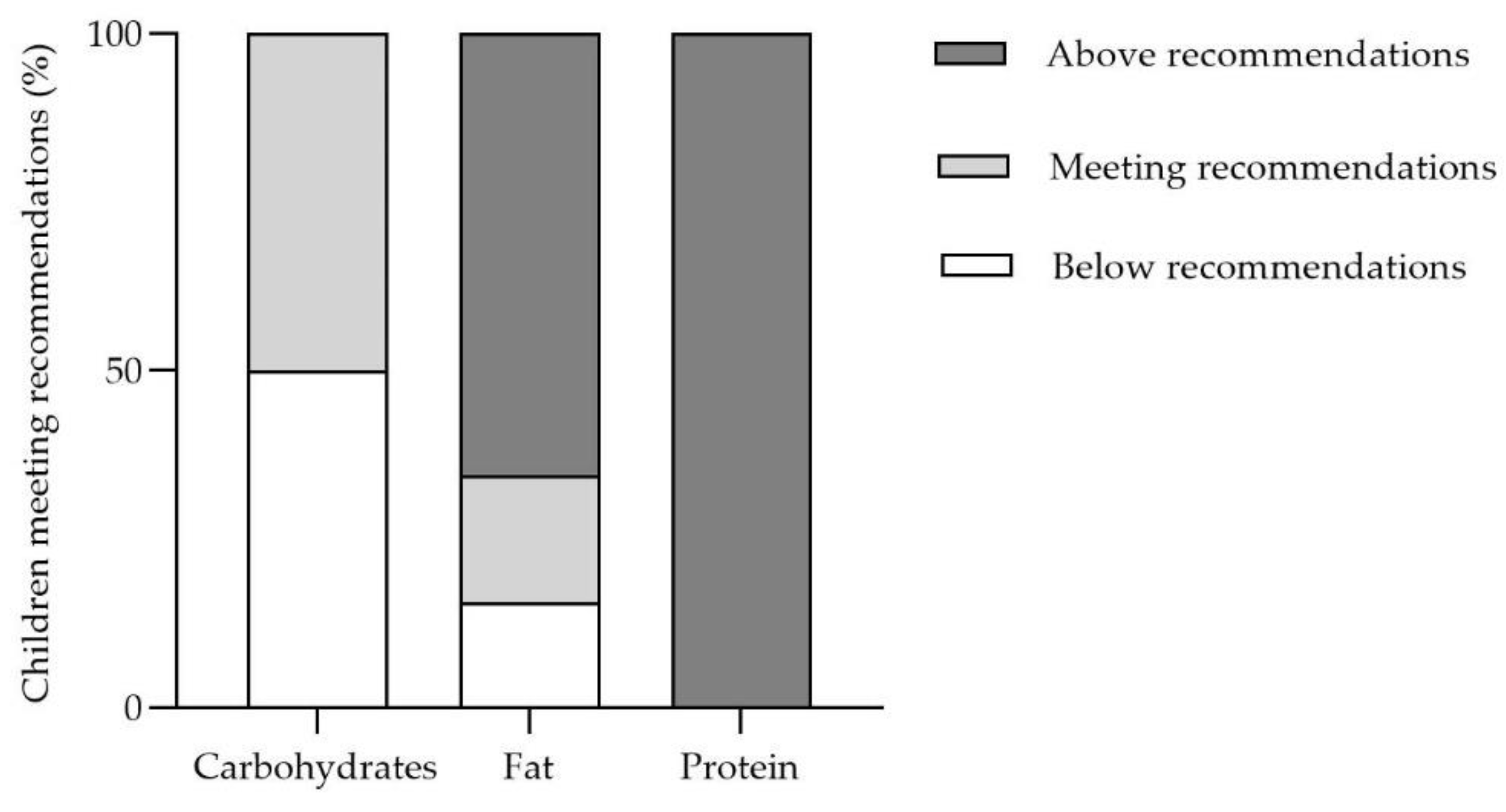
| Fat (% of total energy intake) | 38.2 (6.7) |
| Protein (% of total energy intake) | 16.0 (4.0) |
| Carbohydrates (% of total energy intake) | 44.2 (6.6) |
| NOVA food classification (n = 58) | |
| Unprocessed or minimally processed foods (kcal/day) | 601.0 (215.8) |
| Unprocessed or minimally processed foods (%E) | 39.8 (11.5) |
| Processed culinary ingredients (kcal/day) | 102.3 (63.4) |
| Processed culinary ingredients (%E) | 6.7 (3.4) |
| Processed Foods (kcal/day) | 98.1 (84.1) |
| Processed Foods (%E) | 6.2 (4.9) |
| Ultra-processed food and drink products (kcal) | 739.4 (316.7) |
| Ultra-processed food and drink products (%Energy) | 47.5 (13.1) |
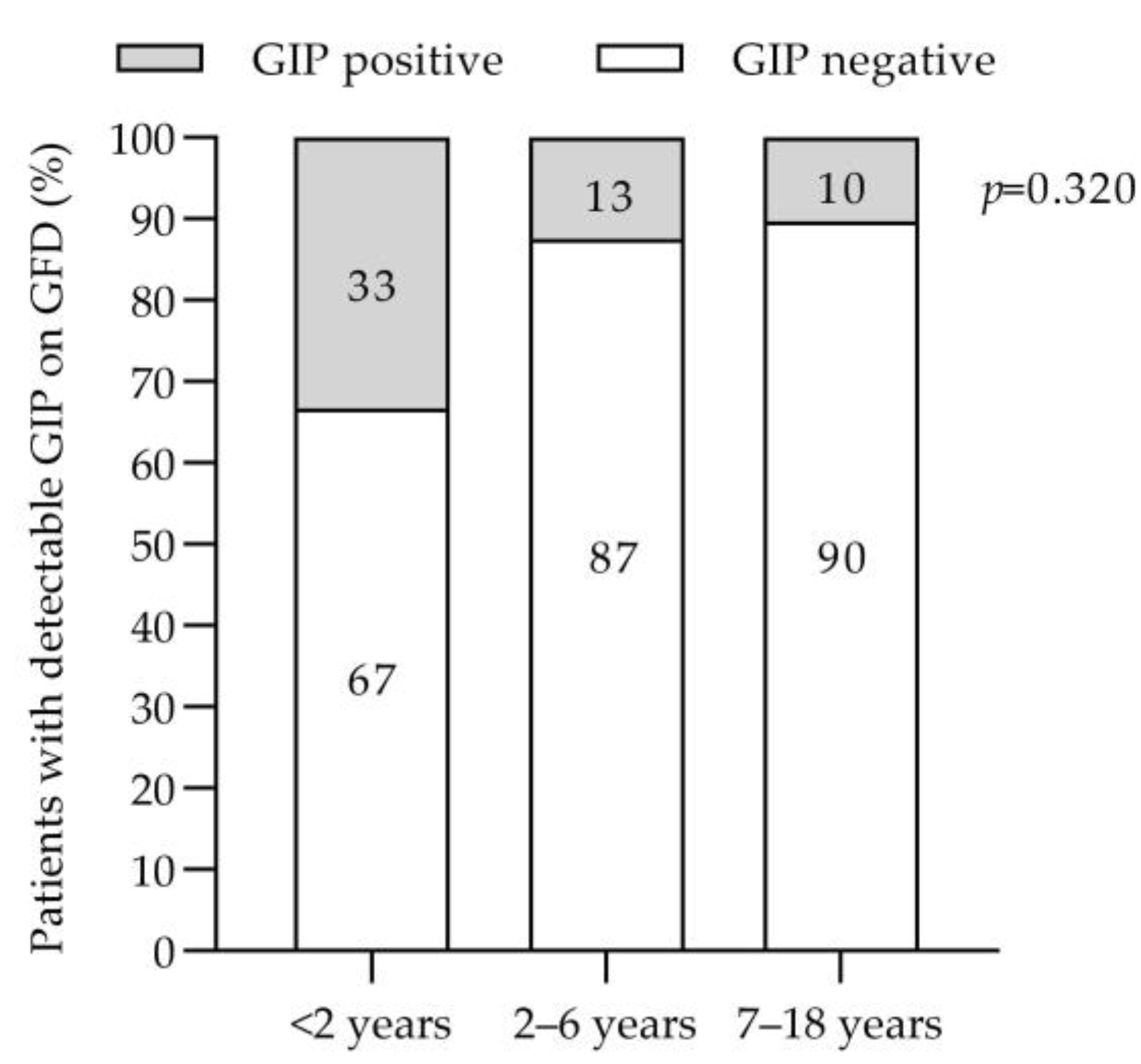
| Fecal gluten immunogenic peptides (n [%]) (n = 60) | |
| Positive | 8 (13.3) |
| Negative | 52 (86.7) |
| Other diseases (yes, n [%]) | 4 (6.6) |
| Negative (n = 49) | Positive (n = 8) | p a | p b | |
|---|---|---|---|---|
| Dietary intake | ||||
| Energy (kcal) | 1559.3 (65.1) | 1568.4 (161.1) | 0.958 | 0.446 |
| Fat (% of E) | 38.9 (0.7) | 38.7 (1.8) | 0.929 | 0.953 |
| Protein (% of E) | 16.1 (0.6) | 15.3 (1.4) | 0.620 | 0.690 |
| Carbohydrates (% E) | 43.9 (0.9) | 45.1 (2.4) | 0.669 | 0.649 |
| Fiber (g/day) | 10.5 (0.7) | 9.6 (1.7) | 0.609 | 0.933 |
| Sugar (g/day) | 22.4 (2.0) | 16.8 (5.2) | 0.342 | 0.525 |
| Vitamin A (µg) | 320.2 (19.0) | 274.6 (47.1) | 0.373 | 0.493 |
| Vitamin D (µg) | 3.8 (0.7) | 2.2 (1.8) | 0.435 | 0.564 |
| Vitamin E | 4.4 (0.3) | 5.2 (0.7) | 0.380 | 0.234 |
| Riboflavin (mg) | 0.9 (0.05) | 1.1 (0.1) | 0.291 | 0.395 |
| Folate (µg) | 97.4 (6.3) | 99.3 (15.5) | 0.911 | 0.747 |
| Cobalamin (µg) | 4.2 (0.5) | 3.3 (1.1) | 0.511 | 0.609 |
| Calcium (mg) | 500.4 (38.5) | 605.2 (95.4) | 0.313 | 0.339 |
| Vitamin C (mg) | 46.1 (6.2) | 31.8 (15.3) | 0.390 | 0.721 |
| Potasium (mg) | 1496.8 (88.8) | 1569.2 (219.7) | 0.761 | 0.582 |
| Magnesium (mg) | 119.4 (6.7) | 129.5 (16.5) | 0.572 | 0.421 |
| NOVA food classification | ||||
| Unprocessed or minimally processed foods (%E) | 39.3 (1.7) | 42.5 (4.1) | 0.472 | 0.447 |
| Processed culinary ingredients (%E) | 6.7 (0.5) | 7.6 (1.2) | 0.489 | 0.463 |
| Processed Foods (%E) | 5.8 (0.7) | 7.6 (1.7) | 0.335 | 0.285 |
| Ultra-processed food and drink products (%Energy) | 48.6 (1.9) | 41.3 (4.6) | 0.146 | 0.088 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-Masot, R.; Jiménez-Muñoz, M.; Herrador-López, M.; Flor-Alemany, M.; Navas-López, V.M.; Nestares, T. The Importance of an Early Evaluation after Establishing a Gluten-Free Diet in Children with Celiac Disease. Nutrients 2023, 15, 1761. https://doi.org/10.3390/nu15071761
Martín-Masot R, Jiménez-Muñoz M, Herrador-López M, Flor-Alemany M, Navas-López VM, Nestares T. The Importance of an Early Evaluation after Establishing a Gluten-Free Diet in Children with Celiac Disease. Nutrients. 2023; 15(7):1761. https://doi.org/10.3390/nu15071761
Chicago/Turabian StyleMartín-Masot, Rafael, María Jiménez-Muñoz, Marta Herrador-López, Marta Flor-Alemany, Víctor Manuel Navas-López, and Teresa Nestares. 2023. "The Importance of an Early Evaluation after Establishing a Gluten-Free Diet in Children with Celiac Disease" Nutrients 15, no. 7: 1761. https://doi.org/10.3390/nu15071761