
Economic Evaluation of Clinical, Nutritional and Rehabilitation Interventions on Oropharyngeal Dysphagia after Stroke: A Systematic Review
 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
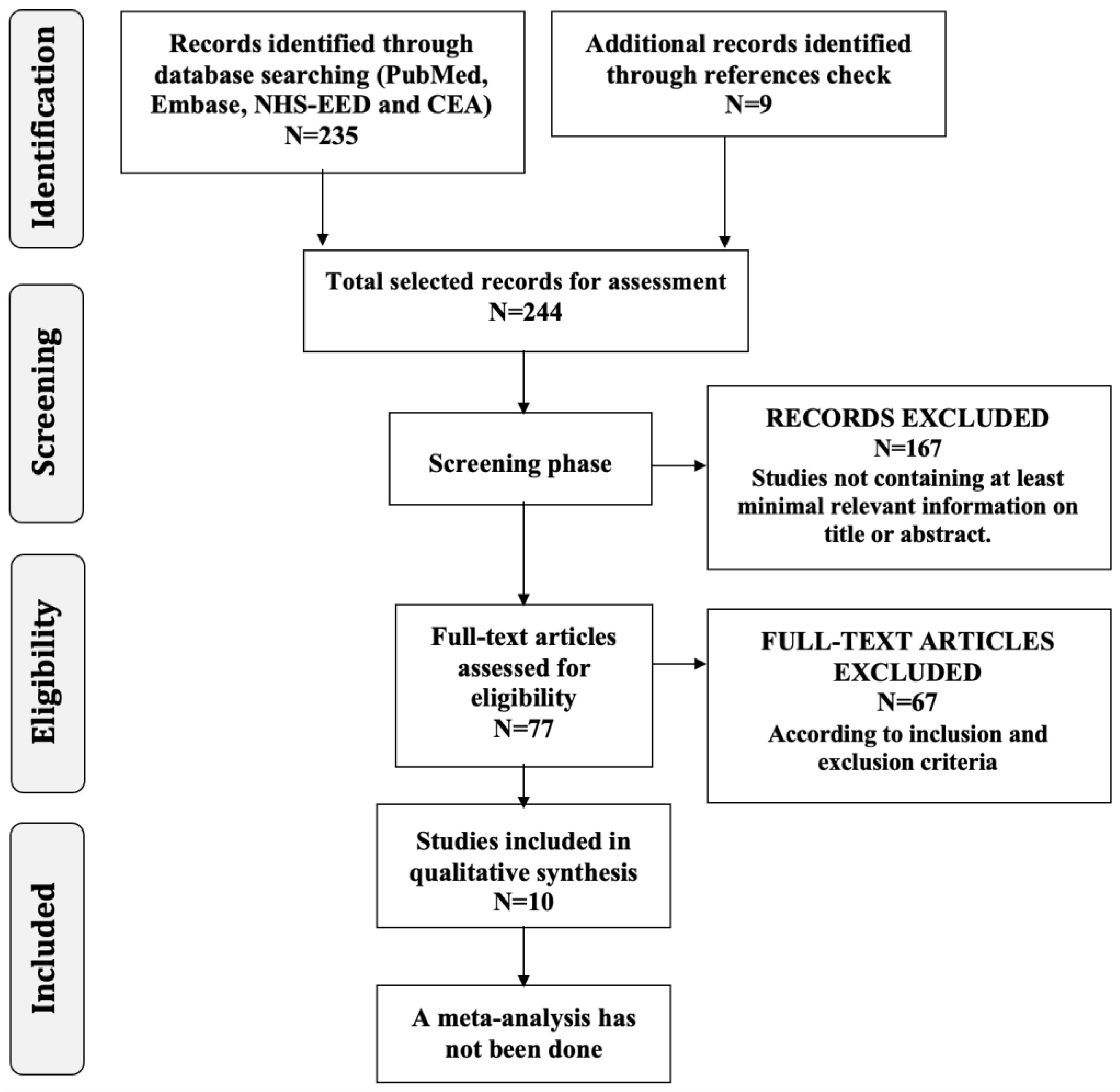
2.2. Selection Process
2.3. Data Presentation and Summary Measures
2.4. Quality Assessment
3. Results
3.1. Data Presentation and Results of Individual Studies
3.1.1. Screening and Assessment of PS-OD
3.1.2. Rehabilitation Services including PS-OD Management
3.1.3. Compensatory Strategies: Food Consistency Modification and Thickened Fluids
3.1.4. Nutrition by Enteral Tube Feeding in Patients with PS-OD
3.2. Synthesis of the Studies Findings
3.2.1. Screening and Assessment of PS-OD
3.2.2. Rehabilitation Services including PS-OD Management
3.2.3. Compensatory Strategies: Food Consistency Modification and Thickened Fluids
3.2.4. Nutrition by Enteral Tube Feeding in Patients with PS-OD
3.3. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rofes, L.; Arreola, V.; Romea, M.; Palomera, E.; Almirall, J.; Cabré, M.; Serra-Prat, M.; Clavé, P. Pathophysiology of oropharyngeal dysphagia in the frail elderly. Neurogastroenterol. Motil. 2010, 22, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Clavé, P.; Shaker, R. Dysphagia: Current reality and scope of the problem. Nat. Rev. Gastroenterol. Hepatol. 2015, 5, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Rofes, L.; Muriana, D.; Palomeras, E.; Vilardell, N.; Palomera, E.; Alvarez-Berdugo, D.; Casado, V.; Clavé, P. Prevalence, risk factors and complications of oropharyngeal dysphagia in stroke patients: A cohort study. Neurogastroenterol. Motil. 2018, 23, e13338. [Google Scholar] [CrossRef] [PubMed]
- Martino, R.; Foley, N.; Bhogal, S.; Diamant, N.; Speechley, M.; Teasell, R. Dysphagia after stroke: Incidence, diagnosis, and pulmonary complications. Stroke 2005, 36, 2756–2763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, G.; Hankey, G.J.; Cameron, D. Swallowing function after stroke: Prognosis and prognostic factors at 6 months. Stroke 1999, 30, 744–748. [Google Scholar] [CrossRef] [Green Version]
- Cabré, M.; Serra-Prat, M.; Palomeras, E.; Almirall, J.; Pallares, R.; Clave, P. Prevalence and prognostic implications of dysphagia in elderly patients with pneumonia. Age Ageing 2010, 39, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Ortega, O.; Martín, A.; Clavé, P. Diagnosis and Management of Oropharyngeal Dysphagia among Older Persons, State of the Art. J. Am. Med. Dir. Assoc. 2017, 18, 576–582. [Google Scholar] [CrossRef]
- Katzan, I.L.; Cebul, R.D.; Husak, S.H.; Dawson, N.V.; Baker, D.W. The effect of pneumonia on mortality among patients hospitalized for acute stroke. Neurology 2003, 60, 620–625. [Google Scholar] [CrossRef]
- Viñas, P.; Bolivar-Prados, M.; Tomsen, N.; Costa, A.; Marin, S.; Riera, S.A.; Barcons, N.; Clavé, P. The Hydration Status of Adult Patients with Oropharyngeal Dysphagia and the Effect of Thickened Fluid Therapy on Fluid Intake and Hydration: Results of Two Parallel Systematic and Scoping Reviews. Nutrients 2022, 14, 2497. [Google Scholar] [CrossRef]
- Attrill, S.; White, S.; Murray, J.; Hammond, S.; Doeltgen, S. Impact of oropharyngeal dysphagia on healthcare cost and length of stay in hospital: A systematic review. BMC Health Serv. Res. 2018, 18, 594. [Google Scholar] [CrossRef] [Green Version]
- Marin, S.; Serra-Prat, M.; Ortega, O.; Clavé, P. Cost of oropharyngeal dysphagia after stroke: Protocol for a systematic review. BMJ Open 2018, 8, e022775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marin, S.; Serra-Prat, M.; Ortega, O.; Clavé, P. Healthcare related cost of oropharyngeal dysphagia and its complications after stroke: A Systematic review. BMJ Open 2020, 10, e031629. [Google Scholar] [CrossRef] [PubMed]
- Marin, S.; Serra-Prat, M.; Ortega, O.; Audouard, M.; Valls, J.; Palomera, E.; Cunillera, R.; Palomeras, E.; Ibàñez, J.M.; Clavé, P. Healthcare costs of post-stroke oropharyngeal dysphagia and its complications: Malnutrition and respiratory infections. Eur. J. Neurol. 2021, 28, 3670–3681. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Baijens, L.; Heijnen, M.; Zwijnenberg, I. Effects of therapy in oropharyngeal dysphagia by speech and language therapists: A systematic review. Dysphagia 2010, 25, 40–65. [Google Scholar] [CrossRef] [Green Version]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef]
- Dziewas, R.; Michou, E.; Trapl-Grundschober, M.; Lal, A.; Arsava, E.M.; Bath, P.M.; Clavé, P.; Glahn, J.; Hamdy, S.; Pownall, S.; et al. European Stroke Organisation and European Society for Swallowing Disorders guideline for the diagnosis and treatment of post-stroke dysphagia. Eur. Stroke J. 2021, 6, LXXXIX. [Google Scholar] [CrossRef] [PubMed]
- European Society for Swallowing Disorders (2012) ESSD Position Statements: Oropharyngeal Dysphagia in Adult Patients. Available online: www.myessd.org/docs/position_statements/ESSD_Position_Statements_on_OD_in_adult_patients_for_web.pdf (accessed on 31 January 2023).
- Bolivar-Prados, M.; Rofes, L.; Arreola, V.; Guida, S.; Nascimento, W.V.; Martin, A.; Vilardell, N.; Ortega, O.; Ripken, D.; Lansink, M.; et al. Effect of a gum-based thickener on the safety of swallowing in patients with poststroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2019, 31, e13695. [Google Scholar] [CrossRef] [Green Version]
- Newman, R.; Vilardell, N.; Clavé, P.; Speyer, R. Effect of Bolus Viscosity on the Safety and Efficacy of Swallowing and the Kinematics of the Swallow Response in Patients with Oropharyngeal Dysphagia: White Paper by the European Society for Swallowing Disorders (ESSD). Dysphagia 2016, 2, 232–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, O.; Bolívar-Prados, M.; Arreola, V.; Nascimento, W.V.; Tomsen, N.; Gallegos, C.; Brito-de La Fuente, E.; Clavé, P. Therapeutic Effect, Rheological Properties and α-Amylase Resistance of a New Mixed Starch and Xanthan Gum Thickener on Four Different Phenotypes of Patients with Oropharyngeal Dysphagia. Nutrients 2020, 6, 1873. [Google Scholar] [CrossRef]
- Leigh, J.H.; Oh, B.M.; Seo, H.G.; Lee, G.J.; Min, Y.; Kim, K.; Lee, J.C.; Han, T.R. Influence of the chin-down and chin-tuck maneuver on the swallowing kinematics of healthy adults. Dysphagia 2015, 1, 89–98. [Google Scholar] [CrossRef] [Green Version]
- McCulloch, T.M.; Hoffman, M.R.; Ciucci, M.R. High-resolution manometry of pharyngeal swallow pressure events associated with head turn and chin tuck. Ann. Otol. Rhinol. Laryngol. 2010, 6, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Cabib, C.; Nascimento, W.; Rofes, L.; Arreola, V.; Tomsen, N.; Mundet, L.; Palomeras, E.; Michou, E.; Clavé, P.; Ortega, O. Short-term neurophysiological effects of sensory pathway neurorehabilitation strategies on chronic poststroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2020, 9, e13887. [Google Scholar] [CrossRef] [PubMed]
- Cheng, I.; Sasegbon, A.; Hamdy, S. Effects of pharmacological agents for neurogenic oropharyngeal dysphagia: A systematic review and meta-analysis. Neurogastroenterol. Motil. 2022, 3, e14220. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Transcutaneous Neuromuscular Electrical Stimulation for Oropharyngeal Dysphagia in Adults. UK IPG634. 2018. Available online: https://www.nice.org.uk/guidance/ipg634/resources/transcutaneous-neuromuscular-electrical-stimulation-for-oropharyngeal-dysphagia-in-adults-pdf-1899874043109061 (accessed on 22 March 2023).
- National Institute for Health and Care Excellence. Transcutaneous Neuromuscular Electrical Stimulation for Oropharyngeal Dysphagia. UK NICE interventional procedure guidance [IPG490]. 2014. Available online: https://www.nice.org.uk/guidance/ipg490 (accessed on 22 March 2023).
- Arreola, V.; Ortega, O.; Álvarez-Berdugo, D.; Rofes, L.; Tomsen, N.; Cabib, C.; Muriana, D.; Palomera, E.; Clavé, P. Effect of Transcutaneous Electrical Stimulation in Chronic Poststroke Patients with Oropharyngeal Dysphagia: 1-Year Results of a Randomized Controlled Trial. Neurorehabil. Neural Repair. 2021, 9, 778–789. [Google Scholar] [CrossRef]
- Cabib, C.; Ortega, O.; Kumru, H.; Palomeras, E.; Vilardell, N.; Alvarez-Berdugo, D.; Muriana, D.; Rofes, L.; Terré, R.; Mearin, F.; et al. Neurorehabilitation strategies for poststroke oropharyngeal dysphagia: From compensation to the recovery of swallowing function. Ann. N. Y. Acad. Sci. 2016, 1380, 121–138. [Google Scholar] [CrossRef]
- Cheng, I.; Hamdy, S. Current perspectives on the benefits, risks, and limitations of noninvasive brain stimulation (NIBS) for post-stroke dysphagia. Expert Rev. Neurother. 2021, 10, 1135–1146. [Google Scholar] [CrossRef]
- Chiang, C.F.; Lin, M.T.; Hsiao, M.Y.; Yeh, Y.C.; Liang, Y.C.; Wang, T.G. Comparative Efficacy of Noninvasive Neurostimulation Therapies for Acute and Subacute Poststroke Dysphagia: A Systematic Review and Network Meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 739–750.e4. [Google Scholar] [CrossRef]
- Cheng, I.; Hamad, A.; Sasegbon, A.; Hamdy, S. Advances in the Treatment of Dysphagia in Neurological Disorders: A Review of Current Evidence and Future Considerations. Neuropsychiatr. Dis. Treat. 2022, 18, 2251–2263. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Marin, S.; Serra-Prat, M.; Ortega, O.; Clavé, P. Economic evaluations of health care interventions in Oropharyngeal Dysphagia after Stroke: Protocol for a Systematic Review. Syst. Rev. 2022, 11, 92. [Google Scholar] [CrossRef]
- Centre for Reviews and Dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care; Centre for Reviews and Dissemination, University of York: York, UK, 2009; Available online: https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf (accessed on 31 January 2023).
- Husereau, D.; Drummond, M.; Augustovski, F.; de Bekker-Grob, E.; Briggs, A.H.; Carswell, C.; Caulley, L.; Chaiyakunapruk, N.; Greenberg, D.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement: Updated reporting guidance for health economic evaluations. BMC Public Health 2022, 22, 179. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.Y.; Zhang, X.P.; Mo, M.M.; Ye, R.C.; Hu, C.X.; Jiang, M.Q.; Lin, M.Q. Impact of the systematic use of the volume-viscosity swallow test in patients with acute ischaemic stroke: A retrospective study. BMC Neurol. 2020, 20, 154. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, M.L.; Ehlers, L.H.; Hundborg, H.H.; Ingeman, A.; Johnsen, S.P. Processes of early stroke care and hospital costs. Int. J. Stroke 2014, 9, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.D.; Howe, E.C. A cost-effectiveness analysis of screening methods for dysphagia after stroke. PMR 2012, 4, 273–282. [Google Scholar] [CrossRef]
- Schwarz, M.; Coccetti, A.; Cardell, E.; Murdoch, A.; Davis, J. Management of swallowing in thrombolysed stroke patients: Implementation of a new protocol. Int. J. Speech Lang Pathol. 2017, 19, 551–561. [Google Scholar] [CrossRef]
- Khiaocharoen, O.; Pannarunothai, S.; Riewpaiboon, W.; Ingsrisawang, L.; Teerawattananon, Y. Economic Evaluation of Rehabilitation Services for Inpatients with Stroke in Thailand: A Prospective Cohort Study. Value Health Reg. Issues 2012, 1, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Suksathien, R.; Chaiyaphan, Y.; Roongyoosiri, C.; Muangkham, P. Outcomes of Short-Course Inpatient Stroke Rehabilitation Program in Tertiary Hospital: A Pilot Study. J. Med. Assoc. Thai. 2015, 98, 1139–1144. [Google Scholar]
- Kotecki, S.; Schmidt, R. Cost and effectiveness analysis using nursing staff-prepared thickened liquids vs. commercially thickened liquids in stroke patients with dysphagia. Nurs. Econ. 2010, 28, 106. [Google Scholar]
- Pelczarska, A.; Jakubczyk, M.; Niewada, M. The cost-effectiveness of food consistency modification with xanthan gum-based Nutilis Clear® in patients with post-stroke dysphagia in Poland. BMC Health Serv. Res. 2020, 20, 552. [Google Scholar] [CrossRef]
- Elia, M.; Stratton, R.J. A cost-utility analysis in patients receiving enteral tube feeding at home and in nursing homes. Clin. Nutr. 2008, 27, 416–423. [Google Scholar] [CrossRef]
- Beavan, J.; Conroy, S.P.; Harwood, R.; Gladman, J.R.; Leonardi-Bee, J.; Sach, T.; Bowling, T.; Sunman, W.; Gaynor, C. Does looped nasogastric tube feeding improve nutritional delivery for patients with dysphagia after acute stroke? A randomised controlled trial. Age Ageing 2010, 39, 624–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riera, S.A.; Marin, S.; Serra-Prat, M.; Tomsen, N.; Arreola, V.; Ortega, O.; Walshe, M.; Clavé, P. A Systematic and a Scoping Review on the Psychometrics and Clinical Utility of the Volume-Viscosity Swallow Test (V-VST) in the Clinical Screening and Assessment of Oropharyngeal Dysphagia. Foods 2021, 10, 1900. [Google Scholar] [CrossRef] [PubMed]
- Martin-Martinez, A.; Miró, J.; Amadó, C.; Ruz, F.; Ruiz, A.; Ortega, O.; Clavé, P. A Systematic and Universal Artificial Intelligence Screening Method for Oropharyngeal Dysphagia: Improving Diagnosis Through Risk Management. Dysphagia 2022. [Google Scholar] [CrossRef] [PubMed]
- Martín, A.; Ortega, O.; Roca, M.; Arús, M.; Clavé, P. Effect of A Minimal-Massive Intervention in Hospitalized Older Patients with Oropharyngeal Dysphagia: A Proof of Concept Study. J. Nutr. Health Aging 2018, 22, 739–747. [Google Scholar] [CrossRef]
- Thavorncharoensap, M.; Teerawattananon, Y.; Nartanan, S. Assessing a Societal Value for a Ceiling Threshold in Thailand; Health Intervention and Technology Assessment Program: Nonthaburi, Thailand, 2009; Available online: https://www.hitap.net/en/research/17630 (accessed on 31 January 2023).
- Arreola, V.; Vilardell, N.; Ortega, O.; Rofes, L.; Muriana, D.; Palomeras, E.; Álvarez-Berdugo, D.; Clavé, P. Natural History of Swallow Function during the Three-Month Period after Stroke. Geriatrics 2019, 3, 42. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Study ID | Aim | Evaluated Intervention | Study Population | Design/Data Gathering | Time Horizon and Perspective |
|---|---|---|---|---|---|
| Assessment of OD after Stroke | |||||
| Wilson, R,D.; 2012 [38] | Cost-effectiveness of dysphagia screening methods |
| Hospitalised acute stroke (model-based) | Cost-effectiveness Decision-analysis model NA | Hospitalisation Societal perspective |
| Svendsen, M.L.; 2014 [37] | Association between processes of early stroke care and hospital costs | Early assessment of the swallowing function and 10 other processes related to acute stroke care | Ischemic and haemorrhagic stroke patients ≥18 years | Cost-saving Prospective | Hospitalisation Hospital perspective |
| Schwarz, M.; 2017 [39] | Impact of an OD screening protocol for thrombolysed stroke patients on operational outcomes (cost, length of stay, service compliance) | Protocol for the early screening of OD in thrombolysed patients | Ischemic stroke ≥18 years | Cost-saving Retrospective | Hospitalisation Hospital perspective |
| Liu, Z.Y.; 2020 [36] | Differences in total hospitalisation costs assessing OD with the WST test vs. the WST test and the V-VST if the first failed | Early assessment of PS-OD with two different screening tests:
| Ischemic stroke >18 years | Cost-saving Retrospective | Hospitalisation Hospital perspective |
| Rehabilitation Services Including OD Management | |||||
| Khiaocharoen, O.; 2012 [40] | Cost-utility of rehabilitation programme, including swallow training |
| Hospitalised acute stroke (subacute and non-acute phases) and discharged >17 years | Cost-utility Prospective | 4 months Societal perspective (also provided data on governmental) |
| Suksathien, R.; 2015 [41] | Efficiency and cost of short-course rehabilitation program | Short-course rehabilitation program (including speech-language therapy) | Inpatient rehabilitation after stroke >18 years | Cost-effectiveness Prospective | Inpatient rehabilitation Hospital perspective |
| Nutrition by Enteral Tube Feeding | |||||
| Elia, M.; 2008 [44] | Cost-utility of long-term enteral tube feeding | Enteral tube feeding | Cerebrovascular disease, nourished by enteral tube at home or nursing home | Cost-utility Retrospective | 3 years after starting tube feeding NA |
| Beavan, J.; 2010 [45] | Cost-effectiveness of nasal loop | Looped vs. non-looped nasogastric tube feeding | Hospitalised acute stroke | Cost-effectiveness Prospective (randomised controlled trial) | 2 weeks Cost associated to feeding perspective |
| Compensatory Strategies: Food Consistency Modification and Thickened Fluids | |||||
| Kotecki, S.; 2010 [42] | Differences in time and costs between nursing-staff-prepared and commercially prepared thickened liquids | Nursing-staff-prepared thickened liquids using Resource ThickenUp® and commercially prepared thickened liquids | NA | Cost-saving NA | Hospitalisation Hospital Perspective |
| Pelczarska, A.; 2020 [43] | Cost-utility of xanthan gum-based consistency modification therapy (Nutilis Clear®) | Routine clinical practice: behavioural compensations, manoeuvres, and rehabilitation exercises Xanthan gum–based consistency modification therapy (Nutilis Clear®) | Adult post-stroke (model-based) | Model-based cost-utility analysis (static and dynamic model) NA | Time horizon: -Static model: 8 weeks -Dynamic model: 1 year Public payer perspective |
| Study ID | Data Source | Elements of Cost Considered: (a) Direct Healthcare Costs (b) Direct Non-Healthcare Costs (c) Indirect Costs | Country, Year and Currency |
|---|---|---|---|
| Assessment of OD after Stroke | |||
| Wilson, R.D.; 2012 [38] | Available literature Estimations | (a) Yes, direct medical costs of VFS, non-oral feeding and pneumonia (b) No (c) No | United States NA USD (2010) |
| Svendsen, M.L.; 2014 [37] | Medical registries, national population-based, including the Danish Stroke Registry, the Danish National Registry of Patients, and the Danish Civil Registration System | (a) Yes, hospitalisation costs (b) No (c) No | Denmark 2005–2010 USD (2010) |
| Schwarz, M.; 2017 [39] | Clinical records | (a) Yes, hospitalisation costs (b) No (c) No | Australia 2011–2014 Australian dollars (year not available) |
| Liu, Z.Y.; 2020 [36] | Questionnaire Clinical records | (a) Yes, hospitalisation costs (b) No (c) No | China 2017 USD (year not available) |
| Rehabilitation Services Including OD Management | |||
| Khiaocharoen, O.; 2012 [40] | Data collection process by health professionals and cost diary recorded by patients and relatives both checked and confirmed by investigators | (a) Yes, including rehabilitation and medical costs (b) Yes, cost of living during the stroke episode (e.g., transport, food) (c) Yes, loss of income of patients and relatives | Thailand 2008–2009 Baht (year NA) |
| Suksathien, R.; 2015 [41] | Data collection process by investigators | (a) Yes, medicine, laboratory, rehabilitation training, nursing, bed, and others (not defined) (b) No (c) No | Thailand 2014 Baht (year NA) |
| Nutrition by Enteral Tube Feeding | |||
| Elia, M.; 2008 [44] | Database of the British Artificial Nutrition Survey | (a) Yes, in hospital cost of gastrostomy insertion and patient training, cost of home visits by general practitioners, dietitians, nurses, speech and language therapists, physiotherapists, chiropodists, community occupational therapists, the cost of feeding, ancillaries and delivery, hospital readmissions and nursing home (b) No (c) No | United Kingdom 1995–2005 Pounds Sterling (2005) |
| Beavan, J.; 2010 [45] | Data collected during randomised controlled trial, local purchase costs and the cost for a single loop set | (a) Yes, direct medical costs of feeding (b) No (c) No | United Kingdom 2006–2007 Pounds Sterling (year NA) |
| Compensatory Strategies: Food Consistency Modification and Thickened Fluids | |||
| Kotecki, S.; 2010 [42] | Data collected during study performance from a neuroscience hospitalisation unit | (a) Yes, direct medical costs of liquid products, thickeners, nurses and technicians, and viscometer (b) No (c) No | United States NA USD (year not available) |
| Pelczarska, A.; 2020 [43] | Literature review Clinical expert consultations | (a) Yes, OD treatment costs, aspiration pneumonia treatment costs and monitoring costs (monitoring costs only for the dynamic model) (b) No (c) No | Poland NA PLN (year NA) |
| Study ID | Age (Years) and Gender (Male) | Patient Inclusion or Exclusion Criteria | Method of OD Diagnostic |
|---|---|---|---|
| Assessment of OD after Stroke | |||
| Wilson, R.D.; 2012 [38] | NA (model-based) | NA (model-based, typical hospitalised stroke patient without previous OD nor contraindication to OD screening) | VFS CBSE CBSE followed by VFS if abnormal swallow |
| Svendsen, M.L.; 2014 [37] | Mean age (SD): Processes received 0–24%: 72.2 (14.3) Processes received 25–49%: 73.6 (12.7) Processes received 50–74%: 72.6 (12.9) Processes received 75–100%: 69.9 (13.3) Gender n (%): Processes received 0–24%: 212 (47.9) Processes received 25–49%: 344 (49.9) Processes received 50–74%: 798 (54.1) Processes received 75–100%: 1875 (56.8) | Inclusion criteria:
| GUS |
| Schwarz, M.; 2017 [39] | Mean age (range): Overall: 69.9 (31–92) Gender n (%): Overall: 37 (44.6) | Inclusion criteria:
| Speech-language pathologist assessment Trained nursing staff using the Royal Brisbane and Women’s Hospital Dysphagia Screening Tool |
| Liu, Z.Y.; 2020 [36] | Mean age (range): Pre-V-VST: 69.73 (80.92–80.54) V-VST period: 67.36 (56.48–78.24) Gender n (%): Pre-V-VST: 93 (63.3) V-VST period: 55 (57.9) | Inclusion criteria:
| WST or WST followed by V-VST if the first failed |
| Rehabilitation Services Including OD Management | |||
| Khiaocharoen, O.; 2012 [40] | Mean age (SD): Control group: 60.8 (12.9) Rehabilitation group: 61.1 (12.5) Gender n (%): Control group: 53 (58.9) Rehabilitation group: 67 (57.3) | Inclusion criteria:
| NA |
| Suksathien, R.; 2015 [41] | Mean age (SD): 57 (19–86) Gender n (%): 28 (56) | Inclusion criteria:
| NA |
| Nutrition by Enteral Tube Feeding | |||
| Elia, M.; 2008 [44] | Mean age (SD): Own home: 73 (13) Nursing home: 78 (10) Gender: NA | Inclusion criteria:
| NA |
| Beavan, J.; 2010 [45] | Mean age (SD): Loop group: 79 (10) Control group: 81 (10) Gender n (%): Loop group: 20 (39) Control group: 23 (43) | Inclusion criteria:
| Standardised WST |
| Compensatory Strategies: Food Consistency Modification and Thickened Fluids | |||
| Kotecki, S.; 2010 [42] | NA | NA | NA |
| Pelczarska, A.; 2020 [43] | NA (model-based) | NA (model-based, adult stroke patient with OD, analysis restricted to patients with an aspiration level of 10–14 on GUS) | GUS (model-based) |
| Study ID | Aim | Sample Size | Specific Data Depending on the Type of Economic Evaluation | Result of Study: Cost Difference (+ Increase and − Reduction)/Incremental Cost-Effectiveness/Utility Ratio | Main Findings of Studies | Quality Assessment c (%) |
|---|---|---|---|---|---|---|
| Assessment of OD after Stroke | ||||||
| Wilson, R.D.; 2012 [38] | Cost-effectiveness of dysphagia screening methods | NA | Cost: VFS: 1853 USD CBSE: 1968 USD CBSE plus VFS: 1943 USD QALY: VFS: 1.791 QALYs CBSE: 1.789 QALYs CBSE plus VFS: 1.790 QALYs | Incremental effectiveness: VFS: NA CBSE plus VFS (vs. VFS): −0.001 CBSE (vs. CBSE plus VFS): −0.001 Incremental costs: VFS: NA CBSE plus VFS (vs. VFS): + 90 USD CBSE (vs. CBSE plus VFS): + 25 USD Cost/QALY of VFS: 1034 USD | VFS was the most cost-effective screening method compared to CBSE and a combination of both | 82.1 |
| Svendsen, M.L.; 2014 [37] | Association between processes of early stroke care and hospital costs | 5909 | Mean crude costs: Early swallowing assessment (first 24 h): 20,232 (25,459) a USD Delayed swallowing assessment: 29,222 (30,177) USD Mean adjusted costs: Early swallowing assessment (first 24 h): 19,487 (10,662) a USD Delayed swallowing assessment: 32,043 (15,097) USD | Adjusted cost difference: −12,556 (95% CI 9751–15,361) USD | Reduction in hospitalisation costs of 12,556 USD when swallow was assessed during the first admission day | 78.8 |
| Schwarz, M.; 2017 [39] | Impact of an OD screening protocol for thrombolysed stroke patients on operational outcomes (cost, length of stay, service compliance) | 83 | Costs: Screening protocol: 16,548 Australian dollars Non screening protocol: 18,053 Australian dollars | Crude costs difference: −1505 Australian dollars (p = 0.722; F = 0.129) | Non-significant reduction of 1505 Australian dollars in hospitalisation costs using a protocol to manage OD after thrombolysis | 61.5 |
| Liu, Z.Y.; 2020 [36] | Differences in total hospitalisation costs assessing OD with the WST test vs. the WST test and the V-VST if the first failed | 242 | No differences in median total hospitalisation costs: -WST group: 2807.8 (1951.4–4461.5) b -WST followed by V-VST: 2899.4 (2012.9–5074.7) b p = 0.0846 | NA | No differences in hospitalisation costs when PS-OD was assessed with the WST vs. V-VST if the WST failed | 57.6 |
| Rehabilitation Services Including OD Management | ||||||
| Khiaocharoen, O.; 2012 [40] | Cost-utility of rehabilitation programme including swallow training | 207 | Incremental program costs:
Rehabilitation group: 0.632 Control group: 0.352 | ICUR (Cost/QALY):
| ICUR of rehabilitation programme including swallow training (starting at the subacute and non-acute stroke phases) of 24,571 bahts from societal perspective | 79.6 |
| Suksathien, R.; 2015 [41] | Efficiency and cost of short-course rehabilitation program | 50 | Change in BI score between admission and discharge: 5.00 (2.25) a Total cost of rehabilitation admission: 7729 (4330) a 95% CI 1828–22,450 bahts | Change score of the BI/LOS: 0.56 (0.33) Cost/change score of the BI: 1545.8 bahts | Positive mean change in the BI score of 5 points between discharge and admission with mean total costs of 7729 bahts | 54.1 |
| Nutrition by Enteral Tube Feeding | ||||||
| Elia, M.; 2008 [44] | Cost-utility of long-term enteral tube feeding | 9895 QoL assessment (n = 25) | QoL (EuroQol): Home: 0.47 (0.28) a Nursing home: 0.47 (0.25) a QoL (both groups): 0.47 (95% CI 0.358–0.582) Mortality at 2 years: Home: 43% Nursing home: 56% | ICUR (Cost/QALY):
| ICUR of home enteral nutrition of £12,817 ICUR of nursing home enteral nutrition of £10,303–£68,064 | 81.4 |
| Beavan, J.; 2010 [45] | Cost-effectiveness of nasal loop | 104 | Percentage of received nutrition of total prescribed:
17% (95% CI 5–28%) Mean feeding costs:
| Incremental cost for an 1% additional total nutrition received: + £5.20 | Higher nutrient intake and low increase in hospitalisation costs using looped-nasogastric tube (£5.20 for every 1% increase) | 70.3 |
| Compensatory Strategies: Food Consistency Modification and Thickened Fluids | ||||||
| Kotecki, S.; 2010 [42] | Differences in time and costs between nursing-staff-prepared and commercially prepared thickened liquids | NA | Cost of preparing thickened liquids: Nectar texture: Water: 0.54 USD Milk: 1.34 USD Orange Juice: 0.86 USD Honey texture: Water: 0.75 USD Milk: 1.41 USD Orange Juice: 0.83 USD Commercially prepared products: Nectar texture: Water (4 ounces): 0.30 USD Milk (8 ounces): 0.61 USD Orange Juice (4 ounces): 0.36 USD Honey texture: Water (4 ounces): 0.31 USD Milk (8 ounces): 0.66 USD Orange Juice (4 ounces): 0.36 USD | Cost savings using commercially prepared thickened liquids: Nectar texture: Water: 44% Milk: 54% Orange Juice: 58% Honey texture: Water: 59% Milk: 53% Orange Juice: 57% | Commercially prepared thickened fluids 44% to 59% cheaper than in situ prepared | 71.7 |
| Pelczarska, A.; 2020 [43] | Cost-utility of xanthan gum-based consistency modification therapy (Nutilis Clear®) | NA | QALY and total costs: Static model:
| ICUR (Cost/QALY): Static model: 21,387 PLN Dynamic model: 20,977 PLN | ICUR of texture-modified diets using a gum-based thickener of 20,977 PLN following a dynamic model and of 21,387 PLN following a static model | 83.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marin, S.; Ortega, O.; Serra-Prat, M.; Valls, E.; Pérez-Cordón, L.; Clavé, P. Economic Evaluation of Clinical, Nutritional and Rehabilitation Interventions on Oropharyngeal Dysphagia after Stroke: A Systematic Review. Nutrients 2023, 15, 1714. https://doi.org/10.3390/nu15071714
Marin S, Ortega O, Serra-Prat M, Valls E, Pérez-Cordón L, Clavé P. Economic Evaluation of Clinical, Nutritional and Rehabilitation Interventions on Oropharyngeal Dysphagia after Stroke: A Systematic Review. Nutrients. 2023; 15(7):1714. https://doi.org/10.3390/nu15071714
Chicago/Turabian StyleMarin, Sergio, Omar Ortega, Mateu Serra-Prat, Ester Valls, Laia Pérez-Cordón, and Pere Clavé. 2023. "Economic Evaluation of Clinical, Nutritional and Rehabilitation Interventions on Oropharyngeal Dysphagia after Stroke: A Systematic Review" Nutrients 15, no. 7: 1714. https://doi.org/10.3390/nu15071714