
Childhood Obesity and Plasma Micronutrient Deficit of Chilean Children between 4 and 14 Years Old

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Survey Design and Application
2.3. Anthropometric Measures and Sociodemographic Characteristics
2.4. Blood Samples
2.5. Biochemistry Analyses
2.5.1. Plasma Metal Measurement
2.5.2. Vitamin Measurement
2.6. Statistical Analysis
3. Results
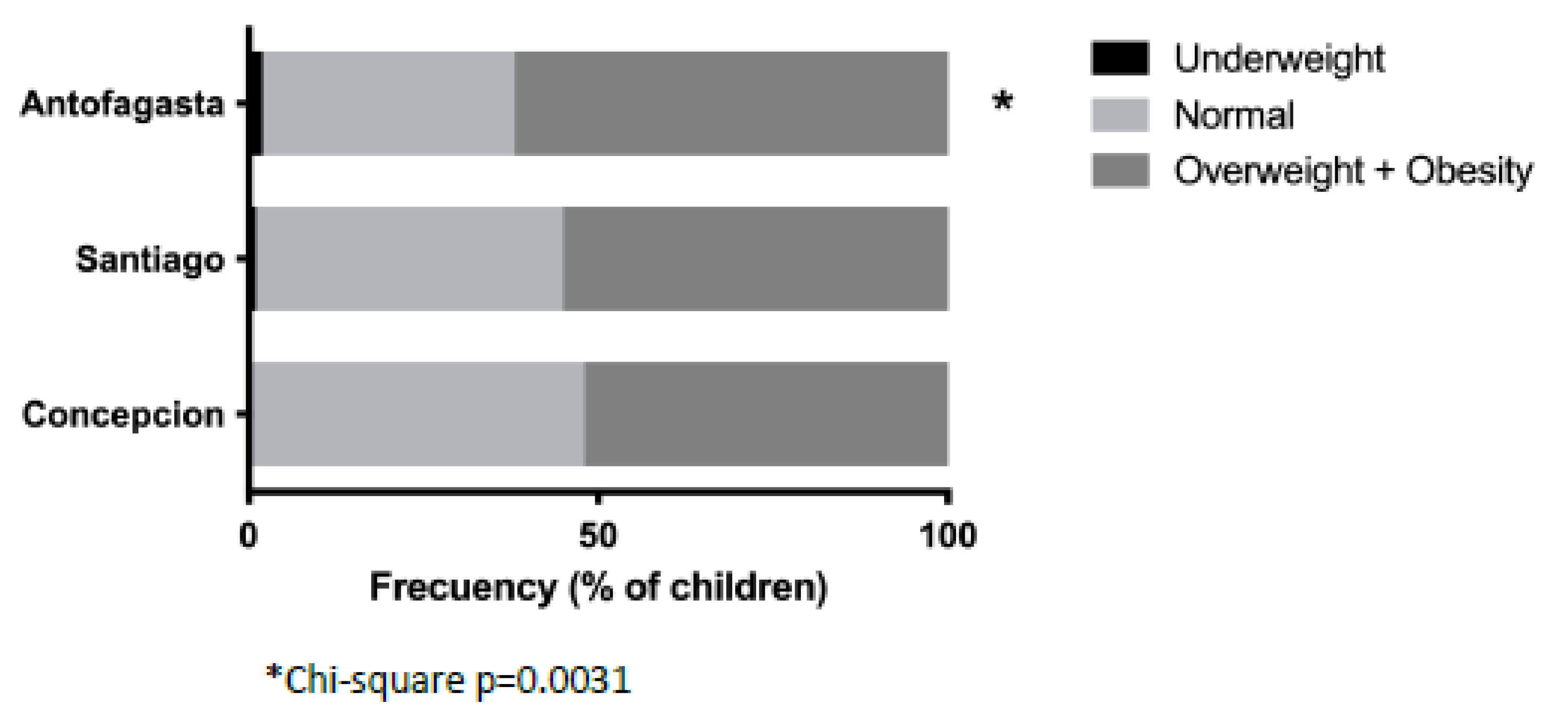
3.1. Physical Characteristics of the Study Group
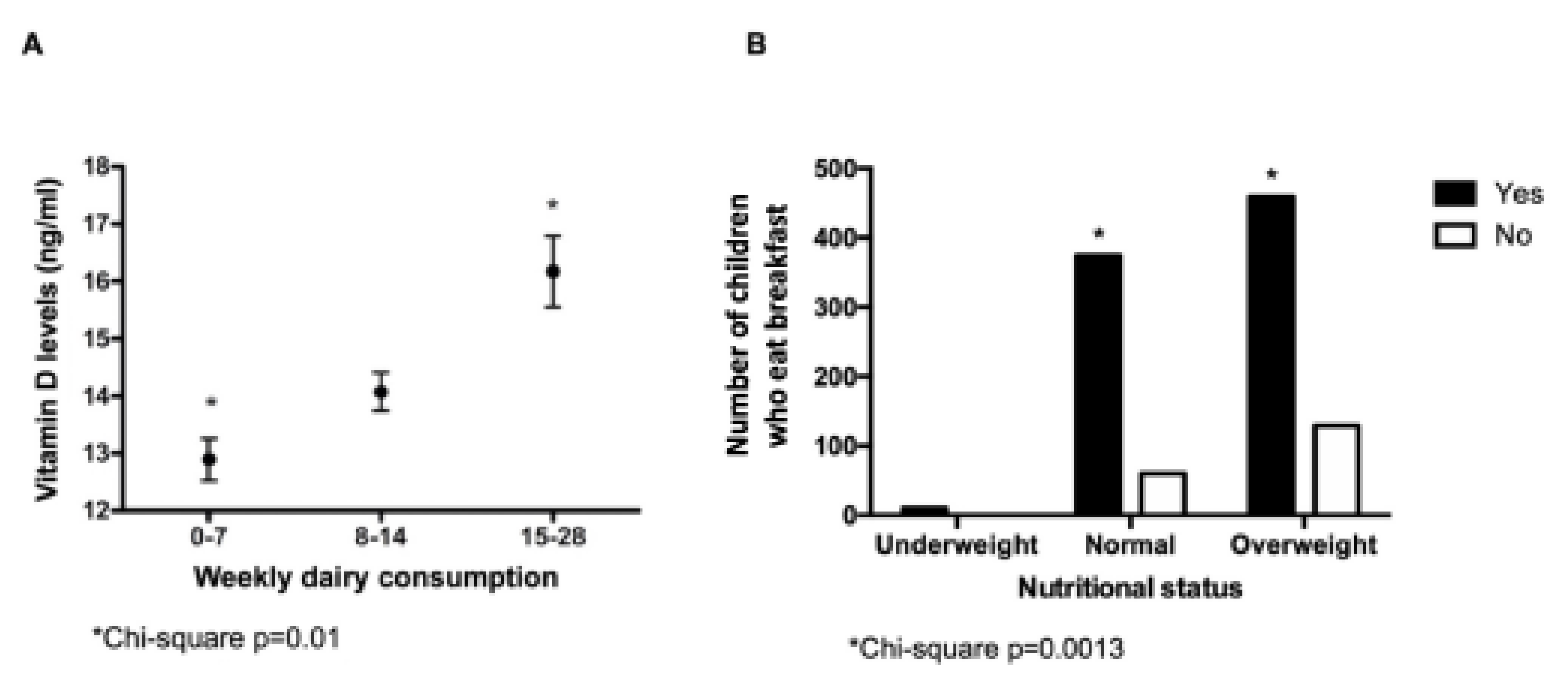
3.2. Analysis of Micronutrients
3.3. Food Consumption and Lifestyle Habits
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rozowski, J.; García-Díaz, D.F.; Pérez-Bravo, F. Nutritional status and biochemical markers of deficiency or excess of micronutrients in 4 to 14 year-old chilean children: A critical review. Nutr. Hosp. 2015, 32, 2916–2925. [Google Scholar]
- FAO. Chile: Nutrition Survey 1961; Interdepartmental Committee on Nutrition for National Defense: Santiago, Chile, 1961. [Google Scholar]
- Universidad de Chile. Encuesta Nacional de Consumo Alimentario [Internet]. Escuela de Nutrición, Universidad de Chile. 2014, p. 329. Available online: http://web.minsal.cl/enca_2014 (accessed on 18 June 2021).
- Caro-Bustos, D.; Uribe-Barra, M.; López-Alegría, F. Obesidad pediátrica y aparición precoz de síndrome cardiometabólico: Revisión sistemática. Rev. Chil. Nutr. 2021, 48, 447–462. [Google Scholar] [CrossRef]
- Organization F and AO of the UN and the PAH. Panorama of Food and Nutrition Security in Latin America and the Caribbean; FAO and PAHO: Santiago, Chile, 2017. [Google Scholar]
- JUNAEB Mapa Nutricional de la Junta Nacional de Auxilio Escolar y Becas 2020 [Internet]. 2022. Available online: https://www.junaeb.cl/wp-content/uploads/2021/03/MapaNutricional2020_.pdf (accessed on 25 January 2022).
- Organisation for Economic Co-operation and Development. Available online: https://data.oecd.org/healthrisk/overweight-or-obese-population.htm (accessed on 25 January 2022).
- Dietz, W.H.; Baur, L.A.; Hall, K.; Puhl, R.M.; Taveras, E.M.; Uauy, R.; Kopelman, P. Management of obesity: Improvement of health-care training and systems for prevention and care. Lancet 2015, 385, 2521–2533. [Google Scholar] [CrossRef] [PubMed]
- INE National Institute of Statistics Report. Vital Birth Statistics 2016. Available online: https://www.ine.gob.cl/docs/default-source/demogr%C3%A1ficas-y-vitales/vitales/anuarios/2016/vitales-2016.pdf?sfvrsn=15 (accessed on 25 January 2022).
- Olivares, S.; Yáñez, R.; Díaz, N. Publicidad de alimentos y conductas alimentarias en escolares de 5° a 8° básico. Rev. Chil. Nutr. 2003, 30, 36–42. [Google Scholar] [CrossRef]
- Child, W.H.O.; Group, W. Growth standards based on length/height, weight and age. Acta Paediatr. Suppl. 2006, 450, 76–85. [Google Scholar]
- Research EES for O and, M. The ESOMAR Standard Demographic Classification: A System of International Socio-Economic Classification of Respondents to Survey Research. In Advances in Cross-National Comparison: A European Working Book for Demographic and Socio-Economic Variables; Springer: Boston, MA, USA, 2003; pp. 97–121. [Google Scholar]
- Liberona, Y.; Castillo, O.; Engler, V.; Villarroel, L.; Rozowski, J. Nutritional profile of schoolchildren from different socio-economic levels in Santiago, Chile. Public Health Nutr. 2011, 14, 142–149. [Google Scholar] [CrossRef] [Green Version]
- Corvalán, C.; Garmendia, M.L.; Jones-Smith, J.; Lutter, C.K.; Miranda, J.J.; Pedraza, L.S.; Popkin, B.M.; Ramirez-Zea, M.; Salvo, D.; Stein, A.D. Nutrition status of children in Latin America. Obes. Rev. 2017, 18, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Shimabuku, R.L.; Delgado, C.A.; Nakachi, G.; Teruya, A.A.; Velasquez, P.M. Double Burden of Excess Weight and Anemia in Latin American Children up to 2019. Tohoku J. Exp. Med. 2020, 252, 159–168. [Google Scholar] [CrossRef]
- Iglesias Vázquez, L.; Valera, E.; Villalobos, M.; Tous, M.; Arija, V. Prevalence of anemia in children from latin america and the caribbean and effectiveness of nutritional interventions: Systematic review and meta–analysis. Nutrients 2019, 11, 183. [Google Scholar] [CrossRef] [Green Version]
- Ministerio de Salud. Encuesta Nacional de Salud 2016–2017 Segunda Entrega de Resultados; Ministerio de Salud: Santiago, Chile, 2018. [Google Scholar]
- Arazo-Rusindo, M.C.; Zúñiga, R.N.; Cortés-Segovia, P.; Benavides-Valenzuela, S.; Pérez-Bravo, F.; Castillo-Valenzuela, O.; Mariotti-Celis, M.S. Nutritional Status and Serum Levels of Micronutrients in an Elderly Group Who Participate in the Program for Complementary Food in Older People (PACAM) from the Metropolitan Region, Santiago de Chile. Nutrients 2021, 14, 3. [Google Scholar] [CrossRef]
- Le Roy, C.; Reyes, M.; González, J.M.; Perez-Bravo, F.; Castillo-Duran, C. Vitamin D nutrition in Chilean pre-school children living in extreme latitudes. Rev. Med. Chil. 2013, 141, 435–441. [Google Scholar] [CrossRef] [Green Version]
- Brinkmann, K.; Le Roy, C.; Iñiguez, G.; Borzutzky, A. Severe vitamin D deficiency in children from Punta Arenas, Chile: Influence of nutritional status on the response to supplementation. Rev. Chil. Pediatría 2015, 86, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Brito, A.; Cori, H.; Olivares, M.; Mujica, M.F.; Cediel, G.; de Romaña, D.L. Less than adequate vitamin D status and intake in Latin America and the Caribbean: A problem of unknown magnitude. Food Nutr. Bull. 2013, 34, 52–64. [Google Scholar] [CrossRef]
- Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellof, M.; Fewtrell, M.; Hojsak, I.; Mihatsch, W.; Molgaard, C.; Shamir, R.; et al. Vitamin D in the healthy European paediatric population. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 692–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lourenço, B.H.; Silva, L.L.S.; Fawzi, W.W.; Cardoso, M.A.; Group, E.W. Vitamin D sufficiency in young Brazilian children: Associated factors and relationship with vitamin A corrected for inflammatory status. Public Health Nutr. 2020, 23, 1226–1235. [Google Scholar] [CrossRef]
- Mujica-Coopman, M.F.; Brito, A.; López de Romaña, D.; Ríos-Castillo, I.; Cori, H.; Olivares, M. Prevalence of anemia in Latin America and the Caribbean. Food Nutr. Bull. 2015, 36 (Suppl. 2), S119–S128. [Google Scholar] [CrossRef] [Green Version]
- Castillo, C.; Balboa, P.; Raimann, X. Modificaciones a la leche del programa Nacional de Alimentación Complementaria (PNAC) en chile. 2009. Rev. Chil. Pediatría 2009, 80, 508–512. [Google Scholar] [CrossRef] [Green Version]
- Díaz, M.S.; Guerra, P.; Campos, M.S.; Letelier, M.A.; Olivares, M. Prevalencia de deficiencia de hierro en preescolares de la comuna La Pintana. Rev. Chil. Nutr. 2002, 29, 10–13. [Google Scholar] [CrossRef]
- Castillo-Duran, C.; García, H.E.; Venegas, P.; Torrealba, I.; Panteon, E.; Concha, N.; Perez, P. Zinc supplementation increases growth velocity of male children and adolescents with short stature. Acta Paediatr. 1994, 83, 833–837. [Google Scholar] [CrossRef] [PubMed]
- Ruz, M. Nutrientes críticos desde el preescolar al adolescente. Rev. Chil. Pediatría 2006, 77, 395–398. [Google Scholar] [CrossRef]
- de Romaña, D.L.; Olivares, M.; Uauy, R.; Araya, M. Risks and benefits of copper in light of new insights of copper homeostasis. J. Trace Elem. Med. Biol. 2011, 25, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Rogers, L.M.; Boy, E.; Miller, J.W.; Green, R.; Sabel, J.C.; Allen, L.H. High prevalence of cobalamin deficiency in Guatemalan schoolchildren: Associations with low plasma holotranscobalamin II and elevated serum methylmalonic acid and plasma homocysteine concentrations. Am. J. Clin. Nutr. 2003, 77, 433–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, M. Situación de Ácido Fólico, Vitamina B12 en Niños, Adolescentes y Mujeres Embarazadas de Venezuela; IVIC-FUNDACREDESA-INN (Instituto Venezolano de Investigaciones Científicas): Caracas, Venezuela, 2003. [Google Scholar]
- Olivares, M.; Llaguno, S.; Cayazzo, M.; Stekel, A. Nutrición de folato en escolares. Rev. Chil. Pediatría 1985, 56, 157–159. [Google Scholar] [CrossRef]
- Mora, J.O.; Gueri, M.; Mora, O.L. Vitamin A deficiency in Latin America and the Caribbean: An overview. Rev. Panam. Salud Pública 1998, 4, 178–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monzani, A.; Ricotti, R.; Caputo, M.; Solito, A.; Archero, F.; Bellone, S.; Prodam, F. A systematic review of the association of skipping breakfast with weight and cardiometabolic risk factors in children and adolescents. What should we better investigate in the future? Nutrients 2019, 11, 387. [Google Scholar] [CrossRef] [Green Version]
- Ruffino, B.; Campo, G.; Crutchik, D.; Reyes, A.; Zanetti, M. Drinking Water Supply in the Region of Antofagasta (Chile): A Challenge between Past, Present and Future. Int. J. Environ. Res. Public Health 2022, 19, 14406. [Google Scholar] [CrossRef]
- da Silva, A.C.; Cureau, F.V.; de Oliveira, C.L.; Giannini, D.T.; Bloch, K.V.; Kuschnir, M.C.; Dutra, E.S.; Schaan, B.D.; de Carvalho, K.M. Physical activity but not sedentary time is associated with vitamin D status in adolescents: Study of cardiovascular risk in adolescents (ERICA). Eur. J. Clin. Nutr. 2019, 73, 432–440. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Antofagasta (n = 410) | Santiago (n = 419) | Concepcion (n = 406) | p-Value | |
|---|---|---|---|---|
| Age (years) | 10.1 ± 2.7 (a) | 9.5 ± 2.7 (b) | 10.0 ± 2.8 (a,b) | 0.010 |
| Weight (Kg) | 46. ± 17.0 (a) | 40.1 ± 15.7 (b) | 42.9 ± 15.9 (b) | 0.001 |
| Height (cm) | 143.0 ± 16.7 (a) | 139.36 ± 17.5 (b) | 142.6 ± 17.2 (c) | 0.012 |
| Waist circumference (cm) | 69.9 ± 12.0 (a) | 64.2 ± 10.6 (b) | 68.2 ± 11.4 (a) | 0.000 |
| BMI (Kg/m2) | 21.7 ± 4.7 (a) | 19.8 ± 3.8 (b) | 20.3 ± 4.1 (b) | 0.000 |
| zBMI/age | 1.2 ± 1.1 | 1.1 ± 1.1 | 1.05 ± 1.1 | 0.320 |
| zHeight/age | 0.50 ± 1.1 (a) | 0.29 ± 1.1 (b) | 0.11 ± 0.9 (c) | 0.000 |
| Region | ||||
|---|---|---|---|---|
| Micronutrients | Antofagasta (n = 410) | Santiago (n = 419) | Concepcion (n = 406) | p-Value |
| Iron (<70 µg/dL) | 15.1 (a) | 19.8 (a) | 26.7 (b) | <0.001 * |
| Copper (<70 µg/dL) | 26.4 (a) | 10.8 (b) | 11.6 (b) | <0.001 * |
| Zinc (<70 µg/dL) | 4.4 (a) | 20.8 (b) | 11.3 (a) | <0.001 * |
| Calcium (<8.8 mg/dL) | 33.0 (a) | 17.7 (b) | 4.7 (b) | <0.001 * |
| Vitamin D (<29.9 ng/mL) | 78.5 | 78.9 | 84.4 | 0.058 |
| Vitamin A (<12 years of age: <0.20 µg/L; >12 years of age: <0.26 µg/L) | 4.9 (a) | 0 (b) | 0.5 (b) | <0.001 * |
| Vitamin E (<12 years of age: <4.0 mg/L; >12 years of age: <6.0 mg/L) | 8.2 (a) | 3.2 (b) | 1.5 (b) | <0.001 * |
| Vitamin B12 < 187 pg/mL | 9.8 (a) | 2.9 (b) | 2.0 (b) | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castillo-Valenzuela, O.; Duarte, L.; Arredondo, M.; Iñiguez, G.; Villarroel, L.; Pérez-Bravo, F. Childhood Obesity and Plasma Micronutrient Deficit of Chilean Children between 4 and 14 Years Old. Nutrients 2023, 15, 1707. https://doi.org/10.3390/nu15071707
Castillo-Valenzuela O, Duarte L, Arredondo M, Iñiguez G, Villarroel L, Pérez-Bravo F. Childhood Obesity and Plasma Micronutrient Deficit of Chilean Children between 4 and 14 Years Old. Nutrients. 2023; 15(7):1707. https://doi.org/10.3390/nu15071707
Chicago/Turabian StyleCastillo-Valenzuela, Oscar, Lissette Duarte, Miguel Arredondo, Germán Iñiguez, Luis Villarroel, and Francisco Pérez-Bravo. 2023. "Childhood Obesity and Plasma Micronutrient Deficit of Chilean Children between 4 and 14 Years Old" Nutrients 15, no. 7: 1707. https://doi.org/10.3390/nu15071707