
Nutrient Patterns and Risk of Osteopenia in Postmenopausal Women
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
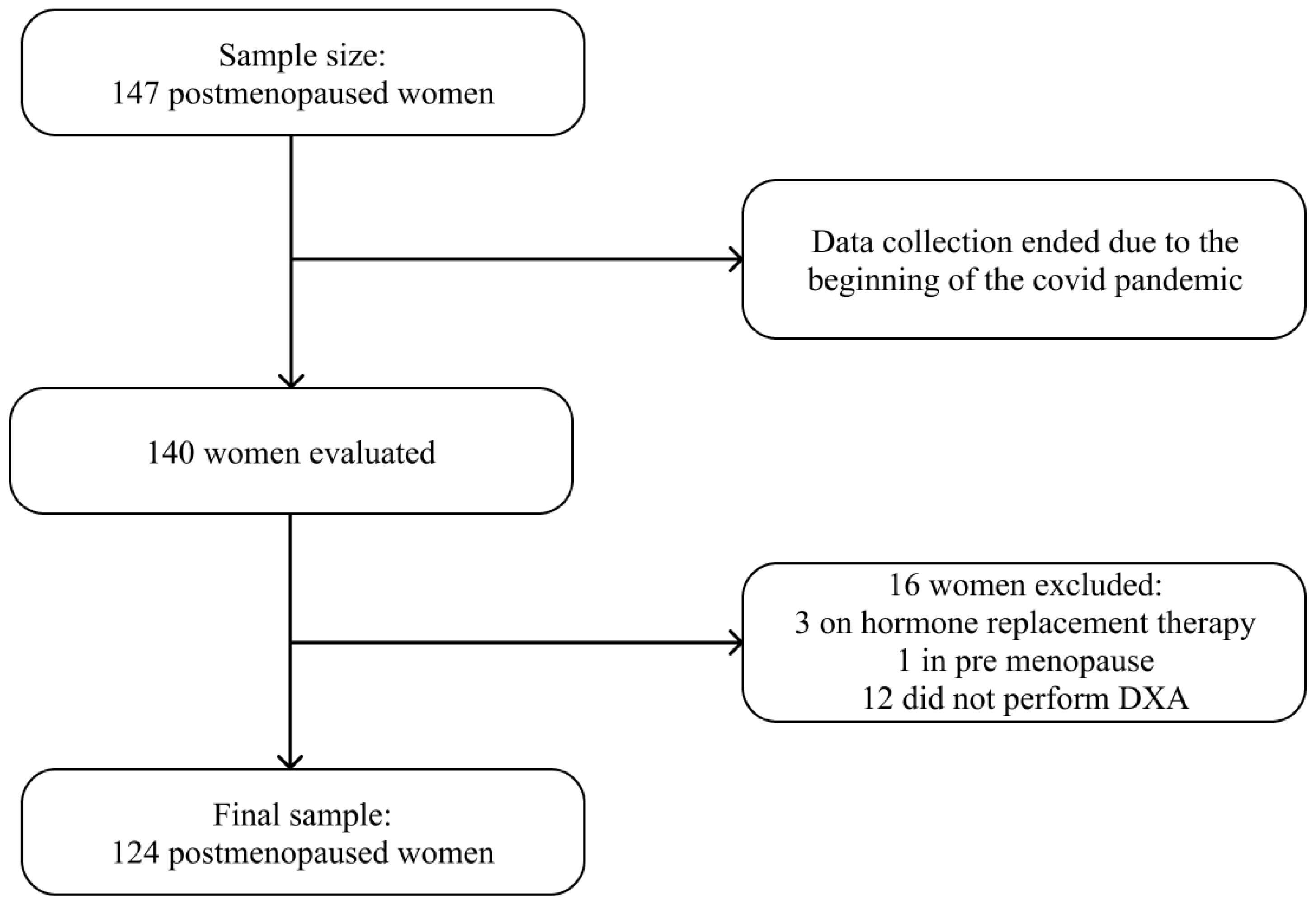
2.1. Study Design, Sample Size, and Population
2.2. Outcome Variable
2.3. Exposure Variable
Nutrient Patterns (NPs)
2.4. Covariates
2.5. Ethical Aspects
2.6. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siris, E.S.; Adler, R.; Bilezikian, J.; Bolognese, M.; Dawson-Hughes, B.; Favus, M.J.; Harris, S.T.; de Beur, S.M.J.; Khosla, S.; Lane, N.E.; et al. The clinical diagnosis of osteoporosis: A position statement from the National Bone Health Alliance Working Group. Osteoporos. Int. 2014, 25, 1439–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, R.D.; Mysiw, W.J. Insights into the epidemiology of postmenopausal osteoporosis: The Women’s Health Initiative. Semin. Reprod. Med. 2014, 32, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Xiao, P.L.; Cui, A.Y.; Hsu, C.J.; Peng, R.; Jiang, N.; Xu, X.H.; Ma, Y.G.; Liu, D.; Lu, H.D. Global, regional prevalence, and risk factors of osteoporosis according to the World Health Organization diagnostic criteria: A systematic review and meta-analysis. Osteoporos. Int. 2022, 33, 2137–2153. [Google Scholar] [CrossRef]
- Davis, S.R.; Lambrinoudaki, I.; Lumsden, M.; Mishra, G.D.; Pal, L.; Rees, M.; Santoro, N.; Simoncini, T. Menopause. Nat. Rev. Dis. Prim. 2015, 1, 15004. [Google Scholar] [CrossRef]
- Eastell, R.; O’Neill, T.W.; Hofbauer, L.C.; Langdahl, B.; Reid, I.R.; Gold, D.T.; Cummings, S.R. Postmenopausal osteoporosis. Nat. Rev. Dis. Primers. 2016, 2, 16069. [Google Scholar] [CrossRef]
- Zaw, J.J.T.; Howe, P.R.C.; Wong, R.H.X. Postmenopausal health interventions: Time to move on from the Women’s Health Initiative? Ageing Res. Rev. 2018, 48, 79–86. [Google Scholar] [CrossRef]
- Aziziyeh, R.; Amin, M.; Habib, M.; Perlaza, J.G.; Szafranski, K.; Mctavish, R.K.; Disher, T.; Lüdke, A.; Cameron, C. The burden of osteoporosis in four Latin American countries: Brazil, Mexico, Colombia, and Argentina. J. Med Econ. 2019, 22, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Baccaro, L.F.; Conde, D.; Costa-Paiva, L.; Pinto-Neto, A.M. The epidemiology and management of postmenopausal osteoporosis: A viewpoint from Brazil. Clin. Interv. Aging 2015, 10, 583. [Google Scholar] [CrossRef] [Green Version]
- Rizzoli, R.; Bischoff-Ferrari, H.; Dawson-Hughes, B.; Weaver, C. Nutrition and Bone Health in Women after the Menopause. Women’s Health 2014, 10, 599–608. [Google Scholar] [CrossRef] [Green Version]
- Rizzoli, R.; Biver, E.; Brennan-Speranza, T.C. Nutritional intake and bone health. Lancet Diabetes Endocrinol. 2021, 9, 606–621. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Moeller, S.M.; Reedy, J.; Millen, A.E.; Dixon, L.B.; Newby, P.K.; Tucker, K.L.; Krebs-Smith, S.M.; Guenther, P.M. Dietary Patterns: Challenges and Opportunities in Dietary Patterns Research. J. Am. Diet. Assoc. 2007, 107, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Karamati, M.; Yousefian-Sanni, M.; Shariati-Bafghi, S.-E.; Rashidkhani, B. Major Nutrient Patterns and Bone Mineral Density among Postmenopausal Iranian Women. Calcif. Tissue Int. 2014, 94, 648–658. [Google Scholar] [CrossRef]
- Melaku, Y.A.; Gill, T.K.; Taylor, A.W.; Adams, R.; Shi, Z. Association between nutrient patterns and bone mineral density among ageing adults. Clin. Nutr. ESPEN 2017, 22, 97–106. [Google Scholar] [CrossRef]
- Ilesanmi-Oyelere, B.L.; Brough, L.; Coad, J.; Roy, N.; Kruger, M.C. The Relationship between Nutrient Patterns and Bone Mineral Density in Postmenopausal Women. Nutrients 2019, 11, 1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilesanmi-Oyelere, B.L.; Kruger, M.C. Nutrient and Dietary Patterns in Relation to the Pathogenesis of Postmenopausal Os-teoporosis—A Literature Review. Life 2020, 10, 220. [Google Scholar] [CrossRef] [PubMed]
- Melaku, Y.; Gill, T.; Appleton, S.; Taylor, A.; Adams, R.; Shi, Z. Prospective Associations of Dietary and Nutrient Patterns with Fracture Risk: A 20-Year Follow-Up Study. Nutrients 2017, 9, 1198. [Google Scholar] [CrossRef] [Green Version]
- Dean, A.G.; Sullivan, K.M.; Soe, M.M. OpenEpi: Open Source Epidemiologic Statistics for Public Health. Version 3.01 (actualized 6 April 2013). Available online: www.OpenEpi.com (accessed on 25 March 2023).
- Baccaro, L.F.; Machado, V.D.S.S.; Costa-Paiva, L.; Sousa, M.H.; Osis, M.J.; Pinto-Neto, A.M. Factors associated with osteoporosis in Brazilian women: A population-based household survey. Arch. Osteoporos. 2013, 8, 138. [Google Scholar] [CrossRef]
- Grili, P.P.D.F.; Vidigal, C.V.; da Cruz, G.F.; Albergaria, B.H.; Marques-Rocha, J.L.; Pereira, T.S.S.; Guandalini, V.R. Dietary consumption of selenium inversely associated with osteoporosis in postmenopausal women. Front. Nutr. 2022, 9, 997414. [Google Scholar] [CrossRef]
- National Health and Nutrition Examination Survey (NHANES). Body Composition Procedures Manual; National Health and Nutrition Examination Survey (NHANES): Washington, DC, USA, 2018; pp. 1–173. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/1999-2000/manuals/bc.pdf (accessed on 25 March 2023).
- World Health Organization (WHO). Assessment of Frature Rish and Its Application to Screening for Postmenopausal Osteo-Porosis; World Health Organization (WHO): Geneva, Switzerland, 1994. [Google Scholar]
- Del Carmen Bisi Molina, M.; Benseñor, I.M.; de Oliveira Cardoso, L.; Velasquez-Melendez, G.; Drehmer, M.; Pereira, T.S.S.; de Faria, C.P.; Melere, C.; Manato, L.; Gomes, A.L.C.G.; et al. Reproducibility and relative validity of the Food Frequency Questionnaire used in the ELSA-Brasil. Cad. Saude Publica 2013, 29, 379–389. [Google Scholar] [CrossRef]
- Mannato, L.W.; Pereira, T.S.S.; Velasquez-Melendez, G.; Cardoso, L.D.O.; Benseñor, I.M.; Molina, M.D.C.B. Comparison of a short version of the Food Frequency Questionnaire with its long version—A cross-sectional analysis in the Brazilian Longitudinal Study of Adult Health [ELSA-Brasil]. Sao Paulo Med. J. 2015, 133, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nutrition Coordinating Center (NCC), University of Minnesota, Minneapolis, United States. Nutrition Data System for Research—NDSR 2010. Available online: http://www.ncc.umn.edu/ (accessed on 25 March 2023).
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical Evaluation of Energy Intake Data Using Fundamental Principles of Energy Physiology: 1. Derivation of Cut-off Limits to Identify underRecording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar] [PubMed]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake: Basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- Ricci, C.; Baumgartner, J.; Wentzel-Viljoen, E.; Smuts, C.M. Food or nutrient pattern assessment using the principal compo-nent analysis applied to food questionnaires. Pitfalls, tips and tricks. Int. J. Food Sci. Nutr. 2019, 70, 738–748. [Google Scholar] [CrossRef]
- Kim, J.O.; Mueller, C.W. Factor Analysis: Statistical Methods and Practical Issues; Sage Publications: Thousand Oaks, CA, USA, 1978. [Google Scholar]
- Instituto Brasileiro de Geografia e Estatística (IBGE); Petruccelli, J.L.; Saboia, A.L. Autoidentificação, Identidade Étnico-Racial e Heteroclassificação; Instituto Brasileiro de Geografia e Estatística (IBGE): Rio de Janeiro, Brazil, 2013. [Google Scholar]
- Matsudo, S.; Araújo, T.; Matsudo, V.; Andrade, D.; Andrade, E.; Oliveira, L.C.; Braggion, G. International Physical Activity Questionnaire [IPAQ]: Study of validity and reliability in Brazil. Ativ. Física Saúde 2001, 6, 5–18. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Guidelines on Physical Activity and Sedentary Behavior; World Health Organization (WHO): Geneva, Switzerland, 2020; ISBN 9789240015128. [Google Scholar]
- World Health Organization (WHO). Physical Status: The Use and Interpretation of Anthropometry; World Health Organization (WHO): Geneva, Switzerland, 1995. [Google Scholar]
- World Health Organization (WHO). Obesity: Preventing and Managing the Global Epidemic; World Health Organization (WHO): Geneva, Switzerland, 2000. [Google Scholar]
- Pan American Health Organization (PAHO). XXXI Reunión del Comité Asesor de Investigaciones en Salud. Rev. Panam. Salud Pública 2002, 1, 471–475. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Garach, A.; García-Fontana, B.; Muñoz-Torres, M. Nutrients and Dietary Patterns Related to Osteoporosis. Nutrients 2020, 12, 1986. [Google Scholar] [CrossRef]
- Weaver, C.M. Nutrition and bone health. Oral Dis. 2017, 23, 412–415. [Google Scholar] [CrossRef]
- Sharma, T.; Mandal, C.C. Omega-3 fatty acids in pathological calcification and bone health. J. Food Biochem. 2020, 44, e13333. [Google Scholar] [CrossRef]
- Shen, D.; Zhang, X.; Li, Z.; Bai, H.; Chen, L. Effects of omega-3 fatty acids on bone turnover markers in postmenopausal women: Systematic review and meta-analysis. Climacteric 2017, 20, 522–527. [Google Scholar] [CrossRef]
- Sadeghi, O.; Djafarian, K.; Ghorabi, S.; Khodadost, M.; Nasiri, M.; Shab-Bidar, S. Dietary intake of fish, n-3 polyunsaturated fatty acids and risk of hip fracture: A systematic review and meta-analysis on observational studies. Crit. Rev. Food Sci. Nutr. 2019, 59, 1320–1333. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, J.K.; Mozaffarian, D.; Willett, W.C.; Feskanich, D. Dietary intake of polyunsaturated fatty acids and risk of hip fracture in men and women. Osteoporos. Int. 2012, 23, 2615–2624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Järvinen, R.; Tuppurainen, M.; Erkkilä, A.T.; Penttinen, P.; Kärkkäinen, M.; Salovaara, K.; Jurvelin, J.S.; Kröger, H. Associations of dietary polyunsaturated fatty acids with bone mineral density in elderly women. Eur. J. Clin. Nutr. 2012, 66, 496–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruger, M.C.; Coetzee, M.; Haag, M.; Weiler, H. Long-chain polyunsaturated fatty acids: Selected mechanisms of action on bone. Prog. Lipid Res. 2010, 49, 438–449. [Google Scholar] [CrossRef] [Green Version]
- Dai, Z.; Koh, W.-P. B-Vitamins and Bone Health–A Review of the Current Evidence. Nutrients 2015, 7, 3322–3346. [Google Scholar] [CrossRef] [Green Version]
- Ma, Q.; Liang, M.; Tang, X.; Luo, F.; Dou, C. Vitamin B5 inhibit RANKL induced osteoclastogenesis and ovariectomy induced osteoporosis by scavenging ROS generation. Am. J. Transl. Res. 2019, 11, 5008–5018. [Google Scholar] [PubMed]
- Fratoni, V.; Brandi, M.L. B Vitamins, Homocysteine and Bone Health. Nutrients 2015, 7, 2176–2192. [Google Scholar] [CrossRef] [Green Version]
- Clarke, M.; Ward, M.; Strain, J.J.; Hoey, L.; Dickey, W.; Mcnulty, H. B-vitamins and bone in health and disease: The current evidence. Proc. Nutr. Soc. 2014, 73, 330–339. [Google Scholar] [CrossRef] [Green Version]
- Yazdanpanah, N.; Zillikens, M.C.; Rivadeneira, F.; de Jong, R.; Lindemans, J.; Uitterlinden, A.G.; Pols, H.A.P.; van Meurs, J.B.J. Effect of dietary B vitamins on BMD and risk of fracture in elderly men and women: The Rotterdam Study. Bone 2007, 41, 987–994. [Google Scholar] [CrossRef]
- Dai, Z.; Wang, R.; Ang, L.W.; Yuan, J.-M.; Koh, W.-P. Dietary B vitamin intake and risk of hip fracture: The Singapore Chinese Health Study. Osteoporos. Int. 2013, 24, 2049–2059. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.R.; Jacques, P.F.; Selhub, J.; Fredman, L.; Tucker, K.L.; Samelson, E.J.; Kiel, D.P.; Cupples, L.A.; Hannan, M.T. Plasma B Vitamins, Homocysteine, and Their Relation with Bone Loss and Hip Fracture in Elderly Men and Women. J. Clin. Endocrinol. Metab. 2008, 93, 2206–2212. [Google Scholar] [CrossRef] [Green Version]
- Cagnacci, A. Relation of homocysteine, folate, and vitamin B12 to bone mineral density of postmenopausal women. Bone 2003, 33, 956–959. [Google Scholar] [CrossRef] [PubMed]
- Golbahar, J.; Hamidi, A.; Aminzadeh, M.A.; Omrani, G.R. Association of plasma folate, plasma total homocysteine, but not methylenetetrahydrofolate reductase C667T polymorphism, with bone mineral density in postmenopausal Iranian women: A cross-sectional study. Bone 2004, 35, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Halıloglu, B.; Aksungar, F.B.; Ilter, E.; Peker, H.; Akın, F.T.; Ozekıcı, U. Relationship between bone mineral density, bone turnover markers and homocysteine, folate and vitamin B12 levels in postmenopausal women. Arch. Gynecol. Obstet. 2010, 281, 663–668. [Google Scholar] [CrossRef]
- Bozkurt, N.; Erdem, M.; Yılmaz, E.; Erdem, A.; Biri, A.; Kubatova, A.; Bozkurt, M. The relationship of homocyteine, B12 and folic acid with the bone mineral density of the femur and lumbar spine in Turkish postmenopausal women. Arch. Gynecol. Obstet. 2009, 280, 381–387. [Google Scholar] [CrossRef]
- Tucker, K.L.; Hannan, M.T.; Qiao, N.; Jacques, P.F.; Selhub, J.; Cupples, L.A.; Kiel, D.P. Low Plasma Vitamin B12 Is Associated with Lower BMD: The Framingham Osteoporosis Study. J. Bone Miner. Res. 2004, 20, 152–158. [Google Scholar] [CrossRef]
- Lowe, N.M.; Fraser, W.D.; Jackson, M.J. Is there a potential therapeutic value of copper and zinc for osteoporosis? Proc. Nutr. Soc. 2002, 61, 181–185. [Google Scholar] [CrossRef]
- Kim, D.E.; Cho, S.H.; Park, H.M.; Chang, Y.K. Relationship between bone mineral density and dietary intake of β-carotene, vitamin C, zinc and vegetables in postmenopausal Korean women: A cross-sectional study. J. Int. Med. Res. 2016, 44, 1103–1114. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.-J.; Huang, M.-N.; Wang, C.-K.; Yang, A.-M.; Lin, C.-Y. Zinc status is independently related to the bone mineral density, fracture risk assessment tool result, and bone fracture history: Results from a U.S. nationally representative survey. J. Trace Elem. Med. Biol. 2021, 67, 126765. [Google Scholar] [CrossRef]
- Qu, X.; He, Z.; Qiao, H.; Zhai, Z.; Mao, Z.; Yu, Z.; Dai, K. Serum copper levels are associated with bone mineral density and total fracture. J. Orthop. Transl. 2018, 14, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Faliva, M.A.; Infantino, V.; Gasparri, C.; Iannello, G.; Perna, S.; Riva, A.; Petrangolini, G.; Tartara, A.; Peroni, G. Copper as Dietary Supplement for Bone Metabolism: A Review. Nutrients 2021, 13, 2246. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Michaëlsson, K.; Olofsson, H.; Johansson, S.; Melhus, H. Association between Oxidative Stress and Bone Mineral Density. Biochem. Biophys. Res. Commun. 2001, 288, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Jacob, R.A.; Bowen, P.E. Update on the Biological Characteristics of the Antioxidant Micronutrients. J. Am. Diet. Assoc. 1996, 96, 693–702. [Google Scholar] [CrossRef]
- Zeng, H.; Cao, J.; Combs, G. Selenium in Bone Health: Roles in Antioxidant Protection and Cell Proliferation. Nutrients 2013, 5, 97–110. [Google Scholar] [CrossRef] [Green Version]
- Wallace, T.C.; Marzorati, M.; Spence, L.; Weaver, C.M.; Williamson, P.S. New Frontiers in Fibers: Innovative and Emerging Research on the Gut Microbiome and Bone Health. J. Am. Coll. Nutr. 2017, 36, 218–222. [Google Scholar] [CrossRef] [Green Version]
- Jakeman, S.A.; Henry, C.N.; Martin, B.R.; McCabe, G.P.; McCabe, L.D.; Jackson, G.S.; Peacock, M.; Weaver, C.M. Soluble corn fiber increases bone calcium retention in postmenopausal women in a dose-dependent manner: A randomized crossover trial. Am. J. Clin. Nutr. 2016, 104, 837–843. [Google Scholar] [CrossRef] [Green Version]
- Weaver, C.M.; Martin, B.R.; Story, J.A.; Hutchinson, I.; Sanders, L. Novel fibers increase bone calcium content and strength beyond efficiency of large intestine fermentation. J. Agric. Food Chem. 2010, 58, 8952–8957. [Google Scholar] [CrossRef]
- Lobo, A.R.; Colli, C.; Filisetti, T.M.C.C. Fructooligosaccharides improve bone mass and biomechanical properties in rats. Nutr. Res. 2006, 26, 413–420. [Google Scholar] [CrossRef]
- Mudgil, D. The interaction between insoluble and soluble fiber. In Dietary Fiber for the Prevention of Cardiovascular Disease; Elsevier: Amsterdam, The Netherlands, 2017; pp. 35–59. [Google Scholar]
- Ebeling, P.R.; Nguyen, H.H.; Aleksova, J.; Vincent, A.J.; Wong, P.; Milat, F. Secondary Osteoporosis. Endocr. Rev. 2022, 43, 240–313. [Google Scholar] [CrossRef]
- De Kam, D.; Smulders, E.; Weerdesteyn, V.; Smits-Engelsman, B.C.M. Exercise interventions to reduce fall-related fractures and their risk factors in individuals with low bone density: A systematic review of randomized controlled trials. Osteoporos. Int. 2009, 20, 2111–2125. [Google Scholar] [CrossRef] [PubMed]
- Marín-Cascales, E.; Alcaraz, P.E.; Ramos-Campo, D.J.; Rubio-Arias, J.A. Effects of multicomponent training on lean and bone mass in postmenopausal and older women: A systematic review. Menopause 2018, 25, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Howe, T.E.; Shea, B.; Dawson, L.J.; Downie, F.; Murray, A.; Ross, C.; Harbour, R.T.; Caldwell, L.M.; Creed, G. Exercise for preventing and treating osteoporosis in postmenopausal women. Cochrane Database Syst. Rev. 2011, 7, CD000333. [Google Scholar] [CrossRef]
- Pinheiro, M.B.; Oliveira, J.; Bauman, A.; Fairhall, N.; Kwok, W.; Sherrington, C. Evidence on physical activity and osteoporosis prevention for people aged 65+ years: A systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 150. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 7, e2014009. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Total (n = 124) | BMD | p Value | ||
|---|---|---|---|---|---|
| Normal (n = 27) | Osteopenia (n = 52) | Osteoporosis (n = 45) | |||
| Mean ± SD | |||||
| Age (years) | 66.8 ± 6.1 | 64.2 a ± 5.3 | 66.6 a ± 6.0 | 68.6 b ± 6.1 | 0.010 |
| Time since menopause (years) | 19.6 ± 8.8 | 14.6 a ± 9.4 | 20.1 b ± 7.7 | 22.2 b ± 8.6 | 0.002 |
| BMI (kg/m2) | 27.3 ± 4.7 | 30.0 a ± 4.2 | 27.7 a ± 4.6 | 25.2 b ± 4.1 | <0.001 |
| n (%) | |||||
| Age group (years) † | 0.022 | ||||
| 50.0–59.9 | 13 (10.5) | 5 (38.5) | 7 (53.8) | 1 (7.7) | |
| 60.0–69.9 | 74 (59.7) | 19 (25.7) | 28 (37.8) | 27 (36.5) | |
| ≥70.0 | 37 (39.8) | 3 (8.1) | 17 (45.9) | 17 (45.9) | |
| Color * | 0.068 | ||||
| White | 47 (37.9) | 9 (19.1) | 15 (31.9) | 23 (48.9) | |
| Non-white | 77 (62.1) | 18 (23.4) | 37 (48.1) | 22 (38.6) | |
| Marital status * | 0.079 | ||||
| No partner | 60 (48.4) | 8 (13.3) | 29 (48.3) | 23 (38.3) | |
| With partner | 64 (51.6) | 19 (29.7) | 23 (35.9) | 22 (34.4) | |
| Education level † | 0.256 | ||||
| No schooling | 11 (8.9) | - | 7 (63.6) | 4 (36.4) | |
| Elementary school | 75 (60.5) | 19 (25.3) | 26 (34.7) | 30 (40.0) | |
| High school | 27 (21.8) | 6 (22.2) | 12 (44.4) | 9 (7.3) | |
| University education | 11 (8.9) | 2 (18.2) | 7 (63.6) | 2 (18.2) | |
| Employment status † | 0.616 | ||||
| Employed | 21 (16.9) | 6 (28.6) | 9 (42.9) | 6 (28.6) | |
| Unemployed | 103 (83.1) | 21 (20.4) | 43 (41.7) | 39 (37.9) | |
| Physical active level * | 0.351 | ||||
| Insufficiently active | 62 (50.0) | 16 (25.8) | 27 (43.5) | 19 (30.6) | |
| Sufficiently active | 62 (50.0) | 11 (17.7) | 25 (40.3) | 26 (41.9) | |
| Smoking † | 0.499 | ||||
| Smoker | 6 (4.8) | - | 3 (50.0) | 3 (50.0) | |
| Non-smoker | 118 (95.2) | 27 (22.9) | 49 (41.5) | 42 (35.6) | |
| Alcohol consumption † | 0.794 | ||||
| Consume | 17 (13.7) | 4 (23.5) | 8 (47.1) | 5 (29.4) | |
| Does not consume | 107 (86.3) | 23 (21.5) | 44 (35.5) | 40 (37.4) | |
| Nutritional status † | <0.001 | ||||
| Underweight | 21 (16.9) | - | 6 (28.6) | 15 (71.4) | |
| Normal weight | 53 (42.7) | 9 (17.0) | 23 (43.4) | 21 (39.6) | |
| Overweight | 18 (14.5) | 7 (38.9) | 7 (38.9) | 4 (22.2) | |
| Obese | 32 (25.8) | 11 (34.4) | 16 (50.0) | 5 (15.2) | |
| Ca supplementation * | <0.001 | ||||
| Yes | 81 (65.3) | 9 (11.1) | 35 (43.2) | 37 (45.7) | |
| No | 43 (34.7) | 18 (41.9) | 17 (39.5) | 8 (18.6) | |
| Vit. D supplementation * | <0.001 | ||||
| Yes | 71 (57.3) | 7 (21.8) | 31 (43.7) | 33 (46.5) | |
| No | 53 (42.7) | 20 (37.7) | 21 (39.6) | 12 (22.6) | |
| Antiresorptive drugs † | <0.001 | ||||
| Yes | 58 (46.8) | 2 (3.4) | 21 (36.2) | 35 (60.3) | |
| No | 66 (53.2) | 25 (37.9) | 31 (47.0) | 10 (15.2) | |
| Nutrients | Total (n = 124) | BMD | p Value | ||
|---|---|---|---|---|---|
| Normal (n = 27) | Osteopenia (n = 52) | Osteoporosis (n = 45) | |||
| Energy (kcal/d) | 2013.1 ± 791.4 | 2178.4 ± 729.3 | 1910.6 ± 818.3 | 2032.3 ± 794.3 | 0.357 |
| Carbohydrate (g/d) | 259.0 ± 40.0 | 276.2 a ± 45.8 | 241.5 b ± 34.7 | 268.8 a ± 34.6 | <0.001 |
| Protein (g/d) | 87.6 ± 18.1 | 94.3 a ± 17.6 | 83.6 b ± 17.5 | 88.2 a,b ± 18.1 | 0.040 |
| Animal Protein (g/d) | 55.6 ± 19.9 | 59.3 ± 20.3 | 54.2 ± 20.0 | 55.2 ± 19.6 | 0.537 |
| Vegetal Protein (g/d) | 31.6 ± 9.9 | 34.5 a ± 10.9 | 29.0 b ± 7.1 | 32.9 a,b ± 8.7 | 0.014 |
| Total Fat (g/d) | 57.2 ± 12.6 | 66.9 a± 15.2 | 53.2 b ± 10.6 | 55.9 b ± 10.1 | <0.001 |
| Total Fibers (g/d) | 27.0 ± 8.0 | 27.6 ± 10.5 | 25.3 ± 6.2 | 28.5 ± 8.0 | 0.254 |
| Soluble Fibers (g/d) | 6.9 ± 2.1 | 6.7 ± 2.3 | 6.6 ± 2.0 | 7.3 ± 2.1 | 0.182 |
| Insoluble Fibers (g/d) | 19.7 ± 7.2 | 20.3 ± 10.2 | 18.3 ± 5.3 | 20.9 ± 6.9 | 0.249 |
| Cholesterol (g/d) | 257.6 ± 115.9 | 287.9 ± 126.5 | 253.0 ± 127.1 | 244.7 ± 92.9 | 0.304 |
| Saturated Fatty Acids (g/d) | 19.1 ± 5.9 | 22.5 a ± 7.4 | 17.3 b ± 4.8 | 19.2 b ± 5.3 | 0.001 |
| MUFA (g/d) | 17.6 ± 4.7 | 20.6 a ± 5.6 | 16.5 b ± 4.5 | 17.1 b ± 3.6 | 0.001 |
| PUFA(g/d) | 14.4 ± 3.4 | 16.6 a ± 3.1 | 13.7 b ± 2.7 | 14.0 b ± 3.8 | 0.001 |
| Trans Fatty Acids (g/d) | 1.3 ± 0.6 | 1.3 ± 0.5 | 1.2 ± 0.6 | 1.3 ± 0.6 | 0.453 |
| Vitamin A (UI/d) | 4903.0 ± 3617.0 | 5014.4 ± 2836.2 | 4509.9 ± 2634.2 | 5290.4 ± 4840.3 | 0.763 |
| Beta Carotene (µg/d) | 245.2 ± 141.5 | 274.7 ± 115.2 | 206.4 ± 115.2 | 272.4 ± 188.4 | 0.065 |
| Retinol (µg/d) | 1163.9 ± 635.9 | 1213.1 ± 529.9 | 1048.6 ± 458.6 | 1267.7 ± 832.1 | 0.314 |
| Vitamin D (µg/g) | 11.5 ± 10.4 | 16.0 ± 14.1 | 9.5 ± 7.4 | 11.1 ± 10.1 | 0.157 |
| Alpha Tocopherol (mg/d) | 8.7 ± 3.0 | 10.2 a ± 3.3 | 8.0 b ± 2.3 | 8.7 a,b ± 3.4 | 0.008 |
| Vitamin E (mg/d) | 7.2 ± 2.6 | 8.4 a ± 3.0 | 6.6 b ± 2.0 | 7.3 a,b ± 2.9 | 0.023 |
| Vitamin K (mcg/d) | 270.7 ± 258.4 | 282.6 ± 156.7 | 249.8 ± 172.7 | 287.7 ± 369.8 | 0.467 |
| Vitamin C (mg/d) | 184.3 ± 107.8 | 209.6 ± 107.0 | 162.6 ± 87.5 | 194.3 ± 125.6 | 0.103 |
| Thiamine (mg/d) | 1.8 ± 0.3 | 2.1 a ± 0.3 | 1.6 b ± 0.2 | 1.8 c ± 0.3 | <0.001 |
| Riboflavin (mg/d) | 1.8 ± 0.4 | 2.1 a ± 0.4 | 1.7 b ± 0.3 | 1.9 a ± 0.5 | <0.001 |
| Niacin (mg/d) | 24.1 ± 6.7 | 25.0 ± 6.5 | 23.3 ± 6.9 | 24.5 ± 6.6 | 0.520 |
| Pantothenic Acid (mg/d) | 6.2 ± 1.1 | 6.7 a ± 1.3 | 5.8 b ± 0.9 | 6.3 a,b ± 1.1 | 0.003 |
| Vitamin B6 (mg/d) | 2.3 ± 0.5 | 2.4 ± 0.6 | 2.2 ± 0.4 | 2.3 ± 0.4 | 0.106 |
| Folate (µg/d) | 509.8 ± 138.8 | 565.1 a ± 178.4 | 460.6 b ± 100.1 | 533.5 a ± 134.6 | 0.010 |
| Vitamin B12 (µg/d) | 3.4 ± 1.4 | 4.1 a ± 1.6 | 3.0 b ± 1.1 | 3.5 a,b ± 1.4 | 0.004 |
| Calcium (mg/d) | 742.4 ± 288.5 | 854.7 a ± 269.5 | 642.4 b ± 210.8 | 790.6 a ± 341.2 | 0.003 |
| Phosphorus (mg/d) | 1230.9 ± 249.3 | 1367.0 a ± 264.0 | 1134.0 b ± 188.5 | 1261.3 a ± 260.7 | <0.001 |
| Magnesium (mg/d) | 329.3 ± 74.7 | 358.5 ± 92.0 | 306.7 ± 58.7 | 337.7 ± 73.3 | 0.008 |
| Iron (mg/d) | 12.6 ± 2.3 | 13.9 a ± 2.7 | 11.9 b ± 1.9 | 12.8 a,b ± 2.3 | 0.001 |
| Zinc (mg/d) | 10.5 ± 2.1 | 11.6 a ± 2.0 | 9.8 b ± 2.1 | 10.5 a,b ± 1.9 | <0.001 |
| Copper (mg/d) | 1.5 ± 0.4 | 1.6 ± 0.6 | 1.4 ± 0.3 | 1.6 ± 0.5 | 0.145 |
| Selenium (µg/d) | 154.4 ± 88.7 | 189.6 a ± 104.6 | 149.0 b ± 89.7 | 139.4 b ± 72.0 | <0.001 |
| Sodium (mg/d) | 2971.1 ± 596.7 | 3247.0 a ± 463.5 | 2777.7 b ± 441.3 | 3029.1 a,b ± 740.4 | 0.002 |
| Potassium (mg/d) | 3216.8 ± 667.4 | 3480.8 a ± 805.4 | 2969.1 b ± 805.4 | 3344.6 a ± 647.3 | 0.001 |
| Total Sugar (g/d) | 88.1 ± 30.6 | 96.4 ± 35.6 | 81.1 ± 28.8 | 91.1 ± 28.3 | 0.052 |
| Omega-3 (g/d) | 2.4 ± 1.1 | 3.0 a ± 1.4 | 2.2 b ± 0.8 | 2.3 b ± 1.1 | 0.012 |
| Nutrients | Factor Loadings | ||
|---|---|---|---|
| NP1 | NP2 | NP3 | |
| Vitamin B12 | 0.864 | −0.094 | −0.169 |
| Pantothenic Acid | 0.846 | 0.162 | 0.274 |
| Phosphorus | 0.837 | 0.286 | −0.052 |
| Riboflavin | 0.757 | 0.078 | 0.019 |
| Animal Protein | 0.742 | −0.219 | −0.346 |
| Total Protein | 0.719 | 0.179 | −0.343 |
| Vitamin B6 | 0.683 | 0.188 | 0.242 |
| Potassium | 0.662 | 0.332 | −0.576 |
| Vitamin D | 0.659 | 0.227 | 0.095 |
| Vitamin E | 0.568 | 0.535 | 0.275 |
| Calcium | 0.552 | −0.061 | −0.041 |
| Cholesterol | 0.537 | −0.161 | −0.180 |
| β-Carotene | 0.537 | −0.314 | −0.071 |
| Omega 3 | 0.536 | 0.524 | −0.014 |
| Magnesium | 0.437 | 0.702 | 0.366 |
| Zinc | 0.466 | 0.268 | −0.459 |
| Niacin | 0.433 | 0.122 | −0.178 |
| Selenium | 0.347 | 0.295 | −0.140 |
| Iron | −0.128 | 0.866 | −0.138 |
| Vegetal Protein | −0.207 | 0.864 | 0.104 |
| Thiamine | 0.081 | 0.798 | −0.149 |
| Folate | 0.026 | 0.787 | 0.289 |
| Insoluble Fibers | 0.048 | 0.703 | 0.392 |
| PUFA | 0.220 | 0.664 | −0.417 |
| Total Fibers | 0.078 | 0.681 | 0.498 |
| Vitamin A | 0.117 | 0.530 | 0.285 |
| Vitamin K | 0.061 | 0.611 | 0.037 |
| Alpha-Tocopherol | 0.529 | 0.606 | 0.218 |
| Copper | 0.083 | 0.580 | 0.204 |
| Sodium | −0.047 | 0.438 | −0.287 |
| Retinol | 0.247 | 0.470 | 0.303 |
| Carbohydrate | −0.353 | 0.200 | 0.691 |
| Total Sugar | 0.173 | −0.239 | 0.671 |
| Soluble Fiber | 0.203 | 0.247 | 0.539 |
| Vitamin C | 0.357 | 0.159 | 0.485 |
| Total Fat | 0.385 | 0.015 | −0.765 |
| MUFA | 0.363 | −0.052 | −0.758 |
| Saturated Fatty Acids | 0.321 | −0.284 | −0.634 |
| Trans Fatty Acids | 0.054 | −0.159 | −0.520 |
| Explicated Variance | 21.9% | 20.4% | 14.4% |
| Osteopenia | Osteoporosis | |||||||
|---|---|---|---|---|---|---|---|---|
| Crude Model OR (CI 95%) | Model 1 OR (CI 95%) | Model 2 OR (CI 95%) | Model 3 OR (CI 95%) | Crude Model OR (CI 95%) | Model 1 OR (CI 95%) | Model 2 OR (CI 95%) | Model 3 OR (CI 95%) | |
| NP1 | ||||||||
| 1st T | 6.00 (1.73–20.82) | 6.66 (1.75–25.35) | 6.65 (1.61–27.53) | 6.64 (1.56–28.16) | 2.80 (0.81–9.74) | 2.61 (0.62–10.90) | 2.50 (0.45–13.74) | 2.44 (0.43–13.78) |
| 2nd T | 3.70 (1.15–11.86) | 3.65 (1.05–12.64) | 4.94 (1.31–18.55) | 5.15 (1.32–20.07) | 2.29 (0.73–7.15) | 1.78 (0.48–6.65) | 3.34 (0.68–16.33) | 3.48 (0.68–17.66) |
| NP2 | ||||||||
| 1st T | 4.84 (1.37–17.09) | 5.06 (1.35–18.98) | 4.99 (1.27–19.65) | 5.03 (1.25–20.32) | 2.98 (0.87–10.16) | 3.25 (0.81–13.00) | 3.13 (0.63–15.65) | 3.23 (0.63–16.67) |
| 2nd T | 3.50 (1.13–10.84) | 3.67 (1.10–12.18) | 3.54 (0.99–12.59) | 3.59 (0.98–13.13) | 1.31 (0.42–4.13) | 1.40 (0.38–5.21) | 1.24 (0.26–5.92) | 1.22 (0.25–6.07) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grili, P.P.d.F.; Vidigal, C.V.; Cruz, G.F.d.; Albergaria, B.-H.; Marques-Rocha, J.L.; Pereira, T.S.S.; Guandalini, V.R. Nutrient Patterns and Risk of Osteopenia in Postmenopausal Women. Nutrients 2023, 15, 1670. https://doi.org/10.3390/nu15071670
Grili PPdF, Vidigal CV, Cruz GFd, Albergaria B-H, Marques-Rocha JL, Pereira TSS, Guandalini VR. Nutrient Patterns and Risk of Osteopenia in Postmenopausal Women. Nutrients. 2023; 15(7):1670. https://doi.org/10.3390/nu15071670
Chicago/Turabian StyleGrili, Patricia Paula da Fonseca, Camila Vilarinho Vidigal, Geise Ferreira da Cruz, Ben-Hur Albergaria, José Luiz Marques-Rocha, Taísa Sabrina Silva Pereira, and Valdete Regina Guandalini. 2023. "Nutrient Patterns and Risk of Osteopenia in Postmenopausal Women" Nutrients 15, no. 7: 1670. https://doi.org/10.3390/nu15071670