

Experiences and Attitudes of Parents Reducing Carbohydrate Intake in the Management of Their Child’s Type 1 Diabetes: A Qualitative Study
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Data Collection
2.3. Data Analysis
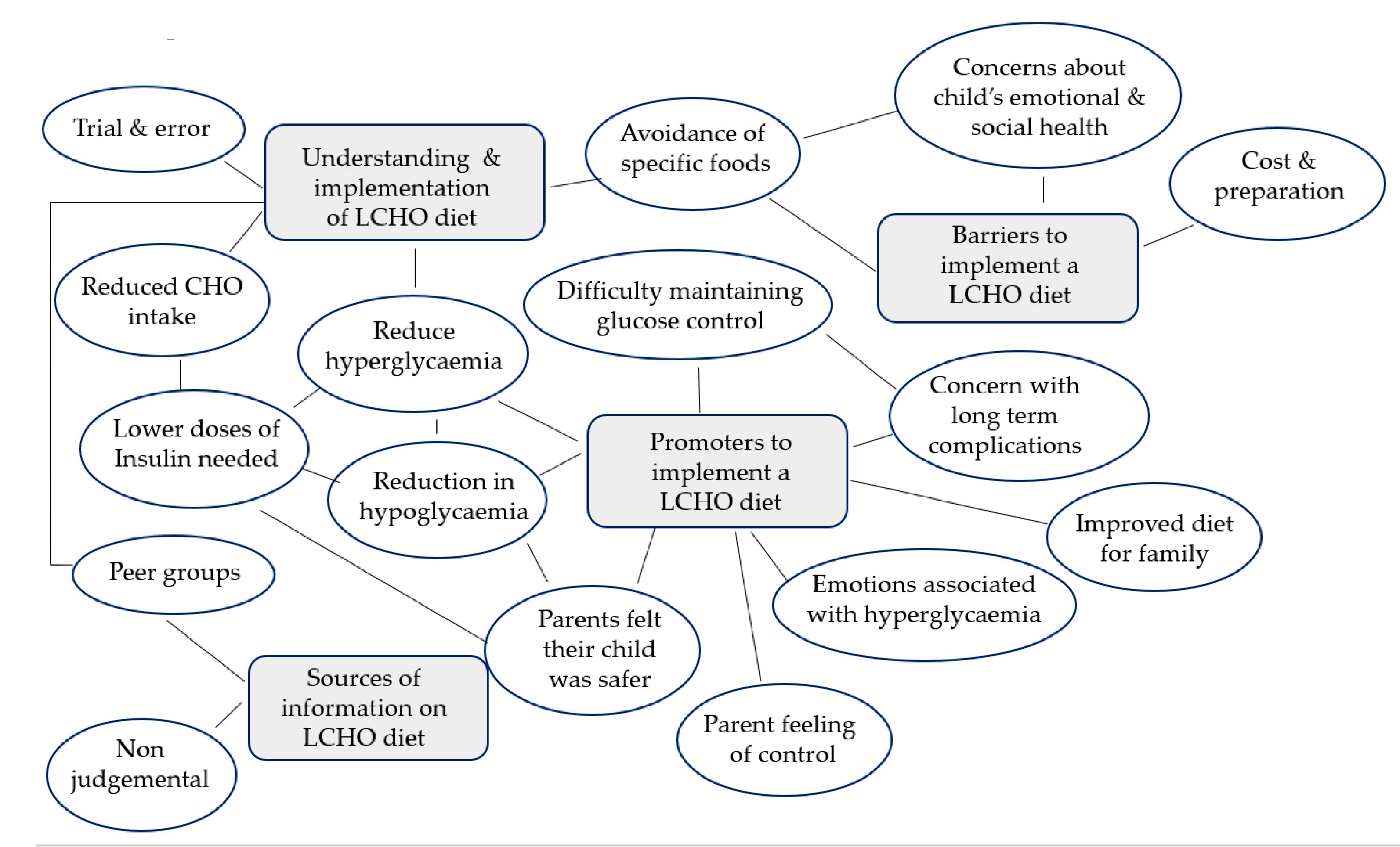
3. Results
3.1. Understanding and Implementation of Low CHO Diets
“I avoid flour at all costs. If I do need to add flour, I’ll halve the amount I need to put in, and I’ll substitute the rest with almond meal, or coconut flour. I do a lot of that kind of stuff as well, err, just because flour’s just a killer, I feel.”(Participant 11)
“So initially we were probably around 30 g per day of carbs, or little more with some snacks. Now, some days might be a little under some might be a bit over but usually I would say it’s still probably less than 50 g a day of carbohydrate, and that usually comes in the form of vegetables, some small amount in some cheeses, nuts.”(Participant 5)
“…I’ll let him eat the cakes and lollies and stuff that are there [party]. It’ll be one of those special treat days that he gets.”(Participant 11)
“We do lot of alternative things… he does sometimes have bread but it’s a low carb bread, but then we do a lot more of the… wraps, things like that. We don’t bail everything out.”(Participant 12)
“…little gift bag with some toys instead of lollies and she’s really happy with that.(Participant 10)
“yeah, or they’re like, even, like one, one grape its ok. Like the other day he was 5.6 and I was trying to get it back down to a bit more normal… “can’t he just have one piece of fruit?” but that fruit will take him from 5.6 to 7 or 8 and that’s when he’ll already feel bad.”(Participant 1)
“The first meal we did was breakfast and, oh my god what a difference… we never did the normal cereals or anything like that. But we replaced it with an omelette. And oh my god, that just changed our day. Like, you know as soon as you start off with fabulous flat numbers, you can just carry on…”(Participant 6)
3.2. Promoters to Implementing a Low CHO Diet
“…the first 6 months was just a complete blur of like not really knowing what on earth was going on.”(Participant 9)
“as we just changed things slowly it just flattened right out. Yeah, so anyway that’s usually when I showed people when they say “why, why do you do that?” Like, this is why!”(Participant 5)
“They’re so much less at risk because you haven’t got this huge amount of insulin on board that’s going to, you know, cause some kind of disaster. You know, like a real emergency.”(Participant 6)
“Hypos are much easier to treat than hypers definitely. Phenomenally more easy and much quicker recovery as well.”(Participant 9)
“…but nothing like the stress of trying to get a super high level down.”(Participant 5)
“I think his last A1C was 6.3 before we went low carb and then that went to 5.3 as soon as we went low carb.”(Participant 6)
“I feel guilty to be honest…. cause I hate to see him higher, and I worry about the damage that it’s doing to his body.”(Participant 15)
“I feel so much better doing it, like I feel I’ve got so much more energy, and feel so much, like I lose weight and everything. For me if I eat more meat and vegetables without all the other stuff um, yeah, but it’s better for me, I know.”(Participant 4)
“…If he hits the number 6.0, or if he hits the number 3.8, he’s going to get emotional and upset and that’s not a good way to remember your birthday… let’s say you’ve got all your friends you’re in the middle of a party and you’re crying in the corner because you’re low or your high… that affects you emotionally.”(Participant 1)
“She was such a grumpy bum. She’s so much happier and more relaxed and you know more confident when her levels are level.”(Participant 8)
“…He will generally say “I think I’m a bit high, mum” and I say “do you think that’s why you’re a bit grumpy?” he goes “yeah”. And I say “you know what?” I said “that’s alright, we’ll just bring you down, what can we do?”(Participant 12)
3.3. Barriers to Implementing a Low CHO Diet
“…Another disadvantage is just that that level of organisation and, and sometimes the cooking, you know having to cook all the time, alternative type foods”.(Participant 7)
“Probably the cost involved–um, ‘cause higher, our weekly shopping list has gone up quite a bit which might be hard for some families. Um, yeah for us we’re quite fortunate that yeah, we can be in that position.”(Participant 4)
“I find that a lot of the recipes that I end up applying are for low keto diets, and I get a bit wary of keto… a lot of the time they are high in fat.”(Participant 11)
“there’s guilt and a bit of doubt a bit of self-doubt that I’m maybe not doing the right thing–am I for this period of time stunting her growth? I don’t know.”(Participant 10)
“We are very careful…my oldest is having his normal lunch box. And [child] never see me like, prepare. [Child] never sees me when I’m making it”(Participant 2)
“We’re sort of worried if he meets someone else with diabetes and they don’t eat the way he does.”(Participant 1)
“If we go to a birthday party or if I’m aware of some sort of treat happening at school, I will give her something … that she likes.”(Participant 10)
“Everyone has learned to have new favourites–like we’ve got an almond porridge that all of the kids really love to eat…”(Participant 5)
3.4. Sources of Information on Low CHO Diets
“I have been too scared to even tell them we’re low-carb because of what happens–what other people say.”(Participant 3)
“I’ve been told constantly by other parents just to not bring up low carb I’m saying this honestly, every single parents tell me to not bring up low carb with clinic, so the dietitians or anyone, just avoid it.”(Participant 8)
“I just shared how hard things were on Facebook one day and a friend of mine from college who has type one, she actually sent me a private message and asked if we’d ever heard about managing with low carb foods.”(Participant 5)
“And it’s a group of low-carb, Type 1 Mums from all around the world and that is my saviour, that’s my group. We can, we laugh, we–fricken cry, we share appropriate jokes, and it really is my one.”(Participant 6)
“I ordered that book [Diabetes Solution by Dr Bernstein] that same day because I just thought–we need some direction, we need to try something because what we’ve tried is not working.”(Participant 5)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Interview Guide
- What understanding do parents have of low CHO diets?
- What are the perceived promoters and barriers to implementing a low CHO diet?
- Where do parents get their information about implementing a low CHO diet?
- How do parents perceive their child’s/family’s enjoyment of a low CHO diet?
- Do parents have any perceived concerns regarding a low CHO diet?
- Icebreaker
- Explain that all questions are valid and there are no ‘wrong’ answers.
- Explain that we want to know more to help guide future research.
- 1.
- Tell me about your experiences of giving your child a low CHO diet?
- 2.
- What do you understand to be a low CHO diet?
- a.
- Are there any specific foods that you try to include or limit?
- 3.
- What benefits have you noticed since having your child on a low CHO diet?
- 4.
- Can you identify any negatives to following a low CHO diet?
- a.
- Do you have any concerns about giving your child a low CHO diet?
- b.
- Do you think it causes you or your child added stress?
- 5.
- How often do you implement a low CHO diet?
- a.
- Do you feel supported by your family members to give your child this diet?
- b.
- Does the whole family follow a low CHO diet?
- c.
- Does your child enjoy the food you offer?
- 6.
- Where do you get your information/advice regarding low CHO diets?
- a.
- Are you actively involved in any online forums related to low CHO diets?
- 7.
- Do you have any other comments or feelings about low CHO diets in T1D?
References
- Newburgh, L.H.; Marsh, M.D. The use of a high fat diet in the treatment of diabetes mellitus: Second paper: Blood sugar. Arch. Intern. Med. 1921, 27, 699–705. [Google Scholar] [CrossRef] [Green Version]
- Smart, C.E.; Annan, F.; Higgins, L.A.; Jelleryd, E.; Lopez, M.; Acerini, C.L. ISPAD Clinical Practice Consensus Guidelines 2018: Nutritional management in children and adolescents with diabetes. Pediatr. Diabetes 2018, 19, 136–154. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, E.; Kizirian, N.V.; Partridge, S.R.; Gill, T.; Colagiuri, S.; Gibson, A.A. Effect of dietary carbohydrate restriction on glycemic control in adults with diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2018, 139, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Turton, J.L.; Raab, R.; Rooney, K.B. Low-carbohydrate diets for type 1 diabetes mellitus: A systematic review. PLoS ONE 2018, 13, e0194987. [Google Scholar] [CrossRef] [Green Version]
- Krebs, J.D.; Parry Strong, A.; Cresswell, P.; Reynolds, A.N.; Hanna, A.; Haeusler, S. A randomised trial of the feasibility of a low carbohydrate diet vs standard carbohydrate counting in adults with type 1 diabetes taking body weight into account. Asia Pac. J. Clin. Nutr. 2016, 25, 78–84. [Google Scholar]
- Nielsen, J.V.; Gando, C.; Joensson, E.; Paulsson, C. Low carbohydrate diet in type 1 diabetes, long-term improvement and adherence: A clinical audit. Diabetol. Metab. Syndr. 2012, 4, 23. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence (NICE). Diabetes (Type 1 and Type 2) in Children and Young People: Diagnosis and Management; National Institute for Health and Care Excellence: London, UK, 2015. [Google Scholar]
- Neuman, V.; Plachy, L.; Pruhova, S.; Kolouskova, S.; Petruzelkova, L.; Obermannova, B.; Vyzralkova, J.; Konecna, P.; Vosahlo, J.; Romanova, M.; et al. Low-carbohydrate diet among children with type 1 diabetes: A multi-center study. Nutrients 2021, 13, 3903. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- Seckold, R.; Fisher, E.; de Bock, M.; King, B.R.; Smart, C.E. The ups and downs of low-carbohydrate diets in the management of Type 1 diabetes: A review of clinical outcomes. Diabet. Med. J. Br. Diabet. Assoc. 2019, 36, 326–334. [Google Scholar] [CrossRef]
- De Bock, M.; Lobley, K.; Anderson, D.; Davis, E.; Donaghue, K.; Pappas, M.; Smart, C. Endocrine and metabolic consequences due to restrictive carbohydrate diets in children with type 1 diabetes: An illustrative case series. Pediatr. Diabetes 2018, 19, 129–137. [Google Scholar] [CrossRef]
- Butwicka, A.; Frisen, L.; Almqvist, C.; Zethelius, B.; Lichtenstein, P. Risks of psychiatric disorders and suicide attempts in children and adolescents with type 1 diabetes: A population-based cohort study. Diabetes Care 2015, 38, 453–459. [Google Scholar] [CrossRef] [Green Version]
- Rydin, A.A.; Spiegel, G.; Frohnert, B.I.; Kaess, A.; Oswald, L.; Owen, D.; Simmons, K.M. Medical management of children with type 1 diabetes on low-carbohydrate or ketogenic diets. Pediatr. Diabetes 2021, 22, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Chun Tie, Y.; Birks, M.; Francis, K. Grounded theory research: A design framework for novice researchers. SAGE Open Med. 2019, 7, 2050312118822927. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)–A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Johnson, D.R.; Scheitle, C.P.; Ecklund, E.H. Beyond the in-person interview? How interview quality varies across in-person, telephone, and Skype interviews. Soc. Sci. Comput. Rev. 2021, 39, 1142–1158. [Google Scholar] [CrossRef]
- NVivo [Internet]. 2020. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 1 July 2021).
- Hart, R.I.; Kimbell, B.; Rankin, D.; Allen, J.M.; Boughton, C.K.; Campbell, F.; de Beaufort, C.; Fröhlich-Reiterer, E.; Ware, J.; Hofer, S.E.; et al. Parents’ experiences of using remote monitoring technology to manage type 1 diabetes in very young children during a clinical trial: Qualitative study. Diabet. Med. 2022, 39, e14828. [Google Scholar] [CrossRef] [PubMed]
- Burckhardt, M.A.; Fried, L.; Bebbington, K.; Hancock, M.; Nicholas, J.A.; Roberts, A.; Abraham, M.B.; Davis, E.A.; Jones, T.W. Use of remote monitoring with continuous glucose monitoring in young children with Type 1 diabetes: The parents’ perspective. Diabet. Med. 2019, 36, 1453–1459. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.S.; Criss, M.M.; Silk, J.S.; Houltberg, B.J. The impact of parenting on emotion regulation during childhood and adolescence. Child. Dev. Perspect. 2017, 11, 233–238. [Google Scholar] [CrossRef]
- Mannucci, E.; Rotella, F.; Ricca, V.; Moretti, S.; Placidi, G.F.; Rotella, C.M. Eating disorders in patients with Type 1 diabetes: A meta-analysis. J. Endocrinol. Investig. 2005, 28, 417–419. [Google Scholar] [CrossRef]
- Gallagher, K.A.S.; DeSalvo, D.; Gregory, J.; Hilliard, M.E. Medical and Psychological Considerations for Carbohydrate-Restricted Diets in Youth With Type 1 Diabetes. Curr. Diab Rep. 2019, 19, 27. [Google Scholar] [CrossRef]
- Merwin, R.M.; Dmitrieva, N.O.; Honeycutt, L.K.; Moskovich, A.A.; Lane, J.D.; Zucker, N.L.; Surwit, R.S.; Feinglos, M.; Kuo, J. Momentary Predictors of Insulin Restriction Among Adults With Type 1 Diabetes and Eating Disorder Symptomatology. Diabetes Care 2015, 38, 2025–2032. [Google Scholar] [CrossRef] [Green Version]
- Cainer, A. Recognising and managing type 1 disordered eating in children and young people with diabetes. Nurs. Child. Young People 2022, 34, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Sherr, J.L.; Schoelwer, M.; Dos Santos, T.J.; Reddy, L.; Biester, T.; Galderisi, A.; van Dyk, J.C.; Hilliard, M.E.; Berget, C.; DiMeglio, L.A. ISPAD Clinical Practice Consensus Guidelines 2022: Diabetes technologies: Insulin delivery. Pediatr. Diabetes 2022, 23, 1406–1431. [Google Scholar] [CrossRef] [PubMed]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample Size in Qualitative Interview Studies:Guided by Information Power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | n (%) | Mean ± St Dev (Range) |
|---|---|---|
| Participants (parents) | 14 (100) | - |
| Mothers | 13 (93) | - |
| Fathers | 1 (7) | - |
| Age of participants (yr) | - | 39.8 ± 6.5 (30.3–49.0) |
| Education level | ||
| College | 3 (21) | - |
| Undergraduate degree | 9 (64) | - |
| Postgraduate degree | 2 (14) | - |
| Employment status | ||
| Full-time | 2 (14) | - |
| Part-time | 4 (28) | - |
| Casual | 3 (21) | - |
| Unemployed | 5 (36) | - |
| Location | ||
| Metropolitan | 12 (86) | - |
| Rural | 2 (14) | - |
| Family history of type 1 diabetes (T1D) | 2 (14) | - |
| Child with T1D | ||
| Female | 4 | |
| Male | 9 | |
| Age (yr) | - | 6.6 ± 2.0 (2–10) |
| Age at diagnosis (yr) | - | 3.9 ± 1.7 (2.0–6.9) |
| Duration of T1D (yr) | - | 2.7 ± 1.9 (0.6–6.5) |
| HbA1c %–participant self-reported | - | 6.06 ± 0.91 (4.4–7.4) |
| HbA1c (mmol/mol) | - | 42.75 ± 9.93 (24.6–57.4) |
| Continuous glucose monitor users | 13 (93) | - |
| Child Insulin Regimen | ||
| Pump | 9 (64) | - |
| Multiple daily injections | 5 (36) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harray, A.J.; Roberts, A.G.; Crosby, N.E.; Shoneye, C.; Bebbington, K. Experiences and Attitudes of Parents Reducing Carbohydrate Intake in the Management of Their Child’s Type 1 Diabetes: A Qualitative Study. Nutrients 2023, 15, 1666. https://doi.org/10.3390/nu15071666
Harray AJ, Roberts AG, Crosby NE, Shoneye C, Bebbington K. Experiences and Attitudes of Parents Reducing Carbohydrate Intake in the Management of Their Child’s Type 1 Diabetes: A Qualitative Study. Nutrients. 2023; 15(7):1666. https://doi.org/10.3390/nu15071666
Chicago/Turabian StyleHarray, Amelia J., Alison G. Roberts, Naomi E. Crosby, Charlene Shoneye, and Keely Bebbington. 2023. "Experiences and Attitudes of Parents Reducing Carbohydrate Intake in the Management of Their Child’s Type 1 Diabetes: A Qualitative Study" Nutrients 15, no. 7: 1666. https://doi.org/10.3390/nu15071666