
How to Monitor Hydration Status and Urine Dilution in Patients with Nephrolithiasis

 , , , and
, , , and
Abstract
:1. Introduction
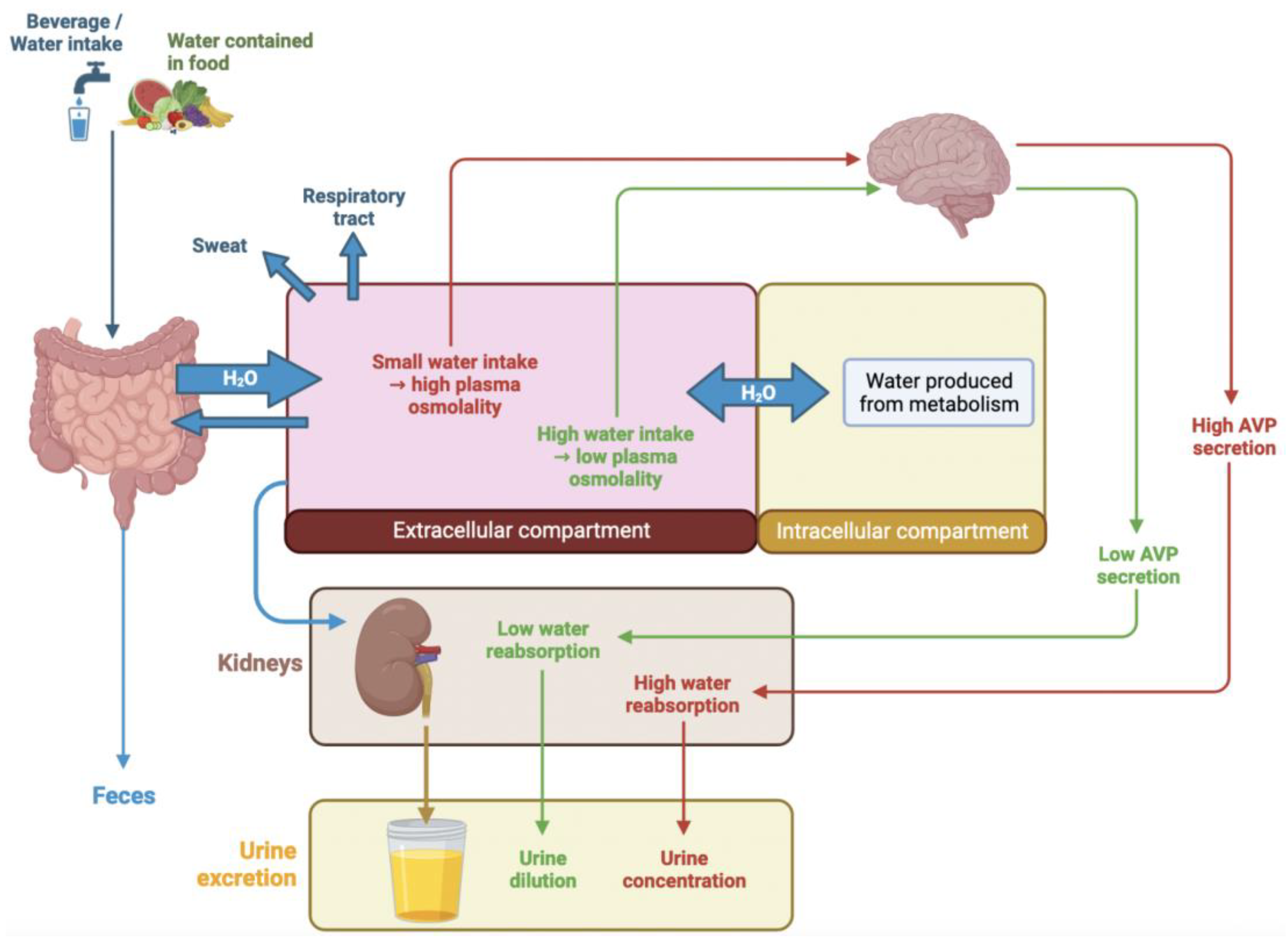
1.1. Regulation of Hydration Balance
1.2. Water Intake and Regulatory Mechanisms
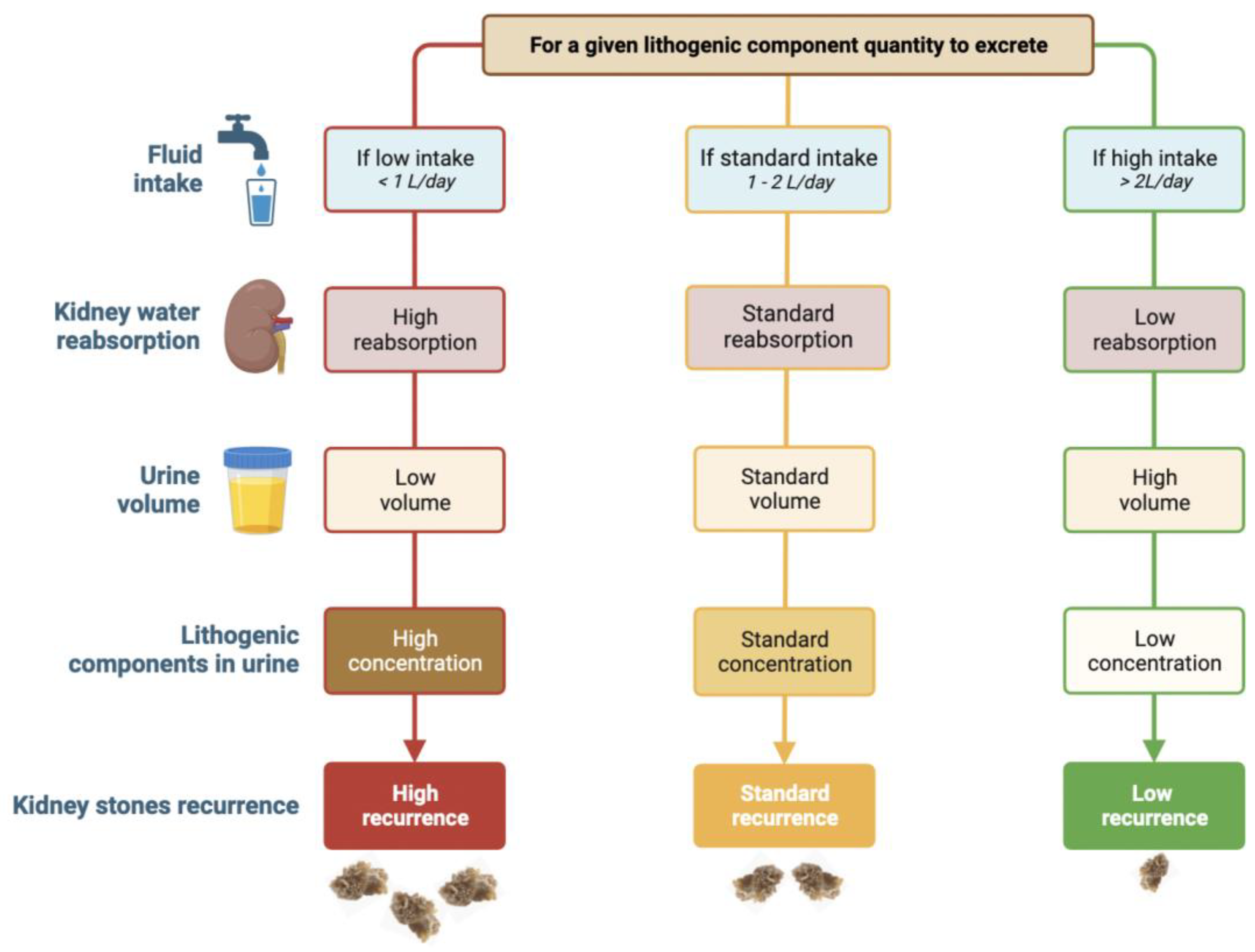
1.3. Nephrolithiasis, Hydration Status and Urine Dilution
2. Which Kind of Urine Should Be Used for Hydration Status and Urine Dilution Monitoring?
2.1. Spot Urine
2.2. 24 h Urine Collection
3. Laboratory Method
3.1. Urine Osmolality
3.2. Urine-Specific Gravity
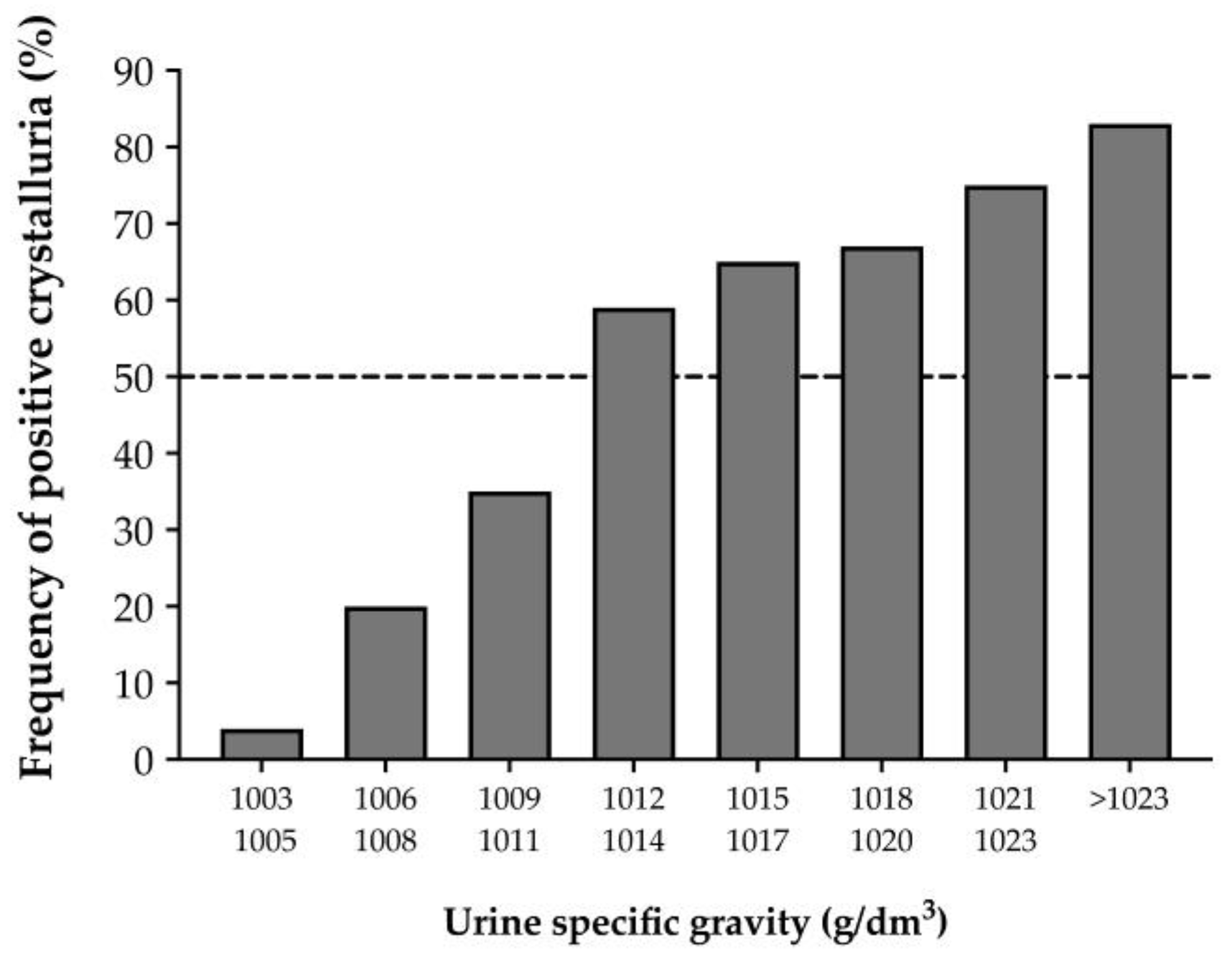
3.3. Crystalluria
4. Home Method
4.1. Urine Colour
4.2. Urinary Strips for Urine-Specific Gravity
4.3. Fluid Intake Monitoring
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perrier, E.; Rondeau, P.; Poupin, M.; Le Bellego, L.; Armstrong, L.E.; Lang, F.; Stookey, J.; Tack, I.; Vergne, S.; Klein, A. Relation between urinary hydration biomarkers and total fluid intake in healthy adults. Eur. J. Clin. Nutr. 2013, 67, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, A.C.; Reimers, K.J.; Buyckx, M.E. Hydration: Issues for the 21st century. Nutr. Rev. 2003, 61, 261–271. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products. Scientific opinion on dietary reference values for water. EFSA J. 2010, 8, 1459–1507. [Google Scholar]
- Meyers, L.D.; Hellwig, J.P.; Otten, J.J. (Eds.) Dietary References Intakes: The Essential Guide to Nutrient Requirements; Institute of Medecine of National Academies: Washington, DC, USA, 2006. [Google Scholar]
- Kettaneh, A.; Fardet, L.; Mario, N.; Retbi, A.; Taright, N.; Tiev, K.; Reinhard, I.; Guidet, B.; Cabane, J. The 2003 heat wave in France: Hydratation status changes in older inpatients. Eur. J. Epidemiol. 2010, 25, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Liu, H.Z.; Ou, C.Q.; Lin, G.Z.; Ding, Y.; Zhou, Q.; Shen, J.C.; Chen, P.Y. Impact of heat wave in 2005 on mortality in Guangzhou, China. Biomed. Environ. Sci. 2013, 26, 647–654. [Google Scholar] [CrossRef]
- Fitzgerald, B.; Middleton, J.K.; Cooper, S.-A. Adverse effects of summer amongst people with learning disabilities: Neuroleptic malignant syndrome. J. Intellect. Disabil. Res. 1997, 41 Pt 3, 273–277. [Google Scholar] [CrossRef]
- Desmazes-Dufeu, N.; Hubert, D.; Burgel, P.R.; Kanaan, R.; Velea, V.; Dusser, D. Severe dehydration and August 2003 heat wave in a cohort of adults with cystic fibrosis. Presse Med. 2005, 34, 647–648. [Google Scholar]
- Biggs, C.; Paterson, M.; Maunder, E. Hydration Status of South African Forestry Workers Harvesting Trees in Autumn and Winter. Ann. Occup. Hyg. 2011, 55, 6–15. [Google Scholar] [CrossRef]
- Bates, G.P.; Miller, V.S.; Joubert, D.M. Hydration Status of Expatriate Manual Workers During Summer in the Middle East. Ann. Occup. Hyg. 2010, 54, 137–143. [Google Scholar] [CrossRef]
- Lang, F.; Busch, G.L.; Ritter, M.; Völkl, H.; Waldegger, S.; Gulbins, E.; Häussinger, D. Functional Significance of Cell Volume Regulatory Mechanisms. Physiol. Rev. 1998, 78, 247–306. [Google Scholar] [CrossRef]
- Koeppen, B.; Stanton, B. Renal Physiology; Mosby-Year Book, Inc.: St. Louis, MI, USA, 2000. [Google Scholar]
- Cheuvront, S.N.; Kenefick, R.W.; Charkoudian, N.; Sawka, M.N. Physiologic basis for understanding quantitative dehydration assessment. Am. J. Clin. Nutr. 2013, 97, 455–462. [Google Scholar] [CrossRef]
- Bourque, C.W. Central mechanisms of osmosensation and systemic osmoregulation. Nat. Rev. Neurosci. 2008, 9, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Yasui, M.; Marples, D.; Belusa, R.; Eklöf, A.C.; Celsi, G.; Nielsen, S.; Aperia, A. Development of urinary concentrating capacity: Role of aquaporin-2. Am. J. Physiol. Ren. Physiol. 1996, 271, F461–F468. [Google Scholar] [CrossRef]
- Shoker, A.S. Application of the clearance concept to hyponatremic and hypernatremic disorders: A phenomenological analysis. Clin. Chem. 1994, 40, 1220–1227. [Google Scholar] [CrossRef] [PubMed]
- Rolls, B.J.; Phillips, P.A. Aging and Disturbances of Thirst and Fluid Balance. Nutr. Rev. 1990, 48, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Kenney, W.L.; Chiu, P. Influence of age on thirst and fluid intake. Med. Sci. Sport. Exerc. 2001, 33, 1524–1532. [Google Scholar] [CrossRef]
- Jéquier, E.; Constant, F. Water as an essential nutrient: The physiological basis of hydration. Eur. J. Clin. Nutr. 2010, 64, 115–123. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Climatic heat stress and the exercising child and adolescent. American Academy of Pediatrics. Committee on Sports Medicine and Fitness. Pediatrics 2000, 106 Pt 1, 158–159. [Google Scholar] [CrossRef]
- Stookey, J.D. High Prevalence of Plasma Hypertonicity among Community-Dwelling Older Adults: Results from NHANES III. J. Am. Diet. Assoc. 2005, 105, 1231–1239. [Google Scholar] [CrossRef]
- Manz, F.; Johner, S.A.; Wentz, A.; Boeing, H.; Remer, T. Water balance throughout the adult life span in a German population. Br. J. Nutr. 2012, 107, 1673–1681. [Google Scholar] [CrossRef]
- Armstrong, L.E. Challenges of linking chronic dehydration and fluid consumption to health outcomes. Nutr. Rev. 2012, 70 (Suppl. 2), S121–S127. [Google Scholar] [CrossRef] [PubMed]
- Borghi, L.; Meschi, T.; Amato, F.; Briganti, A.; Novarini, A.; Giannini, A. Urinary Volume, Water and Recurrences in Idiopathic Calcium Nephrolithiasis: A 5-year Randomized Prospective Study. J. Urol. 1996, 155, 839–843. [Google Scholar] [CrossRef]
- Stheneur, C.; Bergeron, S.; Lapeyraque, A.-L. Renal complications in anorexia nervosa. Eat. Weight. Disord. 2014, 19, 455–460. [Google Scholar] [CrossRef]
- Silber, T.J.; Kass, E.J. Anorexia nervosa and nephrolithiasis. J. Adolesc. Health Care 1984, 5, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Malik, T.F.; Aurelio, D.M. Extraintestinal Manifestations of Inflammatory Bowel Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Manganiotis, A.N.; Banner, M.P.; Malkowicz, S.B. Urologic Complications of Crohn’s Disease. Surg. Clin. North Am. 2001, 81, 197–215. [Google Scholar] [CrossRef]
- Theisen, K.M.; Ayyash, O.; Pere, M.; Ferroni, M.; Riley, J.; Averch, T.D.; Semins, M.J. Defining 24-hour urine parameters and kidney stone risk of student athletes. Clin. Nephrol. 2022, 97, 86–92. [Google Scholar] [CrossRef]
- Bar-David, Y.; Urkin, J.; Kozminsky, E. The effect of voluntary dehydration on cognitive functions of elementary school children. Acta Paediatr. 2005, 94, 1667–1673. [Google Scholar] [CrossRef] [PubMed]
- Borghi, L.; Meschi, T.; Schianchi, T.; Briganti, A.; Guerra, A.; Allegri, F.; Novarini, A. Urine Volume: Stone Risk Factor and Preventive Measure. Nephron 1999, 81 (Suppl. 1), 31–37. [Google Scholar] [CrossRef]
- Wang, J.-S.; Chiang, H.-Y.; Chen, H.-L.; Flores, M.; Navas-Acien, A.; Kuo, C.-C. Association of water intake and hydration status with risk of kidney stone formation based on NHANES 2009–2012 cycles. Public Health Nutr. 2022, 25, 2403–2414. [Google Scholar] [CrossRef]
- Miller, L.A.; Stapleton, F.B. Urinary Volume in Children with Urolithiasis. J. Urol. 1989, 141, 918–920. [Google Scholar] [CrossRef]
- Penido, M.G.M.; Srivastava, T.; Alon, U.S. Pediatric Primary Urolithiasis: 12-Year Experience at a Midwestern Children’s Hospital. J. Urol. 2013, 189, 1493–1497. [Google Scholar] [CrossRef]
- Guerra, A.; Allegri, F.; Meschi, T.; Adorni, G.; Prati, B.; Nouvenne, A.; Novarini, A.; Maggiore, U.; Fiaccadori, E.; Borghi, L. Effects of urine dilution on quantity, size and aggregation of calcium oxalate crystals induced in vitro by an oxalate load. Clin. Chem. Lab. Med. 2005, 43, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Straub, M.; Hautmann, R.E. Developments in stone prevention. Curr. Opin. Urol. 2005, 15, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Daudon, M.; Hennequin, C.; Boujelben, G.; Lacour, B.; Jungers, P. Serial crystalluria determination and the risk of recurrence in calcium stone formers. Kidney Int. 2005, 67, 1934–1943. [Google Scholar] [CrossRef]
- Qaseem, A.; Dallas, P.; Forciea, M.A.; Starkey, M.; Denberg, T.D.; Clinical Guidelines Committee of the American College of Physicians. Dietary and Pharmacologic Management to Prevent Recurrent Nephrolithiasis in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann. Intern. Med. 2014, 161, 659–667. [Google Scholar] [CrossRef]
- Meschi, T.; Nouvenne, A.; Borghi, L. Lifestyle Recommendations to Reduce the Risk of Kidney Stones. Urol. Clin. N. Am. 2011, 38, 313–320. [Google Scholar] [CrossRef]
- Pearle, M.S.; Goldfarb, D.; Assimos, D.G.; Curhan, G.; Denu-Ciocca, C.J.; Matlaga, B.R.; Monga, M.; Penniston, K.L.; Preminger, G.M.; Turk, T.M.; et al. Medical Management of Kidney Stones: AUA Guideline. J. Urol. 2014, 192, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Skolarikos, A.; Neisius, A.; Petrík, A.; Somani, B.; Thomas, K.; Gambaro, G. EAU Guidelines on Urolithiasis. Available online: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Urolithiasis-2023.pdf (accessed on 5 January 2023).
- Servais, A.; Thomas, K.; Strologo, L.D.; Sayer, J.A.; Bekri, S.; Bertholet-Thomas, A.; Bultitude, M.; Capolongo, G.; Cerkauskiene, R.; Daudon, M.; et al. Cystinuria: Clinical practice recommendation. Kidney Int. 2021, 99, 48–58. [Google Scholar] [CrossRef]
- Groothoff, J.W.; Metry, E.; Deesker, L.; Garrelfs, S.; Acquaviva, C.; Almardini, R.; Beck, B.B.; Boyer, O.; Cerkauskiene, R.; Ferraro, P.M.; et al. Clinical practice recommendations for primary hyperoxaluria: An expert consensus statement from ERKNet and OxalEurope. Nat. Rev. Nephrol. 2023, 19, 194–211. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Pumerantz, A.C.; Fiala, K.A.; Roti, M.W.; Kavouras, S.A.; Casa, D.J.; Maresh, C.M. Human hydration indices: Acute and longitudinal reference values. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 145–153. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Arrabal-Polo, M.; Capasso, G.; Croppi, E.; Cupisti, A.; Ernandez, T.; Fuster, D.G.; Galan, J.A.; Grases, F.; Hoorn, E.J.; et al. A preliminary survey of practice patterns across several European kidney stone centers and a call for action in developing shared practice. Urolithiasis 2019, 47, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Shirreffs, S.M.; Maughan, R.J. Urine osmolality and conductivity as indices of hydration status in athletes in the heat. Med. Sci. Sports Exerc. 1998, 30, 1598–1602. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, E.M.; Senden, J.M.; Brouns, F. Urine color, osmolality and specific electrical conductance are not accurate measures of hydration status during postexercise rehydration. J. Sports Med. Phys. Fit. 1999, 39, 47–53. [Google Scholar]
- Armstrong, L.E.; Johnson, E.C.; McKenzie, A.L.; Muñoz, C.X. Interpreting common hydration biomarkers on the basis of solute and water excretion. Eur. J. Clin. Nutr. 2013, 67, 249–253. [Google Scholar] [CrossRef]
- Milose, J.C.; Kaufman, S.R.; Hollenbeck, B.K.; Wolf, J.S., Jr.; Hollingsworth, J.M. Prevalence of 24-Hour Urine Collection in High Risk Stone Formers. J. Urol. 2014, 191, 376–380. [Google Scholar] [CrossRef]
- Ellison, J.S.; Kaufman, S.R.; Kraft, K.H.; Wolf, J.S., Jr.; Hollenbeck, B.K.; Hollingsworth, J.M. Underuse of 24-Hour Urine Collection Among Children With Incident Urinary Stones: A Quality-of-care Concern? Urology 2014, 84, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.S.; McGarry, L.; Bowen, D.K.; Tasian, G.E. Patient Characteristics Associated with Completion of 24-hour Urine Analyses Among Children and Adolescents With Nephrolithiasis. Urology 2019, 127, 102–106. [Google Scholar] [CrossRef]
- Sawyer, M.D.; Dietrich, M.S.; Pickens, R.B.; Herrell, S.D.; Miller, N.L. Adequate or Not? A Comparison of 24-Hour Urine Studies for Renal Stone Prevention by Creatinine to Weight Ratio. J. Endourol. 2013, 27, 366–369. [Google Scholar] [CrossRef]
- Hsi, R.S.; Sanford, T.; Goldfarb, D.S.; Stoller, M.L. The Role of the 24-Hour Urine Collection in the Prevention of Kidney Stone Recurrence. J. Urol. 2017, 197, 1084–1089. [Google Scholar] [CrossRef]
- Lotan, Y.; Antonelli, J.; Jiménez, I.B.; Gharbi, H.; Herring, R.; Beaver, A.; Dennis, A.; Von Merveldt, D.; Carter, S.; Cohen, A.; et al. The kidney stone and increased water intake trial in steel workers: Results from a pilot study. Urolithiasis 2017, 45, 177–183. [Google Scholar] [CrossRef]
- Scales, C.D., Jr.; Desai, A.C.; Harper, J.D.; Lai, H.H.; Maalouf, N.M.; Reese, P.P.; Tasian, G.E.; Al-Khalidi, H.R.; Kirkali, Z.; Wessells, H.; et al. Prevention of Urinary Stones With Hydration (PUSH): Design and Rationale of a Clinical Trial. Am. J. Kidney Dis. 2021, 77, 898–906. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Ely, B.R.; Kenefick, R.W.; Sawka, M.N. Biological variation and diagnostic accuracy of dehydration assessment markers. Am. J. Clin. Nutr. 2010, 92, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Đuras, A.; Kocijan, V.C.; Rade, A.; Lipovec, R.; Ostroški, I.; Biljak, V.R.; Šimundić, A.-M. Serum and urine osmolality: 8 hours, 24 hours and 1-month sample stability. Scand. J. Clin. Lab. Investig. 2022, 82, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Yeh, H.-C.; Lin, Y.-S.; Kuo, C.-C.; Weidemann, D.; Weaver, V.; Fadrowski, J.; Neu, A.; Navas-Acien, A. Urine osmolality in the US population: Implications for environmental biomonitoring. Environ. Res. 2015, 136, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Adams, W.M.; Wininger, M.; Zaplatosch, M.E.; Hevel, D.J.; Maher, J.P.; McGuirt, J.T. Influence of Nutrient Intake on 24 Hour Urinary Hydration Biomarkers Using a Clustering-Based Approach. Nutrients 2020, 12, 2933. [Google Scholar] [CrossRef] [PubMed]
- Manz, F.; Wentz, A. 24-h hydration status: Parameters, epidemiology and recommendations. Eur. J. Clin. Nutr. 2003, 57 (Suppl. 2), S10–S18. [Google Scholar] [CrossRef]
- Kavouras, S.A.; Suh, H.-G.; Vallet, M.; Daudon, M.; Mauromoustakos, A.; Vecchio, M.; Tack, I. Urine osmolality predicts calcium-oxalate crystallization risk in patients with recurrent urolithiasis. Urolithiasis 2021, 49, 399–405. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Johnson, E.C.; McKenzie, A.L.; Muñoz, C.X. An empirical method to determine inadequacy of dietary water. Nutrition 2016, 32, 79–82. [Google Scholar] [CrossRef]
- Perrier, E.T.; Buendia-Jimenez, I.; Vecchio, M.; Armstrong, L.E.; Tack, I.; Klein, A. Twenty-Four-Hour Urine Osmolality as a Physiological Index of Adequate Water Intake. Dis. Markers 2015, 2015, 231063. [Google Scholar] [CrossRef]
- Kang, H.W.; Seo, S.P.; Ha, Y.-S.; Kim, W.T.; Kim, Y.-J.; Yun, S.-J.; Kim, W.-J.; Lee, S.-C. Twenty-four-hour urine osmolality as a representative index of adequate hydration and a predictor of recurrence in patients with urolithiasis. Int. Urol. Nephrol. 2019, 51, 1129–1135. [Google Scholar] [CrossRef]
- Topcu, D.I.; Bayraktar, N. Searching for the urine osmolality surrogate: An automated machine learning approach. Clin. Chem. Lab. Med. 2022, 60, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Yoo, D.; Lee, S.M.; Moon, S.Y.; Kim, I.; Chang, C.L. Evaluation of conductivity-based osmolality measurement in urine using the Sysmex UF5000. J. Clin. Lab. Anal. 2021, 35, e23586. [Google Scholar] [CrossRef] [PubMed]
- Siener, R. Nutrition and Kidney Stone Disease. Nutrients 2021, 13, 1917. [Google Scholar] [CrossRef] [PubMed]
- Chadha, V.; Garg, U.; Alon, U.S. Measurement of urinary concentration: A critical appraisal of methodologies. Pediatr. Nephrol. 2001, 16, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.E.; Maresh, C.M.; Castellani, J.; Bergeron, M.F.; Kenefick, R.W.; Lagasse, K.E.; Riebe, D. Urinary Indices of Hydration Status. Int. J. Sport Nutr. 1994, 4, 265–279. [Google Scholar] [CrossRef]
- Oppliger, R.A.; Magnes, S.A.; Popowski, L.A.; Gisolfi, C.V. Accuracy of Urine Specific Gravity and Osmolality as Indicators of Hydration Status. Int. J. Sport Nutr. Exerc. Metab. 2005, 15, 236–251. [Google Scholar] [CrossRef]
- Perrier, E.; Demazières, A.; Girard, N.; Pross, N.; Osbild, D.; Metzger, D.; Guelinckx, I.; Klein, A. Circadian variation and responsiveness of hydration biomarkers to changes in daily water intake. Eur. J. Appl. Physiol. 2013, 113, 2143–2151. [Google Scholar] [CrossRef] [PubMed]
- Werness, P.G.; Bergert, J.H.; Lee, K.E. Urinary Crystal Growth: Effect of Inhibitor Mixtures. Clin. Sci. 1981, 61, 487–491. [Google Scholar] [CrossRef]
- Caudarella, R.; Rizzoli, E.; Malavolta, N.; Severi, B.; Vasi, V.; Biagini, G. Urinary crystalluria. A debatable problem. Acta Urol. Belg. 1986, 54, 49–56. [Google Scholar]
- Kavouras, S.A. Assessing hydration status. Curr. Opin. Clin. Nutr. Metab. Care 2002, 5, 519–524. [Google Scholar] [CrossRef]
- Simerville, J.A.; Maxted, W.C.; Pahira, J.J. Urinalysis: A comprehensive review. Am. Fam. Physician 2005, 71, 1153–1162. [Google Scholar]
- Perrier, E.T.; Bottin, J.H.; Vecchio, M.; Lemetais, G. Criterion values for urine-specific gravity and urine color representing adequate water intake in healthy adults. Eur. J. Clin. Nutr. 2017, 71, 561–563. [Google Scholar] [CrossRef] [PubMed]
- Khorami, M.H.; Shahdoost, A.A.; Sichani, M.M.; Tadayon, F.; Arezegar, S.H.; Bagherian-Sararoudi, R.; Hashemi, R. The assessment of 24 24-h urine volume by measurement of urine specific gravity with dipstick in adults with nephrolithiasis. Adv. Biomed. Res. 2012, 1, 86. [Google Scholar] [CrossRef] [PubMed]
- Dörner, K.; Campos, R.; Börnsen, S. Further Evaluation of the SG Test Strip for Estimation of Urinary Osmolality. J. Clin. Chem. Clin. Biochem. 1984, 22, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Hennequin, C.; Daudon, M.; Phung, T.; Lacour, B.; Jungers, P. Evaluation of the lithogenic risk in renal lithiasis. Value of urine density measurement. Presse Med. 1995, 24, 1559–1562. [Google Scholar]
- Imran, S.; Eva, G.; Christopher, S.; Flynn, E.; Henner, D. Is specific gravity a good estimate of urine osmolality? J. Clin. Lab. Anal. 2010, 24, 426–430. [Google Scholar] [CrossRef]
- Siegrist, D.; Hess, B.; Montandon, M.; Takkinen, R.; Lippuner, K.; Jaeger, P. Urinary specific gravity—Comparative measurements using reagent strips and refractometer in 340 morning urine samples. Schweiz. Rundsch. Fur Med. Prax. 1993, 82, 112–116. [Google Scholar]
- Rowat, A.; Smith, L.; Graham, C.; Lyle, D.; Horsburgh, D.; Dennis, M. A pilot study to assess if urine specific gravity and urine colour charts are useful indicators of dehydration in acute stroke patients. J. Adv. Nurs. 2011, 67, 1976–1983. [Google Scholar] [CrossRef]
- Souza, A.C.P.; Zatz, R.; De Oliveira, R.B.; Santinho, M.A.R.; Ribalta, M.; Romão, J.E., Jr.; Elias, R.M. Is urinary density an adequate predictor of urinary osmolality? BMC Nephrol. 2015, 16, 46. [Google Scholar] [CrossRef] [PubMed]
- Tarplin, S.; Monga, M.; Stern, K.L.; McCauley, L.R.; Sarkissian, C.; Nguyen, M.M. Predictors of Reporting Success With Increased Fluid Intake Among Kidney Stone Patients. Urology 2016, 88, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Streeper, N.M.; Dubnansky, A.; Sanders, A.B.; Lehman, K.; Thomaz, E.; Conroy, D.E. Improving Fluid Intake Behavior Among Patients With Kidney Stones: Understanding Patients’ Experiences and Acceptability of Digital Health Technology. Urology 2019, 133, 57–66. [Google Scholar] [CrossRef]
- Goble, N.M. Hydration monitoring in the long-term prophylaxis of nephrocalcinosis. West Engl. Med. J. 1991, 106, 15. [Google Scholar] [PubMed]
- Borofsky, M.S.; Dauw, C.A.; York, N.; Terry, C.; Lingeman, J.E. Accuracy of daily fluid intake measurements using a “smart” water bottle. Urolithiasis 2018, 46, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Fernie, G.; Fekr, A.R. Monitoring fluid intake by commercially available smart water bottles. Sci. Rep. 2022, 12, 4402. [Google Scholar] [CrossRef] [PubMed]
- Stout, T.E.; Lingeman, J.E.; Krambeck, A.E.; Humphreys, M.R.; Zisman, A.; Elfering, S.; Large, T.; Dahm, P.; Borofsky, M. A Randomized Trial Evaluating the Use of a Smart Water Bottle to Increase Fluid Intake in Stone Formers. J. Ren. Nutr. 2022, 32, 389–395. [Google Scholar] [CrossRef]
- Rodin, D.; Shapiro, Y.; Pinhasov, A.; Kreinin, A.; Kirby, M. An accurate wearable hydration sensor: Real-world evaluation of practical use. PLoS ONE 2022, 17, e0272646. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Principle | Advantages | Disadvantages | |
|---|---|---|---|
| Urine osmolality | Freezing point depression (or more rarely vapor pressure depression) |
|
|
| Urine-specific gravity | Refractometry |
|
|
| Urine strip with automatic strip reader |
|
| |
| Urine strip |
|
| |
| Crystalluria | Miscroscopic detection of crystals in urine |
|
|
| Urine color | Visual examination |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Travers, S.; Prot-Bertoye, C.; Daudon, M.; Courbebaisse, M.; Baron, S. How to Monitor Hydration Status and Urine Dilution in Patients with Nephrolithiasis. Nutrients 2023, 15, 1642. https://doi.org/10.3390/nu15071642
Travers S, Prot-Bertoye C, Daudon M, Courbebaisse M, Baron S. How to Monitor Hydration Status and Urine Dilution in Patients with Nephrolithiasis. Nutrients. 2023; 15(7):1642. https://doi.org/10.3390/nu15071642
Chicago/Turabian StyleTravers, Simon, Caroline Prot-Bertoye, Michel Daudon, Marie Courbebaisse, and Stéphanie Baron. 2023. "How to Monitor Hydration Status and Urine Dilution in Patients with Nephrolithiasis" Nutrients 15, no. 7: 1642. https://doi.org/10.3390/nu15071642