
Androgen Deprivation Therapy for Prostate Cancer Influences Body Composition Increasing Risk of Sarcopenia

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
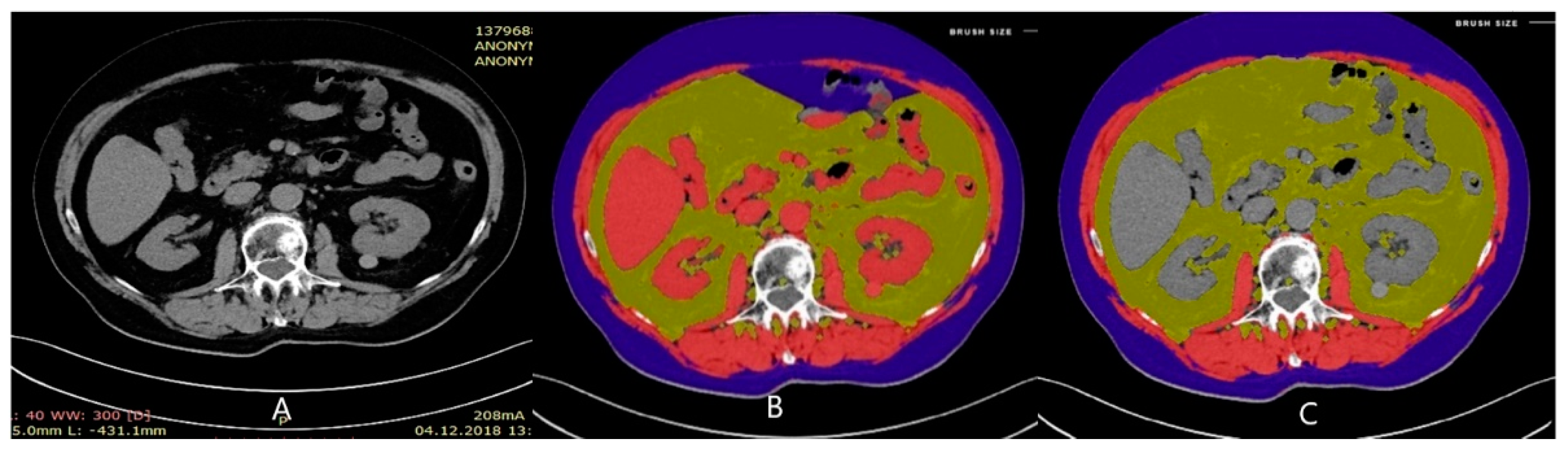
2.2. Methods
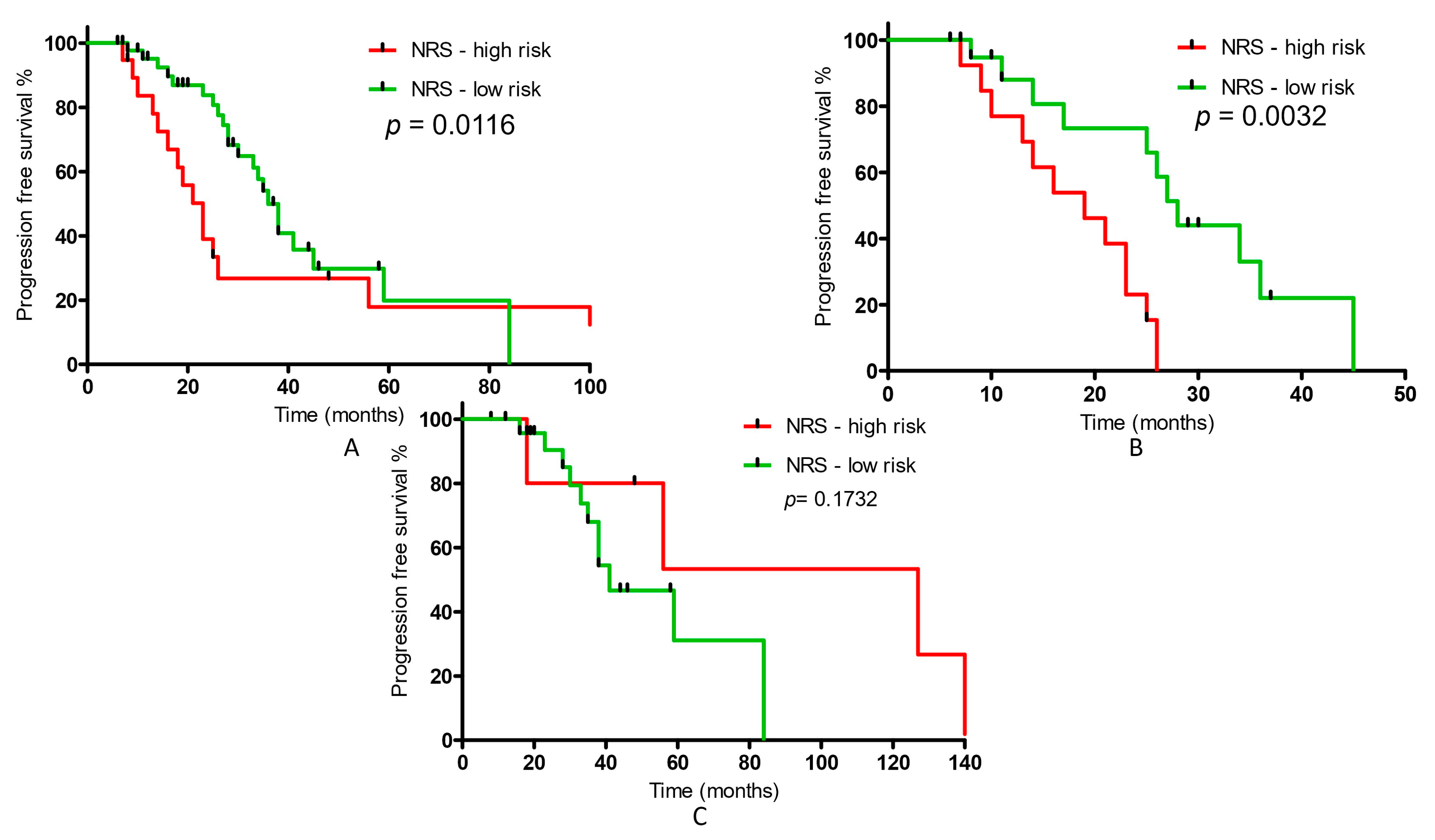
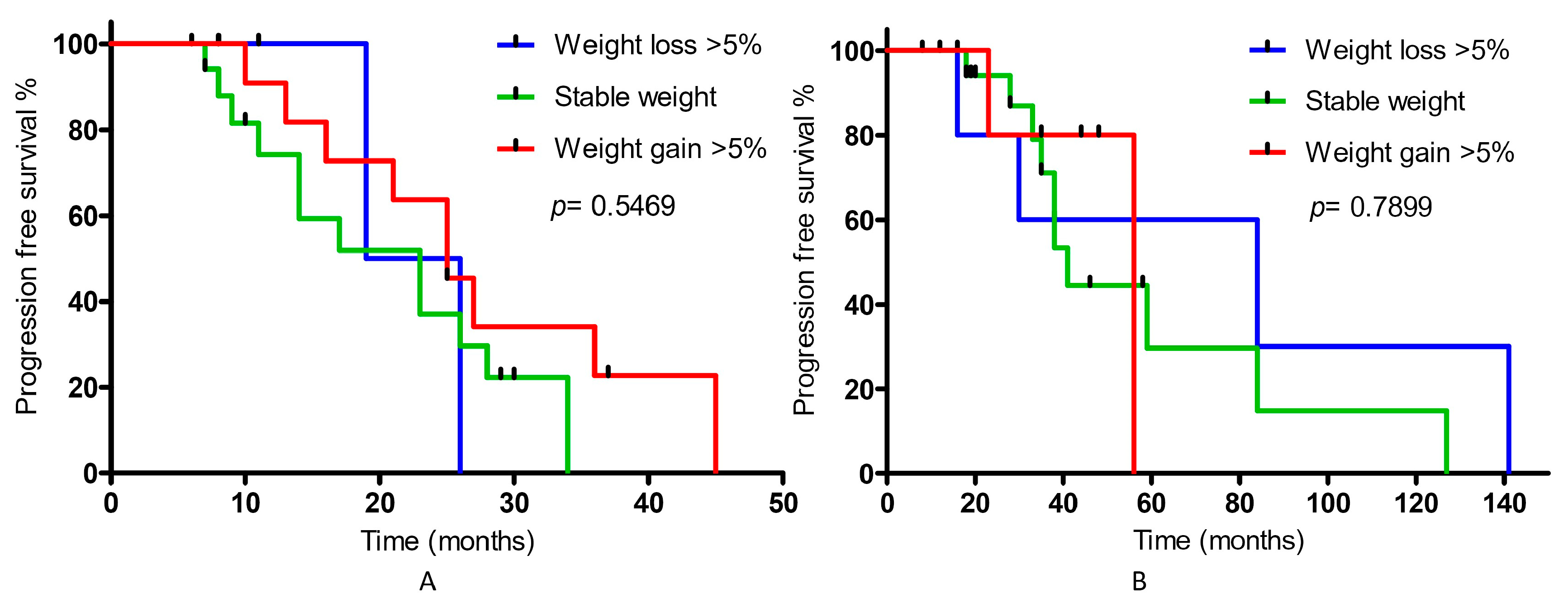
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mattiuzzi, C.; Lippi, G. Current Cancer Epidemiology. J. Epidemiol. Glob. Health 2019, 9, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; LaBonte, M.J.; Craig, S.G.; Finn, S.P.; Allott, E.H. Inflammation and Prostate Cancer: A Multidisciplinary Approach to Identifying Opportunities for Treatment and Prevention. Cancers 2022, 14, 1367. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrit-on—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Torralvo, F.J.; Ruiz-García, I.; Contreras-Bolívar, V.; González-Almendros, I.; Ruiz-Vico, M.; Abuín-Fernández, J.; Barrios, M.; Alba, E.; Olveira, G. CT-Determined Sarcopenia in GLIM-Defined Malnutrition and Prediction of 6-Month Mortality in Cancer Inpatients. Nutrients 2021, 13, 2647. [Google Scholar] [CrossRef]
- Daily, J.W.; Park, S. Sarcopenia Is a Cause and Consequence of Metabolic Dysregulation in Aging Humans: Effects of Gut Dysbiosis, Glucose Dysregulation, Diet and Lifestyle. Cells 2022, 11, 338. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Phu, S.; Vogrin, S.; Zanker, J.; Bani Hassan, E.; Al Saedi, A.; Duque, G. Agreement Between Initial and Revised European Working Group on Sarcopenia in Older People Definitions. J. Am. Med. Dir. Assoc. 2019, 20, 382–383.e1. [Google Scholar] [CrossRef]
- Dunne, R.F.; Loh, K.P.; Williams, G.R.; Jatoi, A.; Mustian, K.M.; Mohile, S.G. Cachexia and Sarcopenia in Older Adults with Cancer: A Comprehensive Review. Cancers 2019, 11, 1861. [Google Scholar] [CrossRef] [Green Version]
- Krzakowski, M.; Warzocha, K.; Stelmach, A.; Potemski, P. Zalecenia Postępowania Diagnostyczno-Terapeutycznego w Nowotworach Złośliwych; Via Medica: Gdańsk, Poland, 2013; Volume 3, pp. 25–35. [Google Scholar]
- Available online: https://uroweb.org/guidelines/prostate-cancer (accessed on 20 March 2022).
- Horwich, A.; Hugosson, J.; de Reijke, T.; Wiegel, T.; Fizazi, K.; Kataja, V.; Panel Members; European Society for Medical Oncology. Prostate cancer: ESMO Consensus Conference Guidelines 2012. Ann. Oncol. 2013, 24, 1141–1162. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, F.; Mori, V. Nutritional support and tumour growth in humans: A narrative review of the literature. Clin. Nutr. 2009, 28, 226–230. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [Green Version]
- Vasques, J.; Guerreiro, C.S.; Sousa, J.; Pinto, M.; Cortez-Pinto, H. Nutritional support in cirrhotic patients with sarcopenia. Clin. Nutr. ESPEN 2019, 33, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Pironi, L.; Boeykens, K.; Bozzetti, F.; Joly, F.; Klek, S.; Lal, S.; Lichota, M.; Mühlebach, S.; Van Gossum, A.; Wanten, G.; et al. ESPEN guideline on home parenteral nutrition. Clin. Nutr. 2020, 39, 1645–1666. [Google Scholar] [CrossRef]
- Van den Broeck, T.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; Cumberbatch, M.; Tilki, D.; De Santis, M.; Fanti, S.; Fossati, N.; Gillessen, S.; et al. Biochemical Recurrence in Prostate Cancer: The European Association of Urology Prostate Cancer Guidelines Panel Recommendations. Eur. Urol. Focus 2020, 6, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Pisansky, T.M.; Thompson, I.M.; Valicenti, R.K.; D’Amico, A.V.; Selvarajah, S. Adjuvant and Salvage Radiation Therapy After Prostatectomy: ASTRO/AUA Guideline Amendment, Executive Summary 2018. Pract. Radiat. Oncol. 2019, 9, 208–213. [Google Scholar] [CrossRef] [Green Version]
- EAU Guidelines. Available online: https://uroweb.org/guideline/prostate-cancer/ (accessed on 20 March 2022).
- Aras, M.; Erdil, T.Y.; Dane, F.; Gungor, S.; Ones, T.; Dede, F. Comparison of WHO, RECIST 1.1, EORTC, and PERCIST criteria in the evaluation of treatment response in malignant solid tumors. Nucl. Med. Commun. 2016, 37, 9–15. [Google Scholar] [CrossRef]
- Available online: https://coreslicer.com/ (accessed on 20 January 2022).
- Martin, L.; Birdsell, L.; Macdonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef]
- Anjanappa, M.; Corden, M.; Green, A.; Roberts, D.; Hoskin, P.; McWilliam, A.; Choudhury, A. Sarcopenia in cancer: Risking more than muscle loss. Tech. Innov. Patient Support Radiat. Oncol. 2020, 16, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Baracos, V.E.; Arribas, L. Sarcopenic obesity: Hidden muscle wasting and its impact for survival and complications of cancer therapy. Ann. Oncol. 2018, 29 (Suppl. 2), ii1–ii9. [Google Scholar] [CrossRef]
- Illa, P.; Tomiskova, M.; Skrickova, J. Nutritional Risk Screening Predicts Tumor Response in Lung Cancer Patients. J. Am. Coll. Nutr. 2015, 34, 425–429. [Google Scholar] [CrossRef]
- Li, Y.F.; Nie, R.C.; Wu, T.; Li, S.M.; Chen, S.; Wang, W.; Chen, X.J.; Chen, G.M.; Chen, Y.B.; Zhou, Z.W.; et al. Prognostic Value of the Nutritional Risk Screening 2002 Scale in Metastatic Gastric Cancer: A Large-Scale Cohort Study. J. Cancer 2019, 10, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Owen, P.J.; Daly, R.M.; Dalla Via, J.; Mundell, N.L.; Livingston, P.M.; Rantalainen, T.; Fraser, S.F. The clinical relevance of adiposity when assessing muscle health in men treated with androgen deprivation for prostate cancer. J. Cachexia Sarcopenia Muscle 2019, 10, 1036–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen, P.J.; Daly, R.M.; Livingston, P.M.; Fraser, S.F. Lifestyle guidelines for managing adverse effects on bone health and body composition in men treated with androgen deprivation therapy for prostate cancer: An update. Prostate Cancer Prostatic Dis. 2017, 20, 137–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebadi, M.; Martin, L.; Ghosh, S.; Field, C.J.; Lehner, R.; Baracos, V.E.; Mazurak, V.C. Subcutaneous adiposity is an independent predictor of mortality in cancer patients. Br. J. Cancer 2017, 117, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Stangl-Kremser, J.; Suarez-Ibarrola, R.; Andrea, D.; Korn, S.M.; Pones, M.; Kramer, G.; Marhold, M.; Krainer, M.; Enikeev, D.V.; Glybochko, P.V.; et al. Assessment of body composition in the advanced stage of castration-resistant prostate cancer: Special focus on sarcopenia. Prostate Cancer Prostatic Dis. 2020, 23, 309–315. [Google Scholar] [CrossRef]
- Hamilton, E.J.; Gianatti, E.; Strauss, B.J.; Wentworth, J.; Lim-Joon, D.; Bolton, D.; Zajac, J.D.; Grossmann, M. Increase in visceral and subcutaneous abdominal fat in men with prostate cancer treated with androgen deprivation therapy. Clin. Endocrinol. 2011, 74, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Storer, T.W.; Miciek, R.; Travison, T.G. Muscle function, physical performance and body composition changes in men with prostate cancer undergoing androgen deprivation therapy. Asian J. Androl. 2012, 14, 204–221. [Google Scholar] [CrossRef] [Green Version]
- Rinninella, E.; Cintoni, M.; Raoul, P.; Pozzo, C.; Strippoli, A.; Bria, E.; Tortora, G.; Gasbarrini, A.; Mele, M.C. Muscle mass, assessed at diagnosis by L3-CT scan as a prognostic marker of clinical outcomes in patients with gastric cancer: A systematic review and meta-analysis. Clin. Nutr. 2020, 39, 2045–2054. [Google Scholar] [CrossRef]
- Ohtaka, A.; Aoki, H.; Nagata, M.; Kanayama, M.; Shimizu, F.; Ide, H.; Tsujimura, A.; Horie, S. Sarcopenia is a poor prognostic factor of castration-resistant prostate cancer treated with docetaxel therapy. Prostate Int. 2019, 7, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Casirati, A.; Vandoni, G.; Della Valle, S.; Greco, G.; Platania, M.; Colatruglio, S.; Lalli, L.; Gavazzi, C. Nutritional status and body composition assessment in patients with a new diagnosis of advanced solid tumour: Exploratory comparison of computed tomography and bioelectrical impedance analysis. Clin. Nutr. 2021, 40, 1268–1273. [Google Scholar] [CrossRef]
- de Rooy, C.; Grossmann, M.; Zajac, J.D.; Cheung, A.S. Targeting muscle signaling pathways to minimize adverse effects of androgen deprivation. Endocr. Relat. Cancer 2016, 23, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyake, H.; Matsushita, Y.; Watanabe, H.; Tamura, K.; Motoyama, D.; Ito, T.; Sugiyama, T.; Otsuka, A. Prognostic Significance of Time to Castration Resistance in Patients With Metastatic Castration-sensitive Prostate Cancer. Anticancer Res. 2019, 39, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Maeda, H.; Takeda, K.; Urushihara, H.; Kurokawa, T. Searching for potential surrogate endpoints of overall survival in clinical trials for patients with prostate cancer. Cancer Rep. 2021, 4, e1334. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Analyzed Parameter | Group 1 (n = 34) | Group 2 (n = 30) | p-Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age [year] | 68.6 | 7.1 | 72.0 | 7.5 | 0.0612 |
| Body weight [kg] | 87.6 | 17.8 | 85.8 | 15.1 | 0.9571 |
| Body height [cm] | 174.9 | 6.3 | 170.7 | 6.7 | 0.001 |
| BMI * [kg/m2] | 28.5 | 4.9 | 29.3 | 4.4 | 0.5316 |
| BMI categories [%] | |||||
| Underweight | 3 | 0 | 0.3441 | ||
| Normal | 20 | 19 | |||
| Overweight | 35 | 37 | |||
| Obesity | 42 | 44 | |||
| Gleason’s score | Median: 8 | Range: 5–9 | Median:7 | Range: 4–9 | |
| 0.5641 | |||||
| GS ≤ 6 (no) | 1 | 9 | |||
| GS 7 | 11 | 14 | 0.008 | ||
| GS 8–10 | 22 | 7 | |||
| Metastasis sites %: | 0.3318 | ||||
| Bones | 94 | 70 | |||
| Lymph nodes | 74 | 53 | |||
| Parenchymal organs | 3 | 0 | |||
| WHO scale [%] | <0.001 | ||||
| 0 | 6 | 100 | |||
| 1 | 70 | ||||
| 2 | 24 | ||||
| NRS [%] * | 0.005 | ||||
| 0–2 | 80 | 62 | |||
| ≥3 | 20 | 38 | |||
| Medical History | Group 1 (n = 34) | Group 2 (n = 30) |
|---|---|---|
| Current radical treatment [%]: | ||
| Lack | 88.2 | 23.3 |
| Radiotherapy | 11.8 | 63.3 |
| Prostatectomy | 0 | 13.3 |
| The presence of additional diseases [%]: | ||
| Diabetes | 26.5 | 16.6 |
| Hypertension | 61.8 | 66.7 |
| Ischemic heart disease | 14.7 | 46.76 |
| Other: (thyroid disease, gout, glaucoma, depression, hepatitis, cardiac arrhythmias, stroke, chronic obstructive pulmonary disease, renal failure, degenerative spine disease, radiation proctitis, valvular disease) | 44.1 | 40.0 |
| Qualification for therapy [%]: | ||
| Docetaxel 75 mg/m2 | 79.5 | - |
| Docetaxel 50 mg/m2 | 20.5 | - |
| Enzalutamide | - | 30 |
| Abiraterone with Prednisone | - | 70 |
| Baseline | Progression | ||||
|---|---|---|---|---|---|
| Analyzed Parameter | Median | SD | Median | SD | p-Value |
| Group 1 (n = 34) | |||||
| TM [cm2] | 164.2 | 31.4 | 153.4 | 28.8 | <0.0001 |
| SF [cm2] | 202.4 | 103.2 | 237.8 | 120.1 | 0.0115 |
| VF [cm2] | 273.8 | 134.6 | 308.9 | 130.6 | 0.0209 |
| SMI [cm2/m2] | 54.01 | 9.85 | 50.4 | 9.61 | <0.0001 |
| SATI [cm2/m2] | 66.47 | 33.36 | 78.2 | 39.2 | 0.0088 |
| VATI [cm2/m2] | 90.40 | 44.2 | 101.7 | 42.6 | 0.0191 |
| Group 2 (n = 30) | |||||
| TM [cm2] | 151.6 | 25.2 | 138.3 | 20.6 | <0.0001 |
| SF [cm2] | 250.9 | 86.3 | 267.8 | 115.0 | 0.1625 |
| VF [cm2] | 321.8 | 113.0 | 326.5 | 114.7 | 0.2966 |
| SMI [cm2/m2] | 52.0 | 8.311 | 47.4 | 6.46 | <0.0001 |
| SATI [cm2/m2] | 86.1 | 29.7 | 92.01 | 40.2 | 0.1591 |
| VATI [cm2/m2] | 110.2 | 37.9 | 112.4 | 39.89 | 0.211 |
| Subgroup with NRS ≥ 3 (n = 19) | |||||
| TM [cm2] | 133.7 | 33.2 | 129.2 | 30.5 | 0.0017 |
| SF [cm2] | 156.0 | 67.9 | 183.4 | 73.2 | 0.0187 |
| VF [cm2] | 192.1 | 126.4 | 238.6 | 111.0 | 0.0075 |
| SMI [cm2/m2] | 44.3 | 9.84 | 43.4 | 8.81 | 0.0012 |
| SATI [cm2/m2] | 54.2 | 24.7 | 62.4 | 25.6 | 0.0187 |
| VATI [cm2/m2] | 70.6 | 40.3 | 87.3 | 36.1 | 0.0084 |
| Comparisons | Hazard Ratio (95% CI) | |
|---|---|---|
| Group 1 | Group 2 | |
| Sarcopenia vs. no sarcopenia | 1.424 (0.5974–3.396) | 0.7539 (0.2615–2.174) |
| BMI < 30 vs. BMI > 30 kg/m2 | 1.159 (0.4732–2.838) | 0.6522 (0.2203–1.930) |
| Muscle mass loss vs. stable muscle mass | 1.363 (0.4850–3.830) | 0.9389 (0.3202–2.753) |
| Subcutaneous fat increase vs. stable subcutaneous fat | 1.018 (0.4220–2.456) | 1.385 (0.3802–5.044) |
| Visceral fat increase vs. stable visceral fat | 1.712 (0.7100–4.129) | 1.132 (0.3488–3.676) |
| SATI < 72 vs. SATI > 72 | 1.218 (0.5002–2.968) | 0.8278 (0.2642–2.593) |
| VATI < 101 vs. VATI > 101 | 1.863 (0.7842–4.424) | 0.7092 (0.2376–2.117) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korczak, J.; Mardas, M.; Litwiniuk, M.; Bogdański, P.; Stelmach-Mardas, M. Androgen Deprivation Therapy for Prostate Cancer Influences Body Composition Increasing Risk of Sarcopenia. Nutrients 2023, 15, 1631. https://doi.org/10.3390/nu15071631
Korczak J, Mardas M, Litwiniuk M, Bogdański P, Stelmach-Mardas M. Androgen Deprivation Therapy for Prostate Cancer Influences Body Composition Increasing Risk of Sarcopenia. Nutrients. 2023; 15(7):1631. https://doi.org/10.3390/nu15071631
Chicago/Turabian StyleKorczak, Jolanta, Marcin Mardas, Maria Litwiniuk, Paweł Bogdański, and Marta Stelmach-Mardas. 2023. "Androgen Deprivation Therapy for Prostate Cancer Influences Body Composition Increasing Risk of Sarcopenia" Nutrients 15, no. 7: 1631. https://doi.org/10.3390/nu15071631