

Prevalence of Front-of-Pack Warning Signs among Commercial Complementary Foods in Seven High and Upper Middle-Income Countries


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Sources and Management
2.3. FOPNL Analysis
3. Results
3.1. Product Characteristics
3.2. Added Sugars or Sweeteners in CPCF
3.3. WHO Europe Commercial Complementary Food High Sugar FOPNL System
3.4. Traffic Light FOPNL System—Australia, UAE, UK and USA
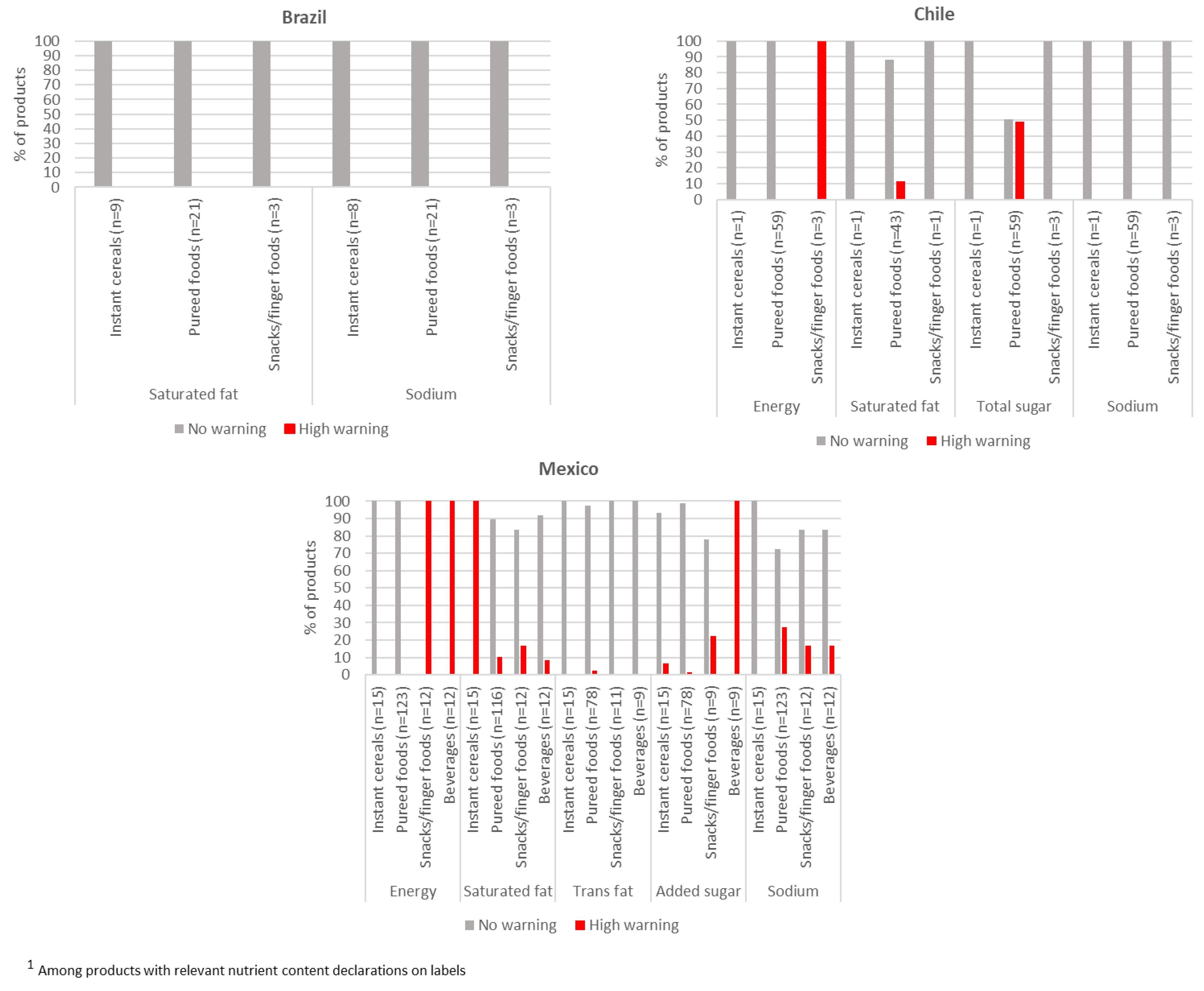
3.5. Warning Sign FOPNL System—Brazil, Chile, and Mexico
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNICEF. Improving Young Children’s Diets During the Complementary Feeding Period-UNICEF Programming Guidance; UNICEF: New York, NY, USA, 2020. [Google Scholar]
- Quinn, V.; Zehner, E.; Schofield, D.; Guyon, A.; Huffman, S. Using the Code to Guide the Marketing of Complementary Foods to Protect Optimal Infant Feeding Practices: GAIN Working Paper Series; Global Alliance for Improved Nutrition (GAIN): Geneva, Switzerland, 2010. [Google Scholar]
- WHO. First Meeting of the WHO Scientific and Technical Advisory Group on Inappropriate Promotion of Foods for Infants and Young Children; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- WHO Regional Office for Europe. Ending Inappropriate Promotion of Commercially Available Complementary Foods for Infants and Young Children between 6 and 36 Months in Europe; Copenhagen, Ø., Ed.; WHO Regional Office for Europe: København, Denmark, 2019. [Google Scholar]
- Maalouf, J.; Cogswell, M.E.; Bates, M.; Yuan, K.; Scanlon, K.S.; Pehrsson, P.; Gunn, J.P.; Merritt, R.K. Sodium, Sugar, and fat content of complementary infant and toddler foods sold in the United States, 2015. Am. J. Clin. Nutr. 2017, 105, 1443–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassetti, E.; Zehner, E.; Mayhew, S.H.; Nasser, N.; Mulder, A.; Badham, J.; Sweet, L.; Crossley, R.; Pries, A.M. Nutrient profiles of commercially produced complementary foods available in Cambodia, Indonesia and the Philippines. Public Health Nutr. 2022, 25, 2720–2730. [Google Scholar] [CrossRef]
- Tzioumis, E.; Kay, M.; Wright, M.; Adair, L. Health Effects of Commercially Available Complementary Foods: A Systematic Review. Available online: https://www.who.int/docs/default-source/nutritionlibrary/complementary-feeding/cf-health-effects-commercially-systematicreview.pdf (accessed on 7 December 2020).
- Breda, J.; Jewell, J.; Keller, A. The importance of the world health organization sugar guidelines for dental health and obesity prevention. Caries Res. 2019, 53, 149–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Cosmi, V.; Scaglioni, S.; Agostoni, C. Early taste experiences and later food choices. Nutrients 2017, 9, 107. [Google Scholar] [CrossRef] [Green Version]
- Pries, A.M.; Filteau, S.; Ferguson, E.L. Snack food and beverage consumption and young child nutrition in low- and middle-income countries: A systematic review. Matern. Child Nutr. 2019, 15 (Suppl. S4), e12729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devenish, G.; Ytterstad, E.; Begley, A.; Do, L.; Scott, J. Intake, sources, and determinants of free sugars intake in Australian children aged 12–14 months. Matern. Child Nutr. 2019, 15, e12692. [Google Scholar] [CrossRef] [Green Version]
- Devenish, G.; Golley, R.; Mukhtar, A.; Begley, A.; Ha, D.; Do, L.; Scott, J.A. Free sugars intake, sources and determinants of high consumption among Australian 2-year-olds in the smile cohort. Nutrients 2019, 11, 161. [Google Scholar] [CrossRef] [Green Version]
- Department of Health and Food Standard Agency. Diet and Nutrition Survey of Infants and Young Children, 2011; Food Standard Agency: London, UK, 2013. [Google Scholar]
- Roess, A.A.; Jacquier, E.F.; Catellier, D.J.; Carvalho, R.; Lutes, A.C.; Anater, A.S.; Dietz, W.H. The journal of nutrition supplement: Feeding infants and toddlers study (FITS) 2016 food consumption patterns of infants and toddlers: Findings from the feeding infants and toddlers study (FITS) 2016. J. Nutr. 2018, 148, 1525S–1535S. [Google Scholar] [CrossRef] [Green Version]
- Isaacs, A.; Neve, K.; Hawkes, C. Why do parents use packaged infant foods when starting complementary feeding? Findings from phase one of a longitudinal qualitative study. BMC Public Health 2022, 22, 1–11. [Google Scholar] [CrossRef]
- Afflerback, S.; Carter, S.K.; Anthony, A.K.; Grauerholz, L. Infant-feeding consumerism in the age of intensive mothering and risk society. J. Consum. Cult. 2013, 13, 387–405. [Google Scholar] [CrossRef]
- Begley, A.; Ringrose, K.; Giglia, R.; Scott, J. Mothers’ Understanding of infant feeding guidelines and their associated practices: A qualitative analysis. Int. J. Environ. Res. Public Health 2019, 16, 1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deming, D.M.; Afeiche, M.C.; Reidy, K.C.; Eldridge, A.L.; Villalpando-Carrión, S. Early feeding patterns among mexican babies: Findings from the 2012 national health and nutrition survey and implications for health and obesity prevention. BMC Nutr. 2015, 1, 1–14. [Google Scholar] [CrossRef] [Green Version]
- WHO Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 21 November 2022).
- Global Nutrition Report. 2022 Global Nutrition Report: Stronger Commitments for Greater Action. Available online: https://globalnutritionreport.org/ (accessed on 22 December 2022).
- Bryan, S.; Afful, J.; Carroll, M.; Te-Ching, C.; Orlando, D.; Fink, S.; Fryar, C. National Health and Nutrition Examination Survey 2017–March 2020 Prepandemic Data Files Development of Files and Prevalence Estimates for Selected Health Outcomes; National Center for Health Statistics: Hyattsville, MD, USA, 2021. [Google Scholar]
- UNICEF. Policy Brief: Front-of-Pack Nutrition Labelling of Foods and Beverages; UNICEF: New York, NY, USA, 2022; Volume 2060. [Google Scholar]
- Croker, H.; Packer, J.; Russell, S.J.; Stansfield, C.; Viner, R.M. Front of pack nutritional labelling schemes: A systematic review and meta-analysis of recent evidence relating to objectively measured consumption and purchasing. J. Hum. Nutr. Diet. 2020, 33, 518–537. [Google Scholar] [CrossRef] [PubMed]
- Nohlen, H.; Bakogianni, I.; Grammatikaki, E.; Ciriolo, E.; Pantazi, M.; Alves Dias, J.; Salesse, F.; Moz Christofoletti, M.; Wollgast, J.; Bruns, H.; et al. Front-of-Pack Nutrition Labelling Schemes: An Update of the Evidence, EUR 31153 EN; Publications Office of the European Union: Luxembourg, 2022; ISBN 978-92-76-55032-7. [Google Scholar] [CrossRef]
- Song, J.; Brown, M.K.; Id, M.T.; Macgregor, G.A.; Webster, J.; Campbell, N.R.C.; Trieuid, K.; Mhurchu, C.N.; Cobb, L.K.; Heid, F.J. Impact of color-coded and warning nutrition labelling schemes: A systematic review and network meta-analysis. PLoS Med. 2021, 18, e1003765. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guiding Principles and Framework Manual for Front-of-Pack Labelling for Promoting Healthy Diets; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Id, M.R.; Smith, L.; Id, T.; Popkin Id, B.; Id, R.K.; Vandevijvere Id, S.; Corvalá, C. Changes in the amount of nutrient of packaged foods and beverages after the initial implementation of the chilean law of food labelling and advertising: A nonexperimental prospective study. PLoS Med. 2020, 17, e1003220. [Google Scholar] [CrossRef]
- Taillie, L.S.; Bercholz, M.; Popkin, B.; Reyes, M.; Colchero, M.A.; Corvalán, C. Changes in food purchases after the chilean policies on food labelling, marketing, and sales in schools: A before and after study. Lancet. Planet. Health 2021, 5, e526–e533. [Google Scholar] [CrossRef]
- Alianza por la Salud Alimentaria. A Un Año de Su Implementación, El Etiquetado Frontal de Advertencia Ha Traído Cambios Positivos Indiscutibles En México; Alianza por la Salud Alimentaria: Mexico City, Mexico, 2021. [Google Scholar]
- WHO Regional Office for Europe. Use of Nutrient Profile Models for Nutrition and Health Policies: Meeting Report on the Use of Nutrient Profile Models in the WHO European Region; Copenhagen, Ø., Ed.; WHO Regional Office for Europe: København, Denmark, 2022. [Google Scholar]
- Ministry of Health of Brazil. Resolução No 429, 2020: Dispõe Sobre a Rotulagem Nutricional Dos Alimentos Embalados (Resolution—Rdc No. 429, of October 2020: Approves the New Changes on the Food Labelling for Packaged Foods). Available online: https://www.in.gov.br/en/web/dou/-/resolucao-de-diretoria-colegiada-rdc-n-429-de-8-de-outubro-de-2020-282070599 (accessed on 24 November 2022).
- Ministerio de Salud de Chile. Informe de La Evaluación de La Implementación de La Ley Sobre Composición Nutricional de Los Alimentos y Su Publicidad. Available online: https://www.minsal.cl/wp-content/uploads/2018/05/Informe-Implementación-Ley-20606-febrero-18-1.pdf (accessed on 24 November 2022).
- Secretaría de Economía de Mexico Modificación a La Norma Oficial Mexicana NOM-051-SCFI/SSA1–2010, Especificaciones Generales de Etiquetado Para Alimentos y Bebidas No Alcohólicas Preenvasados-Información Comercial y Sanitaria, Publicada El 5 de Abril de 2010. Diar. Available online: http://dof.gob.mx/2020/SEECO/NOM_051.pdf (accessed on 24 November 2022).
- United Aran Emirates Ministry of Industry & Advanced Technology. Nutritional Labelling of Pre-Packed Products as Traffic Light Colours (UAE.S 5034: 2018); United Aran Emirates Ministry of Industry & Advanced Technology: Dubai, United Arab Emirates, 2018. [Google Scholar]
- UK Department of Health and the Food Standard Agency. Guide to Creating a Front of Pack (FoP) Nutrition Label for Pre-Packed Products Sold through Retail Outlets. Available online: https://www.food.gov.uk/sites/default/files/media/document/fop-guidance_0.pdf (accessed on 7 March 2021).
- Fidler Mis, N.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.D.; Hojsak, I.; Hulst, J.; Indrio, F.; Lapillonne, A.; et al. Sugar in infants, children and adolescents: A position paper of the european society for paediatric gastroenterology, hepatology and nutrition committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 681–696. [Google Scholar] [CrossRef] [Green Version]
- Vos, M.B.; Kaar, J.L.; Welsh, J.A.; Van Horn, L.V.; Feig, D.I.; Anderson, C.A.M.; Patel, M.J.; Cruz Munos, J.; Krebs, N.F.; Xanthakos, S.A.; et al. Added sugars and cardiovascular disease risk in children: A scientific statement from the american heart association. Circulation 2017, 135, e1017–e1034. [Google Scholar] [CrossRef] [Green Version]
- Hutchinson, J.; Rippin, H.; Threapleton, D.; Jewell, J.; Kanamäe, H.; Salupuu, K.; Caroli, M.; Antignani, A.; Pace, L.; Vassallo, C.; et al. High sugar content of european commercial baby foods and proposed updates to existing recommendations. Matern. Child Nutr. 2021, 17, e13020. [Google Scholar] [CrossRef]
- Elliott, C.; Conlon, M. Packaged baby and toddler foods: Questions of sugar and sodium. Pediatr. Obes. 2014, 10, 149–155. [Google Scholar] [CrossRef]
- Garcia, A.L.; Curtin, L.; Ronquillo, J.D.; Parrett, A.; Wright, C.M. Changes in the UK baby food market surveyed in 2013 and 2019: The rise of baby snacks and sweet/savoury foods. Arch. Dis. Child. 2020, 105, 1162–1166. [Google Scholar] [CrossRef] [PubMed]
- Public Health England (PHE). Foods and Drinks Aimed at Infants and Young Children: Evidence and Opportunities for Action; Public Health England (PHE): London, UK, 2019. [Google Scholar]
- The Lancet Diabetes & Endocrinology. Baby foods: Time to get tough on sugars. Lancet Diabetes Endocrinol. 2019, 7, 583. [Google Scholar] [CrossRef]
- Foterek, K.; Buyken, A.E.; Bolzenius, K.; Hilbig, A.; Nöthlings, U.; Alexy, U. Commercial complementary food consumption is prospectively associated with added sugar intake in childhood. Br. J. Nutr. 2016, 115, 2067–2074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunford, E.; Louie, J.C.Y.; Byrne, R.; Walker, K.Z.; Flood, V.M. The nutritional profile of baby and toddler food products sold in Australian supermarkets. Matern. Child Health J. 2015, 19, 2598–2604. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.L.; McLean, K.; Wright, C.M. Types of fruits and vegetables used in commercial baby foods and their contribution to sugar content. Matern. Child Nutr. 2016, 12, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Grammatikaki, E.; Wollgast, J.; Caldeira, S. High levels of nutrients of concern in baby foods available in Europe that contain sugar-contributing ingredients or are ultra-processed. Nutrients 2021, 13, 3105. [Google Scholar] [CrossRef]
- FAO; WHO. Fats and Fatty Acids in Human Nutrition: Report of an Expert Consultation; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Codex Alimentarius. CXS 74-1981; Standard for Processed Cereal-Based Foods for Infants and Young Children Codex. Revised in 2006; Amended in 2017; Codex Alimentarius: Rome, Italy, 2019.
- WHO Regional Office for Europe. Commercial Foods for Infants and Young Children in the WHO European Region: A Study of the Availability, Composition and Marketing of Baby Foods in Four European Countries; WHO Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- Dewey, K.G. The challenge of meeting nutrient needs of infants and young children during the period of complementary feeding: An evolutionary perspective. J. Nutr. 2013, 143, 2050–2054. [Google Scholar] [CrossRef] [Green Version]
- Rousham, E.K.; Goudet, S.; Markey, O.; Griffiths, P.; Boxer, B.; Carroll, C.; Petherick, E.S.; Pradeilles, R. Unhealthy food and beverage consumption in children and risk of overweight and obesity: A systematic review and meta-analysis. Adv. Nutr. 2022, 13, 1669–1696. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA). Scientific opinion on nutrient requirements and dietary intakes of infants and young children in the european union. EFSA J. 2013, 11, 1–103. [Google Scholar] [CrossRef] [Green Version]
- Cecchini, M.; Warin, L. Impact of food labelling systems on food choices and eating behaviours: A systematic review and meta-analysis of randomized studies. Obes. Rev. 2016, 17, 201–210. [Google Scholar] [CrossRef]
- Codex Alimentarius. Proposed Draft Guidelines on Front-of-Pack Nutrition Labelling; Codex Alimentarius: Ottawa, ON, Canada, 2019. [Google Scholar]
- Maslin, K.; Galvin, A.D.; Shepherd, S. A qualitative study of mothers perceptions of weaning and the use of commercial infant food in the United Kingdom. Matern. Pediatr. Nutr. 2015, 1, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Scarpelli, D.; Fernandes, A.; Osiac, L.; Quevedo, T. Changes in nutrient declaration after the food labeling and advertising law in Chile: A longitudinal approach. Nutrients 2020, 12, 2371. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Social Care; Food Standard Agency. Building on the Success of Front-of-Pack Nutrition Labelling in the UK: A Public Consultation; Food Standard Agency: London, UK, 2020. [Google Scholar]
- Vargas-Meza, J.; Jáuregui, A.; Pacheco-Miranda, S.; Contreras-Manzano, A.; Barquera, S. Front-of-pack nutritional labels: Understanding by low- and middle-income mexican consumers. PLoS ONE 2019, 14, e0225268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correa, T.; Fierro, C.; Reyes, M.; Dillman Carpentier, F.R.; Smith Taillie, L.; Corvalan, C. Responses to the chilean law of food labeling and advertising: Exploring knowledge, perceptions and behaviors of mothers of young children. Int. J. Behav. Nutr. Phys. Activity 2019, 16, 21. [Google Scholar] [CrossRef] [PubMed]
- Codex Alimentarius Commission. Forty-Forth Session Virtual 8–18 November 2021 Report of the Forty-Sixth Session of the Codex Committee on Food Labelling; Codex Alimentarius Commission: Ottawa, ON, Canada, 2021. [Google Scholar]


{kind=link}
| Per 100 g food | Low | Medium | High | High 1 | |
| Fat | ≤3 g | >3 g to ≤17.5 g | >17.5 g | >21 g/portion | |
| Saturated fat | ≤1.5 g | >1.5 g to ≤5 g | >5.0 g | >6.0 g/portion | |
| Total sugar | ≤5 g | >5 g to ≤22.5 g | >22.5 g | >27 g/portion | |
| Salt | ≤0.3 g | >0.3 g to ≤1.5 g | >1.5 g | >1.8 g/portion | |
| Per 100 mL drinks | Low | Medium | High | High 2 | |
| Fat | ≤1.5 g | >1.5 g to ≤8.75 g | >8.75 g | >10.5 g/portion | |
| Saturated fat | ≤0.75 g | >0.75 g to ≤2.5 g | >2.5 g | >3 g/portion | |
| Total sugar | ≤2.5 g | >2.5 g to ≤11.25 g | >11.25 g | >13.5 g/portion | |
| Salt | ≤0.3 g | >0.3 g to ≤0.75 | >0.75 g | >0.9 g/portion |
| Country | Dataset Source | Total Products (n) | Instant Cereals % (n) | Pureed Foods % (n) | Snacks/Finger Foods % (n) | Beverages % (n) |
|---|---|---|---|---|---|---|
| Australia | INNOVA | 266 | 6.8 (18) | 52.3 (139) | 38.7 (103) | 2.2 (6) |
| Brazil | Euromonitor | 41 | 41.5 (17) | 51.2 (21) | 7.3 (3) | -- |
| Chile | Euromonitor | 73 | 15.1 (11) | 80.8 (59) | 4.1 (3) | -- |
| Mexico | Euromonitor | 164 | 10.4 (17) | 75.0 (123) | 7.3 (12) | 7.3 (12) |
| UAE | Euromonitor | 135 | 39.3 (53) | 41.5 (56) | 18.5 (25) | 0.7 (1) |
| UK | Euromonitor | 643 | 10.6 (68) | 69.0 (444) | 20.4 (131) | -- |
| USA | Euromonitor | 562 | 5.0 (28) | 79.2 (445) | 15.5 (87) | 0.3 (2) |
| Country | All Products | Instant Cereals | Pureed Foods | Snacks/Finger Foods | Beverages |
|---|---|---|---|---|---|
| Australia | 266 | 18 | 139 | 103 | 6 |
| Contain added sugar/sweetener % (n) | 27.8 (74) | 0.0 (0) | 15.8 (22) | 49.5 (51) | 16.7 (1) |
| Brazil | 38 | 14 | 21 | 3 | -- |
| Contain added sugar/sweetener % (n) | 47.4 (18) | 100.0 (14) | 19.1 (4) | 0.0 (0) | |
| Chile | 69 | 11 | 55 | 3 | -- |
| Contain added sugar/sweetener % (n) | 7.3 (5) | 27.3 (3) | 0.0 (0) | 66.7 (2) | |
| Mexico | 161 | 15 | 123 | 11 | 12 |
| Contain added sugar/sweetener % (n) | 38.5 (62) | 33.3 (5) | 31.7 (39) | 54.6 (6) | 100.0 (12) |
| United Arab Emirates | 110 | 47 | 43 | 19 | 1 |
| Contain added sugar/sweetener % (n) | 34.6 (38) | 36.2 (17) | 11.6 (5) | 79.0 (15) | 100.0 (1) |
| United Kingdom | 642 | 67 | 444 | 131 | -- |
| Contain added sugar/sweetener % (n) | 15.0 (96) | 11.9 (8) | 7.2 (32) | 42.8 (56) | |
| United States of America | 556 | 28 | 440 | 86 | 2 |
| Contain added sugar/sweetener % (n) | 20.2 (112) | 17.9 (5) | 8.9 (39) | 79.1 (68) | 0.0 (0) |
| Dry/Instant Cereals 2 % | Pureed Foods 3 % | Snack/Finger Foods 4 % | |
|---|---|---|---|
| Australia | 0.0% | 67.4% | 39.8% |
| Brazil | 0.0% | 100.0% | 0.0% |
| Chile | 0.0% | 52.5% | 0.0% |
| Mexico | 5.9% | 74.8% | 33.3% |
| United Arab Emirates (UAE) | 2.5% | 92.3% | 60.0% |
| United States (US) | 0.0% | 86.0% | 66.7% |
| United Kingdom (UK) | 0.0% | 62.6% | 39.7% |
| Total Fat | Saturated Fat | Total Sugar | Salt | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Green (%) | Amber (%) | Red (%) | Missing (n) 1 | Green (%) | Amber (%) | Red (%) | Missing (n) 1 | Green (%) | Amber (%) | Red (%) | Missing (n) 1 | Green (%) | Amber (%) | Red (%) | Missing (n) 1 | ||
| Australia | Dry/instant cereals (n = 18) | 100.0 | 0.0 | 0.0 | 2 | 100.0 | 0.0 | 0.0 | 10 | 100.0 | 0.0 | 0.0 | 2 | 100.0 | 0.0 | 0.0 | 2 |
| Pureed foods (n = 139) | 72.6 | 16.7 | 0.7 | 1 | 82.2 | 16.8 | 1.0 | 38 | 51.5 | 47.8 | 0.7 | 1 | 100.0 | 0.0 | 0.0 | 1 | |
| Snacks/finger foods (n = 103) | 19.4 | 69.9 | 10.7 | 0 | 52.0 | 31.4 | 16.7 | 1 | 38.8 | 32.0 | 29.1 | 0 | 79.8 | 20.2 | 0.0 | 0 | |
| beverages (n = 6) | 66.7 | 33.3 | 0.0 | 0 | 50.0 | 0.0 | 50.0 | 0 | 33.3 | 33.3 | 33.3 | 0 | 100.0 | 0.0 | 0.0 | 0 | |
| United Arab Emirates | Dry/instant cereals (n = 53) | 80.0 | 20.0 | 0.0 | 23 | 95.5 | 4.5 | 0.0 | 31 | 50.0 | 50.0 | 0.0 | 35 | 100.0 | 0.0 | 0.0 | 23 |
| Pureed foods (n = 56) | 94.0 | 6.0 | 0.0 | 6 | 85.5 | 15.0 | 0.0 | 36 | 14.3 | 83.7 | 2.0 | 7 | 95.7 | 0.0 | 4.3 | 9 | |
| Snacks/finger foods (n = 25) | 9.1 | 81.8 | 9.1 | 3 | 15.4 | 61.5 | 23.1 | 12 | 22.7 | 31.8 | 45.5 | 3 | 86.4 | 13.6 | 0.0 | 3 | |
| Beverages (n = 1) | 100.0 | 0.0 | 0.0 | 0 | - | - | - | 1 | - | - | - | 1 | 100.0 | 0.0 | 0.0 | 0 | |
| United Kingdom | Dry/instant cereals (n = 68) | 61.4 | 38.6 | 0.0 | 24 | 95.4 | 4.6 | 0.0 | 24 | 18.2 | 81.8 | 0.0 | 24 | 100.0 | 0.0 | 0.0 | 24 |
| Pureed foods (n = 444) | 89.4 | 10.6 | 0.0 | 0 | 88.7 | 11.3 | 0.0 | 0 | 55.2 | 44.6 | 0.2 | 0 | 99.8 | 0.2 | 0.0 | 15 | |
| Snacks/finger foods (n = 131) | 19.2 | 73.9 | 6.9 | 1 | 57.7 | 33.1 | 9.2 | 1 | 32.3 | 40.0 | 27.7 | 1 | 80.0 | 19.2 | 0.8 | 1 | |
| United States | Dry/instant cereals (n = 28) | 100.0 | 0.0 | 0.0 | 23 | 100.0 | 0.0 | 0.0 | 26 | 40.0 | 60.0 | 0.0 | 23 | 100.0 | 0.0 | 0.0 | 23 |
| Pureed foods (n = 445) | 95.1 | 4.7 | 0.2 | 0 | 97.2 | 2.8 | 0.0 | 127 | 22.8 | 76.7 | 0.5 | 7 | 97.1 | 2.9 | 0.0 | 0 | |
| Snacks/finger foods (n = 87) | 66.7 | 20.7 | 12.6 | 0 | 95.1 | 1.6 | 3.3 | 26 | 17.3 | 49.4 | 33.3 | 6 | 50.6 | 48.3 | 1.1 | 0 | |
| Beverages (n = 2) | 100.0 | 0.0 | 0.0 | 0 | 100.0 | 0.0 | 0.0 | 0 | 100.0 | 0.0 | 0.0 | 0 | 100.0 | 0.0 | 0.0 | 0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bassetti, E.; Khosravi, A.; Pries, A.M. Prevalence of Front-of-Pack Warning Signs among Commercial Complementary Foods in Seven High and Upper Middle-Income Countries. Nutrients 2023, 15, 1629. https://doi.org/10.3390/nu15071629
Bassetti E, Khosravi A, Pries AM. Prevalence of Front-of-Pack Warning Signs among Commercial Complementary Foods in Seven High and Upper Middle-Income Countries. Nutrients. 2023; 15(7):1629. https://doi.org/10.3390/nu15071629
Chicago/Turabian StyleBassetti, Eleonora, Asha Khosravi, and Alissa M. Pries. 2023. "Prevalence of Front-of-Pack Warning Signs among Commercial Complementary Foods in Seven High and Upper Middle-Income Countries" Nutrients 15, no. 7: 1629. https://doi.org/10.3390/nu15071629