
Moderate Beer Consumption Is Associated with Good Physical and Mental Health Status and Increased Social Support

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Alcohol and Beer Consumption
2.3. Health and Social Support Variables
2.4. Health-Related Lifestyle Variables
2.5. Sociodemographic Variables
2.6. Statistical Analysis
3. Results
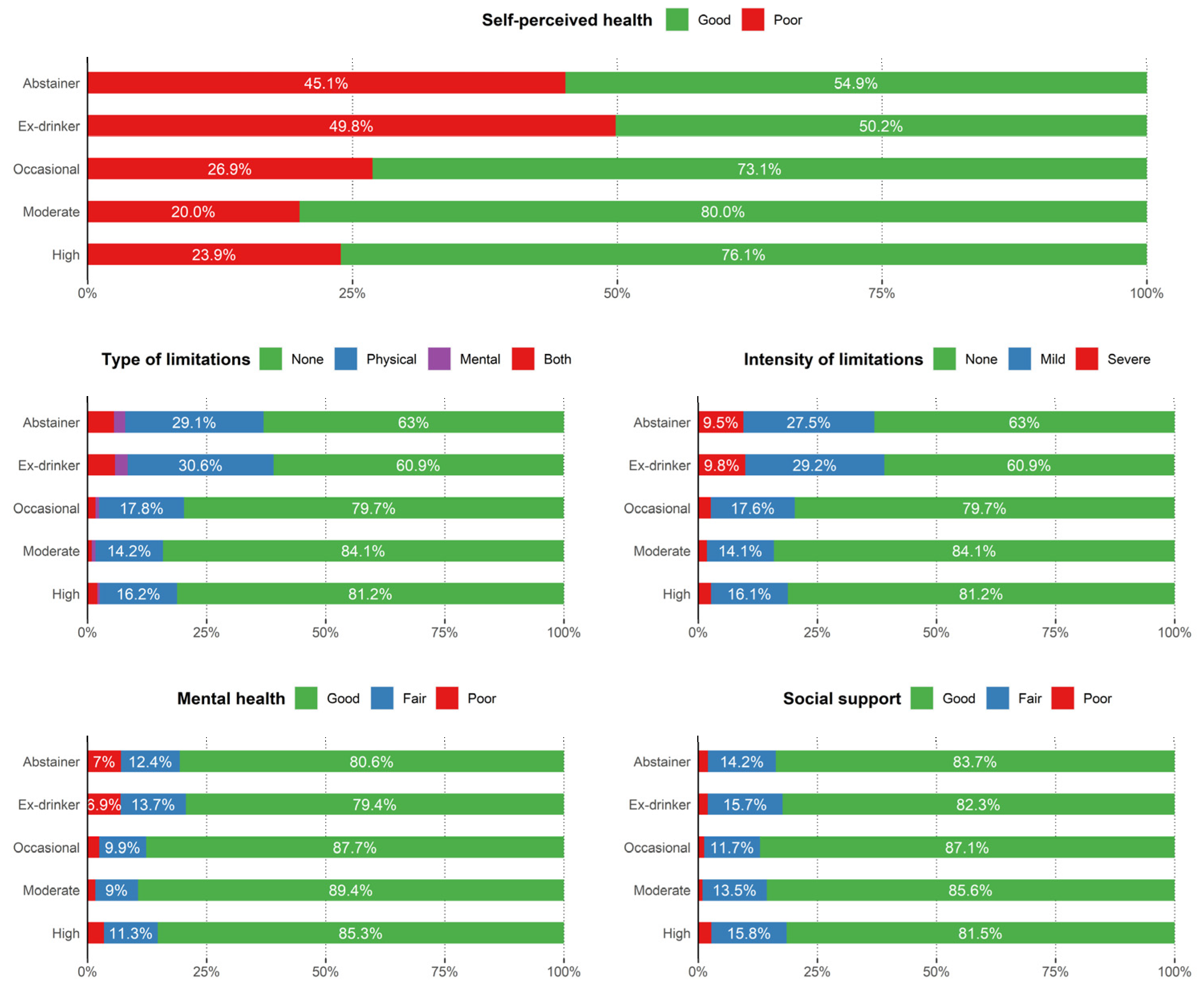
3.1. Descriptive Results
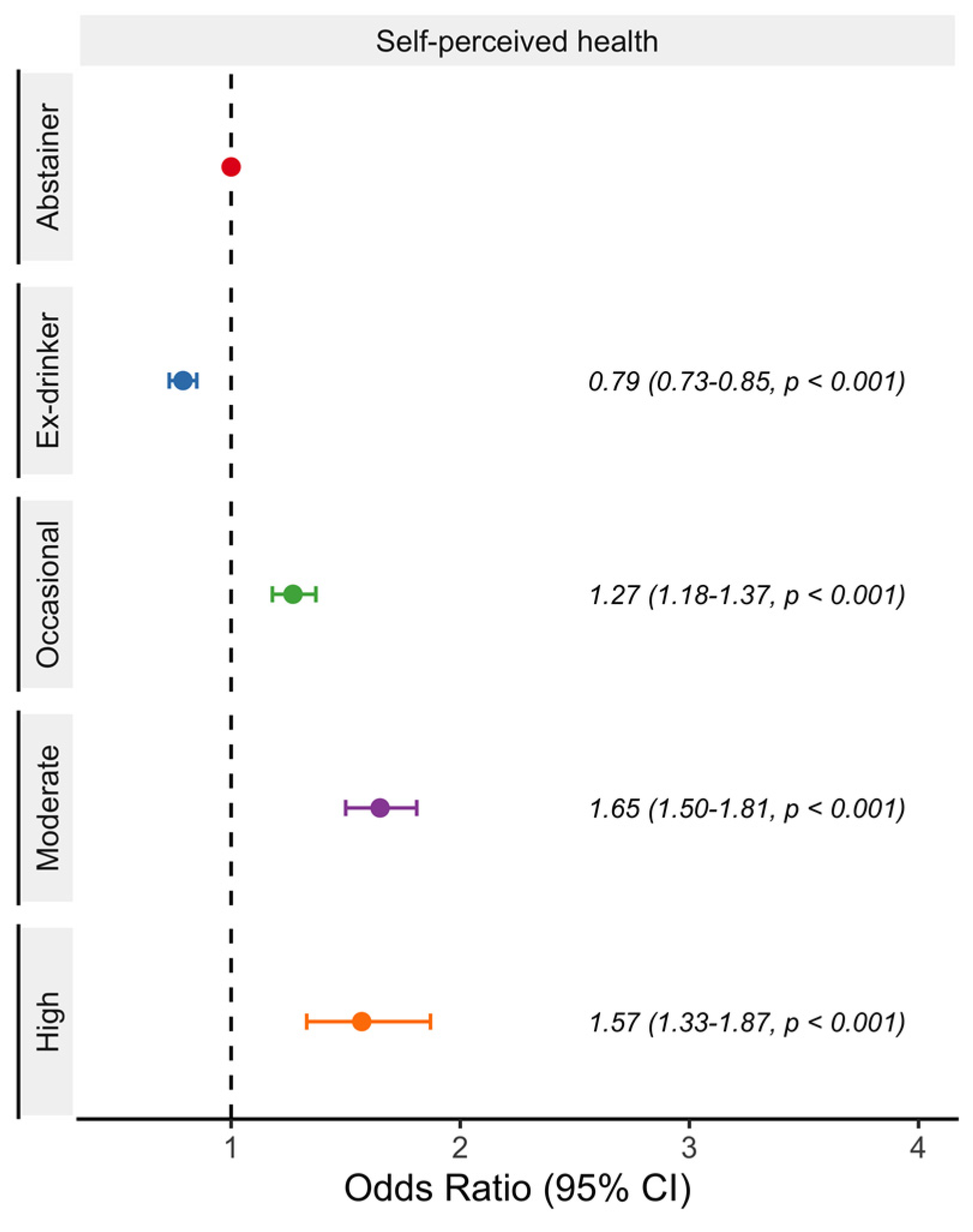
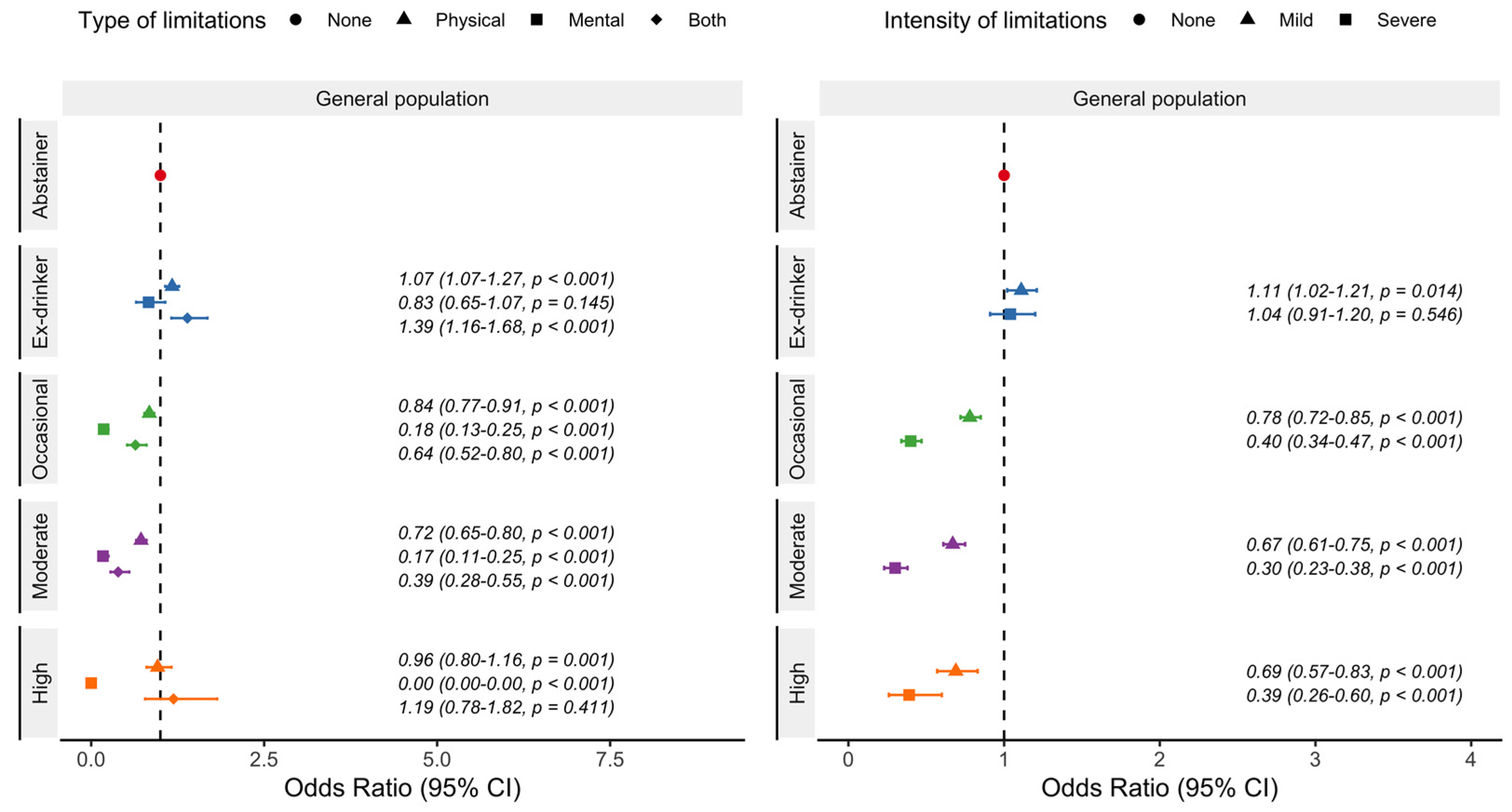
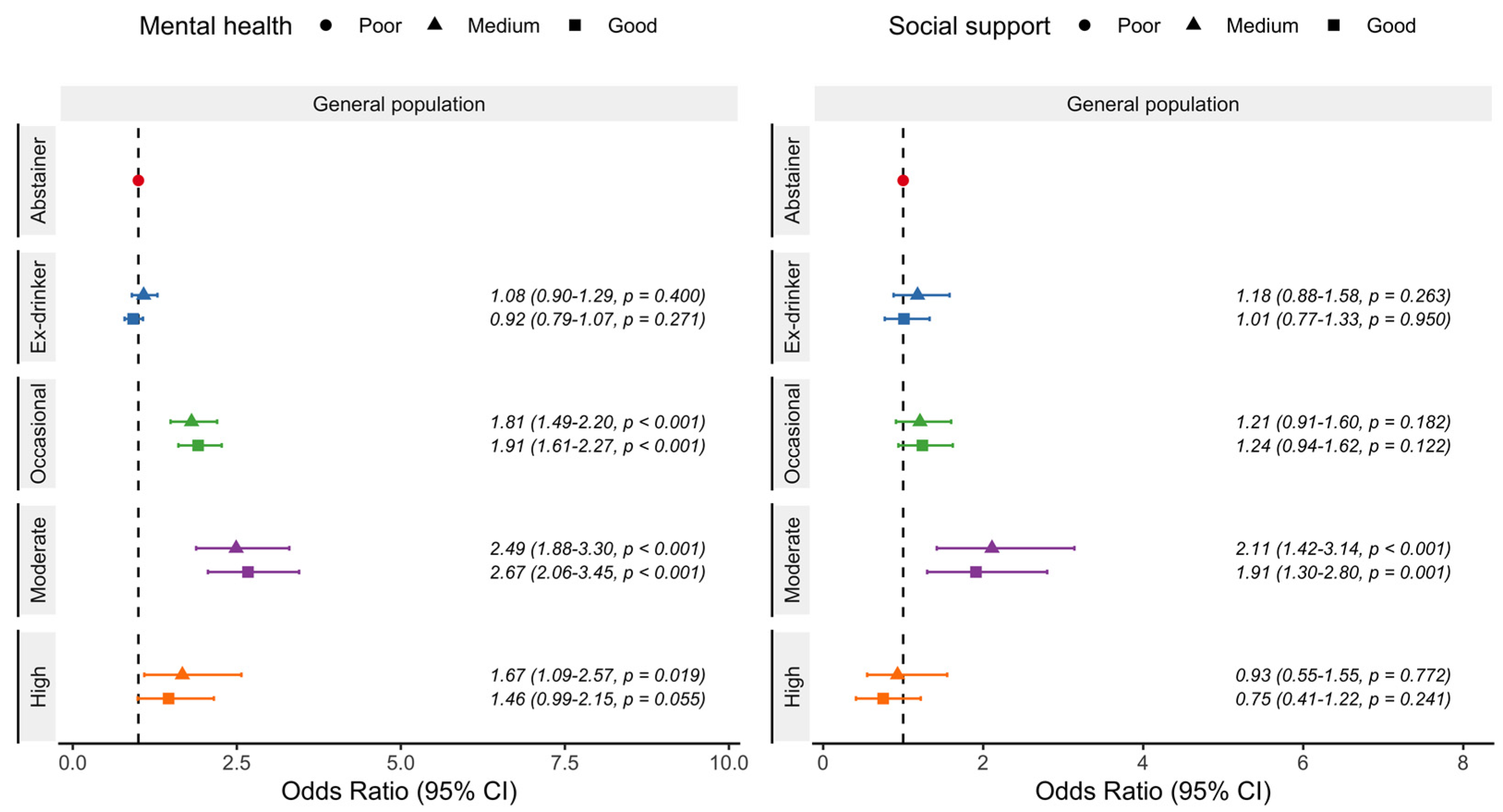
3.2. General Logistic Regression Model Results and Sensitive Analyses
3.3. Gender and Age Logistic Regression Model Results
4. Discussion
4.1. Main Findings
4.2. Comparisons with Other Studies and Potential Hypothetical Explanations
4.3. Study Limitations
4.4. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Day, E.; Rudd, J.H.F. Alcohol use disorders and the heart. Addiction 2019, 114, 1670–1678. [Google Scholar] [PubMed] [Green Version]
- Spaggiari, G.; Cignarelli, A.; Sansone, A.; Baldi, M.; Santi, D. To beer or not to beer: A meta-analysis of the effects of beer consumption on cardiovascular health. PLoS ONE 2020, 15, e0233619. [Google Scholar]
- Parekh, N.; Lin, Y.; Chan, M.; Juul, F.; Makarem, N. Longitudinal dimensions of alcohol consumption and dietary intake in the Framingham Heart Study Offspring Cohort (1971–2008). Br. J. Nutr. 2021, 125, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Marcos, A.; Serra-Majem, L.; Pérez-Jiménez, F.J.; Pascual, V.; Tinahones, F.J.; Estruch, R. Moderate consumption of beer and its effects on cardiovascular and metabolic health: An updated review of recent scientific evidence. Nutrients 2021, 13, 879. [Google Scholar] [CrossRef]
- Liu, Y.T.; Lee, J.H.; Tsai, M.K.; Cheng, J.; Wei, C. The effects of modest drinking on life expectancy and mortality risks: A population-based cohort study. Sci. Rep. 2022, 12, 7476. [Google Scholar]
- Ronksley, P.E.; Brien, S.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Association of alcohol consumption with selected cardiovascular disease outcomes: A systematic review and meta-analysis. BMJ 2011, 342, d671. [Google Scholar]
- GBD 2020 Alcohol Collaborators. Population-level risks of alcohol consumption by amount, geography, age, sex, and year: A systematic analysis for the Global Burden of Disease Study 2020. Lancet 2022, 400, 185–235. [Google Scholar]
- Weyerer, S.; Schäufele, M.; Wiese, B.; Maier, W.; Tebarth, F.; Van den Bussche, H.; Pentzek, M.; Bickel, H.; Luppa, M.; Riedel-Heller, S.G. Current alcohol consumption and its relationship to incident dementia: Results from a 3-year follow-up study among primary care attenders aged 75 years and older. Age Ageing 2011, 40, 456–463. [Google Scholar]
- Kondo, K. Beer and health: Preventive effects of beer components on lifestyle-related diseases. BioFactors 2004, 22, 303–310. [Google Scholar] [CrossRef]
- GBD 2016 Alcohol Collaborators. Alcohol use and burden for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef] [Green Version]
- Ding, C.; O’Neill, D.; Bell, S.; Stamatakis, E.; Britton, A. Association of alcohol consumption with morbidity and mortality in patients with cardiovascular disease: Original data and meta-analysis of 48,423 men and women. BMC Med. 2021, 19, 167. [Google Scholar] [CrossRef]
- Schutte, R.; Smith, L.; Wannamethee, G. Alcohol—The myth of cardiovascular protection. Clin. Nutr. 2021, 41, 348–355. [Google Scholar] [CrossRef]
- Stockwell, T.; Zhao, J.; Panwar, S.; Roemer, A.; Naimi, T.; Chikritzhs, T. Do “Moderate” Drinkers Have Reduced Mortality Risk? A Systematic Review and Meta-Analysis of Alcohol Consumption and All-Cause Mortality. J. Stud. Alcohol Drugs 2016, 77, 185–198. [Google Scholar] [CrossRef] [Green Version]
- Burton, R.; Sheron, N. Complex relationship between health and moderate alcohol use. Lancet 2022, 400, 141–143. [Google Scholar] [CrossRef]
- Eckardt, M.J.; File, S.E.; Gessa, G.L.; Grant, K.A.; Guerri, C.; Hoffman, P.L.; Kalant, H.; Koob, G.F.; Li, T.K.; Tabakoff, B. Effects of moderate alcohol consumption on the central nervous system. Alcohol. Clin. Exp. Res. 1998, 22, 998–1040. [Google Scholar]
- Le Daré, B.; Lagente, V.; Gicquel, T. Ethanol and its metabolites: Update on toxicity, benefits, and focus on immunomodulatory effects. Drug Metab. Rev. 2019, 51, 545–561. [Google Scholar] [CrossRef]
- Fernández-Solà, J. Cardiovascular risks and benefits of moderate and heavy alcohol consumption. Nat. Rev. Cardiol. 2015, 12, 576–587. [Google Scholar]
- Diao, Y.; Nie, J.; Tan, P.; Zhao, Y.; Zhao, T.; Tu, J.; Ji, H.; Cao, Y.; Wu, Z.; Liang, H.; et al. Long-term low-dose ethanol intake improves healthspan and resists high-fat diet-induced obesity in mice. Aging 2020, 12, 13128–13146. [Google Scholar] [CrossRef]
- Tizabi, Y.; Getachew, B.; Ferguson, C.L.; Csoka, A.B.; Thompson, K.M.; Gomez-Paz, A.; Ruda-Kucerova, J.; Taylor, R.E. Low Vs. High Alcohol: Central Benefits Vs. Detriments. Neurotox. Res. 2018, 34, 860–869. [Google Scholar] [CrossRef]
- Olas, B.; Bryś, M. Beer components and their beneficial effect on the hemostasis and cardiovascular diseases—Truth or falsehood. Food Chem. Toxicol. 2020, 146, 111782. [Google Scholar]
- Arranz, S.; Chiva-Blanch, G.; Valderas-Martínez, P.; Medina-Remón, A.; Lamuela-Raventós, R.M.; Estruch, R. Wine, Beer, Alcohol and Polyphenols on Cardiovascular Disease and Cancer. Nutrients 2012, 4, 759–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcos, A.; López Díaz-Ufano, M.; Pascual Fuster, V. ¿El consumo moderado de cerveza podría incluirse dentro de una alimentación saludable? Semergen 2015, 41, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redondo, N.; Nova, E.; Díaz-Prieto, L.E.; Marcos, A. Efectos del consumo moderado de cerveza en la salud. Nutr. Hosp. 2018, 35, 41–44. [Google Scholar] [PubMed]
- Schrieks, I.C.; Joosten, M.M.; Klöpping-Ketelaars, W.A.A.; Witkamp, R.F.; Hendriks, H.F.J. Moderate alcohol consumption after a mental stressor attenuates the endocrine stress response. Alcohol 2016, 57, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Hawkley, L.C. Loneliness and health. Nat. Rev. 2022, 8, 1–2. [Google Scholar]
- Knox, J.; Schneider, J.; Greene, E.; Nicholson, J.; Hasin, D.; Sandfort, T. Using social network analysis to examine alcohol use among adults: A systematic review. PLoS ONE 2019, 14, e0221360. [Google Scholar] [CrossRef] [Green Version]
- Silva, A.P.; Jager, G.; Van Zyl, H.; Voss, H.P.; Pintado, M.; Hogg, T.; De Graaf, C. Cheers, proost, saúde: Cultural, contextual and psychological factors of wine and beer consumption in Portugal and in the Netherlands. Crit. Rev. Food Sci. Nutr. 2017, 57, 1340–1349. [Google Scholar] [CrossRef]
- STROBE Statement. STROBE Statement—Checklist of items that should be included in reports of observational studies (© STROBE Initiative). Int. J. Public Health 2008, 53, 3–4. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. Encuesta Nacional de Salud de España. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176783&menu=resultados&idp=1254735573175#!tabs-1254736195650 (accessed on 1 April 2022).
- Del Boca, F.K.; Darkes, J. The validity of self-reports of alcohol consumption: State of the science and challenges for research. Addiction 2003, 98, 1–12. [Google Scholar] [CrossRef]
- Herbeth, B.; Samara, A.; Stathopoulou, M.; Siest, G.; Visvikis-Siest, S. Alcohol consumption, beverage preference, and diet in middle-aged men from the Stanislas study. J. Nutr. Metab. 2012, 2012, 987243. [Google Scholar] [CrossRef] [Green Version]
- Mortensen, E.L.; Jensen, H.H.; Sanders, S.A.; Reinisch, J.M. Better Psychological Functioning and Higher Social Status May Largely Explain the Apparent Health Benefits of Wine. Arch. Intern. Med. 2001, 161, 1844–1848. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef]
- Broadhead, W.E.; Gehlbach, S.H.; de Gruy, F.V.; Kaplan, B.H. The Duke-UNC functional social support questionnaire: Measurement of social support in family medicine patients. Med. Care 1988, 26, 707–721. [Google Scholar] [CrossRef]
- World Health Organization. WHO Technical Report Series 894: Obesity: Preventing and Managing the Global Epidemic; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- United Nations Educational, Scientific and Cultural Organization (UNESCO); Unesco Institute for Statistics. ISCED International Standard Classification of Education 2011; UNESCO: Paris, France, 2012. [Google Scholar]
- Domingo-Salvany, A.; Bacigalupe, A.; Carrasco, J.M.; Espelt, A.; Ferrando, J.; Borrell, C. Propuestas de clase social neoweberiana y neomarxista a partir de la Clasificación Nacional de Ocupaciones 2011. Gac. Sanit. 2013, 27, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Chan, T.W.; Goldthorpe, J.H. Class and status: The conceptual distinction and its empirical relevance. Am. Sociol. Rev. 2007, 72, 512–532. [Google Scholar] [CrossRef]
- Kunst, A.E.; Bos, V.; Mackenbach, J. Monitoring Socio-Economic Inequalities in Health in the European Union: Guidelines and illustrations; Erasmus University Rotterdam: Rotterdam, The Netherlands, 2001. [Google Scholar]
- De Gaetano, G.; Costanzo, S.; Di Castelnuovo, A.; Badimon, L.; Bejko, D.; Alkerwi, A.; Chiva-Blanch, G.; Estruch, R.; La Vecchia, C.; Panico, S.; et al. Effects of moderate beer consumption on health and disease: A consensus document. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 443–467. [Google Scholar] [CrossRef] [Green Version]
- Nichols, T.; Levey, D. Alcohol consumption and telomere length: Mendelian randomization clarifies alcohol’s effects. Mol. Psychiatry 2022, 27, 4001–4008. [Google Scholar]
- Guallar-Castillón, P.; Rodríguez-Artalejo, F.; Díez Gañán, L.; Banegas Banegas, J.R.; Lafuente Urdinguio, P.; Herruzo Cabrera, R. Consumption of alcoholic beverages and subjective health in Spain. J. Epidemiol. Community Health 2001, 55, 648–652. [Google Scholar] [CrossRef] [Green Version]
- González-Rubio, E.; San Mauro, I.; López-Ruíz, C.; Díaz-Prieto, L.E.; Marcos, A.; Nova, E. Relationship of moderate alcohol intake and type of beverage with health behaviors and quality of life in elderly subjects. Qual. Life Res. 2016, 25, 1931–1942. [Google Scholar] [CrossRef]
- Strandberg, T.E.; Strandberg, A.Y.; Salomaa, V.V.; Pitkälä, K.; Tilvis, R.S.; Miettinen, T.A. Alcoholic beverage preference, 29-year mortality, and quality of life in men in old age. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Sayette, M.A.; Creswell, K.G.; Dimoff, J.D.; Fairbairn, C.E.; Cohn, J.F.; Heckman, B.W.; Kirchner, T.R.; Levine, J.M.; Moreland, R.L. Alcohol and Group Formation: A Multimodal Investigation of the Effects of Alcohol on Emotion and Social Bonding. Psychol. Sci. 2012, 23, 869–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunsberger, M.; Mehlig, K.; Björkelund, C.; Lissner, L. Regular versus episodic drinking in Swedish women: Reporting of regular drinking may be less biased by social desirability. Alcohol 2020, 86, 57–63. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abstainer | Ex-Drinker | Occasional | Beer Consumption | p-Value | ||
|---|---|---|---|---|---|---|
| Moderate | High | |||||
| Total (n, %) | 8929 (26.91) | 6350 (19.14) | 11,421 (34.42) | 5468 (16.48) | 1017 (3.06) | - |
| Gender (n, %) | ||||||
| Men | 1956 (21.91) | 2393 (37.69) | 4735 (41.46) | 3673 (67.17) | 621 (61.06) | <0.001 |
| Women | 6973 (78.09) | 3957 (62.31) | 6686 (58.54) | 1795 (32.83) | 396 (38.94) | |
| Age (mean, SD) | 58.26 (19.94) | 59.95 (18.61) | 47.43 (17.24) | 46.68 (13.70) | 49.27 (12.97) | <0.001 |
| Age group (n, %) | ||||||
| 18–34 | 1288 (14.42) | 664 (10.46) | 2875 (25.17) | 1024 (18.73) | 132 (12.98) | <0.001 |
| 35–64 | 3787 (42.41) | 2858 (45.01) | 6433 (56.33) | 3846 (70.34) | 754 (74.14) | |
| ≥65 | 3854 (43.16) | 2828 (44.54) | 2113 (18.50) | 598 (10.94) | 131 (12.88) | |
| Education (n, %) | ||||||
| Primary or no education | 4385 (49.17) | 2795 (44.06) | 2471 (21.66) | 867 (15.86) | 221 (21.77) | <0.001 |
| Secondary | 3730 (41.83) | 2932 (46.22) | 6703 (58.76) | 3369 (61.65) | 611 (60.20) | |
| University | 803 (9.00) | 616 (9.71) | 2234 (19.58) | 1229 (22.49) | 183 (18.03) | |
| Occupational social class (n, %) | ||||||
| Low | 6009 (72.06) | 4341 (70.85) | 6698 (60.09) | 3042 (56.27) | 609 (61.02) | <0.001 |
| Middle | 1317 (15.79) | 1046 (17.07) | 2235 (20.05) | 1137 (21.03) | 205 (20.54) | |
| High | 1013 (12.15) | 740 (12.08) | 2214 (19.86) | 1227 (22.70) | 184 (18.44) | |
| Resident place (n, %) | ||||||
| Rural | 2208 (24.73) | 1674 (26.36) | 2294 (20.09) | 1072 (19.60) | 273 (26.84) | <0.001 |
| Suburban | 5872 (65.76) | 3989 (62.82) | 7659 (67.06) | 3577 (65.42) | 607 (59.69) | |
| Urban | 849 (9.51) | 687 (10.82) | 1468 (12.85) | 819 (14.98) | 137 (13.47) | |
| Year of survey (n, %) | ||||||
| 2012 | 4558 (51.05) | 2839 (44.71) | 5131 (44.93) | 2492 (45.57) | 409 (40.22) | <0.001 |
| 2017 | 4371 (48.95) | 3511 (55.29) | 6290 (55.07) | 2976 (54.43) | 608 (59.78) | |
| Leisure time physical activity (n, %) | ||||||
| Never | 4738 (53.08) | 3213 (50.62) | 4285 (37.53) | 1953 (35.72) | 417 (41.00) | <0.001 |
| Occasionally | 3203 (35.88) | 2440 (38.44) | 4280 (37.48) | 1897 (34.69) | 366 (35.99) | |
| Several times per month | 495 (5.55) | 373 (5.88) | 1483 (12.99) | 845 (15.45) | 136 (13.37) | |
| Several times per week | 490 (5.49) | 321 (5.06) | 1371 (12.01) | 773 (14.14) | 98 (9.64) | |
| Fruit intake (n, %) | ||||||
| Almost never or never | 204 (2.29) | 175 (2.76) | 298 (2.61) | 211 (3.86) | 90 (8.86) | <0.001 |
| Less than once per week | 212 (2.38) | 177 (2.79) | 372 (3.26) | 206 (3.77) | 74 (7.28) | |
| Once or twice per week | 562 (6.30) | 427 (6.73) | 1049 (9.19) | 578 (10.57) | 167 (16.44) | |
| Three or more times per week, but not daily | 1496 (16.77) | 1113 (17.54) | 2615 (22.90) | 1119 (20.46) | 219 (21.56) | |
| Once or more times per day | 6448 (72.27) | 4453 (70.18) | 7086 (62.05) | 3354 (61.34) | 466 (45.87) | |
| Vegetables intake (n, %) | ||||||
| Almost never or never | 125 (1.40) | 97 (1.53) | 117 (1.02) | 50 (0.91) | 19 (1.87) | <0.001 |
| Less than once per week | 205 (2.30) | 142 (2.24) | 253 (2.22) | 136 (2.49) | 34 (3.35) | |
| Once or twice per week | 1012 (11.35) | 692 (10.91) | 1265 (11.08) | 659 (12.05) | 139 (13.69) | |
| Three or more times per week, but not daily | 3546 (39.77) | 2625 (41.39) | 4816 (42.18) | 2278 (41.66) | 443 (43.65) | |
| Once or more times per day | 4029 (45.18) | 2786 (43.93) | 4967 (43.50) | 2345 (42.89) | 380 (37.44) | |
| Sweets intake (n, %) | ||||||
| Almost never or never | 1729 (19.40) | 1241 (19.57) | 1613 (14.13) | 873 (15.97) | 214 (21.10) | <0.001 |
| Less than once per week | 1469 (16.48) | 1119 (17.65) | 1947 (17.06) | 889 (16.26) | 182 (17.95) | |
| Once or twice per week | 1650 (18.51) | 1166 (18.39) | 2543 (22.28) | 1219 (22.30) | 217 (21.40) | |
| Three or more times per week, but not daily | 1548 (17.37) | 1012 (15.96) | 2249 (19.70) | 1062 (19.43) | 184 (18.15) | |
| Once or more times per day | 2516 (28.23) | 3063 (26.83) | 3063 (26.83) | 1423 (26.03) | 217 (21.40) | |
| Sweetened beverages intake (n, %) | ||||||
| Almost never or never | 5173 (58.06) | 3538 (55.85) | 4900 (42.95) | 2289 (41.91) | 454 (44.73) | <0.001 |
| Less than once per week | 1333 (14.96) | 1152 (18.18) | 2385 (20.90) | 1089 (19.94) | 207 (20.39) | |
| Once or twice per week | 1071 (12.02) | 693 (10.94) | 1952 (17.11) | 961 (17.59) | 142 (13.99) | |
| Three or more times per week, but not daily | 605 (6.79) | 412 (6.50) | 1055 (9.25) | 566 (10.36) | 86 (8.47) | |
| Once or more times per day | 728 (8.17) | 540 (8.52) | 1117 (9.79) | 557 (10.20) | 126 (12.41) | |
| Fast food intake (n, %) | ||||||
| Almost never or never | 5236 (58.79) | 3538 (55.84) | 4392 (38.49) | 1884 (34.48) | 346 (34.16) | <0.001 |
| Less than once per week | 1998 (22.43) | 1596 (25.19) | 3493 (30.61) | 1663 (30.44) | 305 (30.11) | |
| Once or twice per week | 1309 (14.70) | 942 (14.87) | 2820 (24.72) | 1517 (27.76) | 275 (27.15) | |
| Three or more times per week, but not daily | 304 (3.41) | 205 (3.24) | 568 (4.98) | 299 (5.47) | 60 (5.92) | |
| Once or more times per day | 59 (0.66) | 55 (0.87) | 137 (1.20) | 101 (1.85) | 27 (2.67) | |
| Snacks intake (n, %) | ||||||
| Almost never or never | 4905 (55.06) | 3430 (54.12) | 4501 (39.46) | 1734 (31.73) | 288 (28.37) | <0.001 |
| Less than once per week | 2315 (25.99) | 1713 (27.03) | 3531 (30.95) | 1728 (31.63) | 288 (28.37) | |
| Once or twice per week | 1229 (13.80) | 926 (14.61) | 2647 (23.21) | 1504 (27.53) | 273 (26.90) | |
| Three or more times per week, but not daily | 379 (4.25) | 219 (3.46) | 601 (5.27) | 397 (7.27) | 127 (12.51) | |
| Once or more times per day | 80 (0.90) | 50 (0.79) | 127 (1.11) | 101 (1.85) | 39 (3.84) | |
| Body Mass Index (n, %) | ||||||
| Insufficient weight | 176 (2.22) | 108 (1.89) | 252 (2.33) | 71 (1.34) | 23 (2.33) | <0.001 |
| Normal weight | 3221 (40.57) | 2195 (38.43) | 5043 (46.65) | 2355 (44.29) | 425 (43.06) | |
| Overweight | 2834 (35.70) | 2164 (37.89) | 3784 (35.00) | 2145 (40.34) | 379 (38.40) | |
| Obesity | 1708 (21.51) | 1244 (21.78) | 1731 (16.01) | 746 (14.03) | 160 (16.21) | |
| Tobacco use (n, %) | ||||||
| Never | 6892 (77.23) | 3513 (55.36) | 5930 (51.94) | 1939 (35.60) | 188 (18.50) | <0.001 |
| Ex-smoker | 906 (10.15) | 1619 (25.51) | 2528 (22.14) | 1527 (27.93) | 248 (24.41) | |
| Current smoker | 1126 (12.62) | 1214 (19.13) | 2960 (25.92) | 2001 (36.60) | 580 (57.09) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno-Llamas, A.; De la Cruz-Sánchez, E. Moderate Beer Consumption Is Associated with Good Physical and Mental Health Status and Increased Social Support. Nutrients 2023, 15, 1519. https://doi.org/10.3390/nu15061519
Moreno-Llamas A, De la Cruz-Sánchez E. Moderate Beer Consumption Is Associated with Good Physical and Mental Health Status and Increased Social Support. Nutrients. 2023; 15(6):1519. https://doi.org/10.3390/nu15061519
Chicago/Turabian StyleMoreno-Llamas, Antonio, and Ernesto De la Cruz-Sánchez. 2023. "Moderate Beer Consumption Is Associated with Good Physical and Mental Health Status and Increased Social Support" Nutrients 15, no. 6: 1519. https://doi.org/10.3390/nu15061519