

An Assessment of Mushroom Consumption on Cardiometabolic Disease Risk Factors and Morbidities in Humans: A Systematic Review
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Experimental Design
2.2. Inclusion and Exclusion Criteria
2.3. Search Strategy and Article Screening
2.4. Quality Assessment
2.5. Effect Measures, Calculations, and Synthesis Methods
3. Results
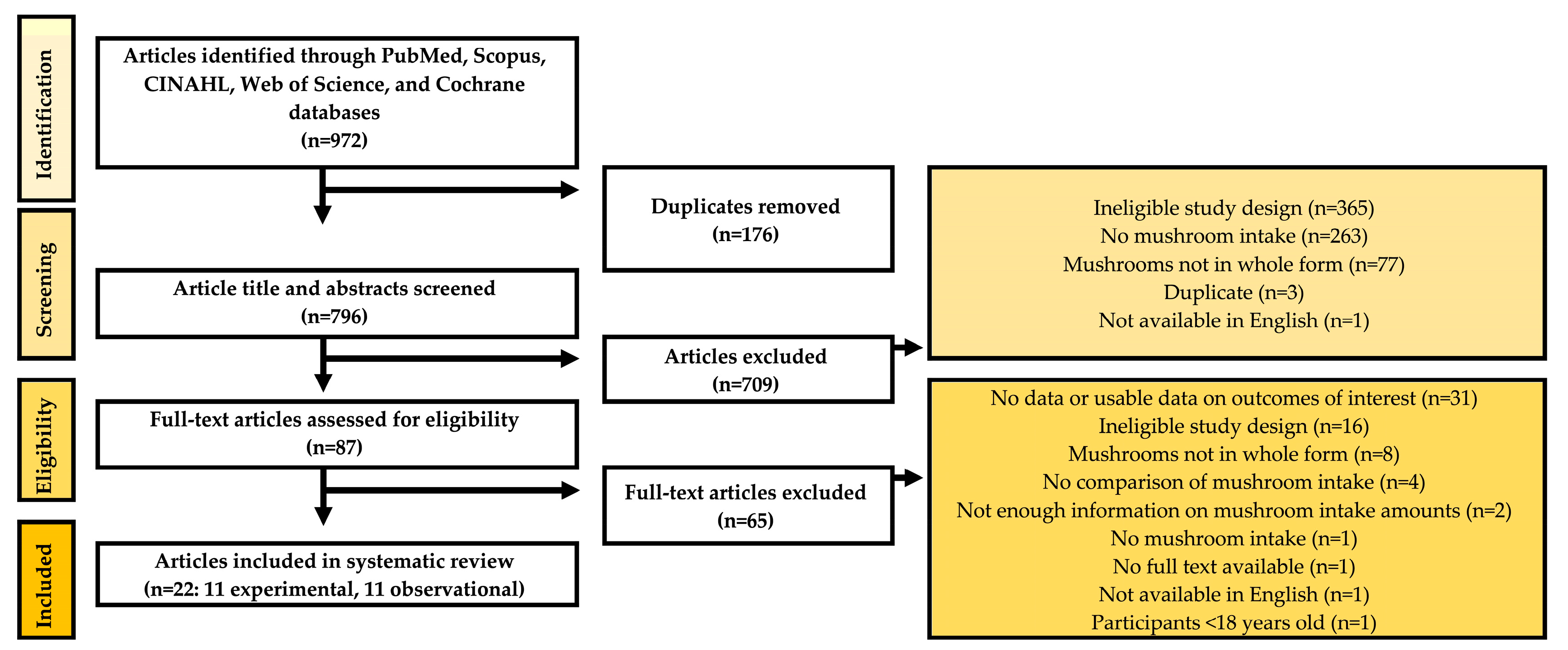
3.1. Search Results
3.2. Article Characteristics
3.3. Quality Assessment
3.4. Effects of Mushroom Consumption on Cardiometabolic Disease Risk Factors
4. Systolic and Diastolic Blood Pressures
5. Blood Lipids—Total Cholesterol, HDL Cholesterol, LDL Cholesterol, and Triglycerides
5.1. Total Cholesterol
5.2. HDL Cholesterol
5.3. LDL Cholesterol
5.4. Triglycerides
6. Glucose Control—Fasting Plasma Glucose and HbA1c
6.1. Fasting Plasma Glucose
6.2. HbA1c
7. Markers of Inflammation—hs-CRP
Associations between Mushroom Consumption and Morbidity/Mortality Related to Cardiovascular Disease or Type 2 Diabetes Mellitus
8. CVD-Related Morbidities and Mortality
8.1. Cardiovascular Disease
8.2. Cerebrovascular Disease
8.3. Coronary Heart Disease
8.4. Stroke
9. T2DM-Related Morbidities and Mortality
9.1. Hyperglycemia
9.2. Elevated HbA1c
9.3. Type 2 Diabetes Mellitus (T2DM)
10. Secondary Outcomes
10.1. Very-Low-Density Lipoprotein (VLDL) Cholesterol
10.2. Apolipoprotein A
10.3. Apolipoprotein B
10.4. Lipoprotein Particle Size
10.5. Fasting Insulin
10.6. C-Peptide
10.7. Postprandial Glucose
10.8. Homeostatic Model Assessment (HOMA)
11. Discussion
12. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- U.S. Department of Agriculture (USDA) Agricultural Research Service. FoodData Central: Foundation Foods. White Button Mushrooms. Available online: https://fdc.nal.usda.gov/ (accessed on 31 July 2022).
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th Edition. December 2020. Available online: http://www.dietaryguidelines.gov/ (accessed on 8 May 2022).
- Cerletti, C.; Esposito, S.; Iacoviello, L. Edible Mushrooms and Beta-Glucans: Impact on Human Health. Nutrients 2021, 13, 2195. [Google Scholar] [CrossRef] [PubMed]
- Kalač, P. Chapter 4: Health-Stimulating Compounds and Effects; Leme, M.K., Garcia, A.C.A., Eds.; Elsevier: Amsterdam, The Netherlands; Academic Press: London Wall, UK, 2016; ISBN 9780128044551. [Google Scholar]
- Kalaras, M.D.; Richie, J.P.; Calcagnotto, A.; Beelman, R.B. Mushrooms: A Rich Source of the Antioxidants Ergothioneine and Glutathione. Food Chem. 2017, 233, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.H.; Nagasaka, R.; Ohshima, T. Chapter 12: The Natural Antioxidant Ergothioneine: Resources, Chemical Characterization, and Applications; Logan, A., Nienaber, U., Pan, X., Eds.; AOCS Press: Urbana, IL, USA, 2013; ISBN 978-0-9830791-6-3. [Google Scholar]
- Cheah, I.K.; Halliwell, B. Ergothioneine; Antioxidant Potential, Physiological Function and Role in Disease. Biochim. Biophys. Acta Mol. Basis Dis. 2012, 1822, 784–793. [Google Scholar] [CrossRef] [Green Version]
- Halliwell, B.; Cheah, I.K.; Tang, R.M.Y. Ergothioneine—A Diet-Derived Antioxidant with Therapeutic Potential. FEBS Lett. 2018, 592, 3357–3366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beelman, R.B.; Kalaras, M.D.; Richie, J.P. Micronutrients and Bioactive Compounds in Mushrooms: A Recipe for Healthy Aging? Nutr. Today 2019, 54, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Beelman, R.B.; Kalaris, M.D.; Phillips, A.T.; Richie, J.P., Jr. Is Ergothioneine a ‘Longevity Vitamin’ Limited in the American Diet? J. Nutr. Sci. 2020, 9, e52. [Google Scholar] [CrossRef]
- Kalaras, M.D.; Beelman, R.B.; Holick, M.F.; Elias, R.J. Generation of Potentially Bioactive Ergosterol-Derived Products Following Pulsed Ultraviolet Light Exposure of Mushrooms (Agaricus Bisporus). Food Chem. 2012, 135, 396–401. [Google Scholar] [CrossRef]
- Tiwari, A.; Singh, G.; Singh, U.; Sapra, L.; Rana, V.; Sharma, V.; Srivastava, R.K.; Sharma, S. Edible Mushrooms: The Potential Game Changer in Alleviating Vitamin D Deficiency and Improving Human Health. Int. J. Food Sci. Technol. 2022, 57, 1367–1377. [Google Scholar] [CrossRef]
- You, S.W.; Hoskin, R.T.; Komarnytsky, S.; Moncada, M. Mushrooms as Functional and Nutritious Food Ingredients for Multiple Applications. ACS Food Sci. Technol. 2022, 2, 1184–1195. [Google Scholar] [CrossRef]
- Badalyan, S.M.; Barkhudaryan, A.; Rapior, S. The Cardioprotective Properties of Agaricomycetes Mushrooms Growing in the Territory of Armenia: Review. Int. J. Med. Mushrooms 2021, 23, 21–31. [Google Scholar] [CrossRef]
- Chaturvedi, V.K.; Agarwal, S.; Gupta, K.K.; Ramteke, P.W.; Singh, M.P. Medicinal Mushroom: Boon for Therapeutic Applications. 3 Biotech 2018, 8, 334. [Google Scholar] [CrossRef] [PubMed]
- Tran, H.; Yamamoto, A.; Matsumoto, S.; Ito, H.; Igami, K.; Miyazaki, T.; Kondo, R.; Shimizu, K. Hypotensive Effects and Angiotensin-Converting Enzyme Inhibitory Peptides of Reishi (Ganoderma lingzhi) Auto-Digested Extract. Molecules 2014, 19, 13473–13485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibadallah, B.X.; Abdullah, N.; Shuib, A.S. Identification of Angiotensin-Converting Enzyme Inhibitory Proteins from Mycelium of Pleurotus Pulmonarius (Oyster Mushroom). Planta Med. J. Med. Plant Nat. Prod. Res. 2015, 81, 123–129. [Google Scholar] [CrossRef]
- Martin, K.R. The Bioactive Agent Ergothioneine, a Key Component of Dietary Mushrooms, Inhibits Monocyte Binding to Endothelial Cells Characteristic of Early Cardiovascular Disease. J. Med. Food 2010, 13, 1340–1346. [Google Scholar] [CrossRef] [PubMed]
- Blumfield, M.; Abbott, K.; Duve, E.; Cassettari, T.; Marshall, S.; Fayet-Moore, F. Examining the Health Effects and Bioactive Components in Agaricus Bisporus Mushrooms: A Scoping Review. J. Nutr. Biochem. 2020, 84, 108453. [Google Scholar] [CrossRef]
- Dicks, L.; Ellinger, S. Effect of the Intake of Oyster Mushrooms (Pleurotus ostreatus) on Cardiometabolic Parameters—A Systematic Review of Clinical Trials. Nutrients 2020, 12, 1134. [Google Scholar] [CrossRef] [Green Version]
- Krittanawong, C.; Isath, A.; Hahn, J.; Wang, Z.; Fogg, S.E.; Bandyopadhyay, D.; Jneid, H.; Virani, S.S.; Tang, W.H.W. Mushroom Consumption and Cardiovascular Health: A Systematic Review. Am. J. Med. 2021, 134, 637–642. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- National Heart, Lung, and Blood Institute (NHLBI) Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 8 May 2022).
- EM, H.; LH, H.; Bougatsos, C. Screening for Lipid Disorders in Children and Adolescents Appendix 2. Units of Measure Conversion Formulas; Evidence, S., Ed.; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2007. [Google Scholar]
- Agrawal, R.P.; Chopra, A.; Lavekar, G.S.; Padhi, M.M.; Srikanth, N.; Ota, S.; Jain, S. Effect of Oyster Mushroom on Glycemia, Lipid Profile and Quality of Life in Type 2 Diabetic Patients. Aust. J. Med. Herbal. 2010, 22, 50–54. [Google Scholar]
- Dai, X.; Stanilka, J.M.; Rowe, C.A.; Esteves, E.A.; Nieves, C.; Spaiser, S.J.; Christman, M.C.; Langkamp-Henken, B.; Percival, S.S.; Nieves, C.J. Consuming Lentinula Edodes (Shiitake) Mushrooms Daily Improves Human Immunity: A Randomized Dietary Intervention in Healthy Young Adults. J. Am. Coll. Nutr. 2015, 34, 478–487. [Google Scholar] [CrossRef]
- Jayasuriya, W.J.A.B.N.; Wanigatunge, C.A.; Fernando, G.H.; Abeytunga, D.T.U.; Suresh, T.S. Hypoglycaemic Activity of Culinary Pleurotus Ostreatus and P. Cystidiosus Mushrooms in Healthy Volunteers and Type 2 Diabetic Patients on Diet Control and the Possible Mechanisms of Action. Phytother. Res. 2015, 29, 303–309. [Google Scholar] [CrossRef]
- Maruyama, C.; Shijo, Y.; Kameyama, N.; Umezawa, A.; Sato, A.; Nishitani, A.; Ayaori, M.; Ikewaki, K.; Waki, M.; Teramoto, T. Effects of Nutrition Education Program for the Japan Diet on Serum Ldl-Cholesterol Concentration in Patients with Dyslipidemia: A Randomized Controlled Trial. J. Atheroscler. Thromb. 2021, 28, 1035–1051. [Google Scholar] [CrossRef] [PubMed]
- Poddar, K.H.; Ames, M.; Hsin-Jen, C.; Feeney, M.J.; Wang, Y.; Cheskin, L.J. Positive Effect of Mushrooms Substituted for Meat on Body Weight, Body Composition, and Health Parameters. A 1-Year Randomized Clinical Trial. Appetite 2013, 71, 379–387. [Google Scholar] [CrossRef]
- Schneider, I.; Kressel, G.; Meyer, A.; Krings, U.; Berger, R.G.; Hahn, A. Lipid Lowering Effects of Oyster Mushroom (Pleurotus ostreatus) in Humans. J. Funct. Foods 2011, 3, 17–24. [Google Scholar] [CrossRef]
- Spim, S.R.V.; Pistila, A.M.H.; Pickler, T.B.; Silva, M.T.; Grotto, D. Effects of Shiitake Culinary-Medicinal Mushroom, Lentinus Edodes (Agaricomycetes), Bars on Lipid and Antioxidant Profiles in Individuals with Borderline High Cholesterol: A Double-Blind Randomized Clinical Trial. Int. J. Med. Mushrooms 2021, 23, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Niu, Z. A Mushroom Diet Reduced the Risk of Pregnancy-Induced Hypertension and Macrosomia: A Randomized Clinical Trial. Food Nutr. Res. 2020, 64, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Abrams, D.I.; Couey, P.; Shade, S.B.; Kelly, M.E.; Kamanu-Elias, N.; Stamets, P. Antihyperlipidemic Effects of Pleurotus ostreatus (oyster mushrooms) in HIV-Infected Individuals Taking Antiretroviral Therapy. BMC Complement. Altern. Med. 2011, 11, 60. [Google Scholar] [CrossRef] [Green Version]
- Harada, E.; Morizono, T.; Sumiya, T.; Kawagishi, H. Effect of the Medicinal Mushroom, Grifola Gargal (Agaricomycetes), on Bone Turnover Markers and Serum Lipids in Middle-Aged and Elderly Japanese Women. Int. J. Med. Mushrooms 2016, 18, 1–7. [Google Scholar] [CrossRef]
- Mehrotra, A.; Calvo, M.S.; Beelman, R.B.; Levy, E.; Siuty, J.; Kalaras, M.D.; Uribarri, J. Bioavailability of Vitamin D2 from Enriched Mushrooms in Prediabetic Adults: A Randomized Controlled Trial. Eur. J. Clin. Nutr. 2014, 68, 1154–1160. [Google Scholar] [CrossRef] [Green Version]
- Ba, D.M.; Gao, X.; Muscat, J.; Al-Shaar, L.; Chinchilli, V.; Zhang, X.; Ssentongo, P.; Beelman, R.B.; Richie, J.P., Jr. Association of Mushroom Consumption with All-Cause and Cause-Specific Mortality among American Adults: Prospective Cohort Study Findings from NHANES III. Nutr. J. 2021, 20, 38. [Google Scholar] [CrossRef]
- Lee, D.H.; Yang, M.; Giovannucci, E.L.; Sun, Q.; Chavarro, J.E. Mushroom Consumption, Biomarkers, and Risk of Cardiovascular Disease and Type 2 Diabetes: A Prospective Cohort Study of US Women and Men. Am. J. Clin. Nutr. 2019, 110, 666–674. [Google Scholar] [CrossRef]
- Lee, K.W.; Woo, H.D.; Cho, M.J.; Park, J.K.; Kim, S.S. Identification of Dietary Patterns Associated with Incidence of Hyperglycemia in Middle-Aged and Older Korean Adults. Nutrients 2019, 11, 1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanri, A.; Mizoue, T.; Shimazu, T.; Ishihara, J.; Takachi, R.; Noda, M.; Iso, H.; Sasazuki, S.; Sawada, N.; Tsugane, S. Dietary Patterns and All-Cause, Cancer, and Cardiovascular Disease Mortality in Japanese Men and Women: The Japan Public Health Center-Based Prospective Study. PLoS ONE 2017, 12, e0174848. [Google Scholar] [CrossRef] [Green Version]
- Htun, N.C.; Suga, H.; Imai, S.; Shimizu, W.; Ishikawa-Takata, K.; Takimoto, H. Dietary Pattern and Its Association with Blood Pressure and Blood Lipid Profiles among Japanese Adults in the 2012 Japan National Health and Nutrition Survey. Asia Pac. J. Clin. Nutr. 2018, 27, 1048–1061. [Google Scholar] [CrossRef] [PubMed]
- Meneses, M.E.; Galicia-Castillo, M.; Pérez-Herrera, A.; Martínez, R.; León, H.; Martínez-Carrera, D. Traditional Mushroom Consumption Associated to Lower Levels of Triglycerides and Blood Pressure in an Indigenous Peasant Community from Oaxaca, Mexico. Int. J. Med. Mushrooms 2020, 22, 953–966. [Google Scholar] [CrossRef] [PubMed]
- Okada, E.; Takahashi, K.; Nakamura, K.; Ukawa, S.; Takabayashi, S.; Nakamura, M.; Sasaki, S.; Tamakoshi, A.; Takimoto, H. Dietary Patterns and Abnormal Glucose Tolerance among Japanese: Findings from the National Health and Nutrition Survey, 2012. Public Health Nutr. 2019, 22, 2460–2468. [Google Scholar] [CrossRef]
- Osonoi, Y.; Mita, T.; Osonoi, T.; Saito, M.; Tamasawa, A.; Nakayama, S.; Someya, Y.; Ishida, H.; Kanazawa, A.; Gosho, M.; et al. Relationship between Dietary Patterns and Risk Factors for Cardiovascular Disease in Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study. Nutr. J. 2016, 15, 15. [Google Scholar] [CrossRef] [Green Version]
- Pounis, G.; Costanzo, S.; Persichillo, M.; de Curtis, A.; Sieri, S.; Vinceti, M.; Zito, F.; di Castelnuovo, A.F.; Donati, M.B.; de Gaetano, G.; et al. Mushroom and Dietary Selenium Intakes in Relation to Fasting Glucose Levels in a Free-Living Italian Adult Population: The Moli-Sani Project. Diabetes Metab. 2014, 40, 34–42. [Google Scholar] [CrossRef]
- Uchiyama, M.; Maruyama, C.; Umezawa, A.; Kameyama, N.; Sato, A.; Kamoshita, K.; Komine, S.; Hasegawa, S. A Cross-Sectional Pilot Study on Food Intake Patterns Identified from Very Short FFQ and Metabolic Factors Including Liver Function in Healthy Japanese Adults. Nutrients 2022, 14, 2442. [Google Scholar] [CrossRef]
- Weikert, C.; Hoffmann, K.; Dierkes, J.; Zyriax, B.-C.; Klipstein-Grobusch, K.; Schulze, M.B.; Jung, R.; Windler, E.; Boeing, H. A Homocysteine Metabolism-Related Dietary Pattern and the Risk of Coronary Heart Disease in Two Independent German Study Populations. J. Nutr. 2005, 135, 1981–1988. [Google Scholar] [CrossRef] [Green Version]
- Kumar, K.; Mehra, R.; Guiné, R.P.F.; Lima, M.J.; Kumar, N.; Kaushik, R.; Ahmed, N.; Yadav, A.N.; Kumar, H. Edible Mushrooms: A Comprehensive Review on Bioactive Compounds with Health Benefits and Processing Aspects. Foods 2021, 10, 2996. [Google Scholar] [CrossRef] [PubMed]
- Cheah, I.K.; Halliwell, B. Ergothioneine, Recent Developments. Redox Biol. 2021, 42, 101868. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Description |
|---|---|
| Population | Adult humans (Age ≥ 18 y) |
| Intervention | Groups consuming mushrooms or statistically significantly higher amounts of mushrooms |
| Comparison | Groups not consuming mushrooms or groups consuming statistically significantly lower amounts of mushrooms |
| Outcomes | Cardiometabolic disease risk factors and morbidities. Primary: diastolic and systolic blood pressures, blood lipids (total cholesterol, HDL cholesterol, LDL cholesterol, triglycerides), fasting plasma glucose, HbA1c, hs-CRP, and morbidity/mortality related to cardiovascular diseases or type 2 diabetes mellitus Secondary: other lipoproteins (VLDL, apolipoprotein A, apolipoprotein B), lipoprotein particle size, fasting insulin, C-peptide, postprandial glucose |
| Study Design | Peer-reviewed randomized controlled trials and observational studies |
| Research Question | In adults, what is the effect of mushroom consumption on cardiometabolic disease risk factors and morbidities compared to those not consuming mushrooms? |
| Source | Search Terms | Results |
|---|---|---|
| PubMed | (Mushroom * OR Agaricales [MeSH Terms] OR Shiitake Mushrooms [MeSH Terms] OR Pleurotus [MeSH Terms] OR Grifola [MeSH Terms]) AND (blood pressure OR blood pressure [MeSH Terms] OR triglycerides OR triglycerides [MeSH Terms] OR Cholesterol OR Epicholesterol OR cholesterol [MeSH Terms] OR cholesterol, LDL [MeSH Terms] OR LDL Cholesterol OR Low Density Lipoprotein Cholesterol OR cholesterol, HDL [MeSH Terms] OR High-Density Lipoprotein Cholesterol OR HDL Cholesterol OR blood glucose OR blood glucose [MeSH Terms] OR blood sugar OR diabetes OR Diabetes Mellitus [MeSH Terms] OR hba1c OR Glycated Hemoglobin A OR Glycated Hemoglobin A [MeSH Terms] OR hs-CRP OR High Sensitivity C-Reactive Protein OR C-Reactive Protein [MeSH Terms] OR CRP OR cardiovascular diseases [MeSH Terms] OR cardiovascular disease * or heart disease * OR vascular disease * OR “diabetes mellitus, type 2” [MeSH Terms] OR diabetes type 2 OR type 2 diabetes) AND (Humans [MeSH Terms]) | 570 |
| CINAHL | (Mushroom * OR Agaricales OR Shiitake Mushrooms OR Pleurotus OR Grifola) AND (blood pressure OR triglycerides OR Cholesterol OR Epicholesterol OR LDL Cholesterol OR Low Density Lipoprotein Cholesterol OR High-Density Lipoprotein Cholesterol OR HDL Cholesterol OR blood glucose OR blood sugar OR diabetes OR Diabetes Mellitus OR hba1c OR Glycated Hemoglobin A OR hs-CRP OR High Sensitivity C-Reactive Protein OR CRP OR type 2 diabetes OR cardiovascular disease) AND (Humans) | 76 |
| Scopus | Mushroom * AND (“blood pressure” OR Cholesterol OR “blood glucose” OR “blood sugar” OR diabetes OR “Diabetes Mellitus” OR “type 2 diabetes” OR “cardiovascular disease”) AND Humans | 69 |
| Web of Science | (Mushroom * OR Agaricales OR Shiitake Mushrooms OR Pleurotus OR Grifola) AND (blood pressure OR triglycerides OR Cholesterol OR Epicholesterol OR LDL Cholesterol OR Low Density Lipoprotein Cholesterol OR High-Density Lipoprotein Cholesterol OR HDL Cholesterol OR blood glucose OR blood sugar OR diabetes OR Diabetes Mellitus OR hba1c OR Glycated Hemoglobin A OR hs-CRP OR High Sensitivity C-Reactive Protein OR CRP OR type 2 diabetes OR cardiovascular disease) AND (Humans) | 256 |
| Cochrane Library | (Mushroom * OR Agaricales OR Shiitake Mushrooms OR Pleurotus OR Grifola) AND (blood pressure OR triglycerides OR Cholesterol OR blood glucose OR diabetes OR Glycated hemoglobin A OR C-Reactive Protein OR type 2 diabetes OR cardiovascular disease) | 1 |
| Author, Year | Study Type and Design | Length of Study Intervention or Follow-Up | Dietary Description | Mushroom Type | Mushroom Form | Mushroom Amount and Frequency | Sample Size | Region | Healthy or Diseased | Age (Years) † | BMI (kg/m2) † |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Abrams et al., 2011 [33] | Exp, Single-arm | 8 weeks | Partial feed | Pleurotus ostreatus | Dried | 15 g daily | 20 | USA | HIV | 36–60 | NR |
| Agrawal et al., 2010 [25] | RCT, Parallel | 3 months | Partial feed | Pleurotus spp. | NR | NR | 111 | India | T2DM | 51.1 ± 8.3 * | 26.67 ± 4.5 * |
| Dai et al., 2015 [26] | RCT, Parallel | 4 weeks | Partial feed | Lentinula edodes | Dried | 5 or 10 g daily | 52 | USA | Healthy | 21–41 * | M: 23.3 ± 7.2 * F: 22.4 ± 8.8 * |
| Harada et al., 2016 [34] | Exp, Single-arm | 2 weeks | Partial feed | Grifola gargal | Dried | 5 g daily | 17 | Japan | NR | 61.2 ± 7.6 | NR |
| Jayasuriya et al., 2015 [27] | RCT, Parallel | 2 weeks | Partial feed | P. ostreatus and P. cystidiousus | Dried | 50 mg/kg BW daily | 88 | Sri Lanka | Healthy | NR | NR |
| Maruyama et al., 2021 [28] | RCT, Parallel | 6 months | Partial feed | NR | NR | 40 ± 33 g daily | 98 | Japan | Dys-lipidemia, T2DM, HTN | 53.5 ± 8.2 * | 24.4 ± 3.7 * |
| Mehrotra et al., 2014 [35] | RCT, Parallel (pre vs. post) | 16 weeks | Partial feed | NR | Fresh | 100 g daily | 36 | USA | Pre-diabetic | 49 ± 12 | NR |
| Poddar et al., 2013 [29] | RCT, Parallel | 12 months | Partial feed | Agaricus bisporus | Fresh | 8 oz, 3x/week | 73 | USA | Healthy | 48.4 ± 12 | 25–40 |
| Schneider et al., 2011 [30] | RCT, Parallel | 21 days | Partial feed | Pleurotus ostreatus | Dried | 30 g daily | 20 | Germany | Hyper-lipidemia | 20–34 | 22.7 ± 3.7 * |
| Spim et al., 2021 [31] | RCT, Parallel | 66 days | Partial feed | Lentinula edodes | Dried | 3.5 g daily | 68 | Brazil | Dys-lipidemia | 40 ± 11 | 26.9 ± 4.4 |
| Sun and Niu, 2020 [32] | RCT, Parallel | Pre-pregnancy-20th week gestation | Partial feed | Agaricus bisporus | Fresh | 100 g daily | 1162 | China | Healthy, pregnant | 31.2 ± 4.5 * | 22.47 ± 3.66 * |
| Ba et al., 2021 [36] | OBS, Pro-spective | 19.5 ± 7.4-year follow-up | NR | NR | NR | 10–72 g daily | 15,546 | USA | NR | 44.3 ± 0.5 | NR; ~45% with BMI <24.9 |
| Htun et al., 2018 [40] | OBS. Cross-sectional | NA | Traditional Japanese | NR | NR | NR; loading factor 0.35 | 8721 | Japan | NR | 40–74 | M: 24.3 ± 3.0 * F: 23.1 ± 3.4 * |
| Lee DH et al., 2019 [37] | OBS, Pro-spective | 26 year follow-up | Prudent | NR | Fresh, cooked, canned | 5 servings per week | 110,680 | USA | Healthy | M: 53.2 ± 9.2 * F: 52.3 ± 6.9 * | M: 25.7 ± 3.6 * F: 25.2 ± 4.6 * |
| Lee KW et al., 2019 [38] | OBS, Pro-spective | 4.9 year follow-up | Prudent | NR | NR | NR; loading factor 0.55 (M), 0.56 (F) | 55,457 | Korea | Healthy | 40–79 | M: 24.5 ± 2.6 F: 23.6 ± 2.8 |
| Meneses et al., 2020 [41] | OBS, Cross-sectional | NA | Traditional Oaxaca Foods | Wild and cultivated mushrooms | Fresh, cooked | 260 g daily | 45 | Mexico | Dys-lipidemia | 48.27 ± 14.08 | 28.69 ± 4.56 |
| Nanri et al., 2017 [39] | OBS, Pro-spective | 5- and 10-year follow-up | Prudent | NR | NR | 5–16 g daily | 81,720 | Japan | Healthy | 40–69 | 23.5 ± 0.2 |
| Okada et al., 2019 [42] | OBS, Cross-sectional | NA | Vegetable | NR | NR | 6.47 ± 12.7 to 40.3 ± 45.8 g daily | 9550 | Japan | Healthy | 64.4 ± 10.8 * | 23.2 ± 3.3 * |
| Osonoi et al., 2016 [43] | OBS, Cross- sectional | NA | Seaweed, veg, soy, mushrooms | NR | NR | NR; loading factor 0.55 | 726 | Japan | T2DM | 57.8 ± 8.6 | 24.6 ± 4.1 |
| Pounis et al., 2013 [44] | OBS, Cross-sectional | NA | Grains, nuts/ seeds, legumes, poultry, fish | NR | NR | <14, 14–28, or >28 g/week | 13,770 | Italy | Healthy | 53.1 ± 11.0 | NR; Obesity prevalence 25.2–28.8% |
| Uchiyama et al., 2022 [45] | OBS, Cross-sectional | NA | Traditional Japanese | NR | NR | 0.20 (0.18–0.40) to 0.40 (0.20-0.80) • | 198 | Japan | Healthy | 37 (28–44) ‡ | 21.2 (19.8–23) ‡ |
| Weikert et al., 2005 [46] | OBS, Case-control (CORA) | NA | Whole-grain bread, fresh fruit, olive oil, mushrooms, cruciferous vegetables, wine, and nuts | NR | NR | 1.0–4.0 g daily | 455 | Germany | Coronary Heart Disease | 30–80 | 26.1 ± 4.8 (case) 25.6 ± 4.3 (con) |
| OBS, Pro-spective (EPIC) | 4.6 year follow-up | NR | NR | 1.0–3.5 g daily | 26,795 | Healthy | 35–65 | 27.5 ± 3.8 (case) 26.3 ± 4.4 (con) |
| Parameter | Experimental Research | Observational Research | ||||||
|---|---|---|---|---|---|---|---|---|
| IMPACT † | IMPACT | |||||||
| Total # of Articles | + | − | Total # of Articles | + | − | |||
| Systolic Blood Pressure | 5 | 40 (2) * | 60 (3) | 0 (0) | 5 | 40 (2) # | 60 (3) | 0 (0) |
| Diastolic Blood Pressure | 5 | 40 (2) * | 60 (3) | 0 (0) | 5 | 60 (3) # | 40 (2) | 0 (0) |
| Total Cholesterol | 7 | 29 (2) | 71 (5) | 0 (0) | 6 | 0 (0) | 100 (6) # | 0 (0) |
| HDL Cholesterol | 8 | 25 (2) | 75 (6) | 0 (0) | 4 | 50 (2) | 50 (2) | 20 (1) |
| LDL Cholesterol | 7 | 29 (2) | 71 (5) | 0 (0) | 3 | 33 (1) | 67 (2) | 0 (0) |
| Triglycerides | 7 | 86 (6) | 0 (0) | 14 (1) | 5 | 40 (2) | 60 (3) # | 0 (0) |
| Glucose | 7 | 57 (4) * | 43 (3) | 0 (0) | 3 | 0 (0) | 100 (3) | 0 (0) |
| HbA1c | 3 | 33 (1) | 67 (2) | 0 (0) | 1 | 0 (0) | 100 (1) | 0 (0) |
| hs-CRP | 3 | 67 (2) | 33 (1) | 0 (0) | 1 | 0 (0) | 100 (1) | 0 (0) |
| Author, Year | Diet Group | Comparator | Mushroom Species and Form | Sys-BP† | Dia-BP | TC | HDL | LDL | TAG | Glu | HbA1c | hs-CRP |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abrams et al., 2011 [33] | Post, 15 g daily | Baseline | Pleurotus ostreatus, dried | NR | NR | ≠ | ≠ | ≠ | ↓ | ≠ | NR | NR |
| Agrawal et al., 2010 [25] | Mushroom biscuits | Baseline | Pleurotus spp., NR | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | ↓ | ↓ | NR |
| Mushroom biscuits | Ajwain biscuits | Pleurotus spp., NR | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | ↓ | ↓ | NR | |
| Dai et al., 2015 [26] | 5 g and 10 g/daily • | Baseline | Letinula edodes, dried | NR | NR | NR | NR | NR | NR | NR | NR | ↓ |
| Harada et al., 2016 [34] | Post, 5 g/daily | Baseline | Grifola gargal, dried | ≠ | ≠ | ≠ | ≠ | ≠ | NR | NR | NR | NR |
| Jayasuriya et al., 2015 [27] | P. ostreatus, 50 mg/kg/bw daily | Control (water) | Pleurotus ostreatus, dried | NR | NR | NR | NR | NR | NR | ↓ | NR | NR |
| P. cystidiousus, 50 mg/kg/bw daily | Control (water) | Pleurotus cystidiousus, dried | NR | NR | NR | NR | NR | NR | ↓ | NR | NR | |
| Maruyama et al., 2021 [28] | Japanese Diet, 40 ± 33 g/d at 6 months | Partial Japanese Diet, 31 ± 27 g/d at 6 months | NR | ≠ | ≠ | ↓ | ≠ | ↓ | ↓ | ≠ | ≠ | ≠ |
| Mehrotra et al., 2014 [35] | Ultraviolet treated mushrooms (500 IU D2/day) + placebo, 100 g/daily | Baseline | NR, fresh | NR | NR | NR | ≠ | NR | ↑ | NR | ≠ | NR |
| Ultraviolet treated mushrooms (2600 IU D2/day) + placebo, 100 g/daily | Baseline | NR, fresh | NR | NR | NR | ≠ | NR | ≠ | NR | ≠ | NR | |
| Untreated mushrooms + 1200 IU D3/day capsules, 100 g/daily | Baseline | NR, fresh | NR | NR | NR | ≠ | NR | ≠ | NR | ≠ | NR | |
| Untreated mushrooms + 7300 IU D3/day capsules, 100 g/daily | Baseline | NR, fresh | NR | NR | NR | ≠ | NR | ≠ | NR | ≠ | NR | |
| Poddar et al., 2013 ¶ [29] | Mushroom diet, 8 oz on 3 d/wk, 0–6 months WL | Meat diet, 90% lean ground beef 3 d/wk, 0–6 months WL | Agaricus bisporus, fresh | ≠ | ≠ | ≠ | NR | ≠ | NR | NR | NR | ↓ |
| Mushroom diet, 8oz on 3 d/wk, 6–12 months WM | Meat diet, 90% lean ground beef 3 d/wk, 6–12 months WM | Agaricus bisporus, fresh | NR | NR | ≠ | NR | ≠ | NR | NR | NR | NR | |
| Mushroom diet, 8oz on 3 d/wk, 0–6 months WL | Baseline | Agaricus bisporus, fresh | NR | NR | NR | ≠ | NR | ↓ | ↓ | NR | NR | |
| Mushroom diet, 8 oz on 3 d/wk, 12 months | Baseline | Agaricus bisporus, fresh | NR | NR | NR | ↓ | NR | ↓ | ≠ | NR | NR | |
| Schneider et al., 2011 [30] | Verum diet, 30 g/d | Baseline | Pleurotus ostreatus, freeze-dried | NR | NR | ≠ | ≠ | ≠ | ↓ | NR | NR | NR |
| Spim et al., 2021 [31] | Intervention group, 3.5 g/d | Placebo group | Letinula edodes, dried | NR | NR | ≠ | ≠ | ≠ | ↓ | ≠ | NR | NR |
| Sun and Niu, 2020 § [32] | MD group, 100 g/d | Placebo group | Agaricus bisporus, fresh | ↓ | ↓ | NR | NR | NR | NR | ↓ | NR | NR |
| Author, Year | Diet Group | Comparator | Mushroom Species and Form | Sys-BP | Dia-BP | TC | HDL | LDL | TAG | Glu | HbA1c | hs-CRP |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lee DH et al., 2019 * [37] | 5 servings/wk (pooled) | Never (pooled) | NS, fresh, cooked, canned | NR | NR | ≠ | ↑ | ≠ | ≠ | NR | NR | ≠ |
| Meneses et al., 2020 * [41] | High frequency, daily consumption | No consumption | Wild and cultivated mushrooms | ≠ | ↓ | ≠ | NR | NR | ↓ | ≠ | NR | NR |
| Pounis et al., 2013 *# [44] | Tertile 3, >28 g/wk | Tertile 1, <14 g/wk | NS | ↓ | ↓ | ≠ | NR | NR | ≠ | ≠ | NR | NR |
| Htun et al., 2018 [40] | Traditional Japanese, Q4 | Traditional Japanese Q1 | NS | ↓ | ↓ | ≠ | ≠ | ↓ | NR | NR | NR | NR |
| Osonoi et al., 2016 [43] | Seaweed, vegetable, soy products, and mushroom diet, Q5 | Seaweed, vegetable, soy products, and mushroom diet, Q1 | NS | ≠ | ≠ | ≠ | ≠ | NR | ≠ | ≠ | ≠ | NR |
| Uchiyama et al., 2022 [45] | Traditional Japanese T3, 0.40 (0.20–0.80) g ^ | Traditional Japanese T1, 0.20 (0.18–0.40) g ^ | NS | ≠ | ≠ | ≠ | ↑ | ≠ | ↓ | NR | NR | NR |
| Author, Year | Diet Group | Comparator | Mushroom Type (Fresh, Dried, Species) | CVD | Cerebrovascular Disease | CHD | Stroke | T2DM | Hyper-Glycemia | Elevated HbA1c |
|---|---|---|---|---|---|---|---|---|---|---|
| Ba et al., 2021 ^ [36] | Mushroom intake, 10–72 g/d | No mushroom intake | NR | HR: 0.82 (0.56, 1.21) | NR | NR | NR | HR: 0.32 (0.06, 1.65) | NR | NR |
| Lee DH et al., 2019 ^ [37] | 5 servings/wk, female | Never, female | NR, fresh, cooked, canned | HR: 1.08 (0.94, 1.25) | NR | HR: 1.09 (0.90, 1.32) | HR: 1.08 (0.86, 1.34) | HR: 1.04 (0.91, 1.19) | NR | NR |
| 5 servings/wk, male | Never, male | HR: 0.93 (0.78, 1.11) | NR | HR: 0.89 (0.72, 1.10) | HR: 1.04 (0.75, 1.43) | HR: 1.04 (0.83, 1.31) | NR | NR | ||
| 5 servings/wk, pooled | Never, pooled | HR: 1.02 (0.91, 1.14) | NR | HR: 1.00 (0.87, 1.16) | HR: 1.05 (0.87, 1.25) | HR: 1.04 (0.93, 1.16) | NR | NR | ||
| Pounis et al., 2013 ^ [44] | Tertile 3, male, >28 g/wk | Tertile 1 male, <14 g/wk | NR | NR | NR | NR | NR | OR: 1.27 (1.05, 1.55) * | NR | NR |
| Tertile 3, female, >28 g/wk | Tertile 1, female, <14 g/wk | NR | NR | NR | NR | NR | OR: 1.38 (1.05, 1.81) * | NR | NR | |
| Lee KW et al., 2019 [38] | Prudent Q5, male | Prudent Q1, male | NR | NR | NR | NR | NR | NR | HR: 0.93 (0.75, 1.15) | NR |
| Prudent Q5, female | Prudent Q1, female | NR | NR | NR | NR | NR | NR | HR: 0.75 (0.63, 0.89) * | NR | |
| Nanri et al., 2017 [39] | Prudent Q4, 16 g/d | Prudent Q1, 5 g/d | NR | HR: 0.72 (0.64, 0.79) * | HR: 0.63 (0.53, 0.75) * | HR: 0.75 (0.66, 0.87) * | NR | NR | NR | NR |
| Okada et al., 2019 [42] | Vegetable Q4, 40.3 ± 45.8 g/d | Vegetable Q1, 6.47 ± 12.7 g/d | NR | NR | NR | NR | NR | NR | NR | OR: 0.68 (0.49, 0.95) * |
| Weikert et al., 2005 [46] | CORA Q5, 4.0 ± 0.4 g/d | CORA Q1, 1.0 ± 0.1 g/d | NR | NR | NR | RR: 0.39 (0.17, 0.92) * | NR | NR | NR | NR |
| EPIC Q5, 3.5 ± 0.1 g/d | EPIC Q1, 1.0 ± 0.1 g/d | NR | NR | NR | RR: 0.72 (0.43, 1.20) | NR | NR | NR | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uffelman, C.N.; Chan, N.I.; Davis, E.M.; Wang, Y.; McGowan, B.S.; Campbell, W.W. An Assessment of Mushroom Consumption on Cardiometabolic Disease Risk Factors and Morbidities in Humans: A Systematic Review. Nutrients 2023, 15, 1079. https://doi.org/10.3390/nu15051079
Uffelman CN, Chan NI, Davis EM, Wang Y, McGowan BS, Campbell WW. An Assessment of Mushroom Consumption on Cardiometabolic Disease Risk Factors and Morbidities in Humans: A Systematic Review. Nutrients. 2023; 15(5):1079. https://doi.org/10.3390/nu15051079
Chicago/Turabian StyleUffelman, Cassi N., Nok In Chan, Eric M. Davis, Yu Wang, Bethany S. McGowan, and Wayne W. Campbell. 2023. "An Assessment of Mushroom Consumption on Cardiometabolic Disease Risk Factors and Morbidities in Humans: A Systematic Review" Nutrients 15, no. 5: 1079. https://doi.org/10.3390/nu15051079