
Controversial Impact of Vitamin D Supplementation on Reducing Insulin Resistance and Prevention of Type 2 Diabetes in Patients with Prediabetes: A Systematic Review
 , and
, and
Abstract
:1. Introduction
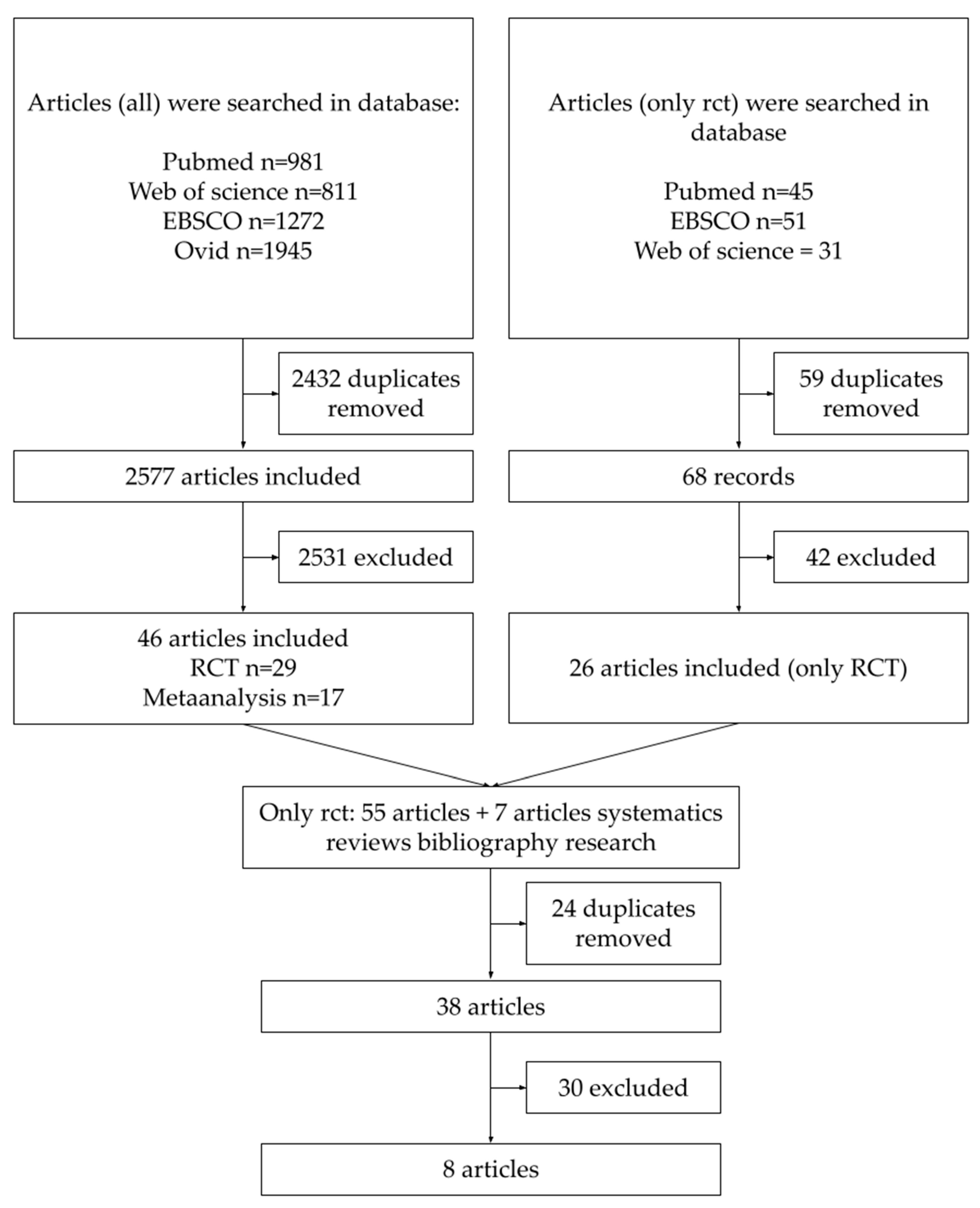
2. Materials and Methods
- participants with prediabetes, over 18 years of age, without other restrictions of age, sex, or ethnicity;
- vitamin D supplementation in the chemical forms of calciferol-D2 or cholecalciferol-D3 in any dose, administered with any frequency and with any time of follow up;
- primary outcome defined as the development of type 2 diabetes or its effect on insulin resistance;
- secondary outcomes included measurements of any conventional marker of glycemic control (fasting glucose, oral glucose tolerance test, insulin secretion, HOMA-IR index, glycated hemoglobin level) [31]
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-Year Trends of the Global Burden of Disease Attributable to Ambient Air Pollution: An Analysis of Data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokdad, A.H.; Forouzanfar, M.H.; Daoud, F.; Mokdad, A.A.; El Bcheraoui, C.; Moradi-Lakeh, M.; Kyu, H.H.; Barber, R.M.; Wagner, J.; Cercy, K.; et al. Global Burden of Diseases, Injuries, and Risk Factors for Young People’s Health during 1990-2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2016, 387, 2383–2401. [Google Scholar] [CrossRef] [PubMed]
- Lovic, D.; Piperidou, A.; Zografou, I.; Grassos, H.; Pittaras, A.; Manolis, A. The Growing Epidemic of Diabetes Mellitus. Curr. Vasc. Pharmacol. 2020, 18, 104–109. [Google Scholar] [CrossRef]
- Edwards, C.M.; Cusi, K. Prediabetes: A Worldwide Epidemic. Endocrinol. Metab. Clin. N. Am. 2016, 45, 751–764. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycaemia: Report of a WHO/IDF Consultation; WHO: Geneva, Switzerland, 2006.
- Diagnosis|ADA. Available online: https://diabetes.org/diabetes/a1c/diagnosis (accessed on 6 January 2023).
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A High-Risk State for Diabetes Development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, B.; Lu, Y.; Hajifathalian, K.; Bentham, J.; Di Cesare, M.; Danaei, G.; Bixby, H.; Cowan, M.J.; Ali, M.K.; Taddei, C.; et al. Worldwide Trends in Diabetes since 1980: A Pooled Analysis of 751 Population-Based Studies with 4.4 Million Participants. Lancet 2016, 387, 1513–1530. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, B.; Gulanick, M.; Lamendola, C. Risk Factors for Type 2 Diabetes Mellitus. J. Cardiovasc. Nurs. 2002, 16, 486. [Google Scholar] [CrossRef]
- Rawshani, A.; Rawshani, A.; Franzén, S.; Sattar, N.; Eliasson, B.; Svensson, A.-M.; Zethelius, B.; Miftaraj, M.; McGuire, D.K.; Rosengren, A.; et al. Risk Factors, Mortality, and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2018, 379, 633–644. [Google Scholar] [CrossRef]
- Brannick, B.; Dagogo-Jack, S. Prediabetes and Cardiovascular Disease: Pathophysiology and Interventions for Prevention and Risk Reduction. Endocrinol. Metab. Clin. N. Am. 2018, 47, 33. [Google Scholar] [CrossRef]
- Zand, A.; Ibrahim, K.; Patham, B. Prediabetes: Why Should We Care? Methodist Debakey Cardiovasc. J. 2018, 14, 289. [Google Scholar] [CrossRef]
- Galaviz, K.I.; Weber, M.B.; Suvada, K.; Gujral, U.P.; Wei, J.; Merchant, R.; Dharanendra, S.; Haw, J.S.; Narayan, K.M.V.; Ali, M.K. Interventions for Reversing Prediabetes: A Systematic Review and Meta-Analysis. Am. J. Prev. Med. 2022, 62, 614–625. [Google Scholar] [CrossRef]
- Heaney, R.P. Vitamin D: Role in the Calcium and Phosphorus Economies. Vitam. D Two-Volume Set 2011, 1–2, 607–624. [Google Scholar] [CrossRef]
- Holick, M.F.; Smith, E.; Pincus, S. Skin as the Site of Vitamin D Synthesis and Target Tissue for 1,25-Dihydroxyvitamin D3: Use of Calcitriol (1,25-Dihydroxyvitamin D3) for Treatment of Psoriasis. Arch. Dermatol. 1987, 123, 1677–1683a. [Google Scholar] [CrossRef]
- Lehmann, B.; Meurer, M. Extrarenal Sites of Calcitriol Synthesis: The Particular Role of the Skin. Recent Results Cancer Res. 2003, 164, 135–145. [Google Scholar] [CrossRef]
- WMA Statement on Vitamin D Insufficiency—WMA—The World Medical Association. Available online: https://www.wma.net/policies-post/wma-statement-on-vitamin-d-insufficiency/ (accessed on 3 February 2023).
- Del Valle, H.B.; Yaktine, A.L.; Taylor, C.L.; Ross, A.C. (Eds.) Dietary Reference Intakes for Calcium and Vitamin D; The National Academic Press: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D Deficiency 2.0: An Update on the Current Status Worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- Binkley, N.; Dawson-Hughes, B.; Durazo-Arvizu, R.; Thamm, M.; Tian, L.; Merkel, J.M.; Jones, J.C.; Carter, G.D.; Sempos, C.T. Vitamin D Measurement Standardization: The Way out of the Chaos. J. Steroid Biochem. Mol. Biol. 2017, 173, 117–121. [Google Scholar] [CrossRef]
- Schoenmakers, I.; Pettifor, J.M.; Peña-Rosas, J.P.; Lamberg-Allardt, C.; Shaw, N.; Jones, K.S.; Lips, P.; Glorieux, F.H.; Bouillon, R. Prevention and Consequences of Vitamin D Deficiency in Pregnant and Lactating Women and Children: A Symposium to Prioritise Vitamin D on the Global Agenda. J. Steroid Biochem. Mol. Biol. 2016, 164, 156–160. [Google Scholar] [CrossRef]
- Aguiar, M.; Atapattu, N.; Bhatia, V.; Braegger, C.; Butler, G.; Cassinelli, H.; DIMeglio, L.A.; Frew, E.; Fu, J.; Goldberg, G.; et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. J. Clin. Endocrinol. Metab. 2016, 101, 394–415. [Google Scholar] [CrossRef]
- Lips, P. Vitamin D Deficiency and Secondary Hyperparathyroidism in the Elderly: Consequences for Bone Loss and Fractures and Therapeutic Implications. Endocr. Rev. 2001, 22, 477–501. [Google Scholar] [CrossRef]
- Borges, M.C.; Martini, L.A.; Rogero, M.M. Current Perspectives on Vitamin D, Immune System, and Chronic Diseases. Nutrition 2011, 27, 399–404. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Associations of Vitamin D with Insulin Resistance, Obesity, Type 2 Diabetes, and Metabolic Syndrome. J. Steroid Biochem. Mol. Biol. 2018, 175, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Autier, P.; Boniol, M.; Pizot, C.; Mullie, P. Vitamin D Status and Ill Health: A Systematic Review. Lancet Diabetes Endocrinol. 2014, 2, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Zhai, Y.; Shen, S.; Wane, D. Association between Vitamin D and Prediabetes: A PRISMA-Compliant Meta-Analysis. Medicine 2020, 99, e19034. [Google Scholar] [CrossRef]
- Zhang, Y.; Tan, H.; Tang, J.; Li, J.; Chong, W.; Hai, Y.; Feng, Y.; Lunsford, L.D.; Xu, P.; Jia, D.; et al. Effects of Vitamin D Supplementation on Prevention of Type 2 Diabetes in Patients With Prediabetes: A Systematic Review and Meta-Analysis. Diabetes Care 2020, 43, 1650–1658. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, S.; Hajhashemy, Z.; Saneei, P. Serum Vitamin D Levels in Relation to Type-2 Diabetes and Prediabetes in Adults: A Systematic Review and Dose-Response Meta-Analysis of Epidemiologic Studies. Crit. Rev. Food Sci. Nutr. 2022, 62, 8178–8198. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S15–S33. [Google Scholar] [CrossRef]
- Rayyan—Intelligent Systematic Review—Rayyan. Available online: https://www.rayyan.ai/ (accessed on 14 January 2023).
- Al Thani, M.; Sadoun, E.; Sofroniou, A.; Jayyousi, A.; Baagar, K.A.M.; Al Hammaq, A.; Vinodson, B.; Akram, H.; Bhatti, Z.S.; Nasser, H.S.; et al. The Effect of Vitamin D Supplementation on the Glycemic Control of Pre-Diabetic Qatari Patients in a Randomized Control Trial. BMC Nutr. 2019, 5, 46. [Google Scholar] [CrossRef] [Green Version]
- Jorde, R.; Sollid, S.T.; Svartberg, J.; Schirmer, H.; Joakimsen, R.M.; Njølstad, I.; Fuskevåg, O.M.; Figenschau, Y.; Hutchinson, M.Y.S. Vitamin D 20,000 IU per Week for Five Years Does Not Prevent Progression From Prediabetes to Diabetes. J. Clin. Endocrinol. Metab. 2016, 101, 1647–1655. [Google Scholar] [CrossRef] [Green Version]
- Zarrin, R.; Ayremlou, P.; Ghassemi, F. The Effect of Vitamin D Supplementation on the Glycemic Status and the Percentage of Body Fat Mass in Adults with Prediabetes: A Randomized Clinical Trial. Iran. Red Crescent Med. J. 2017, 19, e41718. [Google Scholar] [CrossRef] [Green Version]
- Pittas, A.G.; Dawson-Hughes, B.; Sheehan, P.; Ware, J.H.; Knowler, W.C.; Aroda, V.R.; Brodsky, I.; Ceglia, L.; Chadha, C.; Chatterjee, R.; et al. Vitamin D Supplementation and Prevention of Type 2 Diabetes. N. Engl. J. Med. 2019, 381, 520–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuomainen, T.P.; Virtanen, J.K.; Voutilainen, S.; Nurmi, T.; Mursu, J.; De Mello, V.D.F.; Schwab, U.; Hakumäki, M.; Pulkki, K.; Uusitupa, M. Glucose Metabolism Effects of Vitamin D in Prediabetes: The VitDmet Randomized Placebo-Controlled Supplementation Study. J. Diabetes Res. 2015, 2015, 672653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, M.B.; Duran, P.; Lee, M.L.; Friedman, T.C. High-Dose Vitamin D Supplementation in People with Prediabetes and Hypovitaminosis D. Diabetes Care 2013, 36, 260–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, H.J.; Holmes, L.; Ennis, C.N.; Cardwell, C.R.; Woodside, J.V.; Young, I.S.; Bell, P.M.; Hunter, S.J.; McKinley, M.C. Effect of Vitamin D3 Supplementation on Insulin Resistance and β-Cell Function in Prediabetes: A Double-Blind, Randomized, Placebo-Controlled Trial. Am. J. Clin. Nutr. 2019, 110, 1138–1147. [Google Scholar] [CrossRef]
- Moreira-Lucas, T.S.; Duncan, A.M.; Rabasa-Lhoret, R.; Vieth, R.; Gibbs, A.L.; Badawi, A.; Wolever, T.M.S. Effect of Vitamin D Supplementation on Oral Glucose Tolerance in Individuals with Low Vitamin D Status and Increased Risk for Developing Type 2 Diabetes (EVIDENCE): A Double-Blind, Randomized, Placebo-Controlled Clinical Trial. Diabetes. Obes. Metab. 2017, 19, 133–141. [Google Scholar] [CrossRef]
- Chiu, K.C.; Chu, A.; Go, V.L.W.; Saad, M.F. Hypovitaminosis D Is Associated with Insulin Resistance and Beta Cell Dysfunction. Am. J. Clin. Nutr. 2004, 79, 820–825. [Google Scholar] [CrossRef] [Green Version]
- Rasouli, N.; Brodsky, I.G.; Chatterjee, R.; Kim, S.H.; Pratley, R.E.; Staten, M.A.; Pittas, A.G.; Pittas, A.G.; Brodsky, I.; Ceglia, L.; et al. Effects of Vitamin D Supplementation on Insulin Sensitivity and Secretion in Prediabetes. J. Clin. Endocrinol. Metab. 2022, 107, 230–240. [Google Scholar] [CrossRef]
- Giustina, A.; Adler, R.A.; Binkley, N.; Bollerslev, J.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Formenti, A.M.; Lazaretti-Castro, M.; et al. Consensus Statement from 2nd International Conference on Controversies in Vitamin D. Rev. Endocr. Metab. Disord. 2020, 21, 89–116. [Google Scholar] [CrossRef] [Green Version]
- Carrillo-Larco, R.M.; Jaime Miranda, J.; Gilman, R.H.; Checkley, W.; Smeeth, L.; Bernabe-Ortiz, A. The HOMA-IR Performance to Identify New Diabetes Cases by Degree of Urbanization and Altitude in Peru: The CRONICAS Cohort Study. J. Diabetes Res. 2018, 2018, 7434918. [Google Scholar] [CrossRef] [Green Version]
- Abdesselam, A.; Zidoum, H.; Zadjali, F.; Hedjam, R.; Al-Ansari, A.; Bayoumi, R.; Al-Yahyaee, S.; Hassan, M.; Albarwani, S. Estimate of the HOMA-IR Cut-off Value for Identifying Subjects at Risk of Insulin Resistance Using a Machine Learning Approach. Sultan Qaboos Univ. Med. J. 2021, 21, 604. [Google Scholar] [CrossRef]
- Horáková, D.; Štěpánek, L.; Janout, V.; Janoutová, J.; Pastucha, D.; Kollárová, H.; Petráková, A.; Štěpánek, L.; Husár, R.; Martiník, K. Optimal Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) Cut-Offs: A Cross-Sectional Study in the Czech Population. Medicina 2019, 55, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Insulin Resistance—StatPearls—NCBI Bookshelf. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507839/ (accessed on 3 February 2023).
- Chirita-Emandi, A.; Socolov, D.; Haivas, C.; Calapiş, A.; Gheorghiu, C.; Puiu, M. Vitamin D Status: A Different Story in the Very Young versus the Very Old Romanian Patients. PLoS ONE 2015, 10, e0128010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalid, A.T.; Moore, C.G.; Hall, C.; Olabopo, F.; Rozario, N.L.; Holick, M.F.; Greenspan, S.L.; Rajakumar, K. Utility of Sun-Reactive Skin Typing and Melanin Index for Discerning Vitamin D Deficiency. Pediatr. Res. 2017, 82, 444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenna, M.J. Differences in Vitamin D Status between Countries in Young Adults and the Elderly. Am. J. Med. 1992, 93, 69–77. [Google Scholar] [CrossRef]
- Iraj, B.; Aminorroaya, A.; Amini, M. Does the Intramuscular Injection of Vitamin D Increase Insulin Resistance? J. Res. Pharm. Pract. 2012, 1, 60. [Google Scholar] [CrossRef]
- Karamali, M.; Ashrafi, M.; Razavi, M.; Jamilian, M.; Kashanian, M.; Akbari, M.; Asemi, Z. The Effects of Calcium, Vitamins D and K Co-Supplementation on Markers of Insulin Metabolism and Lipid Profiles in Vitamin D-Deficient Women with Polycystic Ovary Syndrome. Exp. Clin. Endocrinol. Diabetes 2017, 125, 316–321. [Google Scholar] [CrossRef]
- Misra, P.; Kant, S.; Misra, A.; Jha, S.; Kardam, P.; Thakur, N.; Bhatt, S. A Community Based Randomized Controlled Trial to See the Effect of Vitamin D Supplementation on Development of Diabetes Among Women with Prediabetes Residing in A Rural Community of Northern India. J. Fam. Med. Prim. care 2021, 10, 3122. [Google Scholar] [CrossRef]
- Kuchay, M.S.; Laway, B.A.; Bashir, M.I.; Wani, A.I.; Misgar, R.A.; Shah, Z. Effect of Vitamin D Supplementation on Glycemic Parameters and Progression of Prediabetes to Diabetes: A 1-Year, Open-Label Randomized Study. Indian J. Endocrinol. Metab. 2015, 19, 387. [Google Scholar] [CrossRef]
- Dutta, D.; Mondal, S.A.; Choudhuri, S.; Maisnam, I.; Hasanoor Reza, A.H.; Bhattacharya, B.; Chowdhury, S.; Mukhopadhyay, S. Vitamin-D Supplementation in Prediabetes Reduced Progression to Type 2 Diabetes and Was Associated with Decreased Insulin Resistance and Systemic Inflammation: An Open Label Randomized Prospective Study from Eastern India. Diabetes Res. Clin. Pract. 2014, 103, e18–e23. [Google Scholar] [CrossRef]
- Elsayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 3. Prevention or Delay of Type 2 Diabetes and Associated Comorbidities: Standards of Care in Diabetes—2023. Diabetes Care 2023, 46, S41–S48. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Year | No. of Participants | Time | Vit D Dose [IU] | Mean BMI | Mean 25(OH) Baseline Level | Outcome | Effect |
|---|---|---|---|---|---|---|---|---|
| Mohammed Al Thani et al. [33] | 2019 | 209 | 6 months | 4000/daily | 30.0 ± 6.2 | 14.9 ± 4.3 ng/mL | Glucose metabolism | No change |
| Rolf Jorde et al. [34] | 2016 | 511 | 5 years | 20,000/weekly | 30.1 ± 4.1 | 59.9 ± 21.9 nmol/L | Progression to T2DM and glucose metabolism | No change |
| Rasoul Zarrin et al. [35] | 2017 | 120 | 3 months | 1000/daily | 28.71 ± 4.29 | 19.36 ± 13.51 ng/mL | Glucose metabolism | Improve |
| Anastassios G Pittas et al. [36] | 2019 | 2423 | 2.5 years | 4000/daily | 32 ± 4.5 | 27.7 ± 10.2 ng/mL | Progression to T2DM and glucose metabolism | No change |
| Tomi-Pekka Tuomainen et al. [37] | 2015 | 73 | 5 months | 1600 or 3200/daily | 29.4 ± 2.7 | 57.0 ± 11.0 nmol/L | Glucose metabolism | No change |
| Mayer B. Davidson et al. [38] | 2013 | 117 | 12 months | ~88,865/weekly | 32.9 ± 4.3 | 22.0 ± 4.8 ng/mL | Glucose metabolism | No change |
| Helen J Wallace et al. [39] | 2019 | 66 | 26 weeks | 3000/daily | 34.7 ± 8.0 | 30.7 ± 14.3 nmol/L | Glucose metabolism | No change |
| Tracy S. Moreira-Lucas et al. [40] | 2016 | 72 | 24 weeks | 28,000/weekly | 30.1 ± 3.9 | 48.1 ± 14.3 nmol/L | Glucose metabolism | No change |
| No. | Concerns Related to Existing Clinical Study Data | Recommendations for Future RCT’s Designing |
|---|---|---|
| 1. | Follow-up too short | Follow-up > 12 months |
| 2. | Too high, too low, non-physiological, and not frequent enough doses of vitamin D | Sufficiently large doses, consistent with the recommendations for a given population |
| 3. | Lack of reported exclusion criteria or a wide variety of exclusion criteria inconsistent between studies | Medications, current medical diseases, participant’s past medical history, which could potentially influence glucose or vitamin D metabolism, and mental illnesses routinely included in the exclusion criteria beside any relevant others |
| 4. | Different endpoints and glycemic parameters measured | Ideal primary endpoint: diabetes mellitus type 2 developmentThe measured parameters should be consistent with prediabetes criteria established by scientific societies |
| 5. | Vitamin D levels in participants not assessed or participants with normal levels of vitamin D included in study groups together with vitamin D deficient participants | Only participants with hypovitaminosis D divided into levels of this deficiency should be considered in order to get reliable results |
| 6. | Study groups not homogenous regarding: diabetes status | Only patients with diabetes or with prediabetes in one study group |
| 7. | Wide age-range and different ethnicity | Homogenous groups analyzed together |
| 8. | Additional interventions in one study | Vitamin D supplementation should be the only intervention; neither lifestyle change nor co-supplementation should be included in study designs, not allowing for separating the effects of individual interventions |
| 9. | Not reporting or assessing sun exposure, the seasons, and geographical location in which the study was performed | Inclusion of sun exposure, seasons, and geographical locations data with respect to vitamin D and participants |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pieńkowska, A.; Janicka, J.; Duda, M.; Dzwonnik, K.; Lip, K.; Mędza, A.; Szlagatys-Sidorkiewicz, A.; Brzeziński, M. Controversial Impact of Vitamin D Supplementation on Reducing Insulin Resistance and Prevention of Type 2 Diabetes in Patients with Prediabetes: A Systematic Review. Nutrients 2023, 15, 983. https://doi.org/10.3390/nu15040983
Pieńkowska A, Janicka J, Duda M, Dzwonnik K, Lip K, Mędza A, Szlagatys-Sidorkiewicz A, Brzeziński M. Controversial Impact of Vitamin D Supplementation on Reducing Insulin Resistance and Prevention of Type 2 Diabetes in Patients with Prediabetes: A Systematic Review. Nutrients. 2023; 15(4):983. https://doi.org/10.3390/nu15040983
Chicago/Turabian StylePieńkowska, Agata, Justyna Janicka, Michał Duda, Karena Dzwonnik, Kamila Lip, Aleksandra Mędza, Agnieszka Szlagatys-Sidorkiewicz, and Michał Brzeziński. 2023. "Controversial Impact of Vitamin D Supplementation on Reducing Insulin Resistance and Prevention of Type 2 Diabetes in Patients with Prediabetes: A Systematic Review" Nutrients 15, no. 4: 983. https://doi.org/10.3390/nu15040983