
Changes in Blood Markers of Oxidative Stress, Inflammation and Cardiometabolic Patients with COPD after Eccentric and Concentric Cycling Training
 , , and
, , and 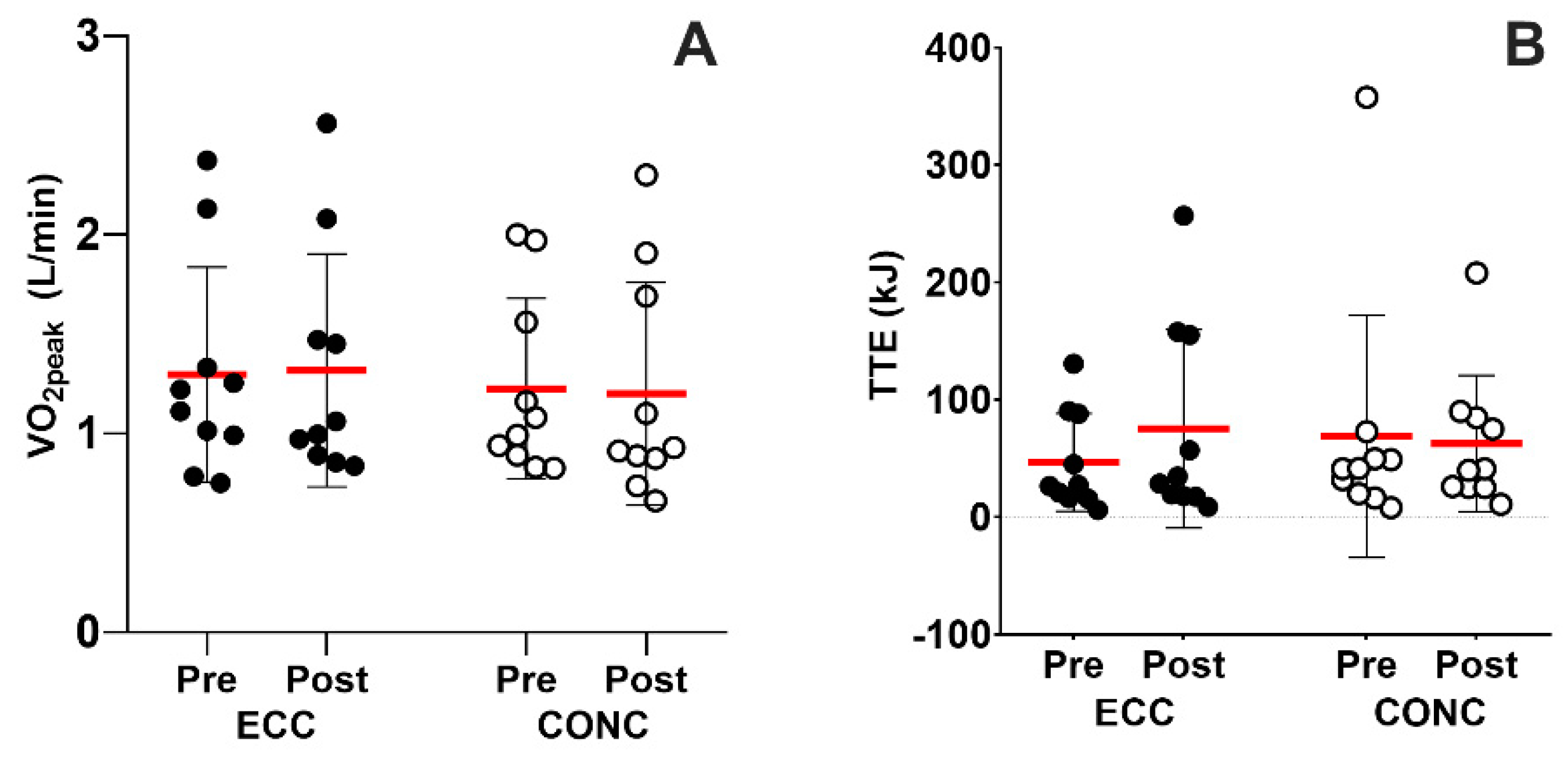{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Exercise Training
2.4. Measurements
2.4.1. Maximal Incremental Cycling Test
2.4.2. Time-to-Exhaustion Test (TTE)
2.4.3. Blood Samples
2.4.4. Oxidative Stress and Inflammatory Markers
2.4.5. Cardiometabolic Health Markers
Insulin Sensitivity
Lipid Profile
2.5. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Maximal Aerobic Capacity
3.3. TTE
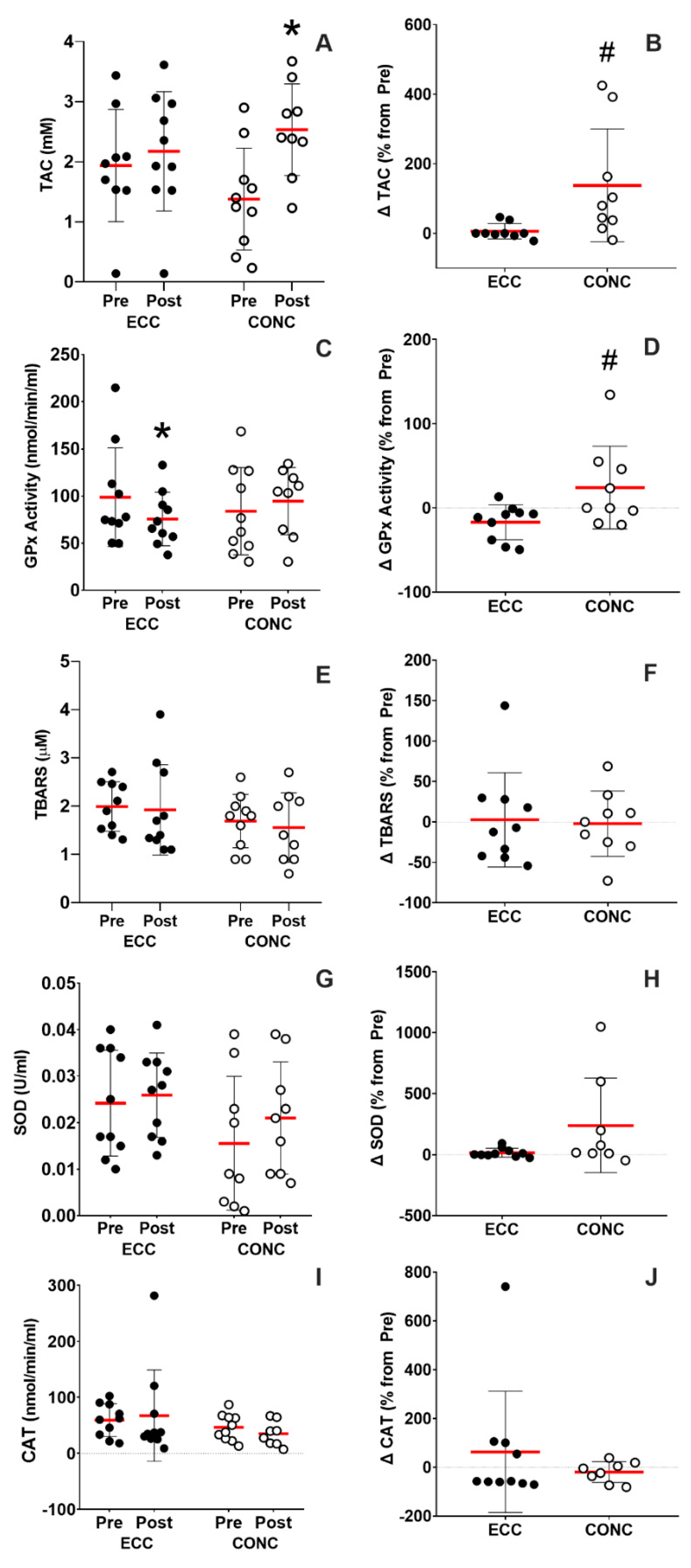
3.4. Systemic Oxidative Stress Markers
3.4.1. At Rest
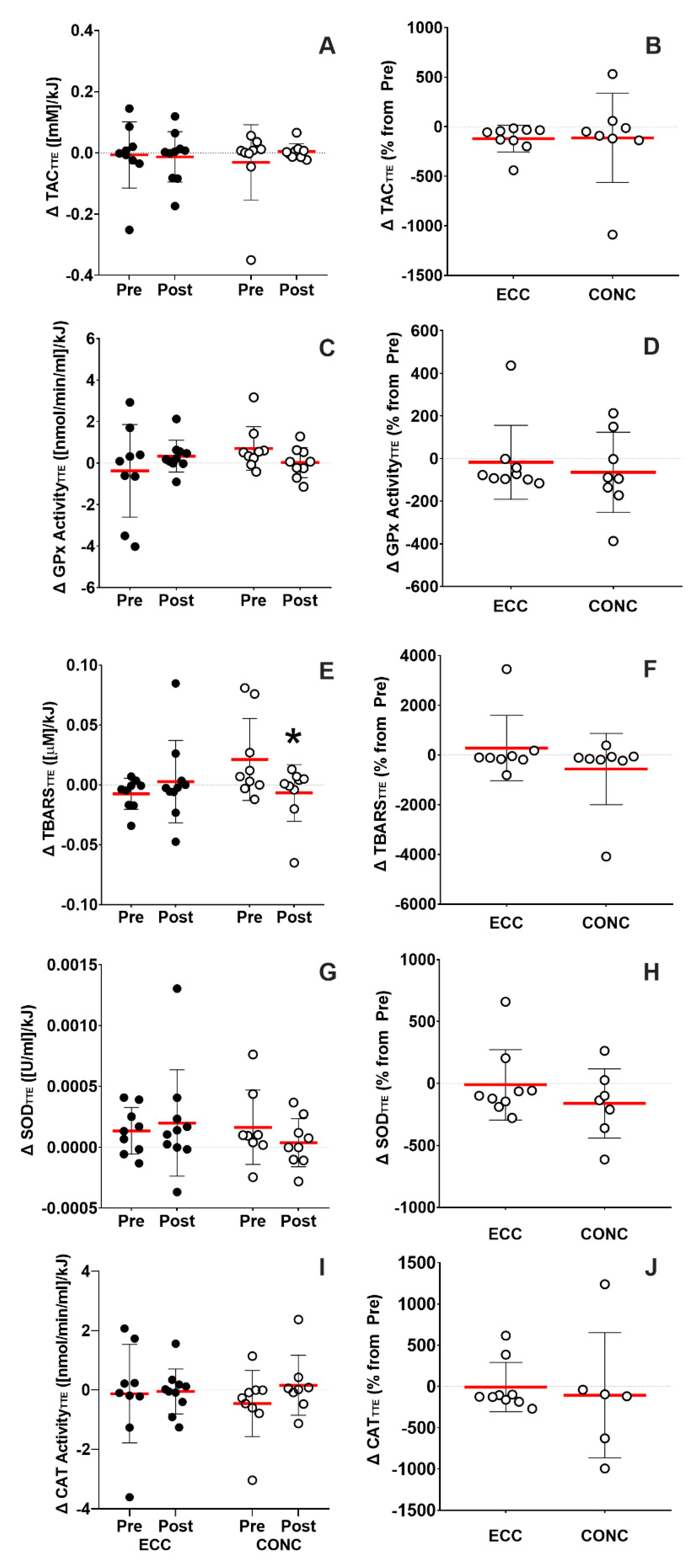
3.4.2. Submaximal Cycling
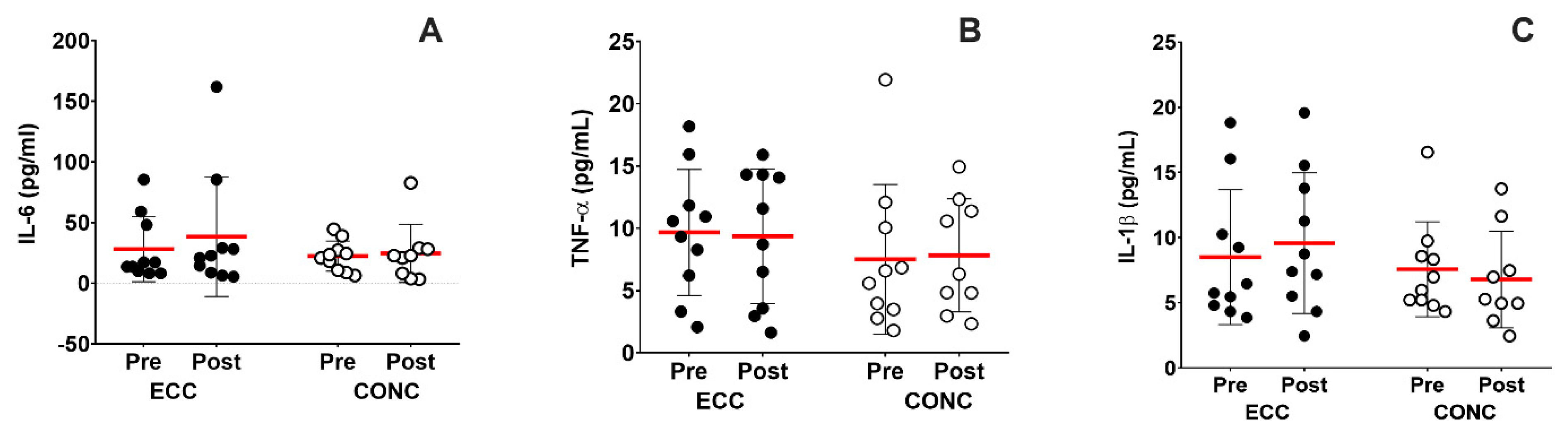
3.5. Systemic Inflammation Markers at Rest
3.6. Cardiometabolic Health Markers
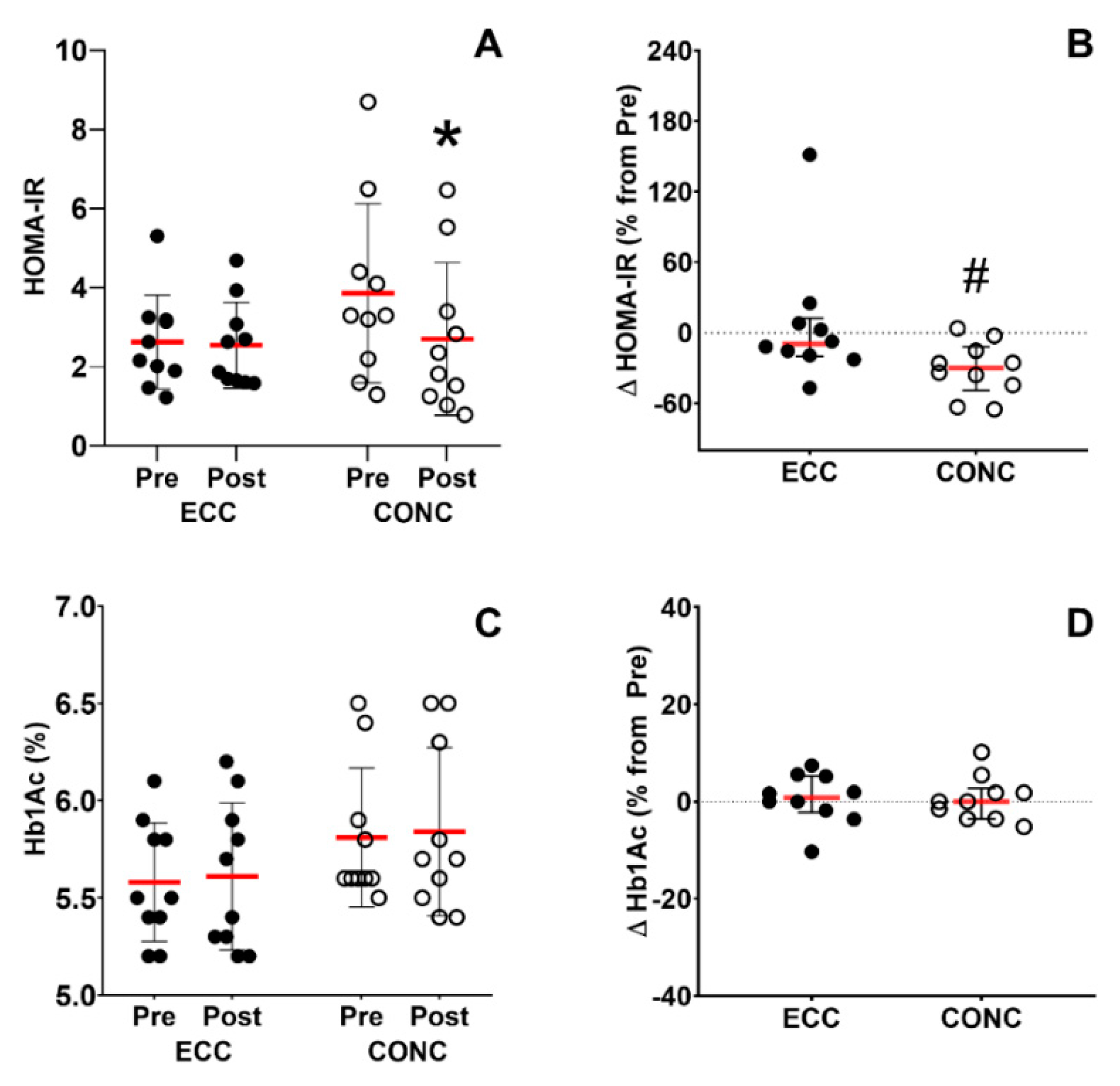
3.6.1. Insulin Sensitivity
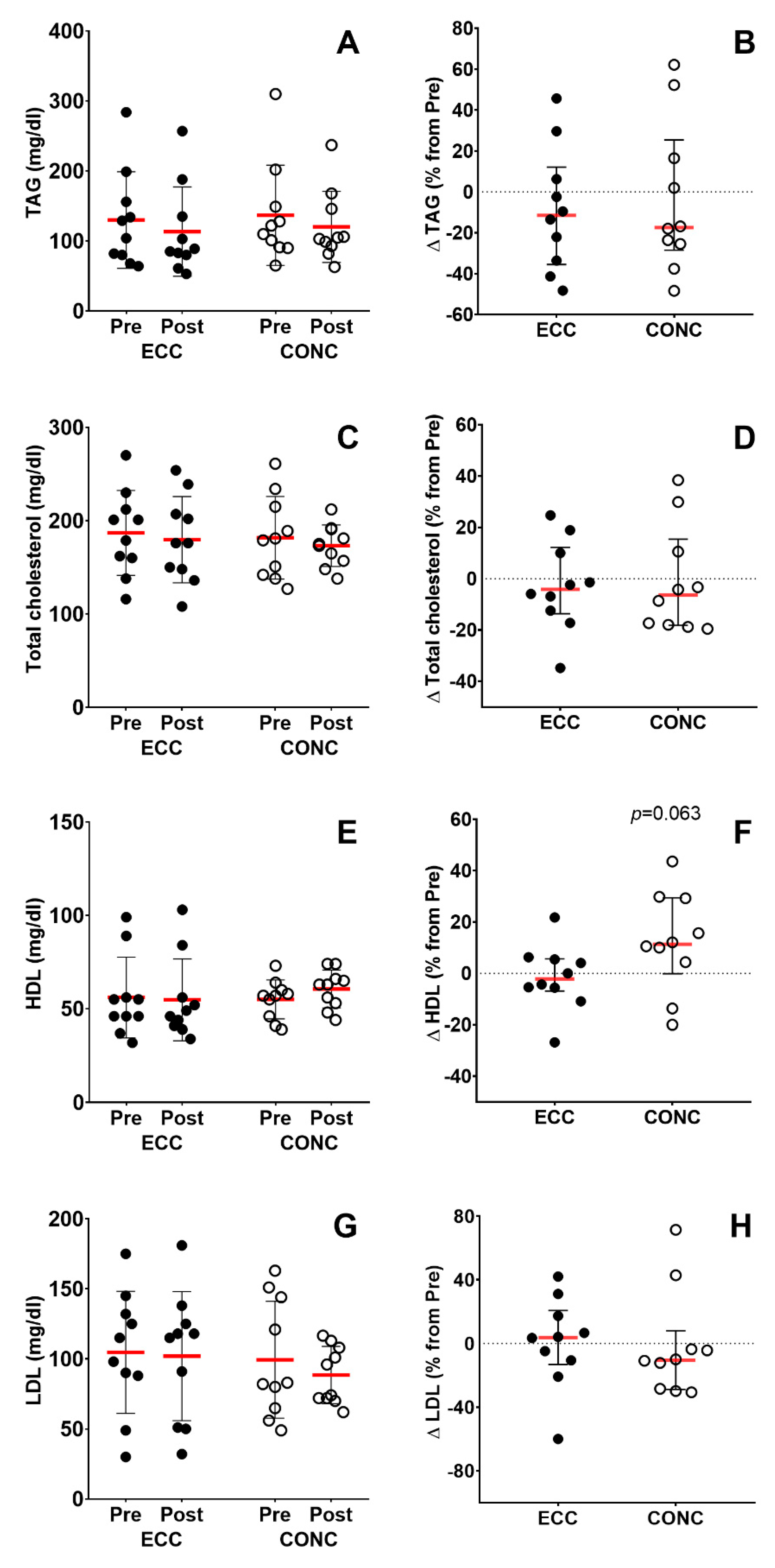
3.6.2. Lipid Profile
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary. Respirology 2017, 22, 575–601. [Google Scholar] [CrossRef]
- Jaitovich, A.; Barreiro, E. Skeletal Muscle Dysfunction in Chronic Obstructive Pulmonary Disease. What We Know and Can Do for Our Patients. Am. J. Respir. Crit. Care Med. 2018, 198, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, A.V.; Maddocks, M.; Martolini, D.; Polkey, M.; Man, W.D.-C. Muscle function in COPD: A complex interplay. Int. J. Chronic Obstr. Pulm. Dis. 2012, 7, 523–535. [Google Scholar] [CrossRef]
- James, B.D.; Jones, A.V.; Trethewey, R.E.; Evans, R. Obesity and metabolic syndrome in COPD: Is exercise the answer? Chronic Respir. Dis. 2018, 15, 173–181. [Google Scholar] [CrossRef]
- Zhao, H.; Li, P.; Wang, J. The role of muscle-specific MicroRNAs in patients with chronic obstructive pulmonary disease and skeletal muscle dysfunction. Front. Physiol. 2022, 13, 954364. [Google Scholar] [CrossRef]
- Singh, S.; Verma, S.; Kumar, S.; Ahmad, M.; Nischal, A.; Singh, S.K.; Dixit, R. Correlation of severity of chronic obstructive pulmonary disease with potential biomarkers. Immunol. Lett. 2018, 196, 1–10. [Google Scholar] [CrossRef]
- Barreiro, E.; Fermoselle, C.; Mateu-Jimenez, M.; Sánchez-Font, A.; Pijuan, L.; Gea, J.; Curull, V. Oxidative stress and inflammation in the normal airways and blood of patients with lung cancer and COPD. Free Radic. Biol. Med. 2013, 65, 859–871. [Google Scholar] [CrossRef]
- De Brandt, J.; Spruit, M.A.; Derave, W.; Hansen, D.; Vanfleteren, L.E.G.W.; Burtin, C. Changes in structural and metabolic muscle characteristics following exercise-based interventions in patients with COPD: A systematic review. Expert Rev. Respir. Med. 2016, 10, 521–545. [Google Scholar] [CrossRef] [PubMed]
- Iepsen, U.W.; Jørgensen, K.J.; Ringbaek, T.; Hansen, H.; Skrubbeltrang, C.; Lange, P. A Systematic Review of Resistance Training Versus Endurance Training in COPD. J. Cardiopulm. Rehabil. Prev. 2015, 35, 163–172. [Google Scholar] [CrossRef]
- Zeng, Y.; Jiang, F.; Chen, Y.; Chen, P.; Cai, S. Exercise assessments and trainings of pulmonary rehabilitation in COPD: A literature review. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 2013–2023. [Google Scholar] [CrossRef] [Green Version]
- Spruit, M.; Gosselink, R.; Troosters, T.; De Paepe, K.; Decramer, M. Resistance versus endurance training in patients with COPD and peripheral muscle weakness. Eur. Respir. J. 2002, 19, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Vogiatzis, I.; Simoes, D.C.M.; Stratakos, G.; Kourepini, E.; Terzis, G.; Manta, P.; Athanasopoulos, D.; Roussos, C.; Wagner, P.D.; Zakynthinos, S. Effect of pulmonary rehabilitation on muscle remodelling in cachectic patients with COPD. Eur. Respir. J. 2010, 36, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wu, W.; Wang, X.; Chen, L. Effect of Endurance Training in COPD Patients Undergoing Pulmonary Rehabilitation: A Meta-Analysis. Comput. Math. Methods Med. 2022, 2022, 4671419. [Google Scholar] [CrossRef]
- Nolan, C.M.; Rochester, C.L. Exercise Training Modalities for People with Chronic Obstructive Pulmonary Disease. COPD J. Chronic Obstr. Pulm. Dis. 2019, 16, 378–389. [Google Scholar] [CrossRef] [PubMed]
- Vogiatzis, I.; Stratakos, G.; Simoes, D.C.M.; Terzis, G.; Georgiadou, O.; Roussos, C.; Zakynthinos, S. Effects of rehabilitative exercise on peripheral muscle TNF, IL-6, IGF-I and MyoD expression in patients with COPD. Thorax 2007, 62, 950–956. [Google Scholar] [CrossRef]
- Whittom, F.; Jobin, J.; Simard, P.M.; Leblanc, P.; Simard, C.; Bernard, S.; Belleau, R.; Maltais, F. Histochemical and morphological characteristics of the vastus lateralis muscle in patients with chronic obstructive pulmonary disease. Med. Sci. Sports Exerc. 1998, 30, 1467–1474. [Google Scholar] [CrossRef]
- Barreiro, E.; Rabinovich, R.; Marin-Corral, J.; Barberà, J.A.; Gea, J.; Roca, J. Chronic endurance exercise induces quadriceps nitrosative stress in patients with severe COPD. Thorax 2009, 64, 13–19. [Google Scholar] [CrossRef]
- Nickel, R.; Troncoso, F.; Flores, O.; Gonzalez-Bartholin, R.; Mackay, K.; Diaz, O.; Jalon, M.; Peñailillo, L. Physiological response to eccentric and concentric cycling in patients with chronic obstructive pulmonary disease. Appl. Physiol. Nutr. Metab. 2020, 45, 1232–1237. [Google Scholar] [CrossRef]
- Inostroza, M.; Valdés, O.; Tapia, G.; Núñez, O.; Kompen, M.J.; Nosaka, K.; Peñailillo, L. Effects of eccentric vs concentric cycling training on patients with moderate COPD. Eur. J. Appl. Physiol. 2022, 122, 489–502. [Google Scholar] [CrossRef]
- MacMillan, N.J.; Kapchinsky, S.; Konokhova, Y.; Gouspillou, G.; Sena, R.D.S.; Jagoe, R.T.; Baril, J.; Carver, T.E.; Andersen, R.E.; Richard, R.; et al. Eccentric Ergometer Training Promotes Locomotor Muscle Strength but Not Mitochondrial Adaptation in Patients with Severe Chronic Obstructive Pulmonary Disease. Front. Physiol. 2017, 8, 114. [Google Scholar] [CrossRef] [Green Version]
- Julian, V.; Thivel, D.; Miguet, M.; Pereira, B.; Costes, F.; Coudeyre, E.; Duclos, M.; Richard, R. Eccentric cycling is more efficient in reducing fat mass than concentric cycling in adolescents with obesity. Scand. J. Med. Sci. Sports 2019, 29, 4–15. [Google Scholar] [CrossRef]
- Valladares-Ide, D.; Bravo, M.J.; Carvajal, A.; Araneda, O.F.; Tuesta, M.; Reyes, A.; Peñailillo, R.; Peñailillo, L. Changes in pulmonary and plasma oxidative stress and inflammation following eccentric and concentric cycling in stable COPD patients. Eur. J. Appl. Physiol. 2021, 121, 1677–1688. [Google Scholar] [CrossRef]
- Alcazar, J.; Losa-Reyna, J.; Lopez, C.R.; Navarro-Cruz, R.; Alfaro-Acha, A.; Ara, I.; García-García, F.J.; Alegre, L.M.; Guadalupe-Grau, A. Effects of concurrent exercise training on muscle dysfunction and systemic oxidative stress in older people with COPD. Scand. J. Med. Sci. Sports 2019, 29, 1591–1603. [Google Scholar] [CrossRef]
- Domaszewska, K.; Górna, S.; Pietrzak, M.; Podgórski, T. Oxidative Stress and Total Phenolics Concentration in COPD Patients—The Effect of Exercises: A Randomized Controlled Trial. Nutrients 2022, 14, 1947. [Google Scholar] [CrossRef] [PubMed]
- Pinho, R.; Chiesa, D.; Mezzomo, K.; Andrades, M.; Bonatto, F.; Gelain, D.; Pizzol, F.D.; Knorst, M.; Moreira, J. Oxidative stress in chronic obstructive pulmonary disease patients submitted to a rehabilitation program. Respir. Med. 2007, 101, 1830–1835. [Google Scholar] [CrossRef] [PubMed]
- Couillard, A.; Maltais, F.; Saey, D.; Debigaré, R.; Michaud, A.; Koechlin, C.; LeBlanc, P.; Préfaut, C. Exercise-induced Quadriceps Oxidative Stress and Peripheral Muscle Dysfunction in Patients with Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2003, 167, 1664–1669. [Google Scholar] [CrossRef]
- Nicolò, A.; Sacchetti, M.; Girardi, M.; McCormick, A.; Angius, L.; Bazzucchi, I.; Marcora, S.M. A comparison of different methods to analyse data collected during time-to-exhaustion tests. Sport Sci. Health 2019, 15, 667–679. [Google Scholar] [CrossRef]
- Saey, D.; Debigaré, R.; LeBlanc, P.; Mador, M.J.; Côté, C.H.; Jobin, J.; Maltais, F. Contractile Leg Fatigue after Cycle Exercise: A factor limiting exercise in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2003, 168, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Barreiro, E.; Gea, J.; Matar, G.; Hussain, S.N. Expression and Carbonylation of Creatine Kinase in the Quadriceps Femoris Muscles of Patients with Chronic Obstructive Pulmonary Disease. Am. J. Respir. Cell Mol. Biol. 2005, 33, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Barreiro, E. Role of Protein Carbonylation in Skeletal Muscle Mass Loss Associated with Chronic Conditions. Proteomes 2016, 4, 18. [Google Scholar] [CrossRef] [Green Version]
- Paschalis, V.; Nikolaidis, M.G.; Theodorou, A.A.; Panayiotou, G.; Fatouros, I.G.; Koutedakis, Y.; Jamurtas, T. A Weekly Bout of Eccentric Exercise Is Sufficient to Induce Health-Promoting Effects. Med. Sci. Sports Exerc. 2011, 43, 64–73. [Google Scholar] [CrossRef]
- Peñailillo, L.; Blazevich, A.; Numazawa, H.; Nosaka, K. Metabolic and Muscle Damage Profiles of Concentric versus Repeated Eccentric Cycling. Med. Sci. Sports Exerc. 2013, 45, 1773–1781. [Google Scholar] [CrossRef] [PubMed]
- Whipp, B.J.; Ward, S.A. Quantifying intervention-related improvements in exercise tolerance. Eur. Respir. J. 2009, 33, 1254–1260. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- McNamara, R.J.; Houben-Wilke, S.; Franssen, F.M.; Smid, D.E.; Vanfleteren, L.E.; Groenen, M.T.; Uszko-Lencer, N.H.; Wouters, E.F.; Alison, J.A.; Spruit, M.A. Determinants of functional, peak and endurance exercise capacity in people with chronic obstructive pulmonary disease. Respir. Med. 2018, 138, 81–87. [Google Scholar] [CrossRef]
- Rooyackers, J.; Berkeljon, D.; Folgering, H. Eccentric exercise training in patients with chronic obstructive pulmonary disease. Int. J. Rehabil. Res. 2003, 26, 47–49. [Google Scholar] [CrossRef]
- Porszasz, J.; Emtner, M.; Goto, S.; Somfay, A.; Whipp, B.J.; Casaburi, R. Exercise Training Decreases Ventilatory Requirements and Exercise-Induced Hyperinflation at Submaximal Intensities in Patients With COPD. Chest 2005, 128, 2025–2034. [Google Scholar] [CrossRef] [PubMed]
- Bauerle, O.; Chrusch, C.A.; Younes, M. Mechanisms by Which COPD Affects Exercise Tolerance. Am. J. Respir. Crit. Care Med. 1998, 157, 57–68. [Google Scholar] [CrossRef]
- Kluchová, Z.; Petrášová, D.; Joppa, P.; Dorková, Z.; Tkáčová, R. The association between oxidative stress and obstructive lung impairment in patients with COPD. Physiol. Res. 2007, 56, 51–56. [Google Scholar] [CrossRef]
- Zarrindast, S.; Ramezanpour, M.; Moghaddam, M. Effects of eight weeks of moderate intensity aerobic training and training in water on DNA damage, lipid peroxidation and total antioxidant capacity in sixty years sedentary women. Sci. Sports 2021, 36, e81–e85. [Google Scholar] [CrossRef]
- Shin, Y.-A.; Lee, J.-H.; Song, W.; Jun, T.-W. Exercise training improves the antioxidant enzyme activity with no changes of telomere length. Mech. Ageing Dev. 2008, 129, 254–260. [Google Scholar] [CrossRef]
- Mercken, E.M.; Hageman, G.J.; Schols, A.M.W.J.; Akkermans, M.A.; Bast, A.; Wouters, E.F.M. Rehabilitation Decreases Exercise-induced Oxidative Stress in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2005, 172, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K. The anti-inflammatory effect of exercise: Its role in diabetes and cardiovascular disease control. Essays Biochem. 2006, 42, 105–117. [Google Scholar] [CrossRef]
- Ryrsø, C.K.; Thaning, P.; Siebenmann, C.; Lundby, C.; Lange, P.; Pedersen, B.K.; Hellsten, Y.; Iepsen, U.W. Effect of endurance versus resistance training on local muscle and systemic inflammation and oxidative stress in COPD. Scand. J. Med. Sci. Sports 2018, 28, 2339–2348. [Google Scholar] [CrossRef]
- De Matos, M.A.; Vieira, D.V.; Pinhal, K.C.; Lopes, J.F.; Dias-Peixoto, M.F.; Pauli, J.R.; Magalhães, F.D.C.; Little, J.P.; Rocha-Vieira, E.; Amorim, F.T. High-Intensity Interval Training Improves Markers of Oxidative Metabolism in Skeletal Muscle of Individuals With Obesity and Insulin Resistance. Front. Physiol. 2018, 9, 1451. [Google Scholar] [CrossRef]
- Álvarez, C.; Ramírez-Campillo, R.; Ramírez-Vélez, R.; Izquierdo, M. Effects and prevalence of nonresponders after 12 weeks of high-intensity interval or resistance training in women with insulin resistance: A randomized trial. J. Appl. Physiol. 2017, 122, 985–996. [Google Scholar] [CrossRef] [PubMed]
- Evans, P.L.; McMillin, S.L.; Weyrauch, L.A.; Witczak, C.A. Regulation of Skeletal Muscle Glucose Transport and Glucose Metabolism by Exercise Training. Nutrients 2019, 11, 2432. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.C.; Hsieh, C.-C.; Tseng, K.-W.; Ho, C.-C.; Nosaka, K. Effects of Descending Stair Walking on Health and Fitness of Elderly Obese Women. Med. Sci. Sports Exerc. 2017, 49, 1614–1622. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.C.-C.; Tseng, W.-C.; Huang, G.-L.; Chen, H.-L.; Tseng, K.-W.; Nosaka, K. Superior Effects of Eccentric to Concentric Knee Extensor Resistance Training on Physical Fitness, Insulin Sensitivity and Lipid Profiles of Elderly Men. Front. Physiol. 2017, 8, 209. [Google Scholar] [CrossRef] [PubMed]
- Drexel, H.; Saely, C.H.; Langer, P.; Loruenser, G.; Marte, T.; Risch, L.; Hoefle, G.; Aczel, S. Metabolic and anti-inflammatory benefits of eccentric endurance exercise—A pilot study. Eur. J. Clin. Investig. 2008, 38, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Yfanti, C.; Tsiokanos, A.; Fatouros, I.G.; A Theodorou, A.; Deli, C.K.; Koutedakis, Y.; Jamurtas, A.Z. Chronic Eccentric Exercise and Antioxidant Supplementation: Effects on Lipid Profile and Insulin Sensitivity. J. Sports Sci. Med. 2017, 16, 375–382. [Google Scholar] [PubMed]
- Zeppetzauer, M.; Drexel, H.; Vonbank, A.; Rein, P.; Aczel, S.; Saely, C.H. Eccentric endurance exercise economically improves metabolic and inflammatory risk factors. Eur. J. Prev. Cardiol. 2013, 20, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, M.G.; Paschalis, V.; Giakas, G.; Fatouros, I.G.; Sakellariou, G.K.; Theodorou, A.A.; Koutedakis, Y.; Jamurtas, A.Z. Favorable and Prolonged Changes in Blood Lipid Profile after Muscle-Damaging Exercise. Med. Sci. Sports Exerc. 2008, 40, 1483–1489. [Google Scholar] [CrossRef]
- Paschalis, V.; Nikolaidis, M.G.; Giakas, G.; Theodorou, A.A.; Sakellariou, G.K.; Fatouros, I.G.; Koutedakis, Y.; Jamurtas, A.Z.; Jamurtas, T. Beneficial changes in energy expenditure and lipid profile after eccentric exercise in overweight and lean women. Scand. J. Med. Sci. Sports 2010, 20, e103–e111. [Google Scholar] [CrossRef] [PubMed]
- Sillanpaa, E.; Hakkinen, A.; Punnonen, K.; Laaksonen, D.E. Effects of strength and endurance training on metabolic risk factors in healthy 40-65-year-old men. Scand. J. Med. Sci. Sports 2009, 19, 885–895. [Google Scholar] [CrossRef]
- Boukabous, I.; Marcotte-Chénard, A.; Amamou, T.; Boulay, P.; Brochu, M.; Tessier, D.; Dionne, I.; Riesco, E. Low-Volume High-Intensity Interval Training Versus Moderate-Intensity Continuous Training on Body Composition, Cardiometabolic Profile, and Physical Capacity in Older Women. J. Aging Phys. Act. 2019, 27, 879–889. [Google Scholar] [CrossRef]
- Barnes, P.J. COPD 2020: New directions needed. Am. J. Physiol. Cell Mol. Physiol. 2020, 319, L884–L886. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valero-Breton, M.; Valladares-Ide, D.; Álvarez, C.; Peñailillo, R.S.; Peñailillo, L. Changes in Blood Markers of Oxidative Stress, Inflammation and Cardiometabolic Patients with COPD after Eccentric and Concentric Cycling Training. Nutrients 2023, 15, 908. https://doi.org/10.3390/nu15040908
Valero-Breton M, Valladares-Ide D, Álvarez C, Peñailillo RS, Peñailillo L. Changes in Blood Markers of Oxidative Stress, Inflammation and Cardiometabolic Patients with COPD after Eccentric and Concentric Cycling Training. Nutrients. 2023; 15(4):908. https://doi.org/10.3390/nu15040908
Chicago/Turabian StyleValero-Breton, Mayalen, Denisse Valladares-Ide, Cristian Álvarez, Reyna S. Peñailillo, and Luis Peñailillo. 2023. "Changes in Blood Markers of Oxidative Stress, Inflammation and Cardiometabolic Patients with COPD after Eccentric and Concentric Cycling Training" Nutrients 15, no. 4: 908. https://doi.org/10.3390/nu15040908