
Underlying Mechanisms Involved in Gambling Disorder Severity: A Pathway Analysis Considering Genetic, Psychosocial, and Clinical Variables
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Clinical Measurements
2.3. Other Variables
2.4. Genetic Information
2.5. Statistical Analyses
3. Results
3.1. Description of the Participants and Distribution of the Genetic Measures
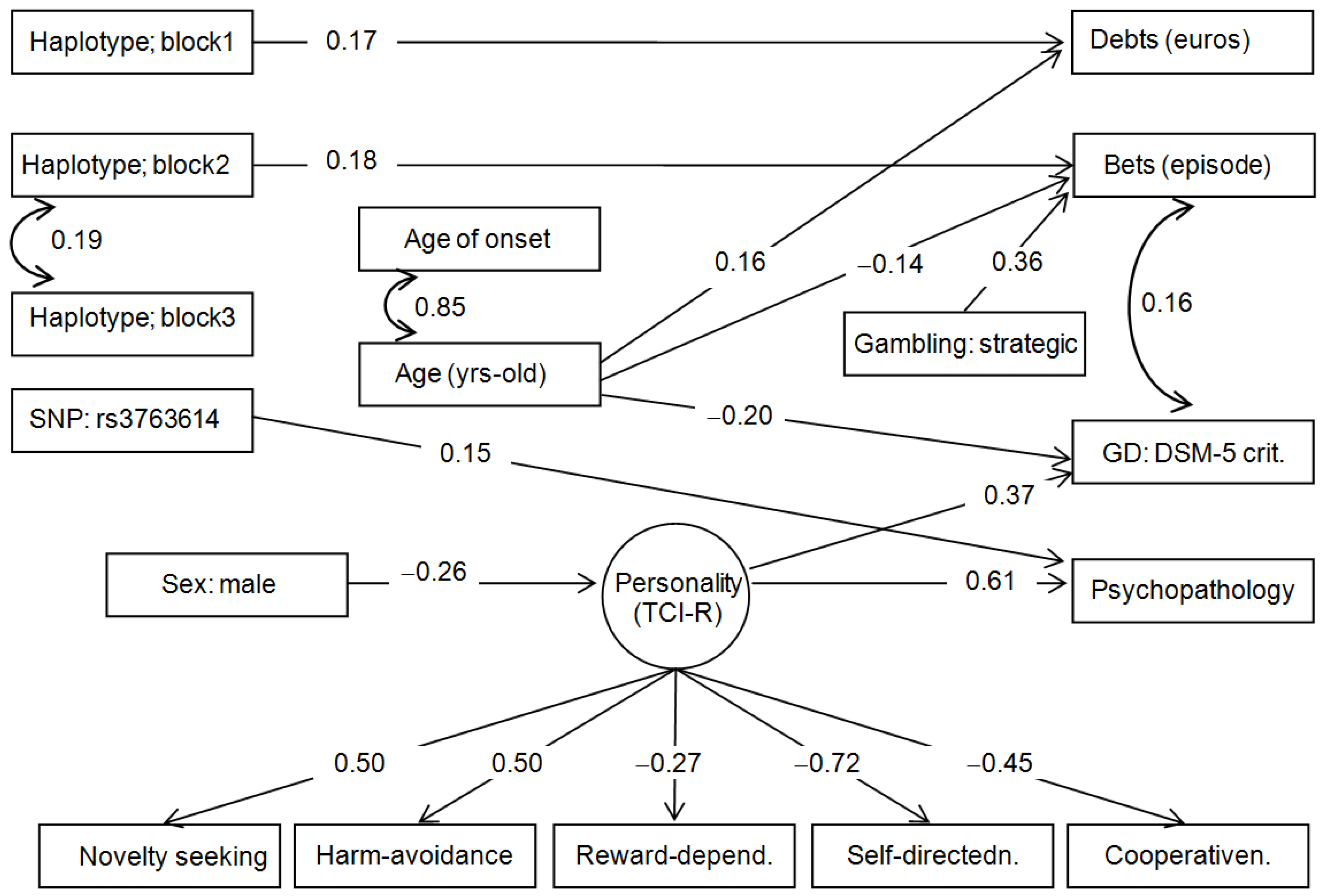
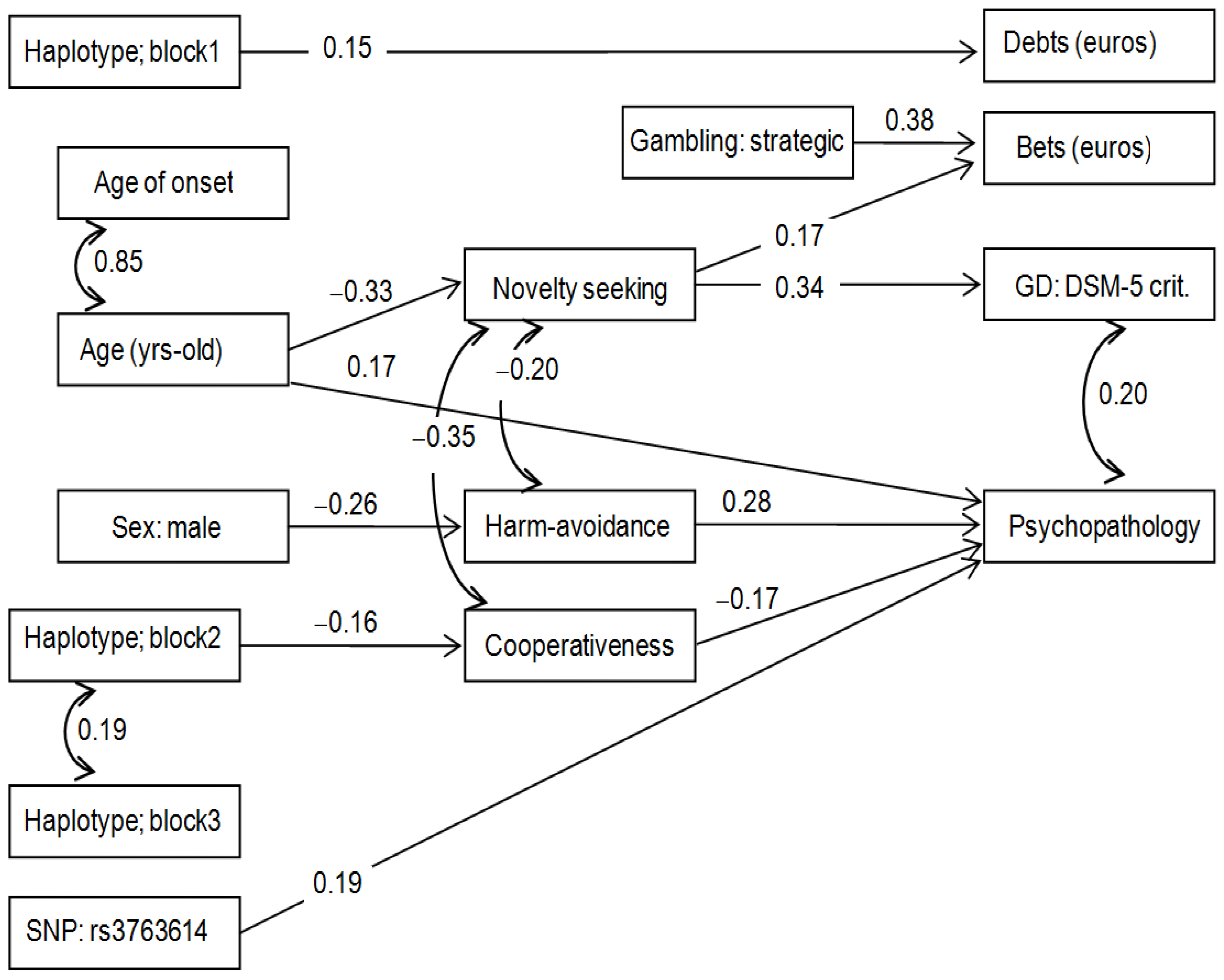
3.2. Path Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ji, L.J.; McGeorge, K.; Li, Y.; Lee, A.; Zhang, Z. Culture and gambling fallacies. Springerplus 2015, 4, 510. [Google Scholar] [CrossRef] [Green Version]
- Potenza, M.N.; Kosten, T.R.; Rounsaville, B.J. Pathological Gambling. JAMA 2001, 286, 141. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Abbott, M.W.; Romild, U.; Volberg, R.A. Gambling and Problem Gambling in Sweden: Changes between 1998 and 2009. J. Gambl. Stud. 2014, 30, 985–999. [Google Scholar] [CrossRef]
- Abbott, M.; Romild, U.; Volberg, R. The prevalence, incidence, and gender and age-specific incidence of problem gambling: Results of the Swedish longitudinal gambling study (Swelogs). Addiction 2018, 113, 699–707. [Google Scholar] [CrossRef]
- Calado, F.; Alexandre, J.; Griffiths, M.D. Prevalence of Adolescent Problem Gambling: A Systematic Review of Recent Research. J. Gambl. Stud. 2017, 33, 397–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calado, F.; Griffiths, M.D. Problem gambling worldwide: An update and systematic review of empirical research (2000–2015). J. Behav. Addict. 2016, 5, 592–613. [Google Scholar] [CrossRef] [Green Version]
- Thomas, S.L.; Thomas, S.D. The big gamble: The need for a comprehensive research approach to understanding the causes and consequences of gambling harm in Australia. Australas. Epidemiol. 2015, 22, 39–42. [Google Scholar]
- Potenza, M.N.; Balodis, I.M.; Deverensky, J.; Grant, J.E.; Petry, N.M.; Verdejo-Garcia, A.; Yip, S.W. Gambling disorder. Nat. Rev. Dis. Prim. 2019, 5, 51. [Google Scholar] [CrossRef]
- Castrén, S.; Basnet, S.; Salonen, A.H.; Pankakoski, M.; Ronkainen, J.E.; Alho, H.; Lahti, T. Factors associated with disordered gambling in Finland. Subst. Abus. Treat. Prev. Policy 2013, 8, 24. [Google Scholar] [CrossRef]
- Hing, N.; Russell, A.M.T.T.; Vitartas, P.; Lamont, M. Demographic, behavioural and normative risk factors for gambling problems amongst sports bettors. J. Gambl. Stud. 2016, 32, 625–641. [Google Scholar] [CrossRef] [Green Version]
- Yücel, M.; Whittle, S.; Youssef, G.J.; Kashyap, H.; Simmons, J.G.; Schwartz, O.; Lubman, D.I.; Allen, N.B. The influence of sex, temperament, risk-taking and mental health on the emergence of gambling: A longitudinal study of young people. Int. Gambl. Stud. 2015, 15, 108–123. [Google Scholar] [CrossRef]
- Jiménez-Murcia, S.; Granero, R.; Tárrega, S.; Angulo, A.; Fernández-Aranda, F.; Arcelus, J.; Fagundo, A.B.; Aymamí, N.; Moragas, L.; Sauvaget, A.; et al. Mediational Role of Age of Onset in Gambling Disorder, a Path Modeling Analysis. J. Gambl. Stud. 2016, 32, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Granero, R.; Penelo, E.; Martínez-Giménez, R.; Álvarez-Moya, E.; Gómez-Peña, M.; Aymamí, M.N.; Bueno, B.; Fernández-Aranda, F.; Jiménez-Murcia, S. Sex differences among treatment-seeking adult pathologic gamblers. Compr. Psychiatry 2009, 50, 173–180. [Google Scholar] [CrossRef]
- Jiménez-Murcia, S.; Stinchfield, R.; Álvarez-Moya, E.; Jaurrieta, N.; Bueno, B.; Granero, R.; Aymamí, M.N.; Gómez-Peña, M.; Martínez-Giménez, R.; Fernández-Aranda, F.; et al. Reliability, validity, and classification accuracy of a spanish translation of a measure of DSM-IV diagnostic criteria for pathological gambling. J. Gambl. Stud. 2009, 25, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.E.; Odlaug, B.L.; Chamberlain, S.R.; Schreiber, L.R.N. Neurocognitive dysfunction in strategic and non-strategic gamblers. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2012, 38, 336–340. [Google Scholar] [CrossRef] [Green Version]
- Slutske, W.S.; Piasecki, T.M.; Deutsch, A.R.; Statham, D.J.; Martin, N.G. Telescoping and gender differences in the time course of disordered gambling: Evidence from a general population sample. Addiction 2015, 110, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Murcia, S. Trastornos del Control de Impulsos: Juego Patológico. In Introducción a la Psicopatología y la Psiquiatría; Ruiloba, J.V., Ed.; Elsevier Masson: Barcelona, Spain, 2015; pp. 433–453. [Google Scholar]
- Granero, R.; Jiménez-Murcia, S.; del Pino-Gutiérrez, A.; Mora, B.; Mendoza-Valenciano, E.; Baenas-Soto, I.; Gómez-Peña, M.; Moragas, L.; Codina, E.; López-González, H.; et al. Gambling Phenotypes in Online Sports Betting. Front. Psychiatry 2020, 11, 482. [Google Scholar] [CrossRef]
- Granero, R.; Penelo, E.; Stinchfield, R.; Fernandez-Aranda, F.; Savvidou, L.G.; Fröberg, F.; Aymamí, N.; Gómez-Peña, M.; Pérez-Serrano, M.; del Pino-Gutiérrez, A.; et al. Is Pathological Gambling Moderated by Age? J. Gambl. Stud. 2014, 30, 475–492. [Google Scholar] [CrossRef]
- Jiménez-Murcia, S.; Giménez, M.; Granero, R.; López-González, H.; Gómez-Peña, M.; Moragas, L.; Baenas, I.; Del Pino-Gutiérrez, A.; Codina, E.; Mena-Moreno, T.; et al. Psychopathogical status and personality correlates of problem gambling severity in sports bettors undergoing treatment for gambling disorder. J. Behav. Addict. 2021, 10, 422–434. [Google Scholar] [CrossRef]
- Brewer, J.A.; Potenza, M.N. The neurobiology and genetics of impulse control disorders: Relationships to drug addictions. Biochem. Pharmacol. 2008, 75, 63–75. [Google Scholar] [CrossRef] [Green Version]
- Blain, B.; Richard Gill, P.; Teese, R. Predicting problem gambling in Australian adults using a multifaceted model of impulsivity. Int. Gambl. Stud. 2015, 15, 239–255. [Google Scholar] [CrossRef]
- Vintró-Alcaraz, C.; Mestre-Bach, G.; Granero, R.; Gómez-Peña, M.; Moragas, L.; Fernández-Aranda, F.; Jiménez-Murcia, S. Do emotion regulation and impulsivity differ according to gambling preferences in clinical samples of gamblers? Addict. Behav. 2022, 126, 107176. [Google Scholar] [CrossRef] [PubMed]
- Dowling, N.A.; Merkouris, S.S.; Greenwood, C.J.; Oldenhof, E.; Toumbourou, J.W.; Youssef, G.J. Early risk and protective factors for problem gambling: A systematic review and meta-analysis of longitudinal studies. Clin. Psychol. Rev. 2017, 51, 109–124. [Google Scholar] [CrossRef] [Green Version]
- Lara-Huallipe, M.L.; Granero, R.; Fernández-Aranda, F.; Gómez-Peña, M.; Moragas, L.; del Pino-Gutierrez, A.; Valenciano-Mendoza, E.; Mora-Maltas, B.; Baenas, I.; Etxandi, M.; et al. Clustering Treatment Outcomes in Women with Gambling Disorder. J. Gambl. Stud. 2021, 38, 1469–1491. [Google Scholar] [CrossRef]
- Ledgerwood, D.M.; Dyshniku, F.; McCarthy, J.E.; Ostojic-Aitkens, D.; Forfitt, J.; Rumble, S.C. Gambling-Related Cognitive Distortions in Residential Treatment for Gambling Disorder. J. Gambl. Stud. 2020, 36, 669–683. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Murcia, S.; Granero, R.; Fernández-Aranda, F.; Stinchfield, R.; Tremblay, J.; Steward, T.; Mestre-Bach, G.; Lozano-Madrid, M.; Mena-Moreno, T.; Mallorquí-Bagué, N.; et al. Phenotypes in gambling disorder using sociodemographic and clinical clustering analysis: An unidentified new subtype? Front. Psychiatry 2019, 10, 173. [Google Scholar] [CrossRef]
- Slutske, W.S.; Meier, M.H.; Zhu, G.; Statham, D.J.; Blaszczynski, A.; Martin, N.G. The Australian Twin Study of Gambling (OZ-GAM): Rationale, Sample Description, Predictors of Participation, and a First Look at Sources of Individual Differences in Gambling Involvement. Twin Res. Hum. Genet. 2009, 12, 63–78. [Google Scholar] [CrossRef]
- Slutske, W.S.; Richmond-Rakerd, L.S. A closer look at the evidence for sex differences in the genetic and environmental influences on gambling in the National Longitudinal Study of Adolescent health: From disordered to ordered gambling. Addiction 2014, 109, 120–127. [Google Scholar] [CrossRef] [Green Version]
- Tak, Y.G.; Farnham, P.J. Making sense of GWAS: Using epigenomics and genome engineering to understand the functional relevance of SNPs in non-coding regions of the human genome. Epigenetics Chromatin 2015, 8, 57. [Google Scholar] [CrossRef] [Green Version]
- Lang, M.; Leménager, T.; Streit, F.; Fauth-Bühler, M.; Frank, J.; Juraeva, D.; Witt, S.H.; Degenhardt, F.; Hofmann, A.; Heilmann-Heimbach, S.; et al. Genome-wide association study of pathological gambling. Eur. Psychiatry 2016, 36, 38–46. [Google Scholar] [CrossRef]
- Munguía, L.; Jiménez-Murcia, S.; Granero, R.; Baenas, I.; Agüera, Z.; Sánchez, I.; Codina, E.; Del Pino-Gutiérrez, A.; Testa, G.; Treasure, J.; et al. Emotional regulation in eating disorders and gambling disorder: A transdiagnostic approach. J. Behav. Addict. 2022, 10, 508–523. [Google Scholar] [CrossRef]
- Koskela, M.; Bäck, S.; Võikar, V.; Richie, C.T.; Domanskyi, A.; Harvey, B.K.; Airavaara, M. Update of neurotrophic factors in neurobiology of addiction and future directions. Neurobiol. Dis. 2017, 97, 189–200. [Google Scholar] [CrossRef] [Green Version]
- Castrén, E. Neurotrophins and Psychiatric Disorders. Handb. Exp. Pharmacol. 2014, 220, 461–479. [Google Scholar] [CrossRef]
- Solé-Morata, N.; Baenas, I.; Etxandi, M.; Granero, R. The role of neurotrophin genes involved in the vulnerability to gambling disorder. Sci. Rep. 2022, 12, 6925. [Google Scholar] [CrossRef] [PubMed]
- Ernfors, P. Local and target-derived actions of neurotrophins during peripheral nervous system development. Cell. Mol. Life Sci. 2001, 58, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Linnet, J. The anticipatory dopamine response in addiction: A common neurobiological underpinning of gambling disorder and substance use disorder? Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 98, 109802. [Google Scholar] [CrossRef] [PubMed]
- Pettorruso, M.; Zoratto, F.; Miuli, A.; De Risio, L.; Santorelli, M.; Pierotti, A.; Martinotti, G.; Adriani, W.; di Giannantonio, M. Exploring dopaminergic transmission in gambling addiction: A systematic translational review. Neurosci. Biobehav. Rev. 2020, 119, 481–511. [Google Scholar] [CrossRef]
- Gratacòs, M.; Escaramís, G.; Bustamante, M.; Saus, E.; Agüera, Z.; Bayés, M.; Cellini, E.; de Cid, R.; Fernández-Aranda, F.; Forcano, L.; et al. Role of the neurotrophin network in eating disorders’ subphenotypes: Body mass index and age at onset of the disease. J. Psychiatr. Res. 2010, 44, 834–840. [Google Scholar] [CrossRef]
- Mercader, J.M.; Fernández-Aranda, F.; Gratacòs, M.; Ribasés, M.; Badía, A.; Villarejo, C.; Solano, R.; González, J.R.; Vallejo, J.; Estivill, X. Blood levels of brain-derived neurotrophic factor correlate with several psychopathological symptoms in anorexia nervosa patients. Neuropsychobiology 2008, 56, 185–190. [Google Scholar] [CrossRef] [Green Version]
- Angelucci, F.; Martinotti, G.; Gelfo, F.; Righino, E.; Conte, G.; Caltagirone, C.; Bria, P.; Ricci, V. Enhanced BDNF serum levels in patients with severe pathological gambling. Addict. Biol. 2013, 18, 749–751. [Google Scholar] [CrossRef]
- Choi, S.-W.; Shin, Y.-C.; Mok, J.Y.; Kim, D.-J.; Choi, J.-S.; Hwang, S.S.-H. Serum BDNF levels in patients with gambling disorder are associated with the severity of gambling disorder and Iowa Gambling Task indices. J. Behav. Addict. 2016, 5, 135–139. [Google Scholar] [CrossRef]
- Geisel, O.; Banas, R.; Hellweg, R.; Müller, C.A. Altered Serum Levels of Brain-Derived Neurotrophic Factor in Patients with Pathological Gambling. Eur. Addict. Res. 2012, 18, 297–301. [Google Scholar] [CrossRef]
- Kim, H.S.; von Ranson, K.M.; Hodgins, D.C.; McGrath, D.S.; Tavares, H. Demographic, psychiatric, and personality correlates of adults seeking treatment for disordered gambling with a comorbid binge/purge type eating disorder. Eur. Eat. Disord. Rev. 2018, 26, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Haniu, M.; Talvenheimo, J.; Le, J.; Katta, V.; Welcher, A.; Rohde, M.F. Extracellular domain of neurotrophin receptor trkB: Disulfide structure, N-glycosylation sites, and ligand binding. Arch. Biochem. Biophys. 1995, 322, 256–264. [Google Scholar] [CrossRef]
- Otsuki, K.; Uchida, S.; Watanuki, T.; Wakabayashi, Y.; Fujimoto, M.; Matsubara, T.; Funato, H.; Watanabe, Y. Altered expression of neurotrophic factors in patients with major depression. J. Psychiatr. Res. 2008, 42, 1145–1153. [Google Scholar] [CrossRef]
- Cho, S.C.; Kim, H.W.; Kim, B.N.; Kim, J.W.; Shin, M.S.; Cho, D.Y.; Chung, S.; Jung, S.W.; Yoo, H.J.; Chung, I.W.; et al. Neurotrophin-3 gene, intelligence, and selective attention deficit in a Korean sample with attention-deficit/hyperactivity disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2010, 34, 1065–1069. [Google Scholar] [CrossRef]
- Ceccarini, M.R.; Tasegian, A.; Franzago, M.; Patria, F.F.; Albi, E.; Codini, M.; Conte, C.; Bertelli, M.; Ragione, L.D.; Stuppia, L.; et al. 5-HT2AR and BDNF gene variants in eating disorders susceptibility. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2020, 183, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Mercader, J.M.; Saus, E.; Agüera, Z.; Bayés, M.; Boni, C.; Carreras, A.; Cellini, E.; de Cid, R.; Dierssen, M.; Escaramís, G.; et al. Association of NTRK3 and its interaction with NGF suggest an altered cross-regulation of the neurotrophin signaling pathway in eating disorders. Hum. Mol. Genet. 2008, 17, 1234–1244. [Google Scholar] [CrossRef]
- Retz, W.; Ringling, J.; Retz-Junginger, P.; Vogelgesang, M.; Rösler, M. Association of attention-deficit/hyperactivity disorder with gambling disorder. J. Neural Transm. 2016, 123, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Fatséas, M.; Hurmic, H.; Serre, F.; Debrabant, R.; Daulouède, J.P.; Denis, C.; Auriacombe, M. Addiction severity pattern associated with adult and childhood Attention Deficit Hyperactivity Disorder (ADHD) in patients with addictions. Psychiatry Res. 2016, 246, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, N.S.; Livesey, E.J.; Blaszczynski, A.; Harris, J.A. Pathological Gambling and Motor Impulsivity: A Systematic Review with Meta-Analysis. J. Gambl. Stud. 2017, 33, 1213–1239. [Google Scholar] [CrossRef] [PubMed]
- Ledgerwood, D.M.; Petry, N.M. Subtyping pathological gamblers based on impulsivity, depression, and anxiety. Psychol. Addict. Behav. 2010, 24, 680–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5 Research Version; American Psychiatric Association: Arlington, VA, USA, 2015. [Google Scholar]
- Stinchfield, R. Reliability, Validity, and Classification Accuracy of a Measure of DSM-IV Diagnostic Criteria for Pathological Gambling. Am. J. Psychiatry 2003, 160, 180–182. [Google Scholar] [CrossRef]
- American Psychiatric Association. DSM-IV-TR. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric association (APA): Washington, DC, USA, 2000; ISBN 0-89042-334-2. [Google Scholar]
- Lesieur, H.R.; Blume, S.B. The South Oaks Gambling Screen (SOGS): A new instrument for the identification of Pathological gamblers. Am. J. Psychiatry 1987, 144, 1184–1188. [Google Scholar] [CrossRef]
- Echeburúa, E.; Báez, C.; Fernández-Montalvo, J.; Páez, D.; Baez, C.; Fernández-Montalvo, J.; Páez, D. Cuestionario de Juego Patológico de South Oaks (SOGS): Validación española. Análisis Modif. Conduct. 1994, 20, 769–791. [Google Scholar]
- Derogatis, L.R. SCL-90-R: Symptom Checklist-90-R. Administration, Scoring and Procedures Manuall—II for the Revised Version; Clinical Psychometric Research: Towson, MD, USA, 1994. [Google Scholar]
- Derogatis, L. SCL-90-R. Cuestionario de 90 Síntomas-Manual; TEA: Madrid, Spain, 2002. [Google Scholar]
- Cloninger, C.R. The Temperament and Character Inventory Revised; Center for Psychobiology of Personality, Washington University: St Louis, MO, USA, 1999. [Google Scholar]
- Gutiérrez-Zotes, J.A.; Bayón, C.; Montserrat, C.; Valero, J.; Labad, A.; Cloninger, C.R.; Fernández-Aranda, F. Temperament and Character Inventory Revised (TCI-R). Standardization and normative data in a general population sample. Actas Españolas Psiquiatr. 2004, 32, 8–15. [Google Scholar]
- Jimenez-Murcia, S.; Aymamí-Sanromà, N.M.; Gómez-Peña, M.; Álvarez-Moya, E.M.; Vallejo, J. Protocols de Tractament Cognitivoconductual Pel Joc Patològic i D’altres Addiccions no Tòxiques; Hospital Universitary de Bellvitge: Barcelona, Spain, 2006. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 2nd ed.; The Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Oertzen, T. Power equivalence in structural equation modelling. Br. J. Math. Stat. Psychol. 2010, 63, 257–272. [Google Scholar] [CrossRef] [PubMed]
- Borsboom, D.; Mellenbergh, G.J.; van Heerden, J. The theoretical status of latent variables. Psychol. Rev. 2003, 110, 203–219. [Google Scholar] [CrossRef] [Green Version]
- Barrett, P. Structural equation modelling: Adjudging model fit. Pers. Individ. Dif. 2007, 42, 815–824. [Google Scholar] [CrossRef]
- Jiménez-Murcia, S.; Granero, R.; Fernández-Aranda, F.; Arcelus, J.; Aymamí, M.N.; Gómez-Peña, M.; Tárrega, S.; Moragas, L.; Del Pino-Gutiérrez, A.; Sauchelli, S.; et al. Predictors of outcome among pathological gamblers receiving cognitive behavioral group therapy. Eur. Addict. Res. 2015, 21, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Sharman, S.; Murphy, R.; Turner, J.; Roberts, A. Psychosocial correlates in treatment seeking gamblers: Differences in early age onset gamblers vs later age onset gamblers. Addict. Behav. 2019, 97, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Volberg, R.A.; Gupta, R.; Griffiths, M.D.; Olason, D.T.; Delfabbro, P. An international perspective on youth gambling prevalence studies. Int. J. Adolesc. Med. Health 2010, 22, 3–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.W.; Grant, J.E.; Eckert, E.D.; Faris, P.L.; Hartman, B.K. Pathological gambling and mood disorders: Clinical associations and treatment implications. J. Affect. Disord. 2006, 92, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Moya, E.M.; Jiménez-Murcia, S.; Aymamí, M.N.; Gómez-Peña, M.; Granero, R.; Santamaría, J.; Menchón, J.M.; Fernández-Aranda, F. Subtyping Study of a Pathological Gamblers Sample. Can. J. Psychiatry 2010, 55, 498–506. [Google Scholar] [CrossRef] [Green Version]
- Granero, R.; Jiménez-Murcia, S.; del Pino-Gutiérrez, A.; Mena-Moreno, T.; Mestre-Bach, G.; Gómez-Peña, M.; Moragas, L.; Aymamí, N.; Giroux, I.; Grall-Bronnec, M.; et al. Gambling Phenotypes in Older Adults. J. Gambl. Stud. 2020, 36, 809–828. [Google Scholar] [CrossRef]
- Jiménez-Murcia, S.; Granero, R.; Giménez, M.; del Pino-Gutiérrez, A.; Mestre-Bach, G.; Mena-Moreno, T.; Moragas, L.; Baño, M.; Sánchez-González, J.; de Gracia, M.; et al. Contribution of sex on the underlying mechanism of the gambling disorder severity. Sci. Rep. 2020, 10, 18722. [Google Scholar] [CrossRef]
- Khanbhai, Y.; Smith, D.; Battersby, M. Gender by Preferred Gambling Activity in Treatment Seeking Problem Gamblers: A Comparison of Subgroup Characteristics and Treatment Outcomes. J. Gambl. Stud. 2017, 33, 99–113. [Google Scholar] [CrossRef] [Green Version]
- Grant, J.E.; Chamberlain, S.R.; Schreiber, L.R.N.; Odlaug, B.L. Gender-related clinical and neurocognitive differences in individuals seeking treatment for pathological gambling. J. Psychiatr. Res. 2012, 46, 1206–1211. [Google Scholar] [CrossRef] [Green Version]
- Odlaug, B.L.; Chamberlain, S.R. Gambling and Personality Dimensions. Curr. Behav. Neurosci. Rep. 2014, 1, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Janiri, L.; Martinotti, G.; Dario, T.; Schifano, F.; Bria, P. The Gamblers’ Temperament and Character Inventory (TCI) Personality Profile. Subst. Use Misuse 2007, 42, 975–984. [Google Scholar] [CrossRef]
- Lobo, D.S.S.; Quilty, L.C.; Martins, S.S.; Tavares, H.; Vallada, H.; Kennedy, J.L.; Bagby, R.M. Pathological gambling subtypes: A comparison of treatment-seeking and non-treatment-seeking samples from Brazil and Canada. Addict. Behav. 2014, 39, 1172–1175. [Google Scholar] [CrossRef] [PubMed]
- Moragas, L.; Granero, R.; Stinchfield, R.; Fernández-Aranda, F.; Fröberg, F.; Aymamí, N.; Gómez-Peña, M.; Fagundo, A.B.; Islam, M.A.; del Pino-Gutiérrez, A.; et al. Comparative analysis of distinct phenotypes in gambling disorder based on gambling preferences. BMC Psychiatry 2015, 15, 86. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Murcia, S.; Fernández-Aranda, F.; Mestre-Bach, G.; Granero, R.; Tárrega, S.; Torrubia, R.; Aymamí, N.; Gómez-Peña, M.; Soriano-Mas, C.; Steward, T.; et al. Exploring the Relationship between Reward and Punishment Sensitivity and Gambling Disorder in a Clinical Sample: A Path Modeling Analysis. J. Gambl. Stud. 2017, 33, 579–597. [Google Scholar] [CrossRef] [PubMed]
- Lorains, F.K.; Cowlishaw, S.; Thomas, S.A. Prevalence of comorbid disorders in problem and pathological gambling: Systematic review and meta-analysis of population surveys. Addiction 2011, 106, 490–498. [Google Scholar] [CrossRef]
- Atkinson, J.; Sharp, C.; Schmitz, J.; Yaroslavsky, I. Behavioral Activation and Inhibition, Negative Affect, and Gambling Severity in a Sample of Young Adult College Students. J. Gambl. Stud. 2012, 28, 437–449. [Google Scholar] [CrossRef] [PubMed]
- Kernie, S.G.; Liebl, D.J.; Parada, L.F. BDNF regulates eating behavior and locomotor activity in mice. EMBO J. 2000, 19, 1290–1300. [Google Scholar] [CrossRef] [Green Version]
- Xu, B.; Goulding, E.H.; Zang, K.; Cepoi, D.; Cone, R.D.; Jones, K.R.; Tecott, L.H.; Reichardt, L.F. Brain-derived neurotrophic factor regulates energy balance downstream of melanocortin-4 receptor. Nat. Neurosci. 2003, 6, 736–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sleeman, M.W.; Garcia, K.; Liu, R.; Murray, J.D.; Malinova, L.; Moncrieffe, M.; Yancopoulos, G.D.; Wiegand, S.J. Ciliary neurotrophic factor improves diabetic parameters and hepatic steatosis and increases basal metabolic rate in db/db mice. Proc. Natl. Acad. Sci. USA 2003, 100, 14297–14302. [Google Scholar] [CrossRef] [Green Version]
- Kokoeva, M.V.; Yin, H.; Flier, J.S. Neurogenesis in the Hypothalamus of Adult Mice: Potential Role in Energy Balance. Science 2005, 310, 679–683. [Google Scholar] [CrossRef]
- Fauth-Bühler, M.; Mann, K.; Potenza, M.N. Pathological gambling: A review of the neurobiological evidence relevant for its classification as an addictive disorder. Addict. Biol. 2017, 22, 885–897. [Google Scholar] [CrossRef]
- Griffiths, M.D. Behavioural addiction and substance addiction should be defined by their similarities not their dissimilarities. Addiction 2017, 112, 1718–1720. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Socio-Demographics | n | % | |
|---|---|---|---|
| Sex | Women | 12 | 8.2% |
| Men | 134 | 91.8% | |
| Civil status | Single | 46 | 31.5% |
| Married—couple | 83 | 56.8% | |
| Divorced—separated | 17 | 11.6% | |
| Education level | Primary | 104 | 71.2% |
| Secondary | 36 | 24.7% | |
| University | 6 | 4.1% | |
| Employment status | Unemployed | 46 | 31.5% |
| Employed | 100 | 68.5% | |
| Age-onset-duration | Mean | SD | |
| Chronological age (years-old) | 40.2 | 12.52 | |
| Onset of gambling problems | 34.24 | 11.89 | |
| Duration of gambling problems | 13.72 | 8.60 | |
| Gambling activity (reason treatment) | n | % | |
| Slot-machines | 131 | 89.7% | |
| Bingo | 32 | 21.9% | |
| Lotteries | 13 | 8.9% | |
| Casino | 15 | 10.3% | |
| Cards | 10 | 6.8% | |
| Preference (reason treatment) | n | % | |
| Only non-strategic | 125 | 85.6% | |
| Only strategic | 5 | 3.4% | |
| Both (non-strategic and strategic) | 16 | 11.0% | |
| Bets | Median | IQR | |
| Maximum euros per episode | 400 | 300 | |
| Debts due to gambling activity | n | % | |
| Yes | 100 | 71.9% | |
| No | 46 | 28.1% | |
| n | % | n | % | |||
|---|---|---|---|---|---|---|
| Block 1 (SNPs: rs6489630, rs7956189) | SNP: rs7956189 AA | |||||
| Haplotype | A | 85 | 58.2% | AA | 98 | 67.1% |
| TA | 13 | 8.9% | AG * | 45 | 30.8% | |
| TG * | 48 | 32.9% | GG * | 3 | 2.1% | |
| Block 2 (SNPs: rs4412435, rs10868241, rs4361832) | SNP: rs3739570 CC * | |||||
| Haplotype | CAA | 2 | 1.4% | CC * | 130 | 89.0% |
| CAG | 4 | 2.7% | CT | 15 | 10.3% | |
| CGG | 9 | 6.2% | TT | 1 | 0.7% | |
| TGG * | 131 | 89.7% | SNP: rs3763614 CC * | |||
| Block 3 (SNPs: rs11140783, rs3739570) | CC * | 137 | 93.8% | |||
| Haplotype | CC * | 119 | 81.5% | CT | 9 | 6.2% |
| CT | 14 | 9.6% | SNP: rs11140783 CC * | |||
| TC | 13 | 8.9% | CC * | 133 | 91.1% | |
| CT | 13 | 8.9% | ||||
| Cramer-V Values | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1 | Haplotype-1 | −0.003 | −0.042 | 1.000 | −0.035 | −0.124 | −0.088 |
| 2 | Haplotype-2 | --- | 0.187 | −0.003 | 0.315 | −0.087 | −0.106 |
| 3 | Haplotype-3 | --- | −0.042 | 0.737 | −0.122 | 0.656 | |
| 4 | rs7956189 | --- | −0.035 | −0.124 | −0.088 | ||
| 5 | rs3739570 | --- | −0.090 | 0.044 | |||
| 6 | rs3763614 | --- | −0.080 | ||||
| 7 | rs11140783 | --- | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solé-Morata, N.; Baenas, I.; Etxandi, M.; Granero, R.; Gené, M.; Barrot, C.; Gómez-Peña, M.; Moragas, L.; Ramoz, N.; Gorwood, P.; et al. Underlying Mechanisms Involved in Gambling Disorder Severity: A Pathway Analysis Considering Genetic, Psychosocial, and Clinical Variables. Nutrients 2023, 15, 418. https://doi.org/10.3390/nu15020418
Solé-Morata N, Baenas I, Etxandi M, Granero R, Gené M, Barrot C, Gómez-Peña M, Moragas L, Ramoz N, Gorwood P, et al. Underlying Mechanisms Involved in Gambling Disorder Severity: A Pathway Analysis Considering Genetic, Psychosocial, and Clinical Variables. Nutrients. 2023; 15(2):418. https://doi.org/10.3390/nu15020418
Chicago/Turabian StyleSolé-Morata, Neus, Isabel Baenas, Mikel Etxandi, Roser Granero, Manel Gené, Carme Barrot, Mónica Gómez-Peña, Laura Moragas, Nicolas Ramoz, Philip Gorwood, and et al. 2023. "Underlying Mechanisms Involved in Gambling Disorder Severity: A Pathway Analysis Considering Genetic, Psychosocial, and Clinical Variables" Nutrients 15, no. 2: 418. https://doi.org/10.3390/nu15020418