
The Association between Sugar-Sweetened Beverages and Male Pattern Hair Loss in Young Men
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
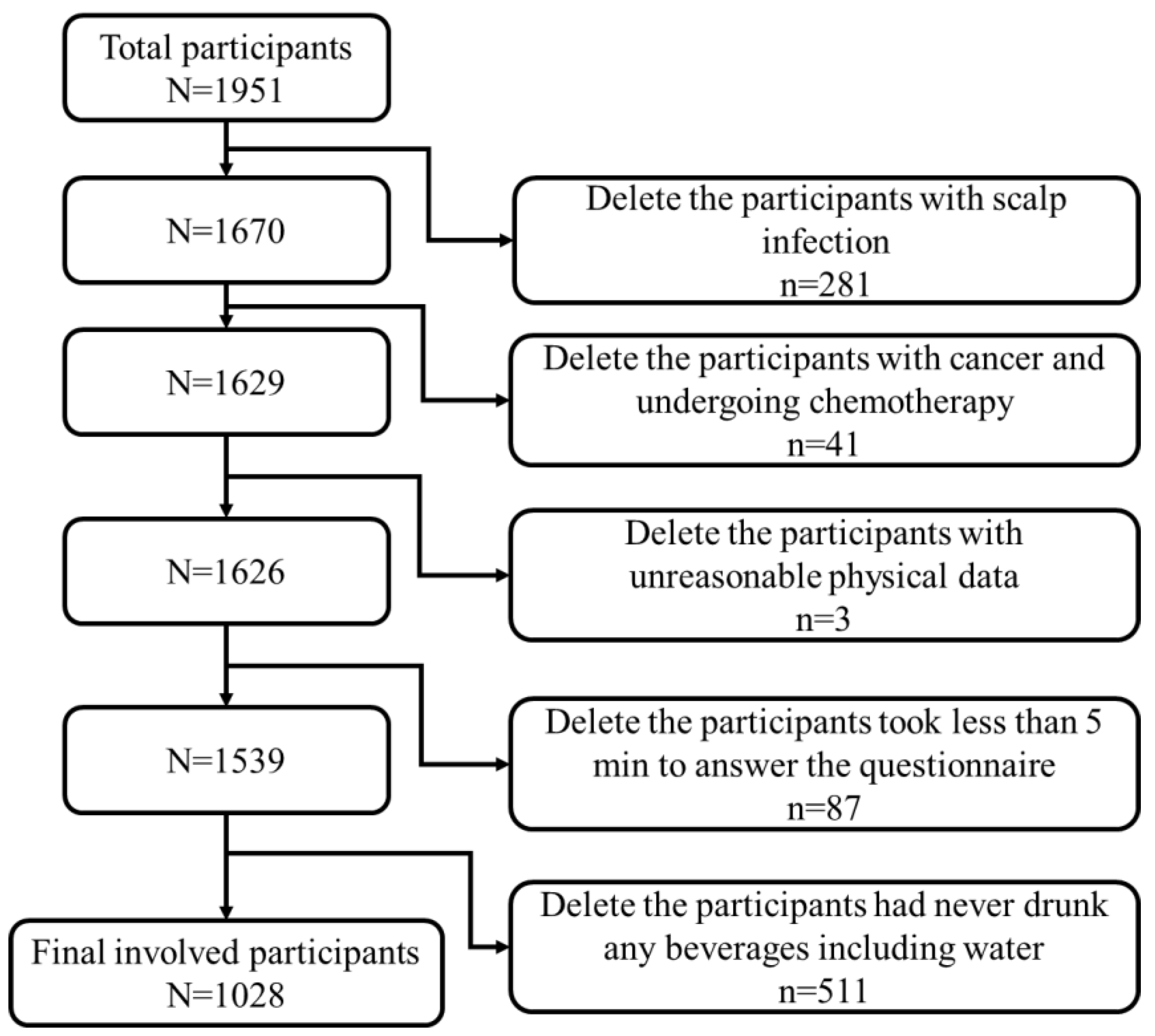
2.1. Study Design and Participants
2.2. Data Collection
2.3. Ethics
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, T.L.; Zhou, C.; Shen, Y.W.; Wang, X.Y.; Ding, X.L.; Tian, S.; Liu, Y.; Peng, G.; Xue, S.; Zhou, J.; et al. Prevalence of androgenetic alopecia in China: A community-based study in six cities. Br. J. Dermatol. 2010, 162, 843–847. [Google Scholar] [CrossRef] [PubMed]
- Mu, Z.; Gao, Y.; Li, K.; Liu, H.; Zhang, J. Androgenetic Alopecia Among Hospital Staff: A Study of Prevalence, Types and a Comparison with General Population in a Secondary Hospital in China. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1387–1392. [Google Scholar] [CrossRef] [PubMed]
- Shellow, W.V.; Edwards, J.E.; Koo, J.Y. Profile of alopecia areata: A questionnaire analysis of patient and family. Int. J. Dermatol. 1992, 31, 186–189. [Google Scholar] [CrossRef] [PubMed]
- McDonald, K.A.; Shelley, A.J.; Colantonio, S.; Beecker, J. Hair pull test: Evidence-based update and revision of guidelines. J. Am. Acad. Dermatol. 2017, 76, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Mounsey, A.L.; Reed, S.W. Diagnosing and treating hair loss. Am. Fam. Physician 2009, 80, 356–362. [Google Scholar]
- Hadshiew, I.M.; Foitzik, K.; Arck, P.C.; Paus, R. Burden of hair loss: Stress and the underestimated psychosocial impact of telogen effluvium and androgenetic alopecia. J. Investig. Dermatol. 2004, 123, 455–457. [Google Scholar] [CrossRef] [Green Version]
- Glaser, R.L.; Dimitrakakis, C.; Messenger, A.G. Improvement in scalp hair growth in androgen-deficient women treated with testosterone: A questionnaire study. Br. J. Dermatol. 2012, 166, 274–278. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.; Zhang, B. Corticosterone inhibits GAS6 to govern hair follicle stem-cell quiescence. Nature 2021, 592, 428–432. [Google Scholar] [CrossRef]
- Yi, Y.; Qiu, J.; Jia, J.; Djakaya, G.D.N.; Li, X.; Fu, J.; Chen, Y.; Chen, Q.; Miao, Y.; Hu, Z. Severity of androgenetic alopecia associated with poor sleeping habits and carnivorous eating and junk food consumption-A web-based investigation of male pattern hair loss in China. Dermatol. Ther. 2020, 33, e13273. [Google Scholar] [CrossRef]
- Paik, J.H.; Yoon, J.B.; Sim, W.Y.; Kim, B.S.; Kim, N.I. The prevalence and types of androgenetic alopecia in Korean men and women. Br. J. Dermatol. 2001, 145, 95–99. [Google Scholar] [CrossRef]
- Yang, C.C.; Hsieh, F.N.; Lin, L.Y.; Hsu, C.K.; Sheu, H.M.; Chen, W. Higher body mass index is associated with greater severity of alopecia in men with male-pattern androgenetic alopecia in Taiwan: A cross-sectional study. J. Am. Acad. Dermatol. 2014, 70, 297–302.e291. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Shi, Q.; Huang, Y.; Li, J.; Xie, H.; Liu, F. Relationship between the exercise and severity of androgenic alopecia. Zhong Nan Da Xue Xue Bao. Yi Xue Ban=J. Cent. South Univ. Med. Sci. 2021, 46, 725–730. [Google Scholar] [CrossRef]
- Finner, A.M. Nutrition and hair: Deficiencies and supplements. Dermatol. Clin. 2013, 31, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Su, L.H.; Chen, T.H. Association of androgenetic alopecia with smoking and its prevalence among Asian men: A community-based survey. Arch. Dermatol. 2007, 143, 1401–1406. [Google Scholar] [CrossRef] [Green Version]
- Sadgrove, N.J. The ‘bald’ phenotype (androgenetic alopecia) is caused by the high glycaemic, high cholesterol and low mineral ‘western diet’. Trends Food Sci. Technol. 2021, 116, 1170–1178. [Google Scholar] [CrossRef]
- Fortes, C.; Mastroeni, S.; Mannooranparampil, T.; Abeni, D.; Panebianco, A. Mediterranean diet: Fresh herbs and fresh vegetables decrease the risk of Androgenetic Alopecia in males. Arch. Dermatol. Res. 2018, 310, 71–76. [Google Scholar] [CrossRef]
- Tzima, N.; Pitsavos, C.; Panagiotakos, D.B.; Skoumas, J.; Zampelas, A.; Chrysohoou, C.; Stefanadis, C. Mediterranean diet and insulin sensitivity, lipid profile and blood pressure levels, in overweight and obese people; the Attica study. Lipids Health Dis. 2007, 6, 22. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.S.; Ro, B.I.; Hong, S.P.; Bak, H.; Sim, W.Y.; Kim, D.W.; Park, J.K.; Ihm, C.W.; Eun, H.C.; Kwon, O.S.; et al. A new classification of pattern hair loss that is universal for men and women: Basic and specific (BASP) classification. J. Am. Acad. Dermatol. 2007, 57, 37–46. [Google Scholar] [CrossRef]
- Figlak, K.; Paus, R.; Williams, G.; Philpott, M. 597 Outer root sheath is able to synthesise glycogen from lactate-investigating glycogen metabolism in human hair follicles. J. Investig. Dermatol. 2019, 139, S317. [Google Scholar] [CrossRef] [Green Version]
- Flores, A.; Schell, J.; Krall, A.S.; Jelinek, D.; Miranda, M.; Grigorian, M.; Braas, D.; White, A.C.; Zhou, J.L.; Graham, N.A.; et al. Lactate dehydrogenase activity drives hair follicle stem cell activation. Nat. Cell Biol. 2017, 19, 1017–1026. [Google Scholar] [CrossRef] [Green Version]
- Yao, Y.C.; Wu, X.Y. Survey of sugar-sweetened beverage consumption among a senior high school students in Hefei city. Anhui J. Prevent. Med. 2019, 25, 139–141. [Google Scholar]
- Mou, L.; Lei, Y.L.; Xiao, C.H.; Liu, H.Y.; Hu, Y.B.; Huang, M.; Ma, X. Current status and influencing factors of sugar-sweetened beverage intake among middle school students in Fushun County, Sichuan Province. Chin. J. Sch. Health 2020, 41, 779–782. [Google Scholar] [CrossRef]
- Pan, F.; Luan, D.C.; Zhang, D.W.; Mao, W.F.; Liang, D.; Liu, A.D.; Li, J.W. Assessment of sugar-sweetened beverages consumption and free sugar intake among urban residents aged 3 and above in China. Chin. J. Hydrog. 2022, 34, 126–130. [Google Scholar] [CrossRef]
- Rosinger, A.; Herrick, K.; Gahche, J.; Park, S. Sugar-sweetened Beverage Consumption among U.S. Youth, 2011–2014. NCHS Data Brief 2017, 271, 1–8. [Google Scholar]
- CNS. Chinese Dietary Guidelines (2016); People’s Medical Publishing House: Beijing, China, 2016. [Google Scholar]
- Valenzuela, M.J.; Waterhouse, B.; Aggarwal, V.R.; Bloor, K.; Doran, T. Effect of sugar-sweetened beverages on oral health: A systematic review and meta-analysis. Eur. J. Public Health 2021, 31, 122–129. [Google Scholar] [CrossRef]
- Bomback, A.S.; Derebail, V.K.; Shoham, D.A.; Anderson, C.A.; Steffen, L.M.; Rosamond, W.D.; Kshirsagar, A.V. Sugar-sweetened soda consumption, hyperuricemia, and kidney disease. Kidney Int. 2010, 77, 609–616. [Google Scholar] [CrossRef] [Green Version]
- Malik, V.S.; Hu, F.B. Fructose and Cardiometabolic Health: What the Evidence From Sugar-Sweetened Beverages Tells Us. J. Am. Coll. Cardiol. 2015, 66, 1615–1624. [Google Scholar] [CrossRef] [Green Version]
- Malik, V.S.; Hu, F.B. Sugar-Sweetened Beverages and Cardiometabolic Health: An Update of the Evidence. Nutrients 2019, 11, 1840. [Google Scholar] [CrossRef] [Green Version]
- Tan, S.; Pan, N.; Xu, X.; Li, H.; Lin, L.; Chen, J.; Jin, C.; Pan, S.; Jing, J.; Li, X. The association between sugar-sweetened beverages and milk intake with emotional and behavioral problems in children with autism spectrum disorder. Front. Nutr. 2022, 9, 927212. [Google Scholar] [CrossRef]
- Pabayo, R.; Dias, J.; Hemenway, D.; Molnar, B.E. Sweetened beverage consumption is a risk factor for depressive symptoms among adolescents living in Boston, Massachusetts, USA. Public Health Nutr. 2016, 19, 3062–3069. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.P.; Jia, C.X.; Li, S.X. Soft drink consumption and depressive symptoms among the adolescents of United States: The mediating role of aggressive behaviors. J. Affect. Disord. 2022, 315, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Kashino, I.; Kochi, T.; Imamura, F.; Eguchi, M.; Kuwahara, K.; Nanri, A.; Kurotani, K.; Akter, S.; Hu, H.; Miki, T.; et al. Prospective association of soft drink consumption with depressive symptoms. Nutrition 2021, 81, 110860. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Fulgoni, V.L.; Cowan, A.E.; Gaine, P.C. Sources of Added Sugars in Young Children, Adolescents, and Adults with Low and High Intakes of Added Sugars. Nutrients 2018, 10, 102. [Google Scholar] [CrossRef] [PubMed]
- Zhao, A.; Li, Z.; Ke, Y.; Huo, S.; Ma, Y.; Zhang, Y.; Zhang, J.; Ren, Z. Dietary Diversity among Chinese Residents during the COVID-19 Outbreak and Its Associated Factors. Nutrients 2020, 12, 1699. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Schumann, M.; Huang, T. Normal weight obesity and physical fitness in Chinese university students: An overlooked association. BMC Public Health 2018, 18, 1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.Z. Guidelines for the diagnosis and treatment of androgenetic alopecia in China. J. Clin. Dermatol. 2014, 43, 182–186. [Google Scholar] [CrossRef]
- Fausnacht, A.G.; Myers, E.A.; Hess, E.L.; Davy, B.M. Update of the BEVQ-15, a beverage intake questionnaire for habitual beverage intake for adults: Determining comparative validity and reproducibility. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2020, 33, 729–737. [Google Scholar] [CrossRef]
- Yan, X.; Xu, Y.; Huang, J.; Li, Y.; Li, Q.; Zheng, J.; Chen, Q.; Yang, W. Association of consumption of sugar-sweetened beverages with cognitive function among the adolescents aged 12-16 years in US, NHANES III, 1988–1994. Front. Nutr. 2022, 9, 939820. [Google Scholar] [CrossRef]
- Wang, S.S.; Lay, S.; Yu, H.N.; Shen, S.R. Dietary Guidelines for Chinese Residents (2016): Comments and comparisons. J. Zhejiang Univ. Sci. B 2016, 17, 649–656. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Dear, B.F.; Titov, N.; Sunderland, M.; McMillan, D.; Anderson, T.; Lorian, C.; Robinson, E. Psychometric comparison of the generalized anxiety disorder scale-7 and the Penn State Worry Questionnaire for measuring response during treatment of generalised anxiety disorder. Cogn. Behav. Ther. 2011, 40, 216–227. [Google Scholar] [CrossRef]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Swinson, R.P. The GAD-7 scale was accurate for diagnosing generalised anxiety disorder. Evid.-Based Med. 2006, 11, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.L.; Sun, X.G.; Han, Z.L.; Tao, J.; Zheng, L.R.; Li, L.J.; Gan, Z.Y.; Wen, S.L.; Shan, H.; Zhang, J.B. ROC curve analysis of optimal cutoff value of PTSD Checklist-Civilian Version for PTSD screening earl after earthquake. Chin. J. Behav. Med. Brain Sci. 2009, 10, 933–935. [Google Scholar]
- Textor, J.; Hardt, J.; Knüppel, S. DAGitty: A graphical tool for analyzing causal diagrams. Epidemiology 2011, 22, 745. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Miao, Y.Q. International experience of reducing sugar-sweetened beverage consumption and its implications for China. J. Food Saf. China 2020, 36, 51–54. [Google Scholar] [CrossRef]
- Gridsum. 2016 Beverage Industry Consumer Insights Report. 2016. Available online: https://max.book118.com/html/2017/0916/134154802.shtm (accessed on 24 November 2022).
- Jiang, Y.; Xu, T.; Dong, W.; Chu, C.; Zhou, M. Study on the death and disease burden caused by high sugar-sweetened beverages intake in China from 1990 to 2019. Eur. J. Public Health 2022, 32, 773–778. [Google Scholar] [CrossRef]
- Bhagavathula, A.S.; Rahmani, J.; Vidyasagar, K.; Tesfaye, W.; Khubchandani, J. Sweetened beverage consumption and risk of cardiovascular mortality: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2022, 16, 102462. [Google Scholar] [CrossRef]
- Malik, V.S.; Hu, F.B. The role of sugar-sweetened beverages in the global epidemics of obesity and chronic diseases. Nat. Rev. Endocrinol. 2022, 18, 205–218. [Google Scholar] [CrossRef]
- Çetinkaya, H.; Romaniuk, P. Relationship between consumption of soft and alcoholic drinks and oral health problems. Cent. Eur. J. Public Health 2020, 28, 94–102. [Google Scholar] [CrossRef]
- Brownbill, A.L.; Braunack-Mayer, A.J.; Miller, C.L. What makes a beverage healthy? A qualitative study of young adults’ conceptualisation of sugar-containing beverage healthfulness. Appetite 2020, 150, 104675. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.J.; Sánchez-Lozada, L.G.; Andrews, P.; Lanaspa, M.A. Perspective: A Historical and Scientific Perspective of Sugar and Its Relation with Obesity and Diabetes. Adv. Nutr. 2017, 8, 412–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, Y.C.; Sato, S.; Tsai, J.Y.; Yan, S.; Bakr, S.; Zhang, H.; Oates, P.J.; Ramasamy, R. Aldose reductase activation is a key component of myocardial response to ischemia. FASEB J. 2002, 16, 243–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macongonde, E.A.; Vilela, T.C.; Scaini, G.; Gonçalves, C.L.; Ferreira, B.K.; Costa, N.L.F.; De Oliveira, M.R.; Avila, S.; Streck, E.L.; Ferreira, G.C.; et al. Evaluation of the in vivo and in vitro effects of fructose on respiratory chain complexes in tissues of young rats. Dis. Markers 2015, 2015, 312530. [Google Scholar] [CrossRef]
- Morinaga, H.; Mohri, Y.; Grachtchouk, M.; Asakawa, K.; Matsumura, H.; Oshima, M.; Takayama, N.; Kato, T.; Nishimori, Y.; Sorimachi, Y.; et al. Obesity accelerates hair thinning by stem cell-centric converging mechanisms. Nature 2021, 595, 266–271. [Google Scholar] [CrossRef]
- Coogan, P.F.; Bethea, T.N.; Cozier, Y.C.; Bertrand, K.A.; Palmer, J.R.; Rosenberg, L.; Lenzy, Y. Association of type 2 diabetes with central-scalp hair loss in a large cohort study of African American women. Int. J. Womens Dermatol. 2019, 5, 261–266. [Google Scholar] [CrossRef]
- Arias-Santiago, S.; Gutiérrez-Salmerón, M.T.; Buendía-Eisman, A.; Girón-Prieto, M.S.; Naranjo-Sintes, R. Hypertension and aldosterone levels in women with early-onset androgenetic alopecia. Br. J. Dermatol. 2010, 162, 786–789. [Google Scholar] [CrossRef]
- Cakir, E. Is prediabetes risk factor for hair loss? Med. Hypotheses 2012, 79, 879. [Google Scholar] [CrossRef]
- Arias-Santiago, S.; Gutiérrez-Salmerón, M.T.; Buendía-Eisman, A.; Girón-Prieto, M.S.; Naranjo-Sintes, R. Sex hormone-binding globulin and risk of hyperglycemia in patients with androgenetic alopecia. J. Am. Acad. Dermatol. 2011, 65, 48–53. [Google Scholar] [CrossRef]
- Krysiak, R.; Kowalcze, K.; Okopień, B. The impact of exogenous vitamin D on thyroid autoimmunity in euthyroid men with autoimmune thyroiditis and early-onset androgenic alopecia. Pharmacol. Rep. 2021, 73, 1439–1447. [Google Scholar] [CrossRef]
- Deo, K.; Sharma, Y.K.; Wadhokar, M.; Tyagi, N. Clinicoepidemiological Observational Study of Acquired Alopecias in Females Correlating with Anemia and Thyroid Function. Dermatol. Res. Pract. 2016, 2016, 6279108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knüppel, A.; Shipley, M.J.; Llewellyn, C.H.; Brunner, E.J. Sugar intake from sweet food and beverages, common mental disorder and depression: Prospective findings from the Whitehall II study. Sci. Rep. 2017, 7, 6287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, D.; Cheng, L.; Jiang, W. Sugar-sweetened beverages consumption and the risk of depression: A meta-analysis of observational studies. J. Affect. Disord. 2019, 245, 348–355. [Google Scholar] [CrossRef]
- Kose, J.; Cheung, A.; Fezeu, L.K.; Péneau, S.; Debras, C.; Touvier, M. A Comparison of Sugar Intake between Individuals with High and Low Trait Anxiety: Results from the NutriNet-Santé Study. Nutrients 2021, 13, 1526. [Google Scholar] [CrossRef]
- Huang, C.H.; Fu, Y.; Chi, C.C. Health-Related Quality of Life, Depression, and Self-esteem in Patients With Androgenetic Alopecia: A Systematic Review and Meta-analysis. JAMA Dermatol. 2021, 157, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.X.; Tai, Y.H.; Chang, Y.T.; Chen, T.J.; Chen, M.H. Posttraumatic Stress Disorder and the Associated Risk of Autoimmune Skin Diseases: A Nationwide Population-Based Cohort Study. Psychosom. Med. 2021, 83, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Browne, J.; Morey, M.C.; Beckham, J.C.; Bosworth, H.B.; Porter Starr, K.N.; Bales, C.W.; McDermott, J.; Sloane, R.; Gregg, J.J.; Hall, K.S. Diet quality and exercise in older veterans with PTSD: A pilot study. Transl. Behav. Med. 2021, 11, 2116–2122. [Google Scholar] [CrossRef]
- Völker, J.M.; Koch, N.; Becker, M.; Klenk, A. Caffeine and Its Pharmacological Benefits in the Management of Androgenetic Alopecia: A Review. Ski. Pharmacol. Physiol. 2020, 33, 93–109. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall (n = 1028) | BASP | p-Value | ||
|---|---|---|---|---|---|
| Normal (n = 436) | MPHL (n = 592) | ||||
| Socio-demographic characteristics | |||||
| Age, year (M ± SD) | 27.8 (±7.2) | 26.5 (±6.5) | 28.7 (±7.5) | <0.001 | |
| BMI, n (%) | 0.094 | ||||
| <18.5 | 88 (8.6) | 40 (45.5) | 48 (54.5) | ||
| 18.5–23.9 | 678 (66.0) | 301 (44.4) | 377 (55.6) | ||
| 24–27.9 | 170 (16.5) | 58 (34.1) | 112 (65.9) | ||
| 28 or higher | 92 (8.9) | 37 (40.2) | 55 (59.8) | ||
| Education level, n (%) | 0.006 | ||||
| Senior high school and below | 298 (29.0) | 125 (41.9) | 173 (58.1) | ||
| Undergraduate | 616 (59.9) | 247 (40.1) | 369 (59.9) | ||
| Graduate and above | 114 (11.1) | 64 (56.1) | 50 (43.9) | ||
| Smoking status, n (%) | <0.001 | ||||
| never smoker | 485 (47.2) | 278 (57.3) | 207 (42.7) | ||
| former smoker | 219 (21.3) | 76 (34.7) | 143 (65.3) | ||
| current smoker | 324 (31.5) | 82 (25.3) | 242 (74.7) | ||
| Alcohol intake in past month, n (%) | <0.001 | ||||
| No | 515 (50.1) | 271 (52.6) | 244 (47.4) | ||
| Yes | 513 (49.9) | 165 (32.2) | 348 (67.8) | ||
| Weekly physical activity time, n (%) | 0.085 | ||||
| 0 | 197 (19.2) | 68 (34.5) | 129 (65.5) | ||
| 0–2.5 h | 124 (12.1) | 53 (42.7) | 71 (57.3) | ||
| 2.5–5 h | 263 (25.6) | 114 (43.3) | 149 (56.7) | ||
| more than 5 h | 444 (43.2) | 201 (45.3) | 243 (54.7) | ||
| Daily sleep time, n (%) | <0.001 | ||||
| 6 h or less | 140 (13.6) | 36 (25.7) | 104 (74.3) | ||
| more than 6 h | 888 (86.4) | 400 (45) | 488 (55) | ||
| MPHL related factors | |||||
| GAD-7, n (%) a | <0.001 | ||||
| 0–4 | 538 (52.3) | 294 (54.6) | 244 (45.4) | ||
| 5–9 | 259 (25.2) | 99 (38.2) | 160 (61.8) | ||
| 10–14 | 146 (14.2) | 35 (24) | 111 (76) | ||
| 15–21 | 85 (8.3) | 8 (9.4) | 77 (90.6) | ||
| PTSD, n (%) b | <0.001 | ||||
| No | 648 (63.0) | 353 (54.5) | 295 (45.5) | ||
| Yes | 380 (37.0) | 83 (21.8) | 297 (78.2) | ||
| Received clinical treatment of hair loss, n (%) | <0.001 | ||||
| No | 991 (96.4) | 435 (43.9) | 556 (56.1) | ||
| Yes | 37 (3.6) | 1 (2.7) | 36 (97.3) | ||
| Disease history, n (%) c | <0.001 | ||||
| No | 768 (74.7) | 392 (51) | 376 (49) | ||
| One chronic disease | 124 (12.1) | 28 (22.6) | 96 (77.4) | ||
| More than one disease | 136 (13.2) | 16 (11.8) | 120 (88.2) | ||
| Family history, n (%) d | <0.001 | ||||
| No | 812 (79.0) | 368 (45.3) | 444 (54.7) | ||
| Yes | 216 (21.0) | 68 (31.5) | 148 (68.5) | ||
| Hair dyeing/perming/bleaching/relaxing, n (%) | <0.001 | ||||
| No | 773 (75.2) | 393 (50.8) | 380 (49.2) | ||
| Yes | 255 (24.8) | 43 (16.9) | 212 (83.1) | ||
| Hair washing frequency, n (%) | 0.339 | ||||
| <3 times/week | 181 (17.6) | 71 (39.2) | 110 (60.8) | ||
| ≥3 times/week | 847 (82.4) | 365 (43.1) | 482 (56.9) | ||
| Characteristics | Overall (n = 1028) | BASP | p-Value | ||
|---|---|---|---|---|---|
| Normal (n = 436) | MPHL (n = 592) | ||||
| Consumption of cereals, n (%) | 0.079 | ||||
| never | 33 (3.2) | 19 (57.6) | 14 (42.4) | ||
| <3 times/week | 472 (45.9) | 190 (40.3) | 282 (59.7) | ||
| 4–6 times/week | 207 (20.1) | 81 (39.1) | 126 (60.9) | ||
| ≥7 times/week | 316 (30.7) | 146 (46.2) | 170 (53.8) | ||
| Consumption of roots and tubers, n (%) | 0.322 | ||||
| never | 120 (11.7) | 58 (48.3) | 62 (51.7) | ||
| <3 times/week | 637 (62.0) | 271 (42.5) | 366 (57.5) | ||
| 4–6 times/week | 176 (17.1) | 66 (37.5) | 110 (62.5) | ||
| ≥7 times/week | 95 (9.2) | 41 (43.2) | 54 (56.8) | ||
| Consumption of vegetables, n (%) | 0.001 | ||||
| <3 times/week | 457 (44.4) | 167 (36.5) | 290 (63.5) | ||
| 4–6 times/week | 241 (23.4) | 101 (41.9) | 140 (58.1) | ||
| ≥7 times/week | 330 (32.1) | 168 (50.9) | 162 (49.1) | ||
| Consumption of fruits, n (%) | 0.315 | ||||
| never | 41 (4.0) | 17 (41.5) | 24 (58.5) | ||
| <3 times/week | 489 (47.6) | 194 (39.7) | 295 (60.3) | ||
| 4–6 times/week | 194 (18.9) | 84 (43.3) | 110 (56.7) | ||
| ≥7 times/week | 304 (29.6) | 141 (46.4) | 163 (53.6) | ||
| Consumption of meat, poultry and offal, n (%) | <0.001 | ||||
| never | 88 (8.6) | 51 (58) | 37 (42) | ||
| <3 times/week | 471 (45.8) | 163 (34.6) | 308 (65.4) | ||
| 4–6 times/week | 225 (21.9) | 90 (40) | 135 (60) | ||
| ≥7 times/week | 244 (23.7) | 132 (54.1) | 112 (45.9) | ||
| Consumption of eggs, n (%) | 0.003 | ||||
| never | 38 (3.7) | 18 (47.4) | 20 (52.6) | ||
| <3 times/week | 523 (50.9) | 193 (36.9) | 330 (63.1) | ||
| 4–6 times/week | 211 (20.5) | 105 (49.8) | 106 (50.2) | ||
| ≥7 times/week | 256 (24.9) | 120 (46.9) | 136 (53.1) | ||
| Consumption of fish and seafoods, n (%) | 0.140 | ||||
| never | 192 (18.7) | 88 (45.8) | 104 (54.2) | ||
| <3 times/week | 705 (68.6) | 287 (40.7) | 418 (59.3) | ||
| 4–6 times/week | 101 (9.8) | 51 (50.5) | 50 (49.5) | ||
| ≥7 times/week | 30 (2.9) | 10 (33.3) | 20 (66.7) | ||
| Consumption of pulses, legumes, and nuts, n (%) | 0.004 | ||||
| never | 125 (12.2) | 71 (56.8) | 54 (43.2) | ||
| <3 times/week | 682 (66.3) | 272 (39.9) | 410 (60.1) | ||
| 4–6 times/week | 151 (14.7) | 60 (39.7) | 91 (60.3) | ||
| ≥7 times/week | 70 (6.8) | 33 (47.1) | 37 (52.9) | ||
| Consumption of oils and fats, n (%) | 0.002 | ||||
| never | 165 (16.1) | 87 (52.7) | 78 (47.3) | ||
| <3 times/week | 503 (48.9) | 189 (37.6) | 314 (62.4) | ||
| 4–6 times/week | 139 (13.5) | 55 (39.6) | 84 (60.4) | ||
| ≥7 times/week | 221 (21.5) | 105 (47.5) | 116 (52.5) | ||
| Consumption of deep-fried food, n (%) | <0.001 | ||||
| never | 249 (24.2) | 134 (53.8) | 115 (46.2) | ||
| <3 times/week | 634 (61.7) | 263 (41.5) | 371 (58.5) | ||
| 4–6 times/week | 120 (11.7) | 33 (27.5) | 87 (72.5) | ||
| ≥7 times/week | 25 (2.4) | 6 (24) | 19 (76) | ||
| Consumption of sugar and honey, n (%) | 0.001 | ||||
| never | 332 (32.3) | 170 (51.2) | 162 (48.8) | ||
| <3 times/week | 542 (52.7) | 210 (38.7) | 332 (61.3) | ||
| 4–6 times/week | 118 (11.5) | 43 (36.4) | 75 (63.6) | ||
| ≥7 times/week | 36 (3.5) | 13 (36.1) | 23 (63.9) | ||
| Consumption of sweets and ice cream, n (%) | 0.002 | ||||
| never | 264 (25.7) | 137 (51.9) | 127 (48.1) | ||
| <3 times/week | 613 (59.6) | 247 (40.3) | 366 (59.7) | ||
| 4–6 times/week | 117 (11.4) | 40 (34.2) | 77 (65.8) | ||
| ≥7 times/week | 34 (3.3) | 12 (35.3) | 22 (64.7) | ||
| Characteristics | Overall (n = 1028) | BASP | p-Value | ||
|---|---|---|---|---|---|
| Normal | MPHL | ||||
| SSB intake frequency, n (%) | <0.001 | ||||
| Never | 121 (11.8) | 73 (60.3) | 48 (39.7) | ||
| 1–3 times per week | 190 (18.5) | 103 (54.2) | 87 (45.8) | ||
| 4–7 times per week | 258 (25.1) | 117 (45.3) | 141 (54.7) | ||
| more than 7 times per week | 459 (44.6) | 143 (31.2) | 316 (68.8) | ||
| SSB intake amount, n (%) a | <0.001 | ||||
| Never | 121 (11.8) | 73 (60.3) | 48 (39.7) | ||
| Small amount | 368 (35.8) | 169 (45.9) | 199 (54.1) | ||
| Middle amount | 290 (28.2) | 119 (41.0) | 171 (59.0) | ||
| Large amount | 249 (24.2) | 75 (30.1) | 174 (69.9) | ||
| MPHL/All Cases | Model 1 a | Model 2 b | Model 3 c | Model 4 d | ||
|---|---|---|---|---|---|---|
| SSB intake frequency | ||||||
| Never | 48/121 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | |
| 1–3 times per week | 87/190 | 1.28 [0.81,2.04] | 1.13 [0.68,1.88] | 1.15 [0.68,1.93] | 1.21 [0.71,2.06] | |
| 4–7 times per week | 141/258 | 1.83 [1.18,2.84] | 1.56 [0.96,2.54] | 1.33 [0.80,2.23] | 1.26 [0.74,2.12] | |
| >7 times per week | 316/459 | 3.36 [2.22,5.09] | 2.03 [1.26,3.27] | 1.78 [1.07,2.95] | 1.57 [0.94,2.64] | |
| SSB intake amount | ||||||
| Never | 48/121 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) | |
| Small amount | 199/368 | 1.79 [1.18,2.72] | 1.44 [0.91,2.29] | 1.32 [0.81,2.13] | 1.34 [0.82,2.19] | |
| Middle amount | 171/290 | 2.19 [1.42,3.37] | 1.66 [1.02,2.71] | 1.43 [0.85,2.39] | 1.35 [0.80,2.27] | |
| Large amount | 174/249 | 3.53 [2.24,5.55] | 1.78 [1.06,2.98] | 1.58 [0.92,2.74] | 1.33 [0.76,2.32] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, X.; Tuan, H.; Na, X.; Yang, H.; Yang, Y.; Zhang, Y.; Xi, M.; Tan, Y.; Yang, C.; Zhang, J.; et al. The Association between Sugar-Sweetened Beverages and Male Pattern Hair Loss in Young Men. Nutrients 2023, 15, 214. https://doi.org/10.3390/nu15010214
Shi X, Tuan H, Na X, Yang H, Yang Y, Zhang Y, Xi M, Tan Y, Yang C, Zhang J, et al. The Association between Sugar-Sweetened Beverages and Male Pattern Hair Loss in Young Men. Nutrients. 2023; 15(1):214. https://doi.org/10.3390/nu15010214
Chicago/Turabian StyleShi, Xiaojin, Hsiaohan Tuan, Xiaona Na, Haibing Yang, Yucheng Yang, Yulin Zhang, Menglu Xi, Yuefeng Tan, Celi Yang, Junhan Zhang, and et al. 2023. "The Association between Sugar-Sweetened Beverages and Male Pattern Hair Loss in Young Men" Nutrients 15, no. 1: 214. https://doi.org/10.3390/nu15010214