
Implementing a Community-Based Initiative to Improve Nutritional Intake among Home-Delivered Meal Recipients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
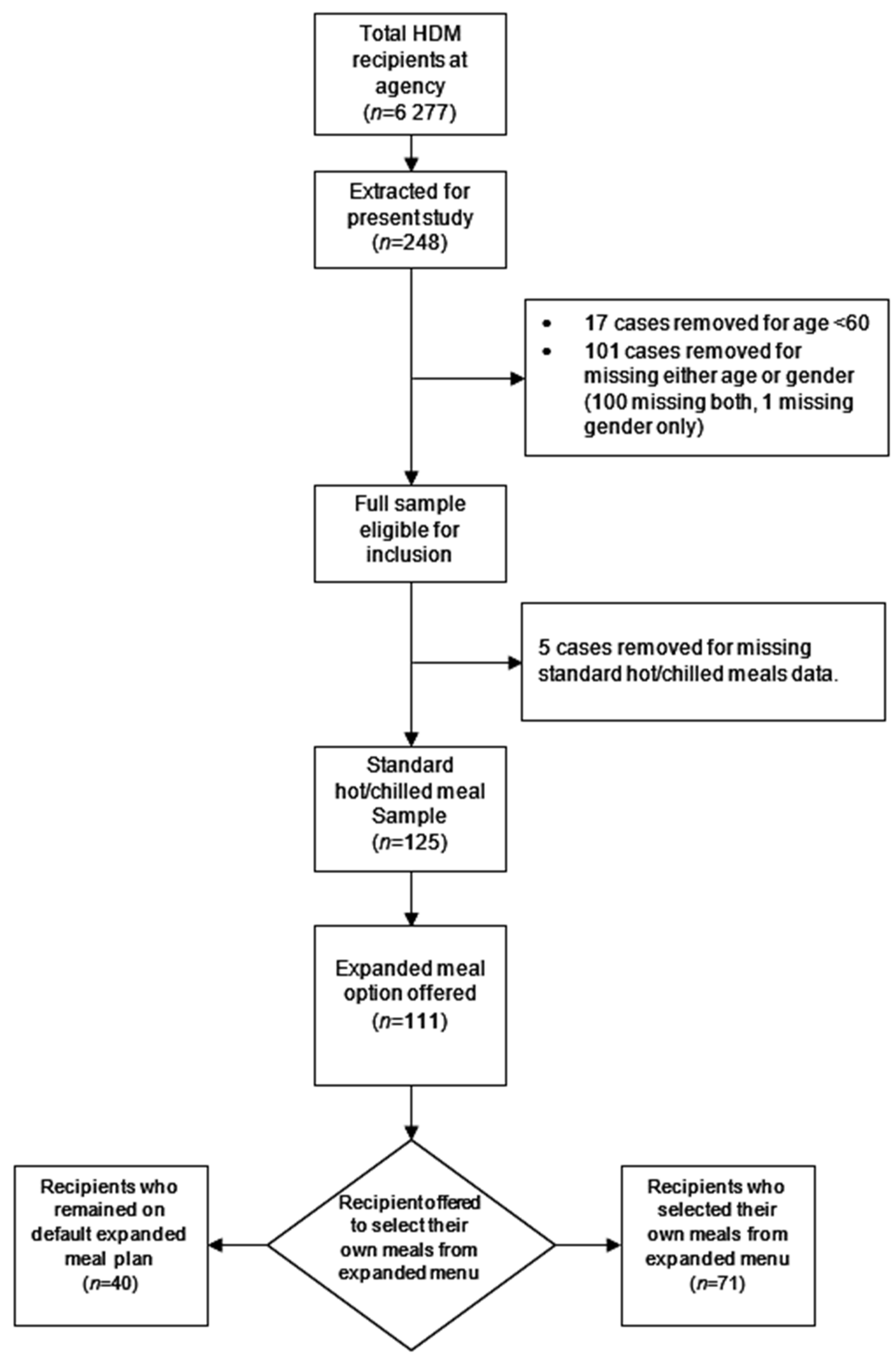
2.2. Design and Participants
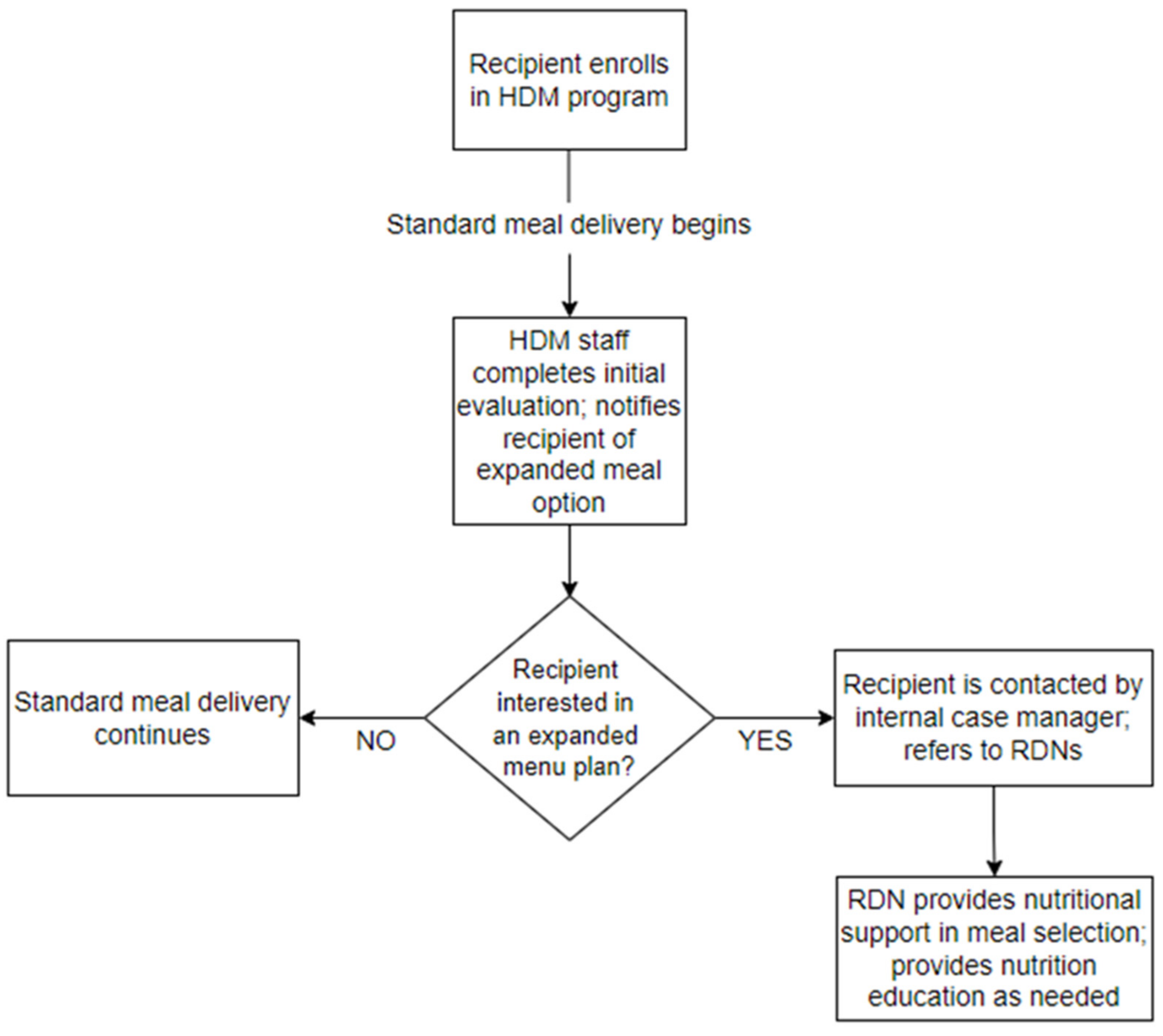
2.3. Expanded Meal Plan
2.4. Data Sources
2.5. Calculation of Nutrition Content of Meals
2.6. Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lloyd, J.L.; Wellman, N.S. Older Americans Act Nutrition Programs: A Community-Based Nutrition Program Helping Older Adults Remain at Home. J. Nutr. Gerontol. Geriatr. 2015, 34, 90–109. [Google Scholar] [CrossRef]
- Administration for Community Living. Older Americans Act Nutrition Programs. 2014. Available online: https://acl.gov/sites/default/files/news%202017-03/OAA-Nutrition_Programs_Fact_Sheet.pdf (accessed on 20 December 2021).
- Wright, L.; Vance, L.; Sudduth, C.; Epps, J.B. The Impact of a Home-Delivered Meal Program on Nutritional Risk, Dietary Intake, Food Security, Loneliness, and Social Well-Being. J. Nutr. Gerontol. Geriatr. 2015, 34, 218–227. [Google Scholar] [CrossRef]
- Thomas, K.S.; Mor, V. Providing More Home-Delivered Meals Is One Way to Keep Older Adults with Low Care Needs out of Nursing Homes. Health Aff. 2013, 32, 1796–1802. [Google Scholar] [CrossRef] [Green Version]
- Thomas, K.S.; Akobundu, U.; Dosa, D. More than a Meal? A Randomized Control Trial Comparing the Effects of Home-Delivered Meals Programs on Participants’ Feelings of Loneliness. J. Gerontol. B Psychol. Sci. Soc. Sci. 2016, 71, 1049–1058. [Google Scholar] [CrossRef] [Green Version]
- Choi, N.G.; Sullivan, J.E.; Marti, C.N. Low-income Homebound Older Adults Receiving Home-delivered Meals: Physical and Mental Health Conditions, Incidence of Falls and Hospitalisations. Health Soc. Care Community 2019, 27, e406–e416. [Google Scholar] [CrossRef]
- Administration for Community Living. 2019 Home Delivered Meals. 2019. Available online: https://agid.acl.gov/DataFiles/NPS/Files.aspx?year=2019&serviceid=4.Codebook_Home_Meals_2019.Pdf. (accessed on 20 December 2021).
- Juckett, L.A.; Bunger, A.C.; Bunck, L.; Balog, E.J. Evaluating the Implementation of Fall Risk Management Practices within Home-Delivered Meal Organizations. J. Gerontol. Soc. Work 2021, 64, 372–387. [Google Scholar] [CrossRef]
- Sabbouh, T.; Torbey, M.T. Malnutrition in Stroke Patients: Risk Factors, Assessment, and Management. Neurocrit. Care 2018, 29, 374–384. [Google Scholar] [CrossRef]
- Tamura, Y.; Omura, T.; Toyoshima, K.; Araki, A. Nutrition Management in Older Adults with Diabetes: A Review on the Importance of Shifting Prevention Strategies from Metabolic Syndrome to Frailty. Nutrients 2020, 12, 3367. [Google Scholar] [CrossRef]
- Lai, S.; Amabile, M.I.; Altieri, S.; Mastroluca, D.; Lai, C.; Aceto, P.; Crudo, M.; D’Angelo, A.R.; Muscaritoli, M.; Molfino, A. Effect of Underlying Renal Disease on Nutritional and Metabolic Profile of Older Adults with Reduced Renal Function. Front. Nutr. 2017, 4, 44. [Google Scholar] [CrossRef]
- Douglas, B.M.; Howard, E.P. Predictors of Self-Management Behaviors in Older Adults with Hypertension. Adv. Prev. Med. 2015, 2015, e960263. [Google Scholar] [CrossRef] [Green Version]
- Bustillos, B.D.; Sharkey, J.R. “I Try to Keep That Sugar Down”. Experiences of Homebound Older Adults with Type 2 Diabetes: Barriers to Self-Management. J. Nutr. Gerontol. Geriatr. 2020, 39, 69–87. [Google Scholar] [CrossRef]
- Fleury, S.; Van Wymelbeke-Delannoy, V.; Lesourd, B.; Tronchon, P.; Maître, I.; Sulmont-Rossé, C. Home-Delivered Meals: Characterization of Food Intake in Elderly Beneficiaries. Nutrients 2021, 13, 2064. [Google Scholar] [CrossRef]
- Meals on Wheels America. COVID-19 and Older Adults: Research Findings and Implications for Meals on Wheels. 2021. Available online: https://Meals-on-Wheels-Covid-19-Strategic-Research_final-Report_09-20-21.Pdf (accessed on 30 December 2021).
- Hollis, J.H.; Henry, C.J.K. Dietary Variety and Its Effect on Food Intake of Elderly Adults. J. Hum. Nutr. Diet 2007, 20, 345–351. [Google Scholar] [CrossRef]
- Whitelock, E.; Ensaff, H. On Your Own: Older Adults’ Food Choice and Dietary Habits. Nutrients 2018, 10, 413. [Google Scholar] [CrossRef] [Green Version]
- Academy of Nutrition and Dietetics. RDN and NDTR Overview. 2021. Available online: https://www.eatrightpro.org/about-us/what-is-an-rdn-and-dtr/rdn-and-ndtr-overview (accessed on 20 December 2021).
- Moloney, L.; Jarrett, B. Nutrition Assessment and Interventions for the Prevention and Treatment of Malnutrition in Older Adults: An Evidence Analysis Center Scoping Review. J. Acad. Nutr. Diet. 2021, 121, 2108. [Google Scholar] [CrossRef]
- Gergerich, E.; Shobe, M.; Christy, K. Sustaining Our Nation’s Seniors through Federal Food and Nutrition Programs. J. Nutr. Gerontol. Geriat 2015, 34, 273–291. [Google Scholar] [CrossRef]
- Juckett, L.A.; Lee, K.; Bunger, A.C.; Brostow, D.P. Implementing Nutrition Education Programs in Congregate Dining Service Settings: A Scoping Review. Gerontologist 2020, 62, e82–e96. [Google Scholar] [CrossRef]
- Administration for Community Living. Projected Future Growth of Older Population. 2021. Available online: https://acl.gov/aging-and-disability-in-america/data-and-research/projected-future-growth-older-population (accessed on 30 December 2021).
- Vincent, G.K.; Velkoff, V.A. The Next Four Decades—The Older Population in the United States: 2010 to 2050. 2010. Available online: https://www.census.gov/prod/2010pubs/p25-1138.pdf (accessed on 20 December 2021).
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in Development of the Index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living1. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Sinnett, S. The Ability of the Nutrition Screening Initiative Determine Checklist to Evaluate the Nutrition Risk Status of Older Georgians. Ph.D. Thesis, University of Georgia, Athens, GA, USA, 2009. [Google Scholar]
- Norman, K.; Haß, U.; Pirlich, M. Malnutrition in Older Adults—Recent Advances and Remaining Challenges. Nutrients 2021, 13, 2764. [Google Scholar] [CrossRef]
- Walton, K.; Charlton, K.E.; Manning, F.; McMahon, A.T.; Galea, S.; Evans, K. The Nutritional Status and Energy and Protein Intakes of MOW Clients and the Need for Further Targeted Strategies to Enhance Intakes. Appetite 2015, 95, 528–532. [Google Scholar] [CrossRef] [Green Version]
- Crichton, M.; Craven, D.; Mackay, H.; Marx, W.; de van der Schueren, M.; Marshall, S. A Systematic Review, Meta-Analysis and Meta-Regression of the Prevalence of Protein-Energy Malnutrition: Associations with Geographical Region and Sex. Age Ageing 2019, 48, 38–48. [Google Scholar] [CrossRef]
- Kramer, H. Diet and Chronic Kidney Disease. Adv. Nutr. 2019, 10, S367–S379. [Google Scholar] [CrossRef]
- Casas, R.; Castro-Barquero, S.; Estruch, R.; Sacanella, E. Nutrition and Cardiovascular Health. Int. J. Mol. Sci. 2018, 19, 3988. [Google Scholar] [CrossRef] [Green Version]
- Thomas, K.S.; Gadbois, E.A.; Shield, R.R.; Akobundu, U.; Morris, A.M.; Dosa, D.M. “It’s Not Just a Simple Meal. It’s So Much More”: Interactions between Meals on Wheels Clients and Drivers. J. Appl. Gerontol. 2020, 39, 151–158. [Google Scholar] [CrossRef]
- Meals on Wheels America. Dispelling Myths: Supporting Public Policy for Greater Impact and Sustainability. 2016. Available online: https://www.mealsonwheelsamerica.org/docs/default-source/membership/executive-summary-2016-final.pdf?sfvrsn=2 (accessed on 28 January 2022).
- Shan, M.; Gutman, R.; Dosa, D.; Gozalo, P.L.; Ogarek, J.A.; Kler, S.; Thomas, K.S. A New Data Resource to Examine Meals on Wheels Clients’ Health Care Utilization and Costs. Med. Care 2019, 57, e15–e21. [Google Scholar] [CrossRef]
- De Boer, I.H.; DCCT/EDIC Research Group. Kidney Disease and Related Findings in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study. Diabetes Care 2014, 37, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Colello, K.J.; Sussman, J.S. Older Americans Act: 2020 Reauthorization. 2020. Available online: https://crsreports.congress.gov/product/pdf/R/R46439 (accessed on 30 January 2022).
- Juckett, L.A.; Bunck, L.; Thomas, K.S. The Older Americans Act 2020 Reauthorization: Overcoming Barriers to Service and Program Implementation. Public Policy Aging Rep. 2021, 32, 25–30. [Google Scholar] [CrossRef]
- Ahn, M.; Kwon, H.J.; Kang, J. Supporting Aging-in-Place Well: Findings from a Cluster Analysis of the Reasons for Aging-in-Place and Perceptions of Well-Being. J. Appl. Gerontol. 2017, 9, 3–15. [Google Scholar] [CrossRef]
- Leung, C.W.; Wolfson, J.A. Food Insecurity among Older Adults: 10-Year National Trends and Associations with Diet Quality. J. Am. Geriatr. Soc. 2021, 69, 964–971. [Google Scholar] [CrossRef]
- Juckett, L.A.; Robinson, M.L. The Occupational Therapy Approach to Addressing Food Insecurity among Older Adults with Chronic Disease. Geriatrics 2019, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Dobrow, L.; Estrada, I.; Burkholder-Cooley, N.; Miklavcic, J. Potential Effectiveness of Registered Dietitian Nutritionists in Healthy Behavior Interventions for Managing Type 2 Diabetes in Older Adults: A Systematic Review. Front. Nutr. 2022, 8, 737410. [Google Scholar] [CrossRef]
- Reckrey, J.M.; Morrison, R.S.; Boerner, K.; Szanton, S.L.; Bollens-Lund, E.; Leff, B.; Ornstein, K.A. Living in the Community With Dementia: Who Receives Paid Care? J. Am. Geriatr. Soc. 2020, 68, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Guo, J.; Hu, L.; Veronese, N.; Smith, L.; Yang, L.; Cao, C. Association between Intake of Energy and Macronutrients and Memory Impairment Severity in US Older Adults, National Health and Nutrition Examination Survey 2011-2014. Nutrients 2020, 12, 3559. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.; Guerchet, M.; Prina, M. The Global Impact of Dementia 2013–2050. Alzheimer’s Disease International. 2013. Available online: http://www.alz.co.uk/research/G8-policy-brief (accessed on 12 February 2022).
- Sadarangani, T.R.; Beasley, J.M.; Yi, S.; Chodosh, J.; Freedman, M.L. Enriching Nutrition Programs to Better Serve the Needs of a Diversifying Aging Population. Fam. Community Health 2020, 43, 100–105. [Google Scholar] [CrossRef]
- Zielinskie, G.; Samuel, L.J.; Szanton, S.; Health Affairs Forefront. To Improve Health and Reduce Costs for Low-Income Seniors, Invest Upstream. 2017. Available online: https://www.healthaffairs.org/do/10.1377/forefront.20171024.786928/full/ (accessed on 30 December 2021).
- Kilbourne, A.M.; Switzer, G.; Hyman, K.; Crowley-Matoka, M.; Fine, M.J. Advancing Health Disparities Research within the Health Care System: A Conceptual Framework. Am. J. Public Health 2006, 96, 2113–2121. [Google Scholar] [CrossRef]
- Agency for Healthcare Quality and Research. 2016 National Healthcare Quality and Disparities Report. 2016. Available online: https://www.ahrq.gov/research/findings/nhqrdr/nhqdr16/index.html (accessed on 20 December 2021).
- Woodward, E.N.; Matthieu, M.M.; Uchendu, U.S.; Rogal, S.; Kirchner, J.E. The Health Equity Implementation Framework: Proposal and Preliminary Study of Hepatitis C Virus Treatment. Implement. Sci. 2019, 14, 26. [Google Scholar] [CrossRef] [Green Version]
- U.S Centers for Disease Control and Prevention. CDC Health Disparities & Inequalities Report (CHDIR)—Minority Health. 2020. Available online: https://www.cdc.gov/minorityhealth/CHDIReport.html (accessed on 20 December 2021).
- Gundersen, C.; Ziliak, J.P. Food Insecurity and Health Outcomes. Health Aff. 2015, 34, 1830–1839. [Google Scholar] [CrossRef] [Green Version]
- Rabaut, L.J. Medically Tailored Meals as a Prescription for Treatment of Food-Insecure Type 2 Diabetics. J. Patient Cent. Res. Rev. 2019, 6, 179–183. [Google Scholar] [CrossRef] [Green Version]
- New England Journal of Medicine Catalyst Group. What Is Value-Based Healthcare? 2017. Available online: https://catalyst.nejm.org/doi/full/10.1056/CAT.17.0558 (accessed on 20 December 2021).
- Centers for Medicare and Medicaid. CMS’ Value-Based Programs. 2021. Available online: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/Value-Based-Programs (accessed on 30 December 2021).
- Berkowitz, S.A.; Terranova, J.; Hill, C.; Ajayi, T.; Linsky, T.; Tishler, L.W.; DeWalt, D.A. Meal Delivery Programs Reduce The Use of Costly Health Care in Dually Eligible Medicare And Medicaid Beneficiaries. Health Aff. 2018, 37, 535–542. [Google Scholar] [CrossRef]
- Morris, J.N.; Howard, E.P.; Steel, K.R. Development of the InterRAI Home Care Frailty Scale. BMC Geriatr. 2016, 16, 188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fund, J. Columbus, Ohio, Is America’s Test Market. 2018. Available online: https://www.nationalreview.com/2018/08/columbus-ohio-special-election-test-market-for-midterms/ (accessed on 4 February 2022).
- Smith, T. Columbus, Ohio: Test Market of the USA. 2012. Available online: https://www.cbsnews.com/news/columbus-ohio-test-market-of-the-usa/ (accessed on 4 February 2022).



{kind=link}
{kind=link}
| Full Sample | Standard Plan | Expanded Plan | ||||
|---|---|---|---|---|---|---|
| Characteristics | n | Mean (SD, Range) | n | Mean (SD, Range) | n | Mean (SD, Range) |
| Age (years) | 130 | 74.8 (10.7, 41) | 125 | 74.7 (10.7, 41) | 111 | 74.7 (10.8, 41) |
| Monthly income (USD) | 68 | 1436.3 (1043.7, 7500) | 66 | 1437.6 (1054.2, 7500) | 59 | 1469.5 (1107.4, 7500) |
| Activities of Daily Living (ADL) score | 95 | 3.9 (4.6, 16) | 91 | 3.7 (4.4, 16) | 82 | 3.7 (4.4, 16) |
| Instrumental Activities of Daily Living (IADL) score | 95 | 10.1 (7.2, 23) | 91 | 10 (7.2, 23) | 82 | 10 (7, 23) |
| Nutrition risk assessment (NRA) score | 95 | 8.3 (4, 21) | 91 | 8.2 (4, 21) | 82 | 8.3 (4, 21) |
| Number of medical conditions | 130 | 2.8 (1.6, 7) | 125 | 2.9 (1.6, 7) | 111 | 2.9 (1.6, 7) |
| Nutrients | Monthly Income (USD) | p-Value * | ||
|---|---|---|---|---|
| <2500 | 2500–5000 | >5000 | ||
| Protein (g) | 29 | 29 | 19 | <0.001 |
| Sodium (Na) (mg) | 811 | 803 | 574 | <0.001 |
| Fat (g) | 18 | 18 | 12 | <0.001 |
| Cholesterol (CHO) (mg) | 68 | 68 | 42 | <0.001 |
| Calories (kcal) | 555 | 554 | 360 | <0.001 |
| Potassium (K) (mg) | 1019 | 1024 | 649 | <0.001 |
| Nutrients | Standard Hot/Chilled | Default Expanded | Default—Standard | |||
|---|---|---|---|---|---|---|
| n | Mean (SD, Range) | n | Mean (SD, Range) | n | Mean (SD, Range) | |
| Protein (g) | 125 | 28.9 (1.2, 11.1) | 111 | 25.5 (3.9, 19.2) | 111 | −3.4 (3.8, 17.1) |
| Sodium (Na) (mg) | 125 | 801.5 (54.6, 487.8) | 111 | 734.3 (144.7, 852.4) | 111 | −67.1 (138.8, 852.4) |
| Fat (g) | 125 | 17.6 (1.3, 11.5) | 111 | 15.7 (3.4, 20.1) | 111 | −1.9 (3.4, 20.1) |
| Cholesterol (CHO) (mg) | 125 | 67.2 (5.6, 42.40) | 111 | 53.3 (13.5, 50.8) | 111 | −15.9 (13.8, 57.7) |
| Calories (kcal) | 125 | 548.5 (35.3, 272.4) | 111 | 461.4 (86.5, 295.6) | 111 | −86.4 (88.7, 303.6) |
| Potassium (K) (mg) | 125 | 1009.1 (77.3, 603.4) | 111 | 776.2 (212.4, 797.3) | 111 | −231 (216.5, 797.3) |
| Recipients Who Remained on Default Expanded Meals | Recipients Who Selected Their Own Expanded Meals | Difference | ||||
|---|---|---|---|---|---|---|
| n | Mean (SD, Range) | n | Mean (SD, Range) | Mean (SD, Range) | p-Value | |
| Protein (g) | 40 | 28.5 (2.1, 11.1) | 71 | 23.8 (3.6, 19.2) | −5.3 (3.6, 17.1) | <0.001 |
| Sodium (Na) mg | 40 | 789.1 (86.5, 487.8) | 71 | 703.4 (161.4, 852.4) | −104.9 (162, 852.4) | <0.001 |
| Fat g | 40 | 17.2 (1.8, 8.6) | 71 | 14.9 (3.8, 20.1) | −2.9 (3.9, 20.1) | <0.001 |
| Cholesterol (CHO) (mg) | 40 | 64.8 (9.2, 42.4) | 71 | 46.9 (11, 50.8) | −21.5 (11.3, 57.7) | <0.001 |
| Calories (kcal) | 40 | 532.7 (57.4, 232.5) | 71 | 421.2 (73.4, 295.6) | −135 (75.6, 303.6) | <0.001 |
| Potassium (K) (mg) | 40 | 975.6 (131.3, 603.4) | 71 | 663.8 (160.5, 797.3) | −361.2 (161.1, 797.3) | <0.001 |
| Recipients Who Remained on Default Expanded Meals | Recipients Who Selected Their Own Expanded Meals | ||||||
|---|---|---|---|---|---|---|---|
| n | Proportion | Std. Dev. | n | Proportion | Std. Dev. | p-Value | |
| Cardiac disorder | 40 | 0.1 | 0.304 | 71 | 0.282 | 0.453 | 0.0132 |
| Renal disorder | 40 | 0.05 | 0.221 | 71 | 0.197 | 0.401 | 0.0141 |
| Thyroid disorder | 40 | 0 | 0 | 71 | 0.085 | 0.28 | 0.0132 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juckett, L.A.; Hariharan, G.; Dodonova, D.C.; Klaus, J.; Rowe, M.; Burak, E.; Mason, B.; Bunck, L. Implementing a Community-Based Initiative to Improve Nutritional Intake among Home-Delivered Meal Recipients. Nutrients 2022, 14, 944. https://doi.org/10.3390/nu14050944
Juckett LA, Hariharan G, Dodonova DC, Klaus J, Rowe M, Burak E, Mason B, Bunck L. Implementing a Community-Based Initiative to Improve Nutritional Intake among Home-Delivered Meal Recipients. Nutrients. 2022; 14(5):944. https://doi.org/10.3390/nu14050944
Chicago/Turabian StyleJuckett, Lisa A., Govind Hariharan, Dimitri Camargo Dodonova, Jared Klaus, Melinda Rowe, Elana Burak, Benetta Mason, and Leah Bunck. 2022. "Implementing a Community-Based Initiative to Improve Nutritional Intake among Home-Delivered Meal Recipients" Nutrients 14, no. 5: 944. https://doi.org/10.3390/nu14050944