
Obesity in Caucasian Seniors on the Rise: Is It Truly Harmful? Results of the PolSenior2 Study
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Activities of Daily Living and the Mini-Mental State Examination
2.3. Statistical Analysis
3. Results
3.1. Frequency of General Obesity and Abdominal Obesity
3.2. Association of the Body Measurements with the Physical and Cognitive Performance
3.3. Association of the Body Measurements with Morbidity
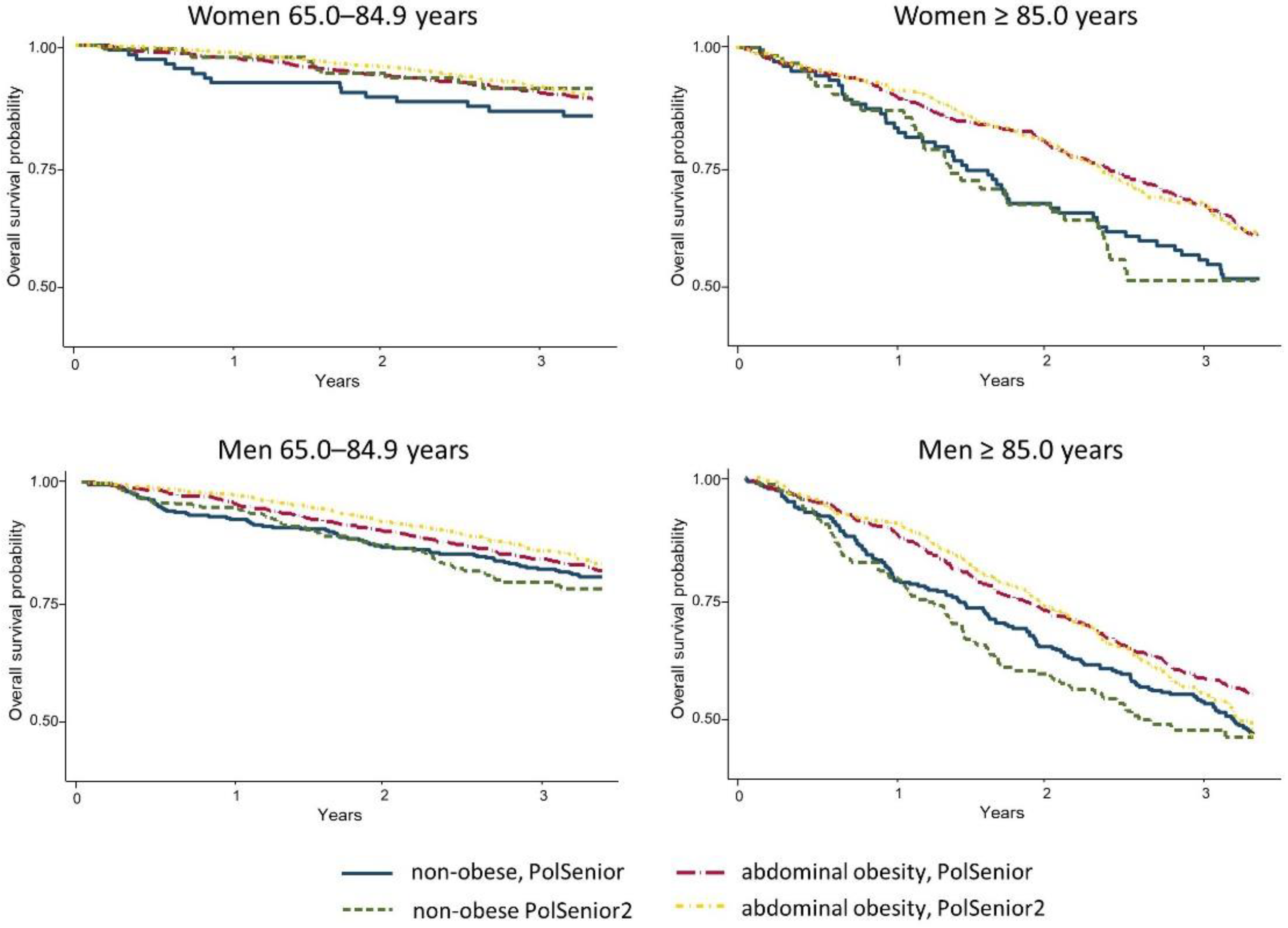
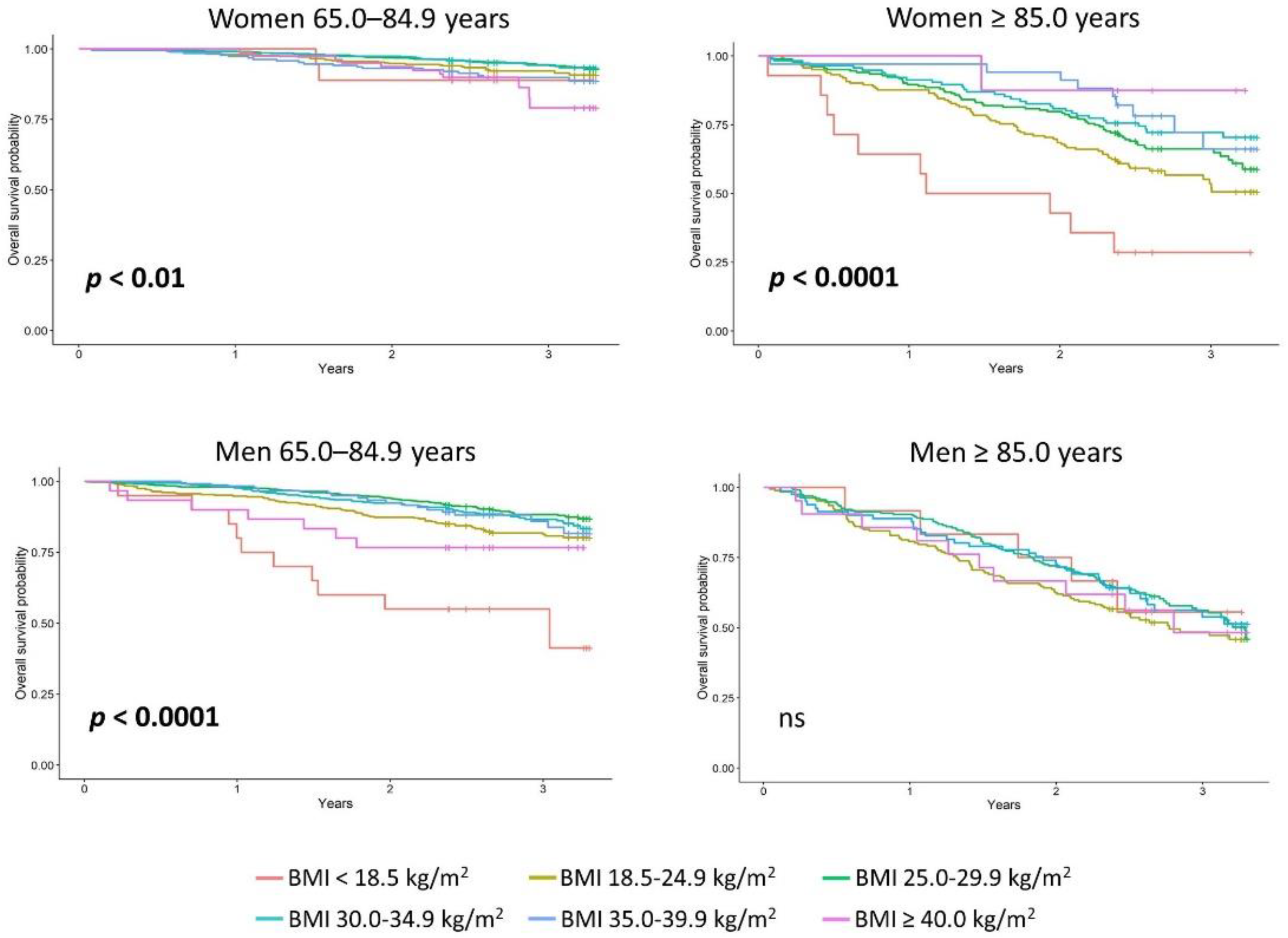
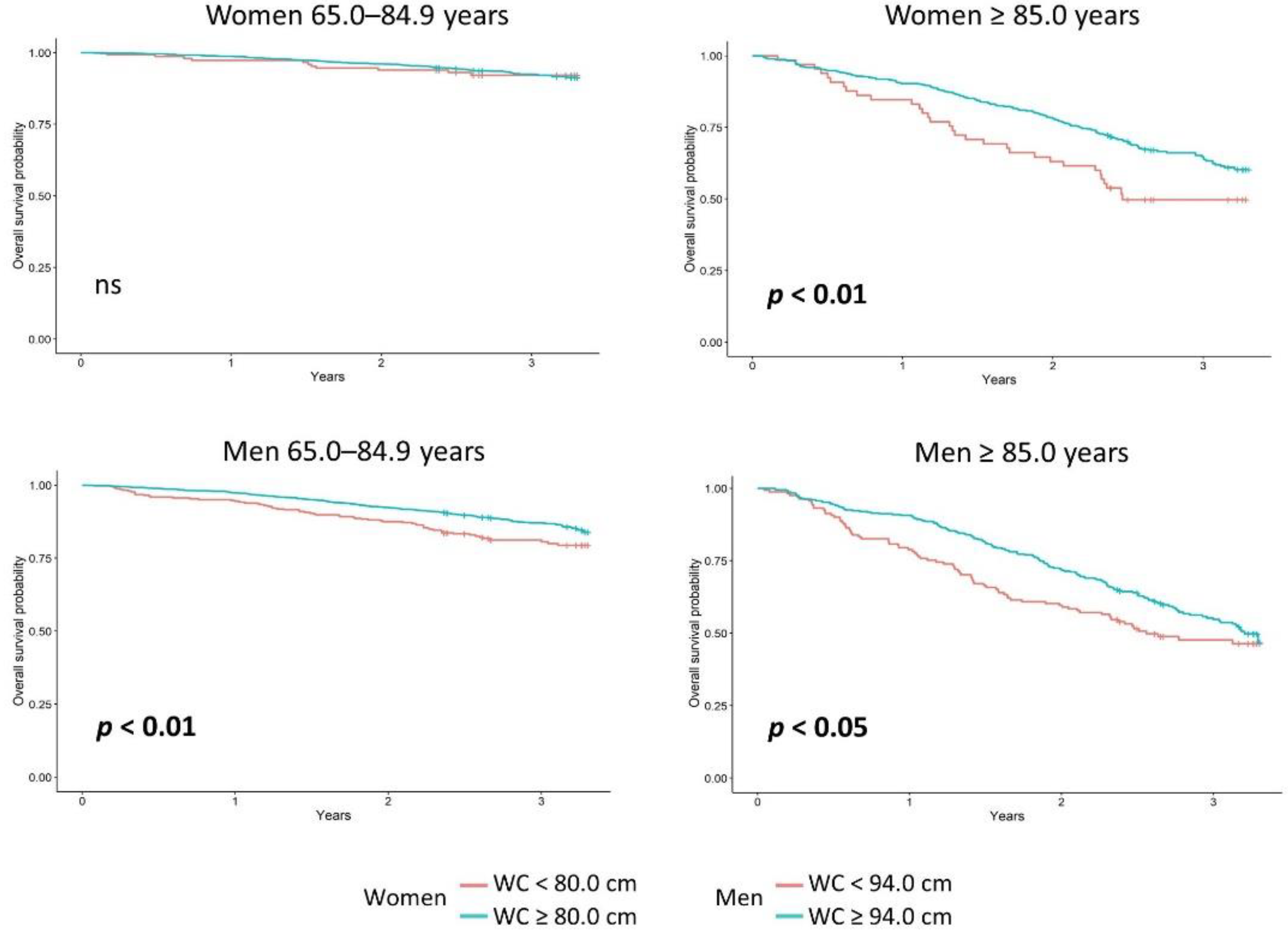
3.4. Association of the Body Measurements with Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eurostat. Ageing Europe—Looking at the Lives of Older People in the EU—2020 Edition; Publications Office of the European Union: Luxembourg, 2020. [Google Scholar] [CrossRef]
- National Institute of Population and Social Security Research. Population Projections for Japan (2017): 2016 to 2065. Available online: https://www.ipss.go.jp/pp-zenkoku/e/zenkoku_e2017/pp29_summary.pdf (accessed on 10 September 2022).
- Vespa, J.; Medina, L.; Armstrong, D.M. Demographic Turning Points for the United States: Population Projections for 2020 to 2060. Population Estimates and Projections; Current Population Reports, P25-1144; U.S. Census Bureau: Washington, DC, USA, 2020. Available online: https://www.census.gov/content/dam/Census/library/publications/2020/demo/p25-1144.pdf (accessed on 10 September 2022).
- United Nations Department of Economic and Social Affairs. World Population Ageing 2019. Highlights; United Nations: New York, NY, USA, 2019; Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 10 September 2022).
- Jaul, E.; Barron, J. Age-related diseases and clinical and public health implications for the 85 years old and over population. Front. Public Health 2017, 5, 335. [Google Scholar] [CrossRef] [Green Version]
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef] [Green Version]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- World Obesity Federation. World Obesity. World Obesity Atlas; World Obesity Federation: London, UK, 2022; Available online: https://data.worldobesity.org/publications/World-Obesity-Atlas-2022.pdf (accessed on 10 September 2022).
- Bhaskaran, K.; Douglas, I.; Forbes, H.; dos-Santos-Silva, I.; Leon, D.A.; Smeeth, L. Body-mass index and risk of 22 specific cancers: A population-based cohort study of 5·24 million UK adults. Lancet 2014, 384, 755–765. [Google Scholar] [CrossRef] [Green Version]
- Global BMI Mortality Collaboration; Di Angelantonio, E.; Bhupathiraju, S.N.; Wormser, D.; Gao, P.; Kaptoge, S.; Berrington de Gonzalez, A.; Cairns, B.J.; Huxley, R.; Jackson, C.L.; et al. Body-mass index and all-cause mortality: Individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet 2016, 388, 776–786. [Google Scholar] [CrossRef] [Green Version]
- Puzianowska-Kuznicka, M.; Owczarz, M.; Wieczorowska-Tobis, K.; Nadrowski, P.; Chudek, J.; Slusarczyk, P.; Skalska, A.; Jonas, M.; Franek, E.; Mossakowska, M. Interleukin-6 and C-reactive protein, successful aging, and mortality: The PolSenior study. Immun. Ageing 2016, 13, 21. [Google Scholar] [CrossRef] [Green Version]
- OECD. The Heavy Burden of Obesity: The Economics of Prevention, OECD Health Policy Studies; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2021: OECD Indicators; OECD Publishing: Paris, France, 2021. [Google Scholar] [CrossRef]
- Larsson, S.C.; Burgess, S. Causal role of high body mass index in multiple chronic diseases: A systematic review and meta-analysis of Mendelian randomization studies. BMC Med. 2021, 19, 320. [Google Scholar] [CrossRef]
- Tartof, S.Y.; Qian, L.; Hong, V.; Wei, R.; Nadjafi, R.F.; Fischer, H.; Li, Z.; Shaw, S.F.; Caparosa, S.L.; Nau, C.L.; et al. Obesity and mortality among patients diagnosed with COVID-19: Results from an integrated Health Care Organization. Ann. Intern. Med. 2020, 173, 773–781. [Google Scholar] [CrossRef]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef]
- Sun, Z.; Wang, Z.T.; Sun, F.R.; Shen, X.N.; Xu, W.; Ma, Y.H.; Dong, Q.; Tan, L.; Yu, J.T.; Alzheimer’s Disease Neuroimaging Initiative. Late-life obesity is a protective factor for prodromal Alzheimer's disease: A longitudinal study. Aging 2020, 12, 2005–2017. [Google Scholar] [CrossRef]
- Amankwaa, I.; Nelson, K.; Rook, H.; Hales, C. Association between body mass index, multi-morbidity and activities of daily living among New Zealand nursing home older adults: A retrospective analysis of nationwide InterRAI data. BMC Geriatr. 2022, 22, 62. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, G.W.P.D.; von Haehling, S. The fatter, the better in old age: The current understanding of a difficult relationship. Curr. Opin. Clin. Nutr. Metab. Care 2022, 25, 1–6. [Google Scholar] [CrossRef]
- Ryg, J.; Anru, P.L.; Engberg, H.; Jorgensen, M.G.; Masud, T.; Christensen, K.; Andersen-Ranberg, K. Association of body mass index with all-cause mortality in acutely hospitalized older patients. J. Am. Med. Dir. Assoc. 2022, 23, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Puzianowska-Kuznicka, M.; Kuryłowicz, A.; Walkiewicz, D.; Borkowska, J.; Owczarz, M.; Olszanecka-Glinianowicz, M.; Wieczorowska-Tobis, K.; Skalska, A.; Szybalska, A.; Mossakowska, M. Obesity paradox in Caucasian seniors: Results of the PolSenior study. J. Nutr. Health Aging 2019, 23, 796–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowman, K.; Atkins, J.L.; Delgado, J.; Kos, K.; Kuchel, G.A.; Ble, A.; Ferrucci, L.; Melzer, D. Central adiposity and the overweight risk paradox in aging: Follow-up of 130,473 UK Biobank participants. Am. J. Clin. Nutr. 2017, 106, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Elagizi, A.; Kachur, S.; Lavie, C.J.; Carbone, S.; Pandey, A.; Ortega, F.B.; Milani, R.V. An overview and update on obesity and the obesity paradox in cardiovascular diseases. Prog. Cardiovasc. Dis. 2018, 61, 142–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donini, L.M.; Pinto, A.; Giusti, A.M.; Lenzi, A.; Poggiogalle, E. Obesity or BMI paradox? Beneath the tip of the iceberg. Front. Nutr. 2020, 7, 53. [Google Scholar] [CrossRef]
- Ma, W.; Liu, Y.; Wu, N.; Zhang, H.; Han, P.; Wang, F.; Wang, J.; Xie, F.; Niu, S.; Hu, H.; et al. Obesity, even in the metabolically healthy, increases the risk of poor physical performance: A cross-sectional study of older people in a Chinese community. Clin. Interv. Aging 2021, 16, 697–706. [Google Scholar] [CrossRef]
- Wierucki, Ł.; Kujawska-Danecka, H.; Mossakowska, M.; Grodzicki, T.; Błędowski, P.; Chudek, J.; Kostka, T.; Więcek, A.; Hajduk, A.; Bandosz, P.; et al. Health status and its socio-economic covariates in the older population in Poland—The assumptions and methods of the nationwide, cross-sectional PolSenior2 survey. Arch. Med. Sci. 2020, 18, 92–102. [Google Scholar] [CrossRef]
- Bledowski, P.; Mossakowska, M.; Chudek, J.; Grodzicki, T.; Milewicz, A.; Szybalska, A.; Wieczorowska-Tobis, K.; Wiecek, A.; Bartoszek, A.; Dabrowski, A.; et al. Medical, psychological and socioeconomic aspects of aging in Poland: Assumptions and objectives of the PolSenior project. Exp. Gerontol. 2011, 46, 1003–1009. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Creavin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.; Elhamoui, H.; Milligan, R.; et al. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. 2016, 2016, CD011145. [Google Scholar] [CrossRef] [Green Version]
- Patnode, C.D.; Perdue, L.A.; Rossom, R.C.; Rushkin, M.C.; Redmond, N.; Thomas, R.G.; Lin, J.S. Screening for Cognitive Impairment in Older Adults: An Evidence Update for the U.S. Preventive Services Task Force; Report No.: 19-05257-EF-1; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2020. [Google Scholar]
- Lo, A.H.; Woodman, R.J.; Pachana, N.A.; Byrne, G.J.; Sachdev, P.S. Associations between lifestyle and cognitive function over time in women aged 40-79 years. J. Alzheimers Dis. 2014, 39, 371–383. [Google Scholar] [CrossRef] [Green Version]
- Hajek, A.; König, H.H. Longitudinal predictors of functional impairment in older adults in Europe—Evidence from the Survey of Health, Ageing and Retirement in Europe. PLoS ONE 2016, 11, e0146967. [Google Scholar] [CrossRef] [Green Version]
- Sonoda, N.; Morimoto, A.; Ugi, S.; Morino, K.; Sekine, O.; Nemoto, K.I.; Maegawa, H.; Miyamatsu, N. Smoking status is associated with mild cognitive impairment assessed with the mini-mental state examination in Japanese diabetic patients. Diabetol. Int. 2016, 7, 361–367. [Google Scholar] [CrossRef]
- Kanter, R.; Caballero, B. Global gender disparities in obesity: A review. Adv. Nutr. 2012, 3, 491–498. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Health Observatory (GHO) Data: Overweight and Obesity; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/gho/ncd/risk_factors/overweight/en (accessed on 10 September 2022).
- Janssen, F.; Bardoutsos, A.; Vidra, N. Obesity prevalence in the long-term future in 18 European countries and in the USA. Obes. Facts 2020, 13, 514–527. [Google Scholar] [CrossRef]
- Kim, K.B.; Shin, Y.A. Males with obesity and overweight. J. Obes. Metab. Syndr. 2020, 29, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Carrard, I.; Rothen, S.; Rodgers, R.F. Body image and disordered eating in older women: A tripartite sociocultural model. Eat. Behav. 2020, 38, 101412. [Google Scholar] [CrossRef] [PubMed]
- McComb, S.E.; Mills, J.S. The effect of physical appearance perfectionism and social comparison to thin-, slim-thick-, and fit-ideal Instagram imagery on young women’s body image. Body Image 2022, 40, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Ek, S. Gender differences in health information behaviour: A Finnish population-based survey. Health Promot. Int. 2015, 30, 736–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, S.A.; Lv, N.; Xiao, L.; Ma, J. Gender differences in weight-related attitudes and behaviors among overweight and obese adults in the United States. Am. J. Mens Health 2016, 10, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Chylińska, J.; Łazarewicz, M.; Rzadkiewicz, M.; Adamus, M.; Jaworski, M.; Haugan, G.; Lillefjel, M.; Espnes, G.A.; Włodarczyk, D. The role of gender in the active attitude toward treatment and health among older patients in primary health care-self-assessed health status and sociodemographic factors as moderators. BMC Geriatr. 2017, 17, 284. [Google Scholar] [CrossRef] [Green Version]
- Fox, A.; Feng, W.; Asal, V. What is driving global obesity trends? Globalization or “modernization”? Global Health 2019, 15, 32. [Google Scholar] [CrossRef]
- Dong, Y.; Zhou, J.; Zhu, Y.; Luo, L.; He, T.; Hu, H.; Liu, H.; Zhang, Y.; Luo, D.; Xu, S.; et al. Abdominal obesity and colorectal cancer risk: Systematic review and meta-analysis of prospective studies. Biosci. Rep. 2017, 37, BSR20170945. [Google Scholar] [CrossRef] [Green Version]
- Xue, R.; Li, Q.; Geng, Y.; Wang, H.; Wang, F.; Zhang, S. Abdominal obesity and risk of CVD: A dose-response meta-analysis of thirty-one prospective studies. Br. J. Nutr. 2021, 126, 1420–1430. [Google Scholar] [CrossRef]
- Bijari, M.; Jangjoo, S.; Emami, N.; Raji, S.; Mottaghi, M.; Moallem, R.; Jangjoo, A.; Saberi, A. The accuracy of visceral adiposity index for the screening of metabolic syndrome: A systematic review and meta-analysis. Int. J. Endocrinol. 2021, 2021, 6684627. [Google Scholar] [CrossRef]
- Costa, D.; Scognamiglio, M.; Fiorito, C.; Benincasa, G.; Napoli, C. Genetic background, epigenetic factors and dietary interventions which influence human longevity. Biogerontology 2019, 20, 605–626. [Google Scholar] [CrossRef]
- Morris, B.J.; Willcox, B.J.; Donlon, T.A. Genetic and epigenetic regulation of human aging and longevity. Biochim. Biophys. Acta Mol. Basis Dis. 2019, 1865, 1718–1744. [Google Scholar] [CrossRef] [PubMed]
- Lynch, D.H.; Petersen, C.L.; Fanous, M.M.; Spangler, H.B.; Kahkoska, A.R.; Jimenez, D.; Batsis, J.A. The relationship between multimorbidity, obesity and functional impairment in older adults. J. Am. Geriatr. Soc. 2022, 70, 1442–1449. [Google Scholar] [CrossRef] [PubMed]
- Banack, H.R.; Kaufman, J.S. From bad to worse: Collider stratification amplifies confounding bias in the “obesity paradox”. Eur. J. Epidemiol. 2015, 30, 1111–1114. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.E.; Kim, J.M.; Joung, K.H.; Lee, J.H.; You, B.R.; Choi, M.J.; Ryu, M.J.; Ko, Y.B.; Lee, M.A.; Lee, J.; et al. The roles of adipokines, proinflammatory cytokines, and adipose tissue macrophages in obesity-associated insulin resistance in modest obesity and early metabolic dysfunction. PLoS ONE 2016, 11, e0154003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henning, R.J. Obesity and obesity-induced inflammatory disease contribute to atherosclerosis: A review of the pathophysiology and treatment of obesity. Am. J. Cardiovasc. Dis. 2021, 11, 504–529. [Google Scholar]
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol. Cell Physiol. 2021, 320, C375–C391. [Google Scholar] [CrossRef]
- Fulop, T.; Larbi, A.; Pawelec, G.; Khalil, A.; Cohen, A.A.; Hirokawa, K.; Witkowski, J.M.; Franceschi, C. Immunology of aging: The birth of inflammaging. Clin. Rev. Allergy Immunol. 2021, 18, 1–14. [Google Scholar] [CrossRef]
- Santoro, A.; Bientinesi, E.; Monti, D. Immunosenescence and inflammaging in the aging process: Age-related diseases or longevity? Ageing Res. Rev. 2021, 71, 101422. [Google Scholar] [CrossRef]
- Franceschi, C.; Capri, M.; Monti, D.; Giunta, S.; Olivieri, F.; Sevini, F.; Panourgia, M.P.; Invidia, L.; Celani, L.; Scurti, M.; et al. Inflammaging and anti-inflammaging: A systemic perspective on aging and longevity emerged from studies in humans. Mech. Ageing Dev. 2007, 128, 92–105. [Google Scholar] [CrossRef]
- Minciullo, P.L.; Catalano, A.; Mandraffino, G.; Casciaro, M.; Crucitti, A.; Maltese, G.; Morabito, N.; Lasco, A.; Gangemi, S.; Basile, G. Inflammaging and anti-inflammaging: The role of cytokines in extreme longevity. Arch. Immunol. Ther. Exp. 2016, 64, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Szymczak, J.; Milewicz, A.; Thijssen, J.H.; Blankenstein, M.A.; Daroszewski, J. Concentration of sex steroids in adipose tissue after menopause. Steroids 1998, 63, 319–321. [Google Scholar] [CrossRef]
- Barakat, R.; Oakley, O.; Kim, H.; Jin, J.; Ko, C.J. Extra-gonadal sites of estrogen biosynthesis and function. BMB Rep. 2016, 49, 488–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens, G.H.; Jocken, J.W.E.; Blaak, E.E. Sexual dimorphism in cardiometabolic health: The role of adipose tissue, muscle and liver. Nat. Rev. Endocrinol. 2021, 17, 47–66. [Google Scholar] [CrossRef] [PubMed]
- Marchand, G.B.; Carreau, A.M.; Weisnagel, S.J.; Bergeron, J.; Labrie, F.; Lemieux, S.; Tchernof, A. Increased body fat mass explains the positive association between circulating estradiol and insulin resistance in postmenopausal women. Am. J. Physiol. Endocrinol. Metab. 2018, 314, E448–E456. [Google Scholar] [CrossRef] [Green Version]
- Iorga, A.; Cunningham, C.M.; Moazeni, S.; Ruffenach, G.; Umar, S.; Eghbali, M. The protective role of estrogen and estrogen receptors in cardiovascular disease and the controversial use of estrogen therapy. Biol. Sex. Differ. 2017, 8, 33. [Google Scholar] [CrossRef] [Green Version]
- Brann, D.W.; Lu, Y.; Wang, J.; Zhang, Q.; Thakkar, R.; Sareddy, G.R.; Pratap, U.P.; Tekmal, R.R.; Vadlamudi, R.K. Brain-derived estrogen and neural function. Neurosci. Biobehav. Rev. 2022, 132, 793–817. [Google Scholar] [CrossRef]
- Anderson, A.L.; Harris, T.B.; Tylavsky, F.A.; Perry, S.E.; Houston, D.K.; Hue, T.F.; Strotmeyer, E.S.; Sahyoun, N.R.; Health ABC Study. Dietary patterns and survival of older adults. J. Am. Diet. Assoc. 2011, 111, 84–91. [Google Scholar] [CrossRef]
- Liu, Y.H.; Gao, X.; Mitchell, D.C.; Wood, G.C.; Still, C.D.; Jensen, G.L. Diet quality is associated with mortality in adults aged 80 years and older: A prospective study. J. Am. Geriatr. Soc. 2019, 67, 2180–2185. [Google Scholar] [CrossRef]
- Leitão, C.; Mignano, A.; Estrela, M.; Fardilha, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. The effect of nutrition on aging—A systematic review focusing on aging-related biomarkers. Nutrients 2022, 14, 554. [Google Scholar] [CrossRef]
- Black, M.; Bowman, M. Nutrition and healthy aging. Clin. Geriatr. Med. 2020, 36, 655–669. [Google Scholar] [CrossRef] [PubMed]
- Blagosklonny, M.V. From rapalogs to anti-aging formula. Oncotarget 2017, 8, 35492–35507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarrete-Villanueva, D.; Gómez-Cabello, A.; Gómez-Bruton, A.; Gesteiro, E.; Rodríguez-Gómez, I.; Pérez-Gómez, J.; Villa-Vicente, J.G.; Espino-Toron, L.; Gusi, N.; González-Gross, M.; et al. Fitness vs. fatness as determinants of survival in non-institutionalized older adults: The EXERNET multi-center study. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Joseph, K.J.V.; Dristhi, D.; Muhammad, T. Interaction of physical activity on the association of obesity-related measures with multimorbidity among older adults: A population-based cross-sectional study in India. BMJ Open 2021, 11, e050245. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, E.; Allison, D.J.; Bullock, A.; Heisz, J.J. Examining the obesity paradox: A moderating effect of fitness on adipose endocrine function in older adults. Mech. Ageing Dev. 2021, 193, 111406. [Google Scholar] [CrossRef]
- Jyväkorpi, S.K.; Urtamo, A.; Kivimäki, M.; Salomaa, V.; Strandberg, T.E. Association of midlife body composition with old-age health-related quality of life, mortality, and reaching 90 years of age: A 32-year follow-up of a male cohort. Am. J. Clin. Nutr. 2020, 112, 1287–1294. [Google Scholar] [CrossRef]
- Backholer, K.; Pasupathi, K.; Wong, E.; Hodge, A.; Stevenson, C.; Peeters, A. The relationship between body mass index prior to old age and disability in old age. Int. J. Obesity 2012, 36, 1180–1186. [Google Scholar] [CrossRef] [Green Version]
- Berry, K.M.; Garcia, S.; Warren, J.R.; Stokes, A.C. Association of weight at different ages and all-cause mortality among older adults in the US. J. Aging Health 2022, 34, 705–719. [Google Scholar] [CrossRef]
- Villareal, D.T.; Chode, S.; Parimi, N.; Sinacore, D.R.; Hilton, T.; Armamento-Villareal, R.; Napoli, N.; Qualls, C.; Shah, K. Weight loss, exercise, or both and physical function in obese older adults. N. Engl. J. Med. 2011, 364, 1218–1229. [Google Scholar] [CrossRef] [Green Version]
- Strandberg, T.E.; Sirola, J.; Pitkälä, K.H.; Tilvis, R.S.; Strandberg, A.Y.; Stenholm, S. Association of midlife obesity and cardiovascular risk with old age frailty: A 26-year follow-up of initially healthy men. Int. J. Obes. 2012, 36, 1153–1157. [Google Scholar] [CrossRef] [Green Version]
- Suh, J.; Cho, Y.J.; Kim, H.J.; Choi, S.S. Age-related difference in weight change and all-cause mortality in middle-aged and older Korean populations: Korean Longitudinal Study of Aging. Korean J. Fam. Med. 2021, 42, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Hartley, H.O.; Rao, I.N. Sampling with unequal probabilities. Ann. Math. Stat. 1962, 33, 350–374. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BMI (kg/m2) | WC (cm) | ||||
|---|---|---|---|---|---|
| Age (Years) | PolSenior | PolSenior2 | PolSenior | PolSenior2 | |
| Women | All | 28.9 (25.6–32.8) | 29.0 (25.3–32.6) | 98.0 (89.5–106.0) | 98.0 (89.0–107.0) |
| 65.0–69.9 | 30.2 (26.6–33.4) | 29.1 (25.3–32.7) * | 99.0 (90.0–107.5) | 97.0 (88.0–107.0) | |
| 70.0–74.9 | 29.2 (25.5–33.6) | 30.0 (26.2–33.9) | 98.0 (90.0–106.0) | 98.5 (89.5–107.0) | |
| 75.0–79.9 | 28.4 (25.5–32.4) | 28.7 (25.2–32.7) | 97.0 (89.0–104.0) | 97.0 (90.0–106.0) | |
| 80.0–84.9 | 28.2 (25.6–32.0) | 28.9 (25.6–32.0) | 97.0 (90.0–107.0) | 98.5 (90.0–107.1) | |
| 85.0–89.9 | 26.5 (24.2–30.3) | 28.5 (24.2-32.0) | 95.0 (86.0-103.0) | 98.0 (88.0-107.0) | |
| ≥ 90.0 | 25.1 (21.4–30.3) | 26.8 (22.8–30.3) | 92.0 (83.0–102.0) | 95.0 (84.5-104.0) | |
| p ⇓ | <0.001 | <0.001 | 0.12 | <0.001 | |
| Men | All | 27.8 (25.2–30.9) | 28.0 (25.3–31.3) | 103.0 (94.5–110.0) | 103.0 (96.0–112.0) |
| 65.0–69.9 | 28.2 (26.0–32.2) | 28.3 (26.1–31.8) | 104.0 (96.5–111.0) | 104.0 (97.0–112.0) | |
| 70.0–74.9 | 28.3 (25.1–31.5) | 28.0 (25.3–31.5) | 102.0 (96.0–111.0) | 103.2 (96.0–111.0) | |
| 75.0–79.9 | 27.5 (25.4–29.8) | 28.4 (25.3–31.5) | 103.0 (94.0–110.0) | 104.0 (97.0–113.0) * | |
| 80.0–84.9 | 27.4 (24.6–30.0) | 27.4 (24.4–30.5) | 101.0 (94.0–108.0) | 102.0 (95.0–111.0) | |
| 85.0–89.9 | 26.2 (23.7–28.9) | 26.5 (23.7–29.7) | 98.5 (90.0–105.0) | 100.0 (92.0–109.0) * | |
| ≥ 90.0 | 25.0 (22.8–28.1) | 25.6 (23.1–28.6) | 96.0 (88.0–104.0) | 98.0 (90.0–107.0) | |
| p ⇓ | <0.05 | <0.001 | 0.10 | <0.001 | |
| Obesity % (95% CI) | ||||
|---|---|---|---|---|
| Men | Women | |||
| Age (Years) | PolSenior | PolSenior2 | PolSenior | PolSenior2 |
| All | 31.5 (26.6–36.3) | 35.4 (32–38.8) | 42.0 (39–45) | 42.9 (40.0–45.8) |
| 65.0–69.9 | 36.1 (25.9–46.4) | 38.2 (32.6–43.8) | 50.3 (43.4–57.2) | 43.3 (37.2–49.4) |
| 70.0–74.9 | 36.1 (27.4–44.7) | 36.9 (30.6–43.3) | 44.3 (35.7–52.8) | 50.3 (44.0–56.7) |
| 75.0–79.9 | 24.4 (18.3–30.4) | 37.5 (32.3–42.6) ** | 38.9 (32.6–45.1) | 40.5 (34.7–46.2) |
| 80.0–84.9 | 25.1 (18.3–32.0) | 28.4 (23.1–33.7) | 35.1 (27.8–42.3) | 42.0 (35.1–48.9) |
| 85.0–89.9 | 15.9 (11.1–20.6) | 24.5 (17.3–31.6) * | 26.6 (20.7–32.6) | 36.6 (28.9–44.3) * |
| ≥ 90.0 | 11.5 (7.2–15.9) | 15.0 (9.3–20.8) | 26.7 (13.4–40.0) | 25.9 (18.1–33.7) |
| p ⇓ | <0.001 | <0.001 | <0.001 | <0.001 |
| OR (±95% CI) | ||||
| All | Ref. | 1.37 # (1.21–1.56) | Ref. | 1.09 (0.96–1.22) |
| 65.0–69.9 | 1.27 (0.96–1.67) | 0.82 (0.63–1.09) | ||
| 70.0–74.9 | 1.07 (0.83–1.38) | 1.01 (0.74–1.29) | ||
| 75.0–79.9 | 1.60 ** (1.20–2.15) | 1.02 (0.77–1.35) | ||
| 80.0–84.9 | 1.07 (0.79–1.46) | 1.08 (0.81–1.45) | ||
| 85.0–89.9 | 1.30 (0.90–1.89) | 1.29 (0.92–1.80) | ||
| ≥ 90.0 | 1.81 * (1.09–3.01) | 1.28 (0.85–1.94) | ||
| Abdominal Obesity NCEP-ATP III, M ≥ 102 cm, W ≥ 88 cm % (95% CI) | Abdominal Obesity IDF, M ≥ 94 cm, W ≥ 80 cm % (95% CI) | |||||||
|---|---|---|---|---|---|---|---|---|
| Men | Women | Men | Women | |||||
| Age (Years) | PolSenior | PolSenior2 | PolSenior | PolSenior2 | PolSenior | PolSenior2 | PolSenior | PolSenior2 |
| All | 53.2 (48.4–58.0) | 56.2 (52.5–59.9) | 78.8 (76.2–81.4) | 77.9 (75.6–80.2) | 77.1 (73.7–80.5) | 81.0 (78.1–83.9) | 92.1 (90.5–93.6) | 91.1 (89.5–92.8) |
| 65.0–69.9 | 58.7 (49.2–68.2) | 58.5 (52.3–64.7) | 81.5 (77.6–85.5) | 76.2 (71.6–80.9) | 78.4 (72.0–84.9) | 83.0 (78.6–87.5) | 94.1 (91.4–96.8) | 90.5 (86.9–94.2) |
| 70.0–74.9 | 51.6 (43.2–60.1) | 56.9 (51.1–62.8) | 78.5 (73.8–83.2) | 79.6 (75.2–84.0) | 80.2 (74.8–85.7) | 82.8 (78.0–87.6) | 91.0 (87.1–95.0) | 92.2 (88.6–95.7) |
| 75.0–79.9 | 53.4 (45.6–61.2) | 57.5 (52.2–62.8) | 79.8 (74.6–85.1) | 80.0 (75.1–85.0) | 76.0 (70.5–81.5) | 80.9 (75.8–86.1) | 93.1 (90.1–96.1) | 90.2 (85.7–94.6) |
| 80.0–84.9 | 48.7 (41.9–55.4) | 53.5 (46.6–60.5) | 81.1 (75.6–86.6) | 79.5 (74.0–85.0) | 75.8 (69.9–81.8) | 78.0 (72.8–83.1) | 92.3 (89.0–95.6) | 95.1 (92.1–98.0) |
| 85.0–89.9 | 37.0 (30.9–43.0) | 45.4 (37.8–53.1) | 73.4 (65.1–81.7) | 76.9 (70.3–83.4) | 67.1 (61.2–73.1) | 72.1 (64.1–80.0) | 89.9 (85.9–93.8) | 90.1 (85.5–94.6) |
| ≥90.0 | 31.5 (25.7–37.3) | 41.1 (33.2–49.1) * | 57.2 (42.7–71.7) | 71.4 (64.7–78.0) | 55.8 (47.1–64.5) | 64.9 (56.1–73.8) | 81.1 (73.8–88.3) | 83.2 (77.5–89.0) |
| p ⇓ | <0.001 | <0.001 | <0.001 | 0.08 | <0.001 | <0.001 | <0.001 | 0.067 |
| OR (95% CI) | ||||||||
| All | Ref. | 1.43 # (1.28–1.60) | Ref. | 1.09 (0.95–1.25) | Ref. | 1.41 # (1.23–1.61) | Ref. | 1.24 * (1.02–1.51) |
| 65.0–69.9 | 1.24 (0.95–1.63) | 0.89 (0.66–1.21) | 1.57 * (1.11–2.20) | 0.80 (0.51–1.27) | ||||
| 70.0–74.9 | 1.25 (0.97–1.61) | 1.01 (0.73–1.38) | 1.17 (0.85–1.62) | 1.13 (0.69–1.87) | ||||
| 75.0–79.9 | 1.47 ** (1.13–1.93) | 1.13 (0.79–1.60) | 1.72 ** (1.24–2.37) | 1.09 (0.67–1.79) | ||||
| 80.0–84.9 | 1.35 * (1.02–1.79) | 0.96 (0.67–1.36) | 1.06 (0.76–1.48) | 1.58 (0.88–2.81) | ||||
| 85.0–89.9 | 1.46 * (1.07–1.99) | 1.15 (0.80–1.66) | 1.19 (0.85–1.68) | 1.11 (0.67–1.85) | ||||
| ≥90.0 | 1.48 * (1.04–2.09) | 1.31 (0.90–2.02) | 1.38 (0.98–1.94) | 1.54 (0.97–2.44) | ||||
| BMI (kg/m2) * | WC (cm) * | |||
|---|---|---|---|---|
| ADL (Points) | <30 | ≥30 | W: <80, M: <94 | W: ≥80, M: ≥94 |
| 5–6 | 59.5% (57.1–61.9) | 40.5% (38.1–42.9) | 12.5% (10.8–14.2) | 87.5% (85.8–89.2) |
| 3–4 | 63.8% (54.0–73.6) | 36.2% (26.4–46.0) | 12.9% (7.5–18.4) | 87.1% (81.6–92.5) |
| 0–2 | 77.9% (68.1–87.6) | 22.1% (12.4–31.9) | 27.2% (18.4–35.9) | 72.8% (64.1–81.6) |
| ADL (Points) | BMI (kg/m2) ** | WC (cm) ** | ||
| 5–6 | 28.6 (25.4–32.2) | 100.0 (91.5–109.0) | ||
| 3–4 | 27.9 (23.4–31.6) | 102.0 (93.0–109.0) | ||
| 0–2 | 26.5 (23.4–29.0) | 93.0 (83.0–105.5) | ||
| BMI (kg/m2) * | WC (cm) * | |||
|---|---|---|---|---|
| MMSE (Points) | <30 | ≥30 | W: <80, M: <94 | W: ≥80, M: ≥94 |
| 28–30 | 59.6% (56.5–62.7) | 40.4% (37.3–43.5) | 12.5% (10.1–14.8) | 87.5% (85.2–89.9) |
| 24–27 | 57.6% (53.8–61.4) | 42.4% (38.6–46.2) | 12.8% (10.4–15.2) | 87.2% (84.8–89.6) |
| 20–23 | 62.3% (56.2–68.5) | 37.7% (31.5–43.8) | 10.5% (7.2–13.8) | 89.5% (86.2–92.8) |
| 10–19 | 75.0% (65.2–84.4) | 25.0% (15.2–34.8) | 20.4% (14.3–26.4) | 79.6% (73.6–85.7) |
| <10 | 68.8% (54.6–82.9) | 31.2% (17.1–45.4) | 21.8% (11.7–32.0) | 78.2% (68.0–88.3) |
| MMSE (Points) | BMI (kg/m2) ** | WC (cm) ** | ||
| 28–30 | 28.7 (25.6–32.0) | 100.0 (92.0–109.0) | ||
| 24–27 | 28.8 (25.4–32.9) | 101.0 (92.0–110.0) | ||
| 20–23 | 28.3 (25.2–31.3) | 101.0 (91.0–110.0) | ||
| 10–19 | 26.5 (23.2–29.8) | 96.0 (88.0–105.0) | ||
| <10 | 27.5 (23.4–30.5) | 95.5 (85.0–104.0) | ||
| ADL | MMSE | |||
|---|---|---|---|---|
| BMI | WC | BMI | WC | |
| Whole cohort * | ||||
| <85 years | rs = 0.01, p = 0.42 | rs = 0.0, p = 0.91 | rs = 0.02, p = 0.22 | rs = −0.02, p = 0.18 |
| ≥85 years | rs = 0.02, p = 0.54 | rs = 0.0, p = 0.91 | rs = 0.11, p < 0.001 | rs = 0.1, p < 0.001 |
| Women * | ||||
| <85 years | rs = −0.04, p = 0.10 | rs = −0.06, p < 0.01 | rs = 0.02, p = 0.29 | rs = −0.03, p = 0.19 |
| ≥85 years | rs = 0.03, p = 0.45 | rs = 0.01, p = 0.84 | rs = 0.15, p < 0.001 | rs = 0.09, p < 0.05 |
| Men * | ||||
| <85 years | rs = 0.08, p < 0.001 | rs = 0.05, p < 0.05 | rs = 0.02, p = 0.43 | rs = −0.02, p = 0.47 |
| ≥85 years | rs = 0.05, p = 0.23 | rs = 0.07, p = 0.12 | rs = 0.13, p < 0.01 | rs = 0.1, p < 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puzianowska-Kuznicka, M.; Kurylowicz, A.; Wierucki, L.; Owczarek, A.J.; Jagiello, K.; Mossakowska, M.; Zdrojewski, T.; Chudek, J. Obesity in Caucasian Seniors on the Rise: Is It Truly Harmful? Results of the PolSenior2 Study. Nutrients 2022, 14, 4621. https://doi.org/10.3390/nu14214621
Puzianowska-Kuznicka M, Kurylowicz A, Wierucki L, Owczarek AJ, Jagiello K, Mossakowska M, Zdrojewski T, Chudek J. Obesity in Caucasian Seniors on the Rise: Is It Truly Harmful? Results of the PolSenior2 Study. Nutrients. 2022; 14(21):4621. https://doi.org/10.3390/nu14214621
Chicago/Turabian StylePuzianowska-Kuznicka, Monika, Alina Kurylowicz, Lukasz Wierucki, Aleksander Jerzy Owczarek, Kacper Jagiello, Malgorzata Mossakowska, Tomasz Zdrojewski, and Jerzy Chudek. 2022. "Obesity in Caucasian Seniors on the Rise: Is It Truly Harmful? Results of the PolSenior2 Study" Nutrients 14, no. 21: 4621. https://doi.org/10.3390/nu14214621