
Inverse Association of Fruit and Vegetable Consumption with Nonalcoholic Fatty Liver Disease in Chinese Patients with Type 2 Diabetes Mellitus
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
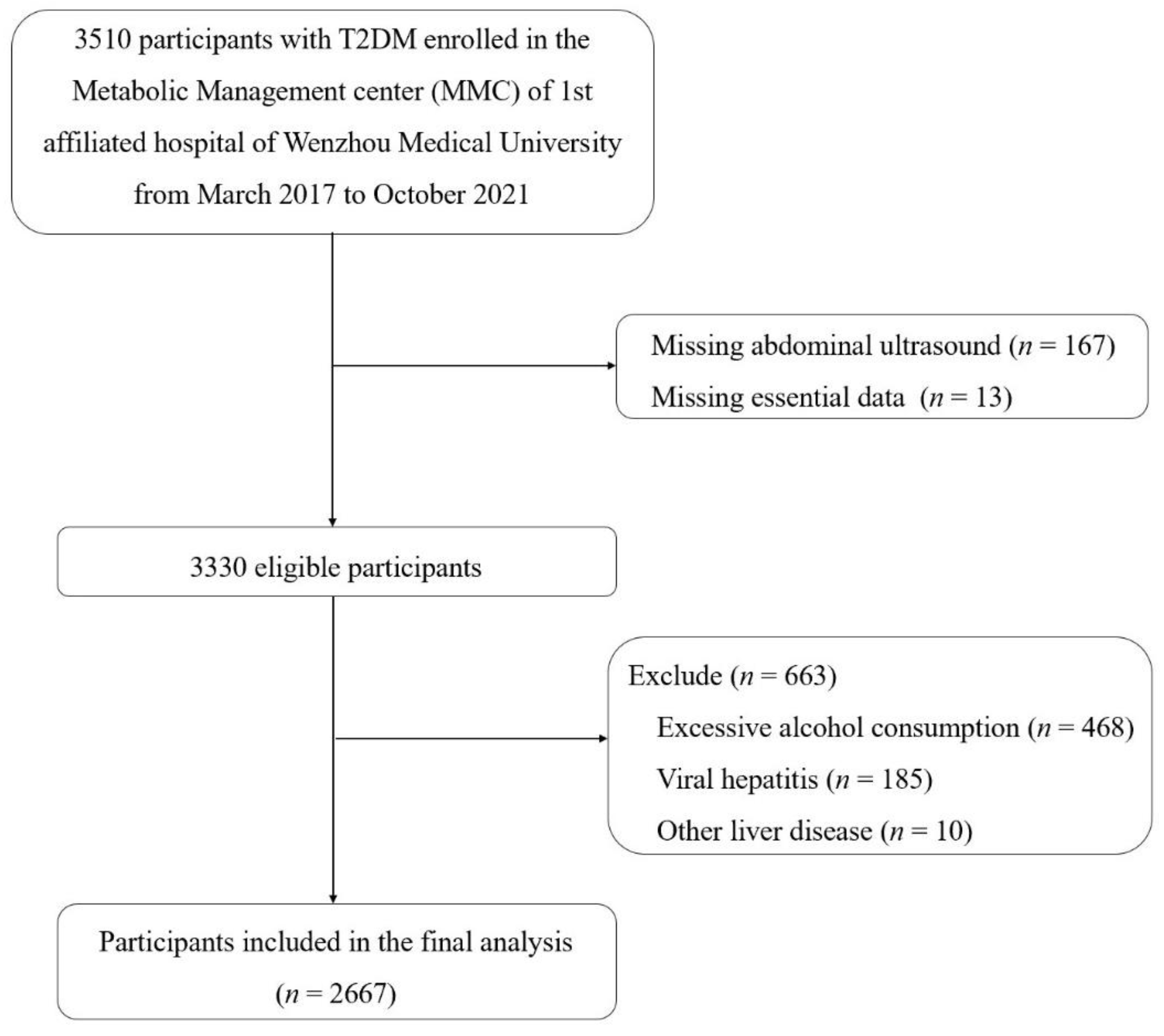
2.1. Study Population
2.2. Diagnosis
2.3. Diet and Covariate Assessments
2.4. Statistical Analyses
2.5. Ethical Approval
3. Results
3.1. Baseline Characteristics
3.2. Fruit and Vegetable Intake and NAFLD
3.3. Subgroup Analyses
3.4. The Effects of Fruit and Vegetable Intake on FLI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Wong, V. Changing NAFLD Epidemiology in China. Hepatology 2019, 70, 1095–1098. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wang, X.; Ye, M.; Zhang, S.; Zhang, Q.; Meng, G.; Liu, L.; Wu, H.; Gu, Y.; Wang, Y.; et al. Does a high intake of green leafy vegetables protect from NAFLD? Evidence from a large population study. Nutr. Metab. Cardiovasc. Dis. NMCD 2021, 31, 1691–1701. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Shin, S. Fruit and vegetable consumption and non-alcoholic fatty liver disease among Korean adults: A prospective cohort study. J. Epidemiol. Community Health 2020, 74, 1035–1042. [Google Scholar] [CrossRef]
- Noureddin, M.; Zelber-Sagi, S.; Wilkens, L.; Porcel, J.; Boushey, C.; Le Marchand, L.; Rosen, H.; Setiawan, V. Diet Associations With Nonalcoholic Fatty Liver Disease in an Ethnically Diverse Population: The Multiethnic Cohort. Hepatology 2020, 71, 1940–1952. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.; Adams, L. Nonalcoholic fatty liver disease and diabetes mellitus: Pathogenesis and treatment. Nat. Rev. Endocrinol. 2011, 7, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Corey, K.E.; Byrne, C.D.; Roden, M. The complex link between NAFLD and type 2 diabetes mellitus-mechanisms and treatments. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 599–612. [Google Scholar] [CrossRef]
- Tilg, H.; Moschen, A.R.; Roden, M. NAFLD and diabetes mellitus. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 32–42. [Google Scholar] [CrossRef]
- Albaugh, V.L.; Banan, B.; Antoun, J.; Xiong, Y.; Guo, Y.; Ping, J.; Alikhan, M.; Clements, B.A.; Abumrad, N.N.; Flynn, C.R. Role of Bile Acids and GLP-1 in Mediating the Metabolic Improvements of Bariatric Surgery. Gastroenterology 2019, 156, 1041–1051.e1044. [Google Scholar] [CrossRef] [PubMed]
- Han, C.Y. Update on FXR Biology: Promising Therapeutic Target? Int. J. Mol. Sci. 2018, 19, 2069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, E.; Wong, V.; Rinella, M. Non-alcoholic fatty liver disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- National Workshop on Fatty Liver and Alcoholic Liver Disease; Chinese Society of Hepatology; Chinese Medical Association; Fatty Liver Expert Committee; Chinese Medical Doctor Association. Guidelines of prevention and treatment for nonalcoholic fatty liver disease (2018, China). J. Dig. Dis. 2019, 20, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Chinese Diabetes Society. Guideline for the prevention and reatment of type 2 diabetes mellitus in China (2020 edition). Zhong Hua Nei Fen Mi Dai Xie Za Zhi 2021, 37, 311–398. [Google Scholar]
- Zhou, B. Predictive values of body mass index and waist circumference to risk factors of related diseases in Chinese adult population. Zhong Hua Liu Xing Bing Xue Za Zhi 2002, 23, 5–10. [Google Scholar]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Mirabelli, M.; Chiefari, E.; Arcidiacono, B.; Corigliano, D.M.; Brunetti, F.S.; Maggisano, V.; Russo, D.; Foti, D.P.; Brunetti, A. Mediterranean Diet Nutrients to Turn the Tide against Insulin Resistance and Related Diseases. Nutrients 2020, 12, 1066. [Google Scholar] [CrossRef] [Green Version]
- Soltani, S.; Shirani, F.; Chitsazi, M.J.; Salehi-Abargouei, A. The effect of dietary approaches to stop hypertension (DASH) diet on weight and body composition in adults: A systematic review and meta-analysis of randomized controlled clinical trials. Obes. Rev. 2016, 17, 442–454. [Google Scholar] [CrossRef] [PubMed]
- Akhlaghi, M. Dietary Approaches to Stop Hypertension (DASH): Potential mechanisms of action against risk factors of the metabolic syndrome. Nutr. Res. Rev. 2020, 33, 1–18. [Google Scholar] [CrossRef]
- Abenavoli, L.; Greco, M.; Milic, N.; Accattato, F.; Foti, D.; Gulletta, E.; Luzza, F. Effect of Mediterranean Diet and Antioxidant Formulation in Non-Alcoholic Fatty Liver Disease: A Randomized Study. Nutrients 2017, 9, 870. [Google Scholar] [CrossRef] [PubMed]
- Doustmohammadian, A.; Clark, C.C.T.; Maadi, M.; Motamed, N.; Sobhrakhshankhah, E.; Ajdarkosh, H.; Mansourian, M.R.; Esfandyari, S.; Hanjani, N.A.; Nikkhoo, M.; et al. Favorable association between Mediterranean diet (MeD) and DASH with NAFLD among Iranian adults of the Amol Cohort Study (AmolCS). Sci. Rep. 2022, 12, 2131. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, M.; Kengne, A.P. Higher adherence to plant-based diets are associated with lower likelihood of fatty liver. Clin. Nutr. 2019, 38, 1672–1677. [Google Scholar] [CrossRef] [PubMed]
- Xiao, M.L.; Lin, J.S.; Li, Y.H.; Liu, M.; Deng, Y.Y.; Wang, C.Y.; Chen, Y.M. Adherence to the Dietary Approaches to Stop Hypertension (DASH) diet is associated with lower presence of non-alcoholic fatty liver disease in middle-aged and elderly adults. Pub. Health Nutr. 2020, 23, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Ni, Y.; Nagata, N.; Xu, L.; Ota, T. Micronutrient Antioxidants and Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2016, 17, 1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Lee, G.; Heo, S.Y.; Roh, Y.S. Oxidative Stress Is a Key Modulator in the Development of Nonalcoholic Fatty Liver Disease. Antioxidants 2021, 11, 91. [Google Scholar] [CrossRef] [PubMed]
- Sohrabipour, S.; Sharifi, M.R.; Sharifi, M.; Talebi, A.; Soltani, N. Effect of magnesium sulfate administration to improve insulin resistance in type 2 diabetes animal model: Using the hyperinsulinemic-euglycemic clamp technique. Fundam. Clin. Pharmacol. 2018, 32, 603–616. [Google Scholar] [CrossRef] [PubMed]
- Fengler, V.H.; Macheiner, T.; Goessler, W.; Ratzer, M.; Haybaeck, J.; Sargsyan, K. Hepatic Response of Magnesium-Restricted Wild Type Mice. Metabolites 2021, 11, 762. [Google Scholar] [CrossRef]
- Xia, Y.; Zhang, S.; Zhang, Q.; Liu, L.; Meng, G.; Wu, H.; Bao, X.; Gu, Y.; Sun, S.; Wang, X.; et al. Insoluble dietary fibre intake is associated with lower prevalence of newly-diagnosed non-alcoholic fatty liver disease in Chinese men: A large population-based cross-sectional study. Nutr. Metab. 2020, 17, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, H.; Yang, A.; Mao, L.; Quan, Y.; Cui, J.; Sun, Y. Association between Dietary Fiber Intake and Non-alcoholic Fatty Liver Disease in Adults. Front. Nutr. 2020, 7, 593735. [Google Scholar] [CrossRef] [PubMed]
- Parnell, J.A.; Raman, M.; Rioux, K.P.; Reimer, R.A. The potential role of prebiotic fibre for treatment and management of non-alcoholic fatty liver disease and associated obesity and insulin resistance. Liver Int. 2012, 32, 701–711. [Google Scholar] [CrossRef] [PubMed]
- Canfora, E.E.; Jocken, J.W.; Blaak, E.E. Short-chain fatty acids in control of body weight and insulin sensitivity. Nat. Rev. Endocrinol. 2015, 11, 577–591. [Google Scholar] [CrossRef] [PubMed]
- Li, X.N.; Song, J.; Zhang, L.; LeMaire, S.A.; Hou, X.; Zhang, C.; Coselli, J.S.; Chen, L.; Wang, X.L.; Zhang, Y.; et al. Activation of the AMPK-FOXO3 pathway reduces fatty acid-induced increase in intracellular reactive oxygen species by upregulating thioredoxin. Diabetes 2009, 58, 2246–2257. [Google Scholar] [CrossRef] [PubMed]
- Long, Y.C.; Zierath, J.R. AMP-activated protein kinase signaling in metabolic regulation. J. Clin. Investig. 2006, 116, 1776–1783. [Google Scholar] [CrossRef] [Green Version]
- Solah, V.A.; Kerr, D.A.; Hunt, W.J.; Johnson, S.K.; Boushey, C.J.; Delp, E.J.; Meng, X.; Gahler, R.J.; James, A.P.; Mukhtar, A.S.; et al. Effect of Fibre Supplementation on Body Weight and Composition, Frequency of Eating and Dietary Choice in Overweight Individuals. Nutrients 2017, 9, 149. [Google Scholar] [CrossRef]
- Chan, R.; Wong, V.W.; Chu, W.C.; Wong, G.L.; Li, L.S.; Leung, J.; Chim, A.M.; Yeung, D.K.; Sea, M.M.; Woo, J.; et al. Diet-Quality Scores and Prevalence of Nonalcoholic Fatty Liver Disease: A Population Study Using Proton-Magnetic Resonance Spectroscopy. PLoS ONE 2015, 10, e0139310. [Google Scholar] [CrossRef] [Green Version]
- Tajima, R.; Kimura, T.; Enomoto, A.; Saito, A.; Kobayashi, S.; Masuda, K.; Iida, K. No association between fruits or vegetables and non-alcoholic fatty liver disease in middle-aged men and women. Nutrition 2019, 61, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Lu, Z.; Lu, M.; Liu, M.; Liu, L.; Meng, G.; Yu, B.; Wu, H.; Bao, X.; Gu, Y.; et al. Raw orange intake is associated with higher prevalence of non-alcoholic fatty liver disease in an adult population. Nutrition 2019, 60, 252–260. [Google Scholar] [CrossRef]
- Fakhoury-Sayegh, N.; Younes, H.; Heraoui, G.; Sayegh, R. Nutritional Profile and Dietary Patterns of Lebanese Non-Alcoholic Fatty Liver Disease Patients: A Case-Control Study. Nutrients 2017, 9, 1245. [Google Scholar] [CrossRef] [Green Version]
- Alperet, D.J.; Butler, L.M.; Koh, W.P.; Yuan, J.M.; van Dam, R.M. Influence of temperate, subtropical, and tropical fruit consumption on risk of type 2 diabetes in an Asian population. Am. J. Clin. Nutr. 2017, 105, 736–745. [Google Scholar] [CrossRef] [Green Version]
- European Association for Study of Liver. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef]


{kind=link}
| Total | <500 g/day | ≥500 g/day | p | |
|---|---|---|---|---|
| Case/participants (%) | 1445/2667 (54.06) | 714/1277 (56.04) | 731/1369 (52.48) | 0.065 |
| Sex (male, %) | 63.52 | 65.23 | 61.96 | 0.080 |
| Age (years) | 49.94 (11.79) | 49.14 (12.21) | 50.68 (11.34) | 0.001 * |
| Diabetes duration (month) | 64 (4–136) | 60 (3–128) | 69 (5–146) | 0.004 * |
| Family history of diabetes (%) | 56.62 | 56.35 | 56.88 | 0.783 |
| Anthropometric parameters | ||||
| DBP (mmHg) | 75.01 (11.02) | 75.49 (11.30) | 74.57 (10.73) | 0.031 * |
| SBP (mmHg) | 126.5 (18.59) | 126.55 (18.81) | 126.45 (18.40) | 0.892 |
| BMI (kg/m2) | 24.55 (3.70) | 24.70 (3.79) | 24.40 (3.60) | 0.039 * |
| WC (cm) | 88.43 (10.15) | 88.95 (10.30) | 87.95 (9.98) | 0.012 * |
| HC (cm) | 94.42 (7.45) | 94.69 (7.47) | 94.17 (7.43) | 0.073 |
| Lifestyle factors | ||||
| Educational attainment (≥12 year%) | 26.30 | 26.81 | 25.84 | 0.571 |
| Current smoking (%) | 29.70 | 33.20 | 26.50 | <0.001 * |
| Current drinking (%) | 34.19 | 34.69 | 33.74 | 0.604 |
| Physical activity (almost never, %) | 27.42 | 29.49 | 25.52 | 0.022 * |
| Fruit and vegetable intake (%) | ||||
| Fruit intake | ||||
| <200 g/day | 69.88 | 79.56 | 61.03 | <0.001 * |
| 200–400 g/day | 21.89 | 18.25 | 25.21 | |
| >400 g/day | 8.23 | 2.19 | 13.75 | |
| Vegetable intake | ||||
| <200 g/day | 13.28 | 25.22 | 2.36 | <0.001 * |
| 200–400 g/day | 39.51 | 52.39 | 27.72 | |
| >400 g/day | 47.21 | 22.40 | 69.91 | |
| Biochemical index | ||||
| HbAc1 (%) | 9.95 (2.45) | 9.90 (2.42) | 9.99 (2.48) | 0.375 |
| UA (μmol/L) | 325.55 (95.57) | 330.42 (100.38) | 321.13 (90.79) | 0.013 * |
| ALT (U/L) | 22 (15–35) | 23 (15–38) | 21 (15–33) | 0.005 * |
| AST (U/L) | 21 (17–28) | 21 (17–29) | 21 (17–27) | 0.196 |
| TGs (mmol/L) | 1.52 (1.04–2.31) | 1.55 (1.05–2.47) | 1.51 (1.03–2.20) | 0.003 * |
| TC (mmol/L) | 4.94 (1.48) | 4.98 (1.55) | 4.91 (1.41) | 0.198 |
| HDL-c (mmol/L) | 0.99 (0.85–1.16) | 0.98 (0.83–1.14) | 1.00 (0.86–1.18) | 0.001 * |
| LDL-c (mmol/L) | 2.71 (0.91) | 2.72 (0.93) | 2.70 (0.89) | 0.488 |
| HOMA-IR | 2.35 (1.41–3.98) | 2.46 (1.47–4.17) | 2.24 (1.35–3.80) | 0.008 * |
| Cases/Participants (n/n, %) | Model 1 | Model 2 | Model 3 | Model 4 | |||||
|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | ||
| Fruit–vegetable intake | |||||||||
| <500 g/day | 714/1274 (56.04) | Ref | Ref | Ref | Ref | ||||
| ≥500 g/day | 731/1393 (52.47) | 0.91 (0.75, 1.09) | 0.302 | 0.90 (0.75, 1.09) | 0.296 | 0.89 (0.73, 1.09) | 0.257 | 0.89 (0.73, 1.09) | 0.252 |
| Fruit intake | |||||||||
| <200 g/day | 976/1865 (52.33) | Ref | Ref | Ref | Ref | ||||
| 200–400 g/day | 338/583 (57.98) | 1.23 (1.01, 1.49) | 0.037 * | 1.16 (0.96, 1.41) | 0.130 | 1.10 (0.90, 1.36) | 0.358 | 1.08 (0.88, 1.33) | 0.462 |
| >400 g/day | 131/219 (59.82) | 1.48 (1.10, 1.98) | 0.009 * | 1.39 (1.03, 1.86) | 0.030 * | 1.18 (0.86, 1.62) | 0.316 | 1.15 (0.84, 1.59) | 0.388 |
| Vegetable intake | |||||||||
| <200 g/day | 222/354 (62.71) | Ref | Ref | Ref | Ref | ||||
| 200–400 g/day | 580/1055 (54.98) | 0.68 (0.53, 0.88) | 0.004 * | 0.72 (0.55, 0.93) | 0.013 * | 0.73 (0.56, 0.96) | 0.027* | 0.74 (0.56, 0.97) | 0.032 * |
| >400 g/day | 643/1258 (51.11) | 0.59 (0.46, 0.75) | 0.000 * | 0.65 (0.50, 0.84) | 0.001 * | 0.66 (0.50, 0.86) | 0.002* | 0.67 (0.51, 0.88) | 0.004 * |
| Cases/Participants (%) | OR (95% CI) | p | p-Interaction | |
|---|---|---|---|---|
| Sex | 0.755 | |||
| Male | 954/1692 (56.38) | 0.69 (0.49, 0.96) | 0.030 | |
| Female | 491/957 (50.36) | 0.57 (0.34, 0.95) | 0.029 | |
| Age | 0.640 | |||
| <50 years | 706/1181 (59.78) | 0.74 (0.50, 1.10) | 0.135 | |
| ≥50 years | 739/1486 (49.73) | 0.59 (0.40, 0.87) | 0.008 | |
| Duration | 0.151 | |||
| <67 months | 766/1310 (58.47) | 0.56 (0.38, 0.81) | 0.002 | |
| ≥67 months | 669/1341 (49.89) | 0.83 (0.54, 1.25) | 0.366 | |
| Overweight/Obesity | 0.598 | |||
| No | 485/1223 (39.66) | 0.70 (0.47, 1.05) | 0.088 | |
| Yes | 948/1423 (66.62) | 0.64 (0.44, 0.94) | 0.024 | |
| Central obesity | 0.432 | |||
| No | 552/1288 (42.86) | 0.73 (0.48, 1.09) | 0.125 | |
| Yes | 877/1350 (64.96) | 0.63 (0.43, 0.92) | 0.016 | |
| Hypertension | 0.201 | |||
| No | 556/1121 (49.6) | 0.84 (0.55, 1.29) | 0.433 | |
| Yes | 889/1546 (57.5) | 0.56 (0.39, 0.81) | 0.002 | |
| Hyperlipidemia | 0.168 | |||
| No | 472/1013 (46.59) | 0.73 (0.45, 1.17) | 0.191 | |
| Yes | 973/1654 (58.83) | 0.62 (0.44, 0.87) | 0.005 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | |
| Fruits | 1.007 (−0.703, 2.717) | 0.248 | −0.255 (−1.137, 0.627) | 0.571 |
| Vegetables | −4.210 (−5.776, −2.644) | <0.001 * | −1.028 (−1.836, −0.219) | 0.013 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, L.-J.; He, Z.-Y.; Gu, X.; Hu, X.; Zhang, X.-X.; Yang, L.-J.; Li, J.; Pan, L.-Y.; Li, Y.-Q.; Yang, B.; et al. Inverse Association of Fruit and Vegetable Consumption with Nonalcoholic Fatty Liver Disease in Chinese Patients with Type 2 Diabetes Mellitus. Nutrients 2022, 14, 4559. https://doi.org/10.3390/nu14214559
Du L-J, He Z-Y, Gu X, Hu X, Zhang X-X, Yang L-J, Li J, Pan L-Y, Li Y-Q, Yang B, et al. Inverse Association of Fruit and Vegetable Consumption with Nonalcoholic Fatty Liver Disease in Chinese Patients with Type 2 Diabetes Mellitus. Nutrients. 2022; 14(21):4559. https://doi.org/10.3390/nu14214559
Chicago/Turabian StyleDu, Lin-Jia, Zhi-Ying He, Xiao Gu, Xiang Hu, Xing-Xing Zhang, Li-Juan Yang, Jing Li, Lin-Yu Pan, Ying-Qian Li, Bo Yang, and et al. 2022. "Inverse Association of Fruit and Vegetable Consumption with Nonalcoholic Fatty Liver Disease in Chinese Patients with Type 2 Diabetes Mellitus" Nutrients 14, no. 21: 4559. https://doi.org/10.3390/nu14214559