
Assessment of SARS-CoV-2 Infection According to Previous Metabolic Status and Its Association with Mortality and Post-Acute COVID-19

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yue, H.; Bai, X.; Wang, J.; Yu, Q.; Liu, W.; Pu, J.; Wang, X.; Hu, J.; Xu, D.; Li, X.; et al. Gansu Provincial Medical Treatment Expert Group of COVID-19. Clinical characteristics of coronavirus disease 2019 in Gansu province, China. Ann. Palliat. Med. 2020, 9, 1404–1412. [Google Scholar] [CrossRef]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 22 June 2022).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Bailly, L.; Fabre, R.; Courjon, J.; Carles, M.; Dellamonica, J.; Pradier, C. Obesity, diabetes, hypertension and severe outcomes among inpatients with coronavirus disease 2019: A nationwide study. Clin. Microbiol. Infect. 2022, 28, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Byrne, C.D.; Zheng, M.H.; Targher, G. Diabetes as a risk factor for greater COVID-19 severity and in-hospital death: A meta-analysis of observational studies. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1236–1248. [Google Scholar] [CrossRef] [PubMed]
- Korakas, E.; Ikonomidis, I.; Kousathana, F.; Balampanis, K.; Kountouri, A.; Raptis, A.; Palaiodimou, L.; Kokkinos, A.; Lambadiari, V. Obesity and COVID-19: Immune and metabolic derangement as a possible link to adverse clinical outcomes. Am. J. Physiol. Endocrinol. Metab. 2020, 319, E105–E109. [Google Scholar] [CrossRef]
- Agouridis, A.P.; Pagkali, A.; Zintzaras, E.; Rizos, E.C.; Ntzani, E.E. High-density lipoprotein cholesterol: A marker of COVID-19 infection severity? Atheroscler. Plus 2021, 44, 1–9. [Google Scholar] [CrossRef]
- Louie, J.K.; Acosta, M.; Winter, K.; Jean, C.; Gavali, S.; Schechter, R.; Vugia, D.; Harriman, K.; Matyas, B.; Glaser, C.A.; et al. California Pandemic (H1N1) Working Group. Factors associated with death or hospitalization due to pandemic 2009 influenza A(H1N1) infection in California. JAMA 2009, 302, 1896–1902. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Zhang, N. Focus on the 2019 novel coronavirus (SARS-CoV-2). Future Microbiol. 2020, 15, 905–918. [Google Scholar]
- Del Sole, F.; Farcomeni, A.; Loffredo, L.; Carnevale, R.; Menichelli, D.; Vicario, T.; Pignatelli, P.; Pastori, D. Features of severe COVID-19: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2020, 50, e13378. [Google Scholar] [CrossRef]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut Off Points. In StatPearls [Internet]; Updated 10 July 2020; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK541070 (accessed on 10 July 2022).
- Touloumi, G.; on Behalf of the EMENO Study Group; Karakosta, A.; Kalpourtzi, N.; Gavana, M.; Vantarakis, A.; Kantzanou, M.; Hajichristodoulou, C.; Chlouverakis, G.; Tryp-sianis, G.; et al. High prevalence of cardiovascular risk factors in adults living in Greece: The EMENO National Health Examination Survey. BMC Public Health 2020, 20, 1665. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, F.M.; Lam, K.; Sounderajah, V.; Clarke, J.M.; Ashrafian, H.; Darzi, A. Characteristics and predictors of acute and chronic post-COVID syndrome: A systematic review and meta-analysis. eClinicalMedicine 2020, 36, 100899. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef]
- van Kessel, S.; Olde Hartman, T.C.; Lucassen, P.; van Jaarsveld, C. Post-acute and long-COVID-19 symptoms in patients with mild diseases: A systematic review. Fam. Pract. 2022, 39, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad. Estrategia de Vacunación Frente a COVID-19 En España. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/covid19/docs/COVID-19_Actualizacion8_EstrategiaVacunacion.pdf (accessed on 11 May 2022).
- Sociedad Española de Médicos Generales y de Familia (SEMG) Guía Clínica Para El Paciente Long COVID/COVID Persistente. 2021. Available online: https://www.semg.es/index.php/consensos-guias-y-protocolos/363-guia-clinica-para-la-atencion-al-paciente-long-covid-covid-persistente (accessed on 19 May 2022).
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.C.; Di Napoli, R. Features, evaluation and treatment coronavirus (COVID-19). In Statpearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Mughal, M.S.; Kaur, I.P.; Jaffery, A.R.; Dalmacion, D.L.; Wang, C.; Koyoda, S.; Kramer, V.E.; Patton, C.D.; Weiner, S.; Eng, M.H.; et al. COVID-19 patients in a tertiary US hospital: Assessment of clinical course and predictors of the disease severity. Respir. Med. 2020, 172, 106130. [Google Scholar] [CrossRef] [PubMed]
- Carod-Artal, F.J. Post-COVID-19 syndrome: Epidemiology, diagnostic criteria and pathogenic mechanisms involved. Rev. Neurol. 2021, 72, 384–396. [Google Scholar] [PubMed]
- Iaccarino, G.; Grassi, G.; Borghi, C.; Ferri, C.; Salvetti, M.; Volpe, M. Age and Multimorbidity Predict Death Among COVID-19 Patients: Results of the SARS-RAS Study of the Italian Society of Hypertension. Hypertension 2020, 76, 366–372. [Google Scholar] [CrossRef]
- Cao, J.; Tu, W.J.; Cheng, W.; Yu, L.; Liu, Y.K.; Hu, X.; Liu, Q. Clinical Features and Short-term Outcomes of 102 Patients with Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 748–755. [Google Scholar] [CrossRef]
- Dietz, W.; Santos-Burgoa, C. Obesity and its Implications for COVID-19 Mortality. Obesity 2020, 28, 1005. [Google Scholar] [CrossRef] [Green Version]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.Y.; Desai, A.; de Lima Lopes, G.; et al. COVID-19 and Cancer Consortium. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Gu, T.; Chu, Q.; Yu, Z.; Fa, B.; Li, A.; Xu, L.; Wu, R.; He, Y. History of coronary heart disease increased the mortality rate of patients with COVID-19: A nested case-control study. BMJ Open 2020, 10, e038976. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk Factors and Disease Profile of Post-Vaccination SARS-CoV-2 Infection in UK Users of the COVID Symptom Study App: A Prospective, Community-Based, Nested, Case-Control Study. Lancet Infect. Dis. 2021, 22, 43–55. [Google Scholar] [CrossRef]
- Kuodi, P.; Gorelik, Y.; Zayyad, H.; Wertheim, O.; Wiegler, K.B.; Jabal, K.A.; Dror, A.A.; Nazzal, S.; Glikman, D.; Edelstein, M. Association between vaccination status and reported incidence of post-acute COVID-19 symptoms in Israel: A cross-sectional study of patients tested between March 2020 and November 2021. medRxiv 2022. [Google Scholar] [CrossRef]
- Arbel, R.; Hammerman, A.; Sergienko, R.; Friger, M.; Peretz, A.; Netzer, D.; Yaron, S. BNT162b2 Vaccine Booster and Mortality Due to COVID-19. N. Engl. J. Med. 2021, 385, 2413–2420. [Google Scholar] [CrossRef]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 1, jiac136. [Google Scholar] [CrossRef]
- Mittal, J.; Ghosh, A.; Bhatt, S.P.; Anoop, S.; Ansari, I.A.; Misra, A. High prevalence of post COVID-19 fatigue in patients with type 2 diabetes: A case-control study. Diabetes Metab. Syndr. 2021, 15, 102302. [Google Scholar] [CrossRef]
- Montefusco, L.; Ben Nasr, M.; D’Addio, F.; Loretelli, C.; Rossi, A.; Pastore, I.; Daniele, G.; Abdelsalam, A.; Maestroni, A.; Dell’Acqua, M.; et al. Acute and long-term disruption of glycometabolic control after SARS-CoV-2 infection. Nat. Metab. 2021, 3, 774–785. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]
- Xie, Y.; Al-Aly, Z. Risks and burdens of incident diabetes in long COVID: A cohort study. Lancet Diabetes Endocrinol. 2022, 10, 311–321. [Google Scholar] [CrossRef]
- Zhu, L.; She, Z.-G.; Cheng, X.; Qin, J.-J.; Zhang, X.-J.; Cai, J.; Lei, F.; Wang, H.; Xie, J.; Wang, W.; et al. Association of Blood Glucose Control and Outcomes in Patients With COVID-19 and Pre-Existing Type 2 Diabetes. Cell Metab. 2020, 31, 1068–1077.e3. [Google Scholar] [CrossRef]
- Ilias, I.; Zabuliene, L. Hyperglycemia and the novel Covid-19 infection: Possible pathophysiologic mechanisms. Med. Hypotheses 2020, 139, 109699. [Google Scholar] [CrossRef] [PubMed]
- Voncken, S.F.J.; Feron, T.M.H.; Laven, S.A.J.S.; Karaca, U.; Beerhorst, K.; Klarenbeek, P.; Straetmans, J.M.J.A.A.; de Vries, G.J.; Kolfoort-Otte, A.A.B.; de Kruif, M.D. Impact of obstructive sleep apnea on clinical outcomes in patients hospitalized with COVID-19. Sleep Breath. 2021, 24, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ezquerra, E.A.; Castellano, V.J.; Alegría, B.A. Obesidad, síndrome metabólico y diabetes: Implicaciones cardiovasculares y actuación terapéutica. Rev. Esp. Cardiol. 2008, 61, 752–764. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
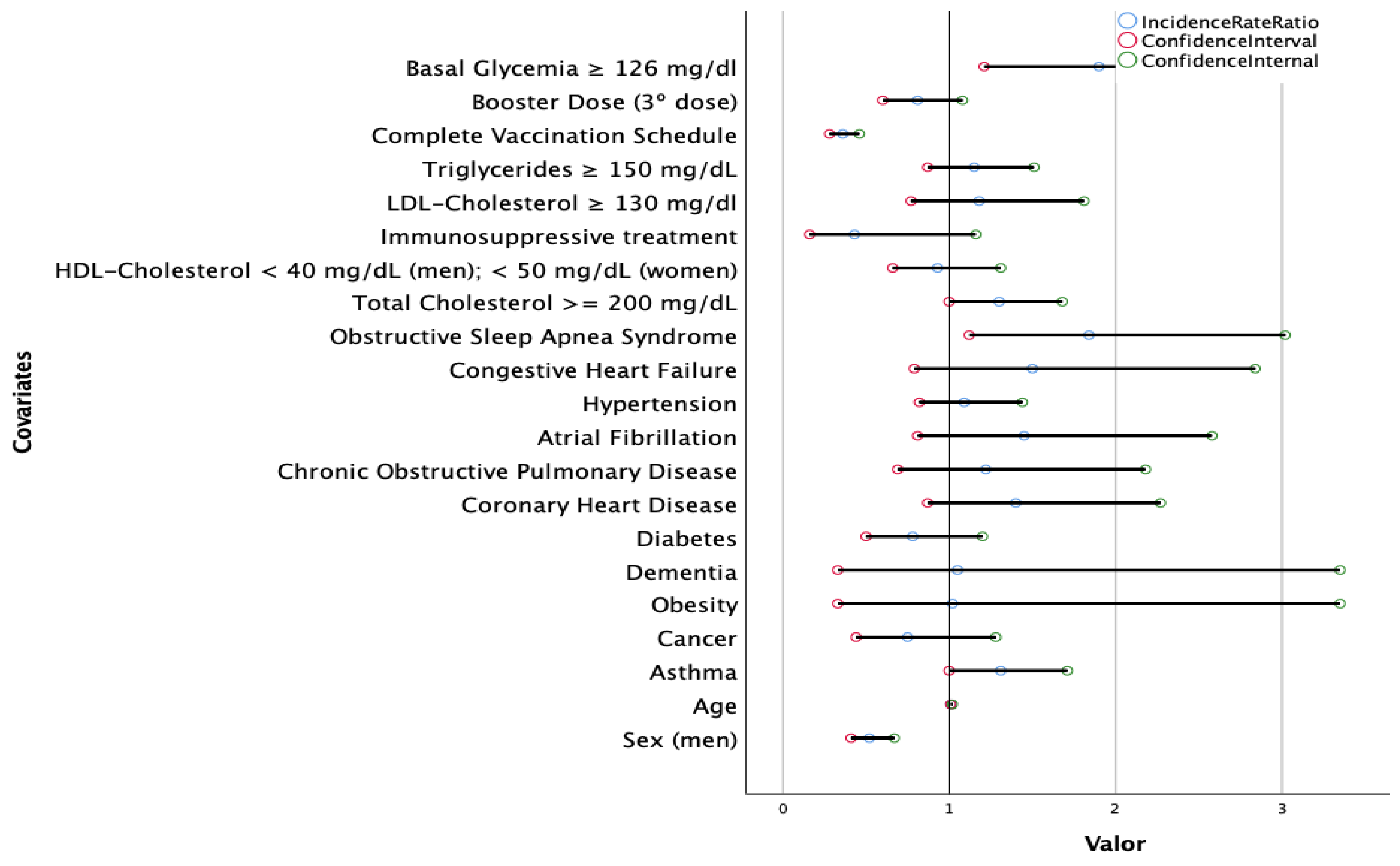
| Variables | N Cases (%) | N Post-Acute COVID-19 | Odds Ratio (CI) | p Value | |
|---|---|---|---|---|---|
| Sex | Women | 61184 (55.3) | 391 | 1.9 (1.6–2.3) | <0.001 |
| Men | 49542 (44.7) | 164 | 1 | ||
| Age | 12–17 | 7.500 (6.8) | 36 | 2.10 (1.40–3.14) | <0.001 |
| 18–49 | 71.527 (64.6) | 301 | 1 | ||
| 50–69 | 24.608 (22.2) | 147 | 1.68 (1.27–2.24) | ||
| >70 | 7.091 (6.4) | 71 | 2.39 (1.85–3.10) | ||
| Immunosuppressive treatment | Yes | 2057 (1.9) | 7 | 0.67 (0.32–1.42) | 0.297 |
| No | 108,669 (98.1) | 548 | 1 | ||
| Diabetes | Yes | 7684 (6.9) | 60 | 1.6 (1.2–2.1) | <0.001 |
| No | 103,042 (93.1) | 495 | 1 | ||
| Coronary heart disease | Yes | 2525 (2.3) | 25 | 2.0 (1.4–3) | <0.001 |
| No | 108,201 (97.7) | 530 | 1 | ||
| Atrial fibrillation | Yes | 1515 (1.4) | 18 | 2.4 (1.5–3.9) | <0.001 |
| No | 109,211 (98.6) | 537 | 1 | ||
| Hypertension | Yes | 20,109 (18.2) | 135 | 1.5 (1.2–1.8) | <0.001 |
| No | 90,617 (81.8) | 420 | 1 | ||
| Chronic obstructive pulmonary disease | Yes | 1648 (1.5) | 15 | 1.85 (1.1–3.09) | 0.018 |
| No | 109,078 (98.5) | 540 | 1 | ||
| Asthma | Yes | 15.295 (13.8) | 96 | 1.31 (1.05–1.63) | 0.017 |
| No | 95.431 (86.2) | 459 | 1 | ||
| Congestive heart failure | Yes | 982 (0.9) | 15 | 3.1 (1.9–5.3) | <0.001 |
| No | 109,744 (99.1) | 540 | 1 | ||
| Cancer | Yes | 3579 (3.2) | 24 | 1.4 (0.9–2) | 0.145 |
| No | 107,147 (96.8) | 531 | 1 | ||
| Obesity | Yes | 1513 (1.4) | 8 | 1.06 (0.52–2.13) | 0.879 |
| No | 109,213 (98.6) | 547 | 1 | ||
| Obstructive sleep apnea syndrome | Yes | 2154 (1.9) | 20 | 1.9 (1.2–3) | 0.005 |
| No | 108,037 (98.1) | 535 | 1 | ||
| Fasting glucose levels | ≥126 mg/dL | 4333 (5.7) | 43 | 1.9 (1.4–2.6) | <0.001 |
| <126 mg/dL | 71,274 (94.3) | 374 | 1 | ||
| LDL cholesterol | <130 mg/dL | 73,494 (93) | 435 | 0.92 (0.63–1.33) | 0.643 |
| ≥130 mg/dL | 5530 (7) | 30 | 1 | ||
| HDL cholesterol | ≥40 mg/dL (men); ≥50 mg/dL (women) | 71,858 (87.3) | 427 | 1.13 (0.85–1.5) | 0.392 |
| <40 mg/dL (men); <50 mg/dL (women) | 10,460 (12.7) | 55 | 1 | ||
| Total cholesterol | <200 mg/dL | 66,304 (69.6) | 372 | 0.93 (0.77–1.13) | 0.457 |
| ≥200 mg/dL | 28,909 (30.4) | 151 | 1 | ||
| Triglycerides | <150 mg/dL | 73,322 (81.8) | 388 | 1 | 0.179 |
| ≥150 mg/dL | 16,261 (18.2) | 100 | 1.16 (0.93–1.45) | ||
| Type of COVID-19 vaccine | Pfizer | 52.601 (47.5) | 195 | 0.27 (0.22–0.34) | <0.001 |
| Moderna | 30.500 (27.5) | 129 | 0.31 (0.25–0.39) | ||
| AstraZeneca | 8.065 (7.3) | 41 | 0.38 (0.27–0.53) | ||
| Janssen | 7.549 (6.8) | 29 | 0.28 (0.19–0.42) | ||
| Not vaccinated | 12.011 (10.9) | 161 | 1 | ||
| Complete vaccination schedule | Yes | 94,167 (85) | 376 | 0.37 (0.31–0.44) | <0.001 |
| No | 16,559 (15) | 179 | 1 | ||
| Booster dose (3rd dose) 12–17 years | Yes | 14 (0.2) | 0 | 1 | 0.795 |
| No | 7486 (99.8) | 36 | 1.005 (1.003–1.006) | ||
| Booster dose (3rd dose) 18–49 years | Yes | 8090 (11.3) | 34 | 1.001 (0.7–1.43) | 0.994 |
| No | 63,437 (88.7) | 267 | 1 | ||
| Booster dose (3rd dose) 50–69 years | Yes | 8887 (36.1) | 42 | 1.42 (0.99–2.03) | 0.056 |
| No | 15721 (63.9) | 105 | 1 | ||
| Booster dose (3rd dose) ≥70 years | Yes | 4939 (69.6) | 38 | 1 | 0.003 |
| No | 2152 (30.4) | 33 | 2 (1.26–3.21) | ||
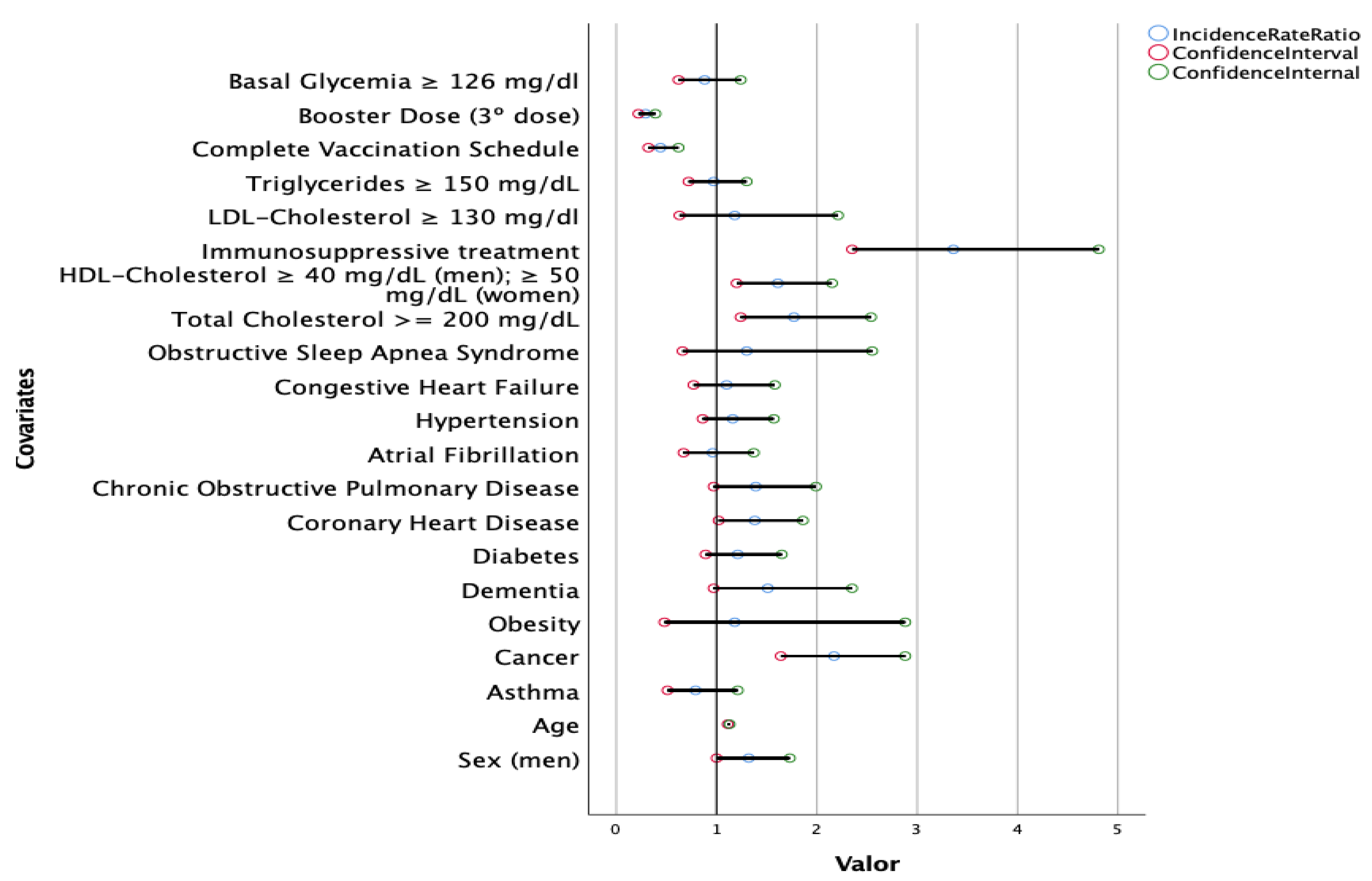
| Variables | N Cases | Deaths | Odds Ratio (CI) | p Value | |
|---|---|---|---|---|---|
| Sex | Women | 61,184 (55.3) | 161 | 0.7 (0.6–0.9) | <0.001 |
| Men | 49,542 (44.7) | 186 | 1 | ||
| Age | 12–49 | 79.027 | 11 | 1 | <0.001 |
| 50–69 | 24.608 | 69 | 20.2 (10.69–38.17) | ||
| ≥70 | 7.091 | 267 | 281.1 (153.71–513.93) | ||
| Immunosuppressive treatment | Yes | 2057 (1.9) | 50 | 9.1 (6.7–12.3) | <0.001 |
| No | 108,669 (98.1) | 297 | 1 | ||
| Diabetes | Yes | 7684 (6.9) | 148 | 10.1 (8.2–12.6) | <0.001 |
| No | 103,042 (93.1) | 199 | 1 | ||
| Coronary heart disease | Yes | 2525 (2.3) | 89 | 15.3 (12–19.5) | <0.001 |
| No | 108,201 (97.7) | 258 | 1 | ||
| Atrial fibrillation | Yes | 1515 (1.4) | 64 | 17 (12.8–22.4) | <0.001 |
| No | 109,211 (98.6) | 283 | 1 | ||
| Hypertension | Yes | 20,109 (18.2) | 242 | 10.5 (8.3–13.2) | <0.001 |
| No | 90,617 (81.8) | 105 | 1 | ||
| Chronic obstructive pulmonary disease | Yes | 1648 (1.5) | 53 | 12.3 (9.1–16.5) | <0.001 |
| No | 109,078 (98.5) | 1648 | 1 | ||
| Asthma | Yes | 15.295 (13.8) | 33 | 0.66 (0.46–0.94) | 0.020 |
| No | 95.431 (86.2) | 314 | 1 | ||
| Congestive heart failure | Yes | 982 (0.9) | 65 | 27.5 (20.8–36.3) | <0.001 |
| No | 109,744 (99.1) | 282 | 1 | ||
| Cancer | Yes | 3579 (3.2) | 103 | 13 (10.3–16.4) | 0.005 |
| No | 107,147 (96.8) | 244 | 1 | ||
| Obesity | Yes | 1513 (1.4) | 6 | 1.27 (0.57–2.85) | 0.560 |
| No | 109,213 (98.6) | 341 | 1 | ||
| Obstructive sleep apnea syndrome | Yes | 2154 (1.9) | 14 | 2.1 (1.2–3.6) | 0.005 |
| No | 108,037 (98.1) | 333 | 1 | ||
| Fasting glucose levels | ≥126 mg/dL | 4333 (5.7) | 83 | 6.2 (4.8–8) | <0.001 |
| <126 mg/dL | 71,274 (94.3) | 223 | 1 | ||
| LDL cholesterol | <130 mg/dL | 73,494 (93) | 281 | 0.57 (0.32–1) | 0.051 |
| ≥130 mg/dL | 5530 (7) | 12 | 1 | ||
| HDL cholesterol | ≥40 mg/dL (men); ≥50 mg/dL (women) | 71,858 (87.3) | 100 | 0.3 (0.24–0.38) | <0.001 |
| <40 mg/dL (men); <50 mg/dL (women) | 10,460 (12.7) | 208 | 1 | ||
| Total cholesterol | <200 mg/dL | 66,304 (69.6) | 263 | 0.53 (0.4–0.7) | <0.001 |
| ≥200 mg/dL | 28,909 (30.4) | 61 | 1 | ||
| Triglycerides | <150 mg/dL | 73,322 (81.8) | 228 | 1 | <0.001 |
| ≥150 mg/dL | 16,261 (18.2) | 99 | 2.1 (1.5–2.8) | ||
| Type of COVID-19 vaccine | Pfizer | 52.601 (47.5) | 125 | 0.32 (0.25–0.42) | <0.001 |
| Moderna | 30.500 (27.5) | 111 | 0.49 (0.37–0.66) | ||
| AstraZeneca | 8.065 (7.3) | 16 | 0.27 (0.16–0.46) | ||
| Janssen | 7.549 (6.8) | 7 | 0.13 (0.06–0.27) | ||
| Not vaccinated | 12.011 (10.9) | 88 | 1 | ||
| Complete vaccination schedule | Yes | 94,167 (85) | 257 | 0.5 (0.39–0.64) | <0.001 |
| No | 16,559 (15) | 90 | 1 | ||
| Booster dose (3rd dose) 12–17 years | Yes | 14 (0.2) | 0 | 1 | |
| No | 7486 (99.8) | 0 | |||
| Booster dose (3rd dose) 18–49 years | Yes | 8090 (11.3) | 2 | 1 | 0.472 |
| No | 63,437 (88.7) | 9 | 0.574 (0.124–2.66) | ||
| Booster dose (3rd dose) 50–69 years | Yes | 8887 (36.1) | 18 | 1 | 0.082 |
| No | 15,721 (63.9) | 51 | 1.6 (0.94–2.75) | ||
| Booster dose (3rd dose) ≥70 years | Yes | 4939 (69.6) | 94 | 1 | <0.001 |
| No | 2152 (30.4) | 173 | 4.51 (3.5–5.8) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Arriba Fernández, A.; Alonso Bilbao, J.L.; Espiñeira Francés, A.; Cabeza Mora, A.; Gutiérrez Pérez, Á.; Díaz Barreiros, M.Á.; Serra Majem, L. Assessment of SARS-CoV-2 Infection According to Previous Metabolic Status and Its Association with Mortality and Post-Acute COVID-19. Nutrients 2022, 14, 2925. https://doi.org/10.3390/nu14142925
de Arriba Fernández A, Alonso Bilbao JL, Espiñeira Francés A, Cabeza Mora A, Gutiérrez Pérez Á, Díaz Barreiros MÁ, Serra Majem L. Assessment of SARS-CoV-2 Infection According to Previous Metabolic Status and Its Association with Mortality and Post-Acute COVID-19. Nutrients. 2022; 14(14):2925. https://doi.org/10.3390/nu14142925
Chicago/Turabian Stylede Arriba Fernández, Alejandro, José Luis Alonso Bilbao, Alberto Espiñeira Francés, Antonio Cabeza Mora, Ángela Gutiérrez Pérez, Miguel Ángel Díaz Barreiros, and Lluís Serra Majem. 2022. "Assessment of SARS-CoV-2 Infection According to Previous Metabolic Status and Its Association with Mortality and Post-Acute COVID-19" Nutrients 14, no. 14: 2925. https://doi.org/10.3390/nu14142925